
Risk Factor Analysis Including Inflammatory Markers for ICU Admission and Survival After Pneumonectomy


Abstract
1. Introduction
2. Materials and Methods
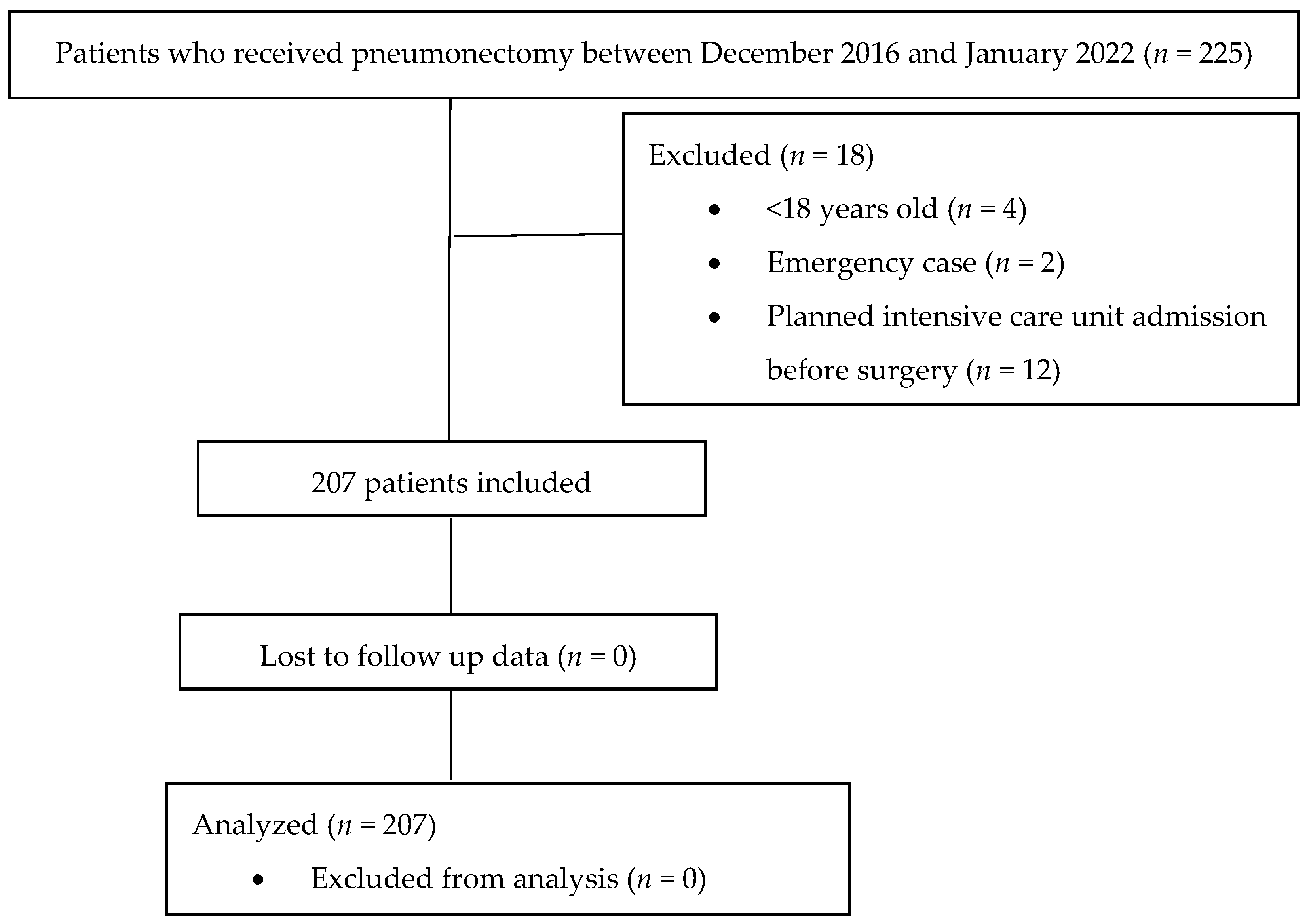
2.1. Study Groups
2.2. Study Design
2.3. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Need for ICU Admission After Pneumonectomy
3.3. Logistic Regression Analysis to Determine Predictors of ICU Admission After Pneumonectomy
3.4. Twenty-Eight-Day Survival After Pneumonectomy
3.5. Ninety-Day Survival After Pneumonectomy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hamaji, M.; Keegan, M.T.; Cassivi, S.D.; Shen, K.R.; Wigle, D.A.; Allen, M.S.; Nichols, F.C., 3rd; Deschamps, C. Outcomes in patients requiring mechanical ventilation following pneumonectomy. Eur. J. Cardio-Thorac. Surg. 2014, 46, e14–e19. [Google Scholar] [CrossRef] [PubMed]
- Blanc, K.; Dechartres, A.; Zaimi, R.; Lefebvre, A.; Janet-Vendroux, A.; Fournel, L.; Dermine, H.; Lorut, C.; Becanne, X.; Hamelin-Canny, E.; et al. Patients experiencing early acute respiratory failure have high postoperative mortality after pneumonectomy. J. Thorac. Cardiovasc. Surg. 2018, 156, 2368–2376. [Google Scholar] [CrossRef] [PubMed]
- Mansour, Z.; Kochetkova, E.A.; Santelmo, N.; Meyer, P.; Wihlm, J.M.; Quoix, E.; Massard, G. Risk factors for early mortality and morbidity after pneumonectomy: A reappraisal. Ann. Thorac. Surg. 2009, 88, 1737–1743. [Google Scholar] [CrossRef] [PubMed]
- Schneider, L.; Farrokhyar, F.; Schieman, C.; Shargall, Y.; D’Souza, J.; Camposilvan, I.; Hanna, W.C.; Finley, C.J. Pneumonectomy: The burden of death after discharge and predictors of surgical mortality. Ann. Thorac. Surg. 2014, 98, 1976–1982. [Google Scholar] [CrossRef]
- Yu, X.; Gao, S.; Xue, Q.; Tan, F.; Gao, Y.; Mao, Y.; Wang, D.; Zhao, J.; Li, Y.; Wang, F.; et al. Development of a nomogram for predicting the operative mortality of patients who underwent pneumonectomy for lung cancer: A population-based analysis. Transl. Lung Cancer Res. 2021, 10, 381–391. [Google Scholar] [CrossRef]
- Daffrè, E.; Prieto, M.; Huang, H.; Janet-Vendroux, A.; Blanc, K.; N’Guyen, Y.L.; Fournel, L.; Alifano, M. Normalized pulmonary artery diameter predicts occurrence of postpneumonectomy respiratory failure, ARDS, and mortality. Cancers 2020, 12, 1515. [Google Scholar] [CrossRef]
- Łochowski, M.; Łochowska, B.; Zawadzka, I.; Cieślik-Wolski, B.; Kozik, D.; Kozak, J. Prognostic value of neutrophil-to-lymphocyte, platelet-to-lymphocyte and lymphocyte-to-monocyte ratio ratios in patients operated on due to non-small cell lung cancer. J. Thorac. Dis. 2019, 11, 3377–3384. [Google Scholar] [CrossRef]
- Brunelli, A.; Begum, H.; Chaudhuri, N.; Agzarian, J.; Milton, R.; Finley, C.; Tcherveniakov, P.; Valuckiene, L.; Gioutsos, K.; Hanna, W.; et al. A risk model to predict an unplanned admission to the intensive care unit following lung resection. Eur. J. Cardio-Thorac. Surg. 2022, 61, 1232–1239. [Google Scholar] [CrossRef]
- Jeon, K.; Yoon, J.W.; Suh, G.Y.; Kim, J.; Kim, K.; Yang, M.; Kim, H.; Kwon, O.J.; Shim, Y.M. Risk factors for post-pneumonectomy acute lung injury/acute respiratory distress syndrome in primary lung cancer patients. Anaesth. Intensive Care 2009, 37, 14–19. [Google Scholar] [CrossRef]
- Roviaro, G.; Varoli, F.; Romanelli, A.; Vergani, C.; Maciocco, M. Complications of tracheal sleeve pneumonectomy: Personal experience and overview of the literature. J. Thorac. Cardiovasc. Surg. 2001, 121, 234–240. [Google Scholar] [CrossRef]
- Kidane, B.; Plourde, M.; Leydier, L.; Chadi, S.A.; Eckert, K.; Srinathan, S.; Fortin, D.; Frechette, E.; Inculet, R.I.; Malthaner, R.A. RBC transfusion is associated with increased risk of respiratory failure after pneumonectomy. J. Surg. Oncol. 2017, 115, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wu, J.; Zhang, F.; Ying, L.; Chen, Y. Prognostic significance of pre-operative monocyte-to-lymphocyte ratio in lung cancer patients undergoing radical surgery. Lab. Med. 2018, 49, e29–e39. [Google Scholar] [CrossRef] [PubMed]
- Micaela, R.; Lucas, C.; Franco, C.; Federico, C.; Agustín, D.; David, S. Dynamic perioperative variation of neutrophil-to-lymphocyte ratio as an independent prognosis factor following lobectomy for NSCLC. Updates Surg. 2021, 73, 1567–1574. [Google Scholar] [CrossRef] [PubMed]
- Ramos, R.; Macía, I.; Navarro-Martin, A.; Déniz, C.; Rivas, F.; Ureña, A.; Masuet-Aumatell, C.; Moreno, C.; Nadal, E.; Escobar, I. Prognostic value of the preoperative lymphocyte-to-monocyte ratio for survival after lung cancer surgery. BMC Pulm. Med. 2021, 21, 75. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Wu, Y.; Chen, J.; Chang, K.Y.; Cherng, Y.G.; Lin, S.P.; Tsou, M.Y.; Tai, Y.H. A comparison of inflammation markers for predicting oncological outcomes after surgical resection of non-small-cell lung cancer: A validated analysis of 2066 patients. Sci. Rep. 2020, 10, 19523. [Google Scholar] [CrossRef]
- Zhang, J.; Bai, W.; Guo, C.; Liu, L.; Wang, G.; Huang, C.; Chen, Y.; Zhang, Y.; Li, S. Postoperative short-term outcomes between sublobar resection and lobectomy in patients with lung adenocarcinoma. Cancer Manag. Res. 2020, 12, 9485–9493. [Google Scholar] [CrossRef]
- Yamagishi, T.; Fujimoto, N.; Nishi, H.; Miyamoto, Y.; Hara, N.; Asano, M.; Fuchimoto, Y.; Wada, S.; Kitamura, K.; Ozaki, S.; et al. Prognostic significance of the lymphocyte-to-monocyte ratio in patients with malignant pleural mesothelioma. Lung Cancer 2015, 90, 111–117. [Google Scholar] [CrossRef]
- Lee, B.M.; Rodrigeuz, A.; Mena, G.; Gottumukkala, V.; Mehran, R.J.; Rice, D.C.; Feng, L.; Yu, J.; Cata, J.P. Platelet-to-lymphocyte ratio and use of NSIADs during perioperative period as prognostic indicators in patients with NSCLC undergoing surgery. Cancer Control 2016, 23, 284–294. [Google Scholar] [CrossRef]
- Xu, F.; Xu, P.; Cui, W.; Gong, W.; Wei, Y.; Liu, B.; Dong, J. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios may aid and identifying patients with non-small cell lung cancer and predicting tumor-node-metastases stage. Oncol. Lett. 2018, 16, 483–490. [Google Scholar] [CrossRef]
- Özer, A.; Tak, S.; Demirtaş, H.; Yıldırım, A.K.; Şimşek, E.; Oktar, G.L.; Kaya, Z. The role of monocyte distribution width in the early prediction of sepsis in patients undergoing cardiovascular surgery: A cross-sectional study. Medicina 2024, 60, 1558. [Google Scholar] [CrossRef]
- Tingle, S.J.; Severs, G.R.; Goodfellow, M.; Moir, J.A.; White, S.A. NARCA: A novel prognostic scoring system using neutrophil-albumin ratio and Ca19-9 to predict overall survival in palliative pancreatic cancer. J. Surg. Oncol. 2018, 118, 680–686. [Google Scholar] [CrossRef]
- Tawfik, B.; Mokdad, A.A.; Patel, P.M.; Li, H.C.; Huerta, S. The neutrophil to albumin ratio as a predictor of pathological complete response in rectal cancer patients following neoadjuvant chemoradiation. Anticancer Drugs 2016, 27, 879–883. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Need for ICU Admission | |||
|---|---|---|---|
| No (n = 119) | Yes (n = 88) | p-Value | |
| Age (year) | 55.59 ± 11.30 | 57.60 ± 12.39 | 0.225 |
| Gender (male/female) | 107/12 | 80/8 | 0.999 |
| Smoking history (no/yes) | 37/82 | 39/49 | 0.059 |
| Comorbidity | |||
| 3 | 4 | 0.463 |
| 10 | 12 | 0.259 |
| 5 | 10 | 0.060 |
| 10 | 9 | 0.808 |
| 6 | 6 | 0.765 |
| Neo-adjuvant therapy | |||
| 94 | 67 | 0.735 |
| 25 | 21 | |
| 17 | 14 | 0.844 |
| 8 | 7 | 0.790 |
| Duration of surgery | |||
| 93 | 75 | 0.214 |
| 26 | 13 | |
| Surgical approach (Thoracotomy/VATS) | 107/12 | 85/3 | 0.102 |
| Side of surgery (right/left) | 42/77 | 36/52 | 0.469 |
| Surgical procedure | |||
| 105 | 60 | |
| 2 | 7 | 0.001 |
| 12 | 21 | |
| Intraoperative complications | |||
| 119 | 85 | |
| 0 | 2 | 0.075 |
| 0 | 1 | |
| Postoperative complications | |||
| 108 | 57 | <0.001 |
| 11 | 31 | |
| 3 | 5 | 0.289 |
| 5 | 1 | 0.244 |
| 1 | 5 | 0.085 |
| 1 | 3 | 0.314 |
| 5 | 13 | 0.011 |
| 0 | 11 | <0.001 |
| 1 | 6 | 0.043 |
| Laboratory parameters | |||
| 2.05 ± 0.79 | 2.10 ± 0.86 | 0.652 |
| 0.83 ± 0.44 | 0.87 ± 0.38 | 0.196 |
| 7.07 ± 3.68 | 6.97 ± 3.97 | 0.545 |
| 308.16 ± 106.29 | 319.36 ± 113.98 | 0.468 |
| 2.86 ± 1.50 | 2.65 ± 1.13 | 0.598 |
| 169.44 ± 77.28 | 181.75 ± 124.90 | 0.848 |
| 4.07 ± 3.14 | 4.07 ± 3.75 | 0.453 |
| 3.38 ± 0.62 | 3.15 ± 0.70 | 0.017 |
| 2.22 ± 1.36 | 2.37 ± 1.42 | 0.396 |
| 10.12 ± 3.92 | 10.34 ± 4.68 | 0.718 |
| 12.99 ± 1.86 | 12.70 ± 1.85 | 0.267 |
| 38.92 ± 5.20 | 38.46 ± 5.41 | 0.531 |
| 13.67 ± 4.16 | 14.87 ± 5.59 | 0.093 |
| 0.83 ± 0.24 | 0.87 ± 0.28 | 0.276 |
| Need for blood transfusion | 16 (13.6%) | 24 (27.3%) | 0.020 |
| Length of hospital stay (day) | 8 (6–9) | 9 (6–14) | 0.026 |
| p-Value | OR | 95%CI for OR | |
|---|---|---|---|
| Age | 0.381 | 1.01 | 0.98–1.05 |
| Gender | 0.366 | 1.70 | 0.54–5.35 |
| Albumin | 0.065 | 0.63 | 0.38–1.03 |
| Procedure (standard pneumonectomy) | 0.006 | Ref. | Ref. |
| Sleeve pneumonectomy | 0.066 | 5.29 | 0.90–31.20 |
| Intra-pericardial pneumonectomy | 0.005 | 3.46 | 1.45–8.23 |
| Postoperative complications | <0.001 | 5.10 | 2.21–11.79 |
| The need for blood transfusion | 0.072 | 2.15 | 0.934–4.94 |
| Alive (n = 199) | Died (n = 8) | p-Value | |
|---|---|---|---|
| Age (year) | 56.21 ± 11.91 | 62.38 ± 5.83 | 0.147 |
| Gender (male/female) | 179/20 | 8/0 | 0.999 |
| Smoking history (no/yes) | 74/125 | 2/6 | 0.713 |
| Comorbidity | |||
| 6 | 1 | 0.245 |
| 20 | 2 | 0.204 |
| 15 | 0 | 0.999 |
| 18 | 1 | 0.544 |
| 12 | 0 | 0.999 |
| Neo-adjuvant therapy | |||
| 156 | 5 | 0.380 |
| 43 | 3 | |
| 30 | 1 | 0.999 |
| 13 | 2 | 0.107 |
| Duration of surgery | |||
| 161 | 7 | 0.999 |
| 38 | 1 | |
| Surgical approach (Thoracotomy/VATS) | 184/15 | 8/0 | 0.999 |
| Side of surgery (right/left) | 74/125 | 4/4 | 0.479 |
| Surgical procedure | |||
| 162 | 3 | |
| 8 | 1 | 0.010 |
| 29 | 4 | |
| Intraoperative complications | |||
| 197 | 7 | |
| 1 | 1 | 0.003 |
| 1 | 0 | |
| Need for mechanical ventilation | 9 (4.5%) | 8 (100%) | <0.001 |
| Postoperative complications | |||
| 164 (82.4%) | 1 (12.5%) | <0.001 |
| 35 (17.6%) | 7 (87.5%) | |
| 7 | 1 | 0.274 |
| 6 | 0 | 0.999 |
| 4 | 2 | 0.018 |
| 2 | 2 | 0.008 |
| 16 | 2 | 0.146 |
| 7 | 4 | <0.001 |
| 5 | 2 | 0.025 |
| Laboratory parameters | |||
| 2.09 ± 0.82 | 1.76 ± 0.67 | 0.262 |
| 0.85 ± 0.42 | 0.90 ± 0.34 | 0.683 |
| 6.96 ± 3.66 | 8.60 ± 6.54 | 0.237 |
| 314.84 ± 110.70 | 265.13 ± 59.10 | 0.209 |
| 2.79 ± 1.36 | 2.17 ± 1.32 | 0.205 |
| 174.75 ± 100.98 | 172.84 ± 85.03 | 0.958 |
| 4.02 ± 3.35 | 5.53 ± 4.46 | 0.219 |
| 3.29 ± 0.65 | 3.22 ± 1.02 | 0.796 |
| 2.26 ± 1.36 | 2.87 ± 1.99 | 0.512 |
| 10.17 ± 4.15 | 11.35 ± 6.56 | 0.442 |
| 12.90 ± 1.87 | 12.03 ± 1.39 | 0.198 |
| 38.78 ± 5.31 | 37.21 ± 4.59 | 0.410 |
| 14.05 ± 4.82 | 17.53 ± 4.62 | 0.046 |
| 0.84 ± 0.25 | 1.11 ± 0.38 | 0.004 |
| Need for blood transfusion | 36 (18.1%) | 4 (50%) | 0.047 |
| Length of hospital stay (day) | 8 (6–11) | 9 (4–23) | 0.098 |
| Alive (n =193) | Died (n =14) | p-Value | |
|---|---|---|---|
| Age (year) | 56.35 ± 11.54 | 57.71 ± 15.19 | 0.677 |
| Gender (male/female) | 174/19 | 13/1 | 0.999 |
| Smoking history (no/yes) | 72/121 | 4/10 | 0.580 |
| Comorbidity | |||
| 6 | 1 | 0.394 |
| 19 | 3 | 0.175 |
| 15 | 0 | 0.605 |
| 18 | 1 | 0.999 |
| 12 | 0 | 0.999 |
| Neo-adjuvant therapy | |||
| 150 | 11 | 0.999 |
| 43 | 3 | |
| 30 | 1 | 0.699 |
| 13 | 2 | 0.269 |
| Duration of surgery | |||
| 155 | 13 | 0.476 |
| 38 | 1 | |
| Surgical approach (Thoracotomy/VATS) | 178/15 | 14/0 | 0.605 |
| Side of surgery (right/left) | 70/123 | 8/6 | 0.154 |
| Surgical procedure | |||
| 159 | 6 | |
| 7 | 2 | 0.002 |
| 27 | 6 | |
| Intraoperative complications | |||
| 191 | 13 | |
| 1 | 1 | 0.049 |
| 1 | 0 | |
| Need for mechanical ventilation (no/yes) | 187/6 | 3/11 | <0.001 |
| Postoperative complications | |||
| 162 (83.9%) | 3 (21.4%) | <0.001 |
| 31 (16.1%) | 11 (78.6%) | |
| 7 | 1 | 0.435 |
| 6 | 0 | 0.999 |
| 4 | 2 | 0.055 |
| 0 | 4 | <0.001 |
| 15 | 3 | 0.109 |
| 4 | 7 | <0.001 |
| 2 | 5 | <0.001 |
| Laboratory parameters | |||
| 2.10 ± 0.82 | 1.72 ± 0.73 | 0.093 |
| 0.85 ± 0.42 | 0.78 ± 0.33 | 0.525 |
| 6.93 ± 3.67 | 8.38 ± 5.29 | 0.168 |
| 313.41 ± 111.05 | 306 ± 88.22 | 0.811 |
| 2.80 ± 1.37 | 2.41 ± 1.17 | 0.307 |
| 171.47 ± 96.34 | 218 ± 140.90 | 0.880 |
| 3.93 ± 3.17 | 6.13 ± 5.47 | 0.019 |
| 3.30 ± 0.6 | 2.97 ± 1.0 | 0.067 |
| 2.23 ± 1.35 | 3.03 ± 1.73 | 0.061 |
| 10.15 ± 4.18 | 11.01 ± 5.21 | 0.468 |
| 12.89 ± 1.87 | 12.50 ± 1.72 | 0.453 |
| 38.76 ± 5.30 | 38.22 ± 5.26 | 0.713 |
| 14.07 ± 4.82 | 15.72 ± 5.13 | 0.219 |
| 0.84 ± 0.25 | 1.03 ± 0.30 | 0.008 |
| Need for blood transfusion | 158/35 | 9/5 | 0.152 |
| Length of hospital stay (day) | 9.57 ± 5.48 | 20.36 ± 21.16 | <0.001 |
| 8 (6–10) | 11 (6–29) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turktan, M.; Gulec, E.; Avcı, A.; Hatıpoglu, Z.; Unal, I. Risk Factor Analysis Including Inflammatory Markers for ICU Admission and Survival After Pneumonectomy. Medicina 2024, 60, 1768. https://doi.org/10.3390/medicina60111768
Turktan M, Gulec E, Avcı A, Hatıpoglu Z, Unal I. Risk Factor Analysis Including Inflammatory Markers for ICU Admission and Survival After Pneumonectomy. Medicina. 2024; 60(11):1768. https://doi.org/10.3390/medicina60111768
Chicago/Turabian StyleTurktan, Mediha, Ersel Gulec, Alper Avcı, Zehra Hatıpoglu, and Ilker Unal. 2024. "Risk Factor Analysis Including Inflammatory Markers for ICU Admission and Survival After Pneumonectomy" Medicina 60, no. 11: 1768. https://doi.org/10.3390/medicina60111768
APA StyleTurktan, M., Gulec, E., Avcı, A., Hatıpoglu, Z., & Unal, I. (2024). Risk Factor Analysis Including Inflammatory Markers for ICU Admission and Survival After Pneumonectomy. Medicina, 60(11), 1768. https://doi.org/10.3390/medicina60111768