

One-Year Outcomes of CGuard Double Mesh Stent in Carotid Artery Disease: A Systematic Review and Meta-Analysis

 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
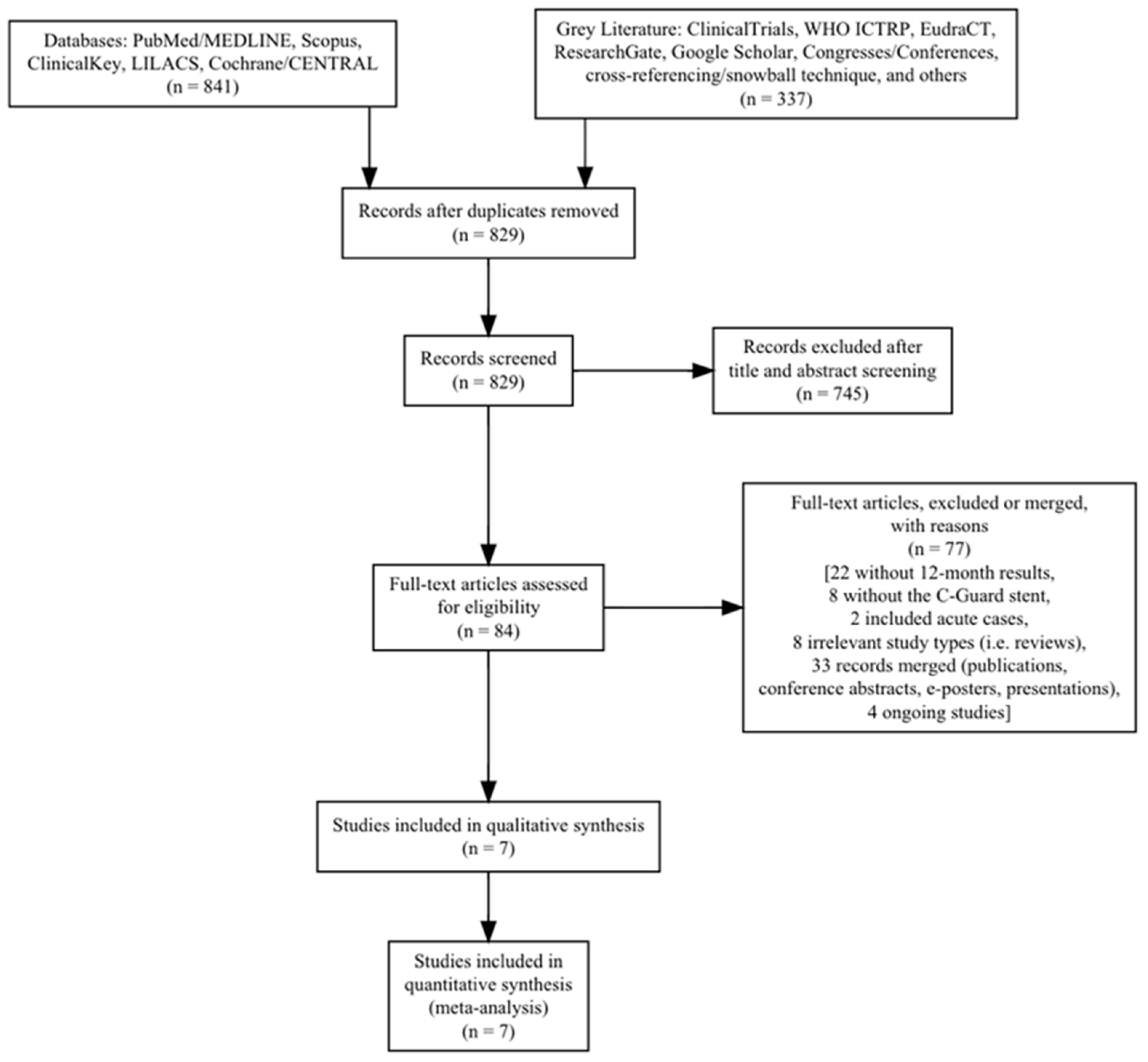
2. Methods
2.1. Inclusion–Exclusion Criteria
2.2. Data Search
2.3. Data Collection
2.4. Critical Appraisal
2.5. Statistical Analysis
2.6. Endpoints–Definitions
3. Results
Characteristics of Included Studies
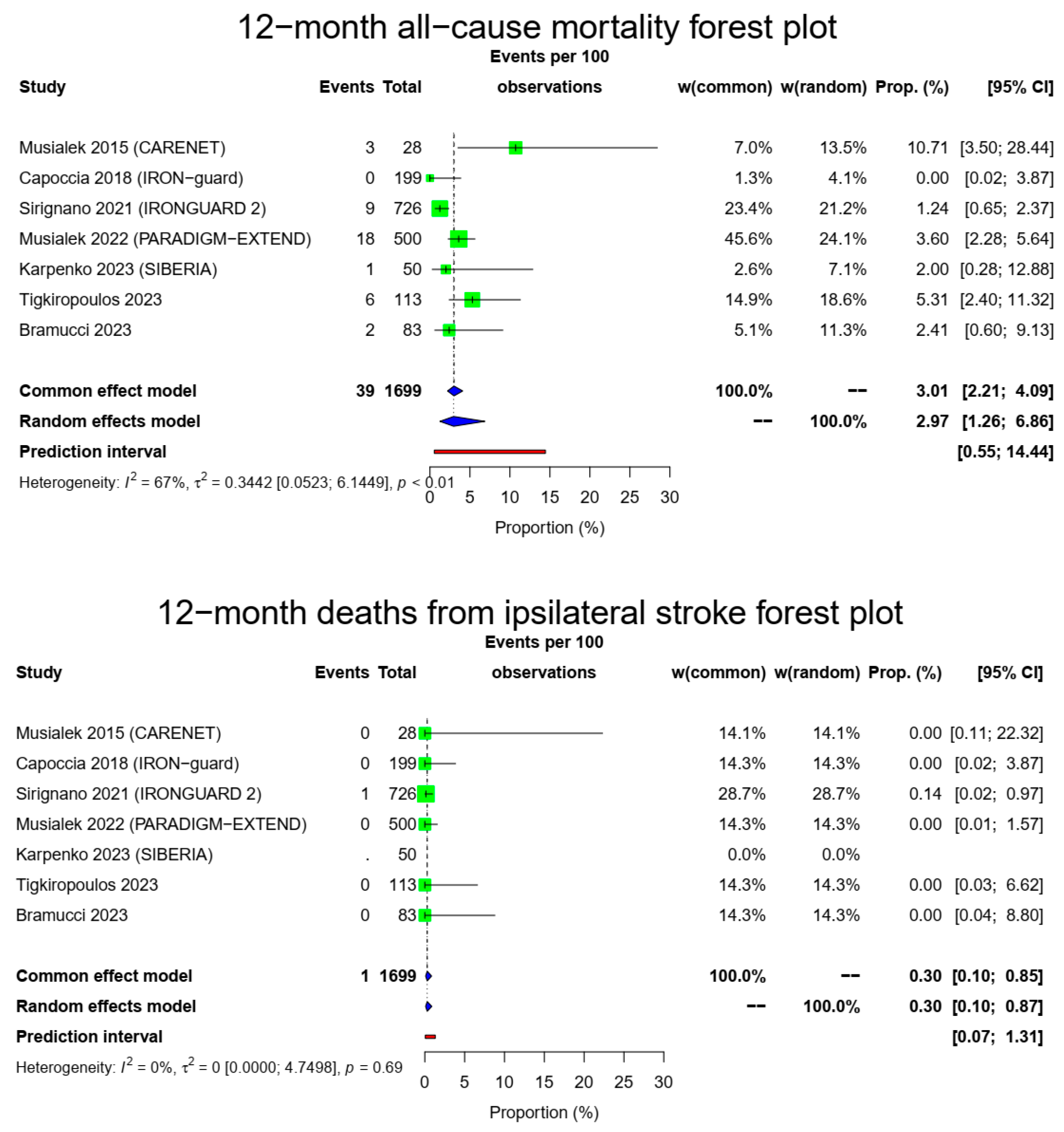
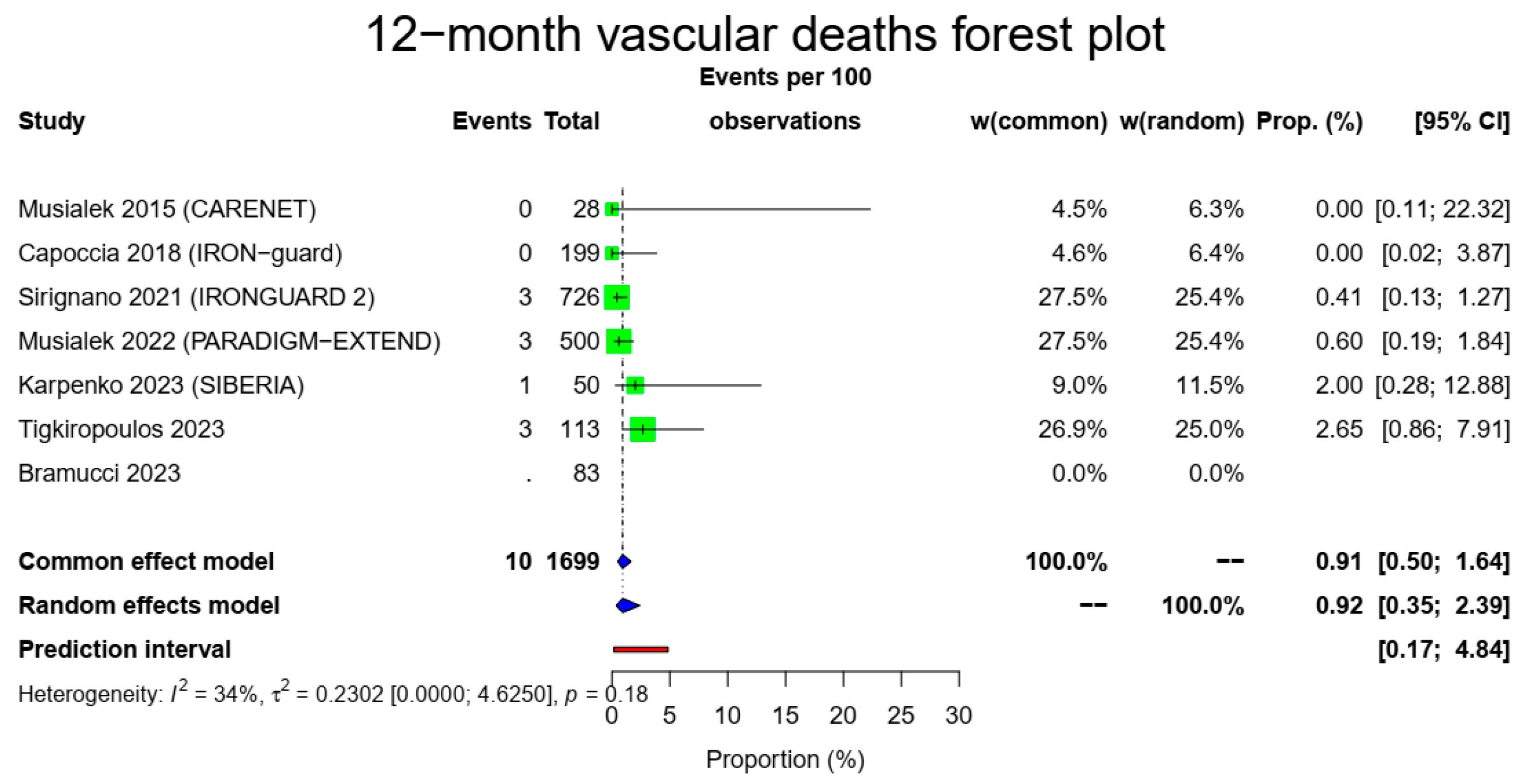
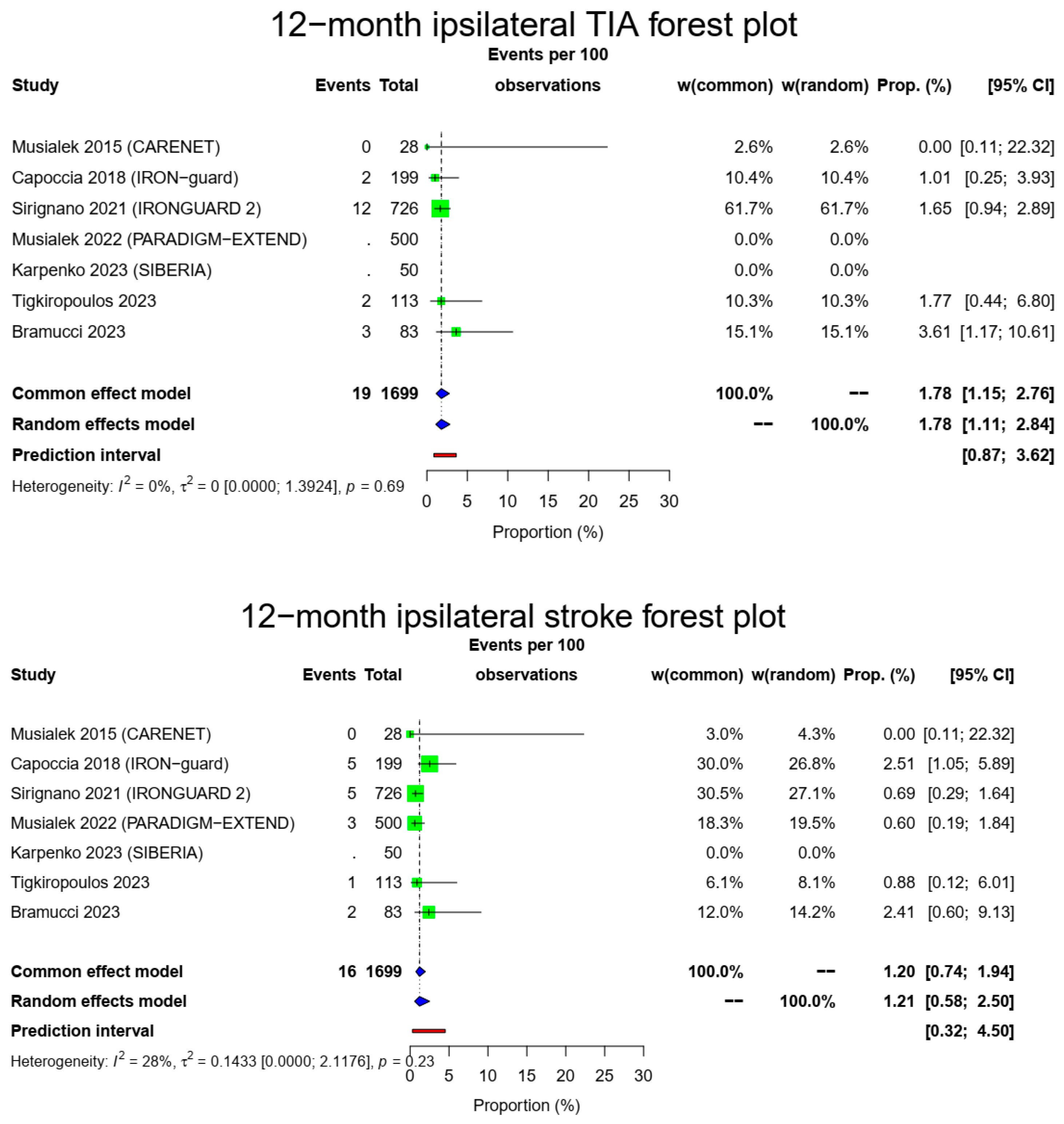
4. Findings
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hill, M.; Brooks, W.H.; Mackey, A.; Clark, M.W.; Meschia, F.J.; Morrish, F.W.; Mohr, J.P.; Rhodes, J.D.; Popma, J.J.; Lal, K.B.; et al. Stroke after carotid stenting and endarterectomy in the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST). Circulation 2012, 126, 3054–3061. [Google Scholar] [CrossRef]
- Bonati, L.H.; Jongen, L.M.; Haller, S.; Flach, H.Z.; Dobson, J.; Nederkoorn, P.J.; Macdonald, S.; Gaines, P.A.; Waaijer, A.; Stierli, P.; et al. New ischemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: A sub study of the International Carotid Stenting Study (ICSS). Lancet Neurol. 2010, 9, 353–362. [Google Scholar] [CrossRef]
- Fairman, R.; Gray, W.A.; Scicli, A.P.; Wilburn, O.; Verta, P.; Atkinson, R.; Yadav, J.S.; Wholey, M.; Hopkins, L.N.; Raabe, R.; et al. The CAPTURE registry-Analysis of strokes resulting from carotid artery stenting in the post approval setting: Timing, location, severity, and type. Ann. Surg. 2007, 246, 551–556. [Google Scholar] [CrossRef]
- Bosiers, M.; de Donato, G.; Deloose, K.; Verbist, J.; Peeters, P.; Castriota, F.; Cremonesi, A.; Setacci, C. Does free cell area influence the outcome in carotid artery stenting? Eur. J. Vasc. Endovasc. Surg. 2007, 33, 135–141. [Google Scholar] [CrossRef]
- Christopher, M.D. 30-Day Results from the C-Guardians Pivotal Trial of the CGuard™ Carotid Stent System. In Proceedings of the VIVA 2023, Las Vegas, NV, USA, 1 November 2023. [Google Scholar]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef]
- Musialek, P. The 3 Micromesh Stents and Their Value in CAS: Do the Design Differences Matter? Update on Carotid and Other Uses of the MicroNet-Covered Stent (C-Guard). In Proceedings of the Veith Symposium, New York, NY, USA, 19 November 2022. [Google Scholar]
- Musialek, P. OPTIMA Endovascular Exclusion of Consecutive Patient High-Risk Carotid Plaque Using the MicroNet Covered Stent (OPTIMA). ClinicalTrialsGov.ID. Available online: http://www.clinicaltrials.gov/study/NCT04234854 (accessed on 2 January 2024).
- Szkolka, L.; Lyko-Morawska, D.; Balocco, S.; Bedkowski, L.; Buczek, M.; Medon, E.; Wolkowski, M.; Dryjski, M.; Kuczmik, W. Vascular surgery study of the CGuard MicroNet-covered stent in patients with indication to carotid revascularization: POLGUARD. J. Cardiovasc. Surg. 2023, 18. [Google Scholar] [CrossRef]
- Schofer, J.; Musiałek, P.; Bijuklic, K.; Kolvenbach, R.; Trystula, M.; Siudak, Z.; Sievert, H. Prospective, Multicenter Study of a Novel Mesh-Covered Carotid Stent: The CGuard CARENET Trial (Carotid Embolic Protection Using MicroNet). JACC Cardiovasc. Interv. 2015, 8, 1229–1234. [Google Scholar] [CrossRef]
- Capoccia, L.; Sirignano, P.; Mansour, W.; Sbarigia, E.; Speziale, F. Twelve-month results of the Italian registry on protected CAS with the mesh-covered CGuard stent: The IRON-Guard study. EuroIntervention 2018, 14, 1150–1152. [Google Scholar] [CrossRef]
- Sirignano, P.; Stabile, E.; Mansour, W.; Capoccia, L.; Faccenna, F.; Intrieri, F.; Ferri, M.; Saccà, S.; Sponza, M.; Mortola, P.; et al. 1-Year Results From a Prospective Experience on CAS Using the CGuard Stent System: The IRONGUARD 2 Study. JACC Cardiovasc. Interv. 2021, 14, 1917–1923. [Google Scholar] [CrossRef]
- Karpenko, A.; Bugurov, S.; Ignatenko, P.; Starodubtsev, V.; Popova, I.; Malinowski, K.; Musialek, P. Randomized Controlled Trial of Conventional Versus MicroNet-Covered Stent in Carotid Artery Revascularization. JACC Cardiovasc. Interv. 2021, 14, 2377–2387. [Google Scholar] [CrossRef]
- Tigkiropoulos, K.; Sidiropoulou, K.; Abatzis-Papadopoulos, M.; Lazaridis, I.; Saratzis, N. 12-Month Outcomes of Carotid Artery Stenting with CGuard MicroNET-Covered Stent: A Single-Center Study in 113 Patients. Angiology 2023, 4, 33197231213679. [Google Scholar] [CrossRef]
- Bramucci, A.; Fontana, A.; Massoni, C.B.; Vecchiati, E.; Freyrie, A.; Tusini, N. Dual-vs. single-layer stents for endovascular treatment of symptomatic and asymptomatic internal carotid artery stenosis. Cardiovasc. Revasc. Med. 2023, 57, 34–40. [Google Scholar] [CrossRef]
- Müller, M.D.; Lyrer, P.; Brown, M.M.; Bonati, L.H. Carotid artery stenting versus endarterectomy for treatment of carotid artery stenosis. Cochrane Database Syst. Rev. 2020, 2, CD000515. [Google Scholar]
- He, D.; Liu, W.; Zhang, T. The Development of Carotid Stent Material. Interv. Neurol. 2015, 3, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Sheth, S.; Litvack, F.; Dev, V.; Fishbein, M.C.; Forrester, J.S.; Eigler, N. Subacute thrombosis and vascular injury resulting from slotted-tube nitinol and stainless steel stents in a rabbit carotid artery model. Circulation 1996, 94, 1733–1740. [Google Scholar] [CrossRef]
- Li, L.; Pan, S.; Zhou, X.; Meng, X.; Han, X.; Ren, Y.; Yang, K.; Guan, Y. Reduction of in-stent restenosis risk on nickel-free stainless steel by regulating cell apoptosis and cell cycle. PLoS ONE 2013, 8, e62193. [Google Scholar] [CrossRef]
- Tanaka, N.; Martin, J.B.; Tokunaga, K.; Abe, T.; Uchiyama, Y.; Hayabuchi, N.; Berkefeld, J.; Rüfenacht, D.A. Conformity of carotid stents with vascular anatomy: Evaluation in carotid models. AJNR Am. J. Neuroradiol. 2004, 25, 604–607. [Google Scholar]
- Vajda, Z.; Miloslavski, E.; Guthe, T.; Schmid, E.; Schul, C.; Albes, G.; Henkes, H. Treatment of intracranial atherosclerotic arterial stenoses with a balloon-expandable cobalt chromium stent (Coroflex Blue): Procedural safety, efficacy, and midterm patency. Neuroradiology 2010, 52, 645–651. [Google Scholar] [CrossRef]
- Stoeckel, D.; Pelton, A.; Duerig, T. Self-expanding nitinol stents: Material and design considerations. Eur. Radiol. 2004, 14, 292–301. [Google Scholar] [CrossRef]
- Nerla, R.; Micari, A.; Castriota, F.; Miccichè, E.; Ruffino, M.A.; de Donato, G.; Setacci, C.; Cremonesi, A. Carotid artery stenting with a new-generation double-mesh stent in three high-volume Italian centres: 12-month follow-up results. EuroIntervention 2018, 14, 1147–1149. [Google Scholar] [CrossRef]
- Bosiers, M.; Deloose, K.; Torsello, G.; Scheinert, D.; Maene, L.; Peeters, P.; Müller-Hülsbeck, S.; Sievert, H.; Langhoff, R.; Callaert, J.; et al. Evaluation of a new dual-layer micromesh stent system for the carotid artery: 12-month results from the CLEAR-ROAD study. EuroIntervention 2018, 14, 1144–1146. [Google Scholar] [CrossRef] [PubMed]
- Kedev, S.; Müller-Hülsbeck, S.; Langhoff, R. Real-World Study of a Dual-Layer Micromesh Stent in Elective Treatment of Symptomatic and Asymptomatic Carotid Artery Stenosis (ROADSAVER). Cardiovasc. Interv. Radiol. 2022, 45, 277–282. [Google Scholar] [CrossRef]
- Stabile, E.; de Donato, G.; Musialek, P.; Deloose, K.; Nerla, R.; Sirignano, P.; Mazurek, A.; Mansour, W.; Fioretti, V.; Esposito, F.; et al. Use of Dual-Layered Stents for Carotid Artery Angioplasty: 1-Year Results of a Patient-Based Meta-Analysis. JACC Cardiovasc. Interv. 2020, 13, 1709–1715. [Google Scholar] [CrossRef]
- Mazurek, A.; Malinowski, K.; Rosenfield, K.; Capoccia, L.; Speziale, F.; de Donato, G.; Setacci, C.; Wissgott, C.; Sirignano, P.; Tekieli, L.; et al. Clinical Outcomes of Second- versus First-Generation Carotid Stents: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 4819. [Google Scholar] [CrossRef] [PubMed]
- Reiff, T.; Eckstein, H.H.; Mansmann, U.; Jansen, O.; Fraedrich, G.; Mudra, H.; Böckler, D.; Böhm, M.; Brückmann, H.; Debus, E.S.; et al. Angioplasty in asymptomatic carotid artery stenosis vs. endarterectomy compared to best medical treatment: One-year interim results of SPACE-2. Int. J. Stroke 2019, 15, 1747493019833017. [Google Scholar] [CrossRef]
- Rosenfield, K.; Matsumura, J.S.; Chaturvedi, S.; Riles, T.; Ansel, G.M.; Metzger, D.C.; Wechsler, L.; Jaff, M.R.; Gray, W.; ACT I Investigators. Randomized Trial of Stent versus Surgery for Asymptomatic Carotid Stenosis. N. Engl. J. Med. 2016, 374, 1011–1020. [Google Scholar] [CrossRef]
- Steinvil, A.; Sadeh, B.; Arbel, Y.; Justo, D.; Belei, A.; Borenstein, N.; Banai, S.; Halkin, A. Prevalence and predictors of concomitant carotid and coronary artery atherosclerotic disease. J. Am. Coll. Cardiol. 2011, 57, 779. [Google Scholar] [CrossRef]
- Subherwal, S.; Bhatt, D.L.; Li, S.; Wang, T.Y.; Thomas, L.; Alexander, K.P.; Patel, M.R.; Ohman, E.M.; Gibler, W.B.; Peterson, E.D.; et al. Polyvascular disease and long-term cardiovascular outcomes in older patients with non-ST-segment-elevation myocardial infarction. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 541. [Google Scholar] [CrossRef]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European society for vascular surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Site(s) | Setting | Trial Identifier | Patients (Estimated) | Enrollment Phase | Already Published |
|---|---|---|---|---|---|---|---|
| PARADIGM-EXTEND [7] | Poland | Multi-center | Academic | NCT04271033 | 550 | Recruiting | 12-month results of up to 500 patients presented * |
| C-GUARDIANS [5] | Multiple countries | Multi-center | Company-sponsored | NCT04900844 | 316 | Finished | 30-day results, awaiting 12-month results |
| OPTIMA [8] | Multiple countries | Multi-center | Academic | NCT04234854 | 339 | Finished | 30-day results, awaiting 12-month results |
| POLGUARD [9] | Poland | Single-center | Academic | - | 203 | Finished | 30-day results, awaiting 12-month results |
| Study (First Author, Year, Acronym) | Country | Centers | Timing and Type | Source(s) of Information | All Patients | All Arteries | Patients Available for Follow-Up Studies |
|---|---|---|---|---|---|---|---|
| Musialek 2015 (CARENET) [10] | Germany, Poland | Multi-center | Prospective (cohort) | Publications, presentations | 30 | 30 | 28 |
| Capoccia 2018 (IRON-guard) [11] | Italy | Multi-center | Prospective (cohort) | Publications, presentations, conference abstracts | 200 | 200 | 199 |
| Sirignano 2021 (IRONGUARD 2) [12] | Italy | Multi-center | Prospective (cohort) | Publications, presentations, conference abstracts | 733 | 733 | 726 |
| Musialek 2022 (PARADIGM-EXTEND) [7] | Poland | Multi-center | Prospective (cohort) | Publications, ClinicalTrials protocol, presentations, conference abstracts | 500 | 533 | 500 |
| Karpenko 2023 (SIBERIA) [13] | Russia | Single-center | Prospective (RCT) | Publications, ClinicalTrials protocol, presentations, conference abstracts | 50 | 50 | 50 |
| Tigkiropoulos 2023 [14] | Greece | Single-center | Prospective (cohort) | Publications, individual patient data | 113 | 113 | 113 |
| Bramucci 2023 [15] | Italy | Single-center | Retrospective (cohort) | Publications, individual patient data | 83 | 83 | 83 |
| Study | All Patients | Patients with Follow-Up Available * | Males (%) | Arteries | Symptoms (%) | Age (m ± SD) | HTN (%) | CAD (%) | DM (%) | PAD (%) | Smoking History (%) ** | AF (%) | DLP (%) | EPD (%) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All EPD (%) | Proximal EPD (%) | Distal EPD (%) | ||||||||||||||
| Musialek 2015 (CARENET) [10] | 30 | 28 (93.3%) | 19 (63.3%) | 30 | 10 (33.3%) | 71.6 ± 7.6 | 25 (83.3%) | 8 (26.7%) | 7 (23.3%) | NR | 4 (13.3%) | NR | 27 (90%) | 30 (100%) | 1 (3.3%) | 29 (96.7%) |
| Capoccia 2018 (IRON-guard) [11] | 200 | 199 (0.5%) | 132 (66%) | 200 | 17 (8.5%) | 72.6 ± 7.09 | 174 (87%) | 68 (34%) | 56 (28%) | NR | 124 (62%) | NR | 148 (74%) | 200 (100%) | 18 (9%) | 182 (91%) |
| Sirignano 2021 (IRONGUARD 2) [12] | 733 | 726 (99%) | 516 (70.4%) | 733 | 131 (17.9%) | 73.03 ± 7.84 | 622 (84.9%) | 278 (37.9%) | 264 (36%) | NR | 429 (58.5%) | NR | 552 (75.3%) | 731 (99.7%) | 138 (18.9%) | 593 (81.1%) |
| Musialek 2022 (PARADIGM-EXTEND) [7] *** | 500 | 500 (100%) | 363 (72.6%) | 533 | 299 (59.8%) | 69.96 ± 8.14 | NR | 152 (30.4%) | NR | NR | NR | 68 (13.6%) | NR | 533 (100%) | 259 (48.6%) | 274 (51.4%) |
| Karpenko 2023 (SIBERIA) [13] | 50 | 50 (100%) | 38 (76%) | 50 | 16 (32%) | 65 ± 7.5 | 48 (96%) | 39 (78%) | 10 (20%) | 15 (30%) | 17 (34%) | NR | NR | 50 (100%) | 0 (0%) | 50 (100%) |
| Tigkiropoulos 2023 [14] **** | 113 | 113 (100%) | 82 (72.6%) | 113 | 54 (47.8%) | 70.14 ± 8.63 | 91 (80.5%) | 44 (38.9%) | 42 (37.2%) | 42 (37.2%) | 66 (58.4%) | 12 (10.6%) | 89 (78.8%) | 6 (5.3%) | 0 (0%) | 6 (100%) |
| Bramucci 2023 [15] **** | 83 | 83 (100%) | 65 (78.3%) | 83 | 30 (36.1%) | 73 ± 13 | 77 (92.8%) | 32 (38.6%) | 41 (49.4%) | NR | 64 (77.1%) | 14 (16.9%) | 79 (95.2%) | 81 (97.6%) | 59 (72.8%) | 22 (27.2%) |
| Total (%) | 1709 | 1699/1709 (99.4%) | 1215/1709 (71.1%) | 1742 | 557/1709 (32.6%) | 71.63 ± 8.39 | 1037/1209 (85.8%) | 621/1709 (36.3%) | 420/1209 (34.7%) | 57/163 (35%) | 704/1209 (58.2%) | 94/696 (13.5%) | 895/1159 (77.2%) | 1631/1742 (93.6%) | 475/1631 (29.1%) | 1156/1631 (70.9%) |
| Study | Clear Inclusion Criteria | Standard, Reliable Measurement | Valid Identification Method | Consecutive Inclusion of Patients | Complete Inclusion of Patients | Clear Report of Participant Demographics | Clear Report of Patient Clinical Information | Clear Report of Outcomes/Follow Up | Clear Report of Presenting Site(s)’/Clinic(s)’ Demographic Information * | Appropriate Statistical Analysis ** | Overall Appraisal |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Musialek 2015 (CARENET) [10] | Yes | Yes | Yes | Yes | Unsure | Yes | Yes | Yes | Unsure | Not applicable | Include |
| Capoccia 2018 (IRON-guard) [11] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unsure | Yes | Include |
| Sirignano 2021 (IRONGUARD 2) [12] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unsure | Yes | Include |
| Musialek 2022 (PARADIGM-EXTEND) [7] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unsure | Yes | Include |
| Karpenko 2023 (SIBERIA) [13] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unsure | Yes | Include |
| Tigkiropoulos [14] 2023 | Yes | Yes | Yes | Yes | Unsure | Yes | Yes | Yes | Unsure | Not applicable | Include |
| Bramucci 2023 [15] | Yes | Yes | Yes | No | Unsure | Yes | Yes | Yes | Unsure | Not applicable | Include |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tigkiropoulos, K.; Nikas, S.; Manolis, A.-P.; Sidiropoulou, K.; Stavridis, K.; Karamanos, D.; Lazaridis, I.; Saratzis, N. One-Year Outcomes of CGuard Double Mesh Stent in Carotid Artery Disease: A Systematic Review and Meta-Analysis. Medicina 2024, 60, 286. https://doi.org/10.3390/medicina60020286
Tigkiropoulos K, Nikas S, Manolis A-P, Sidiropoulou K, Stavridis K, Karamanos D, Lazaridis I, Saratzis N. One-Year Outcomes of CGuard Double Mesh Stent in Carotid Artery Disease: A Systematic Review and Meta-Analysis. Medicina. 2024; 60(2):286. https://doi.org/10.3390/medicina60020286
Chicago/Turabian StyleTigkiropoulos, Konstantinos, Spyridon Nikas, Abatzis-Papadopoulos Manolis, Katerina Sidiropoulou, Kyriakos Stavridis, Dimitrios Karamanos, Ioannis Lazaridis, and Nikolaos Saratzis. 2024. "One-Year Outcomes of CGuard Double Mesh Stent in Carotid Artery Disease: A Systematic Review and Meta-Analysis" Medicina 60, no. 2: 286. https://doi.org/10.3390/medicina60020286
APA StyleTigkiropoulos, K., Nikas, S., Manolis, A.-P., Sidiropoulou, K., Stavridis, K., Karamanos, D., Lazaridis, I., & Saratzis, N. (2024). One-Year Outcomes of CGuard Double Mesh Stent in Carotid Artery Disease: A Systematic Review and Meta-Analysis. Medicina, 60(2), 286. https://doi.org/10.3390/medicina60020286