The Effectiveness of Lifestyle Changes in Glycemic Control among Pregnant Women with Gestational Diabetes Mellitus


Abstract
:1. Introduction
2. Materials and Methods
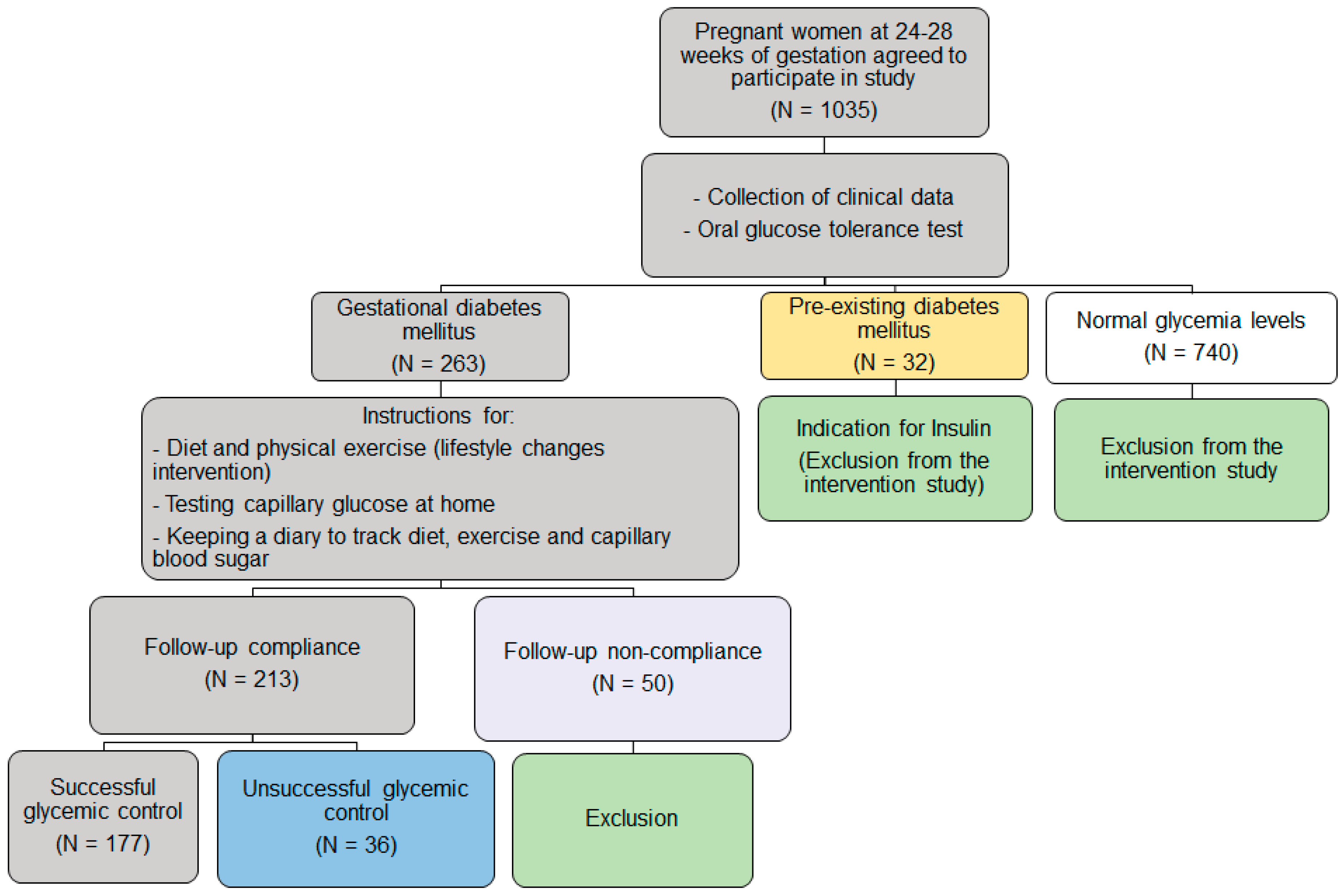
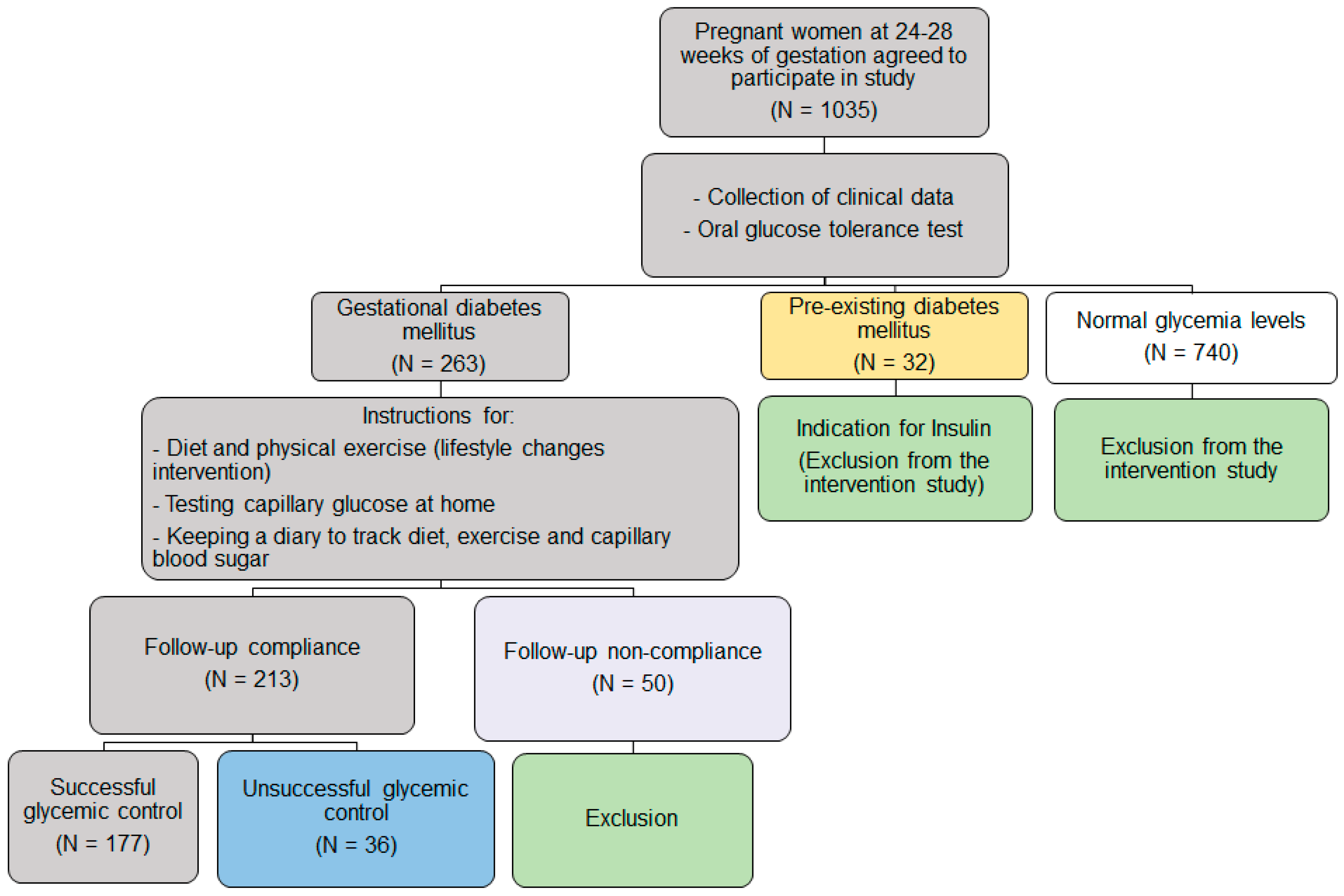
2.1. Study Design and Study Participants
2.2. Selection and Exclusion Criteria
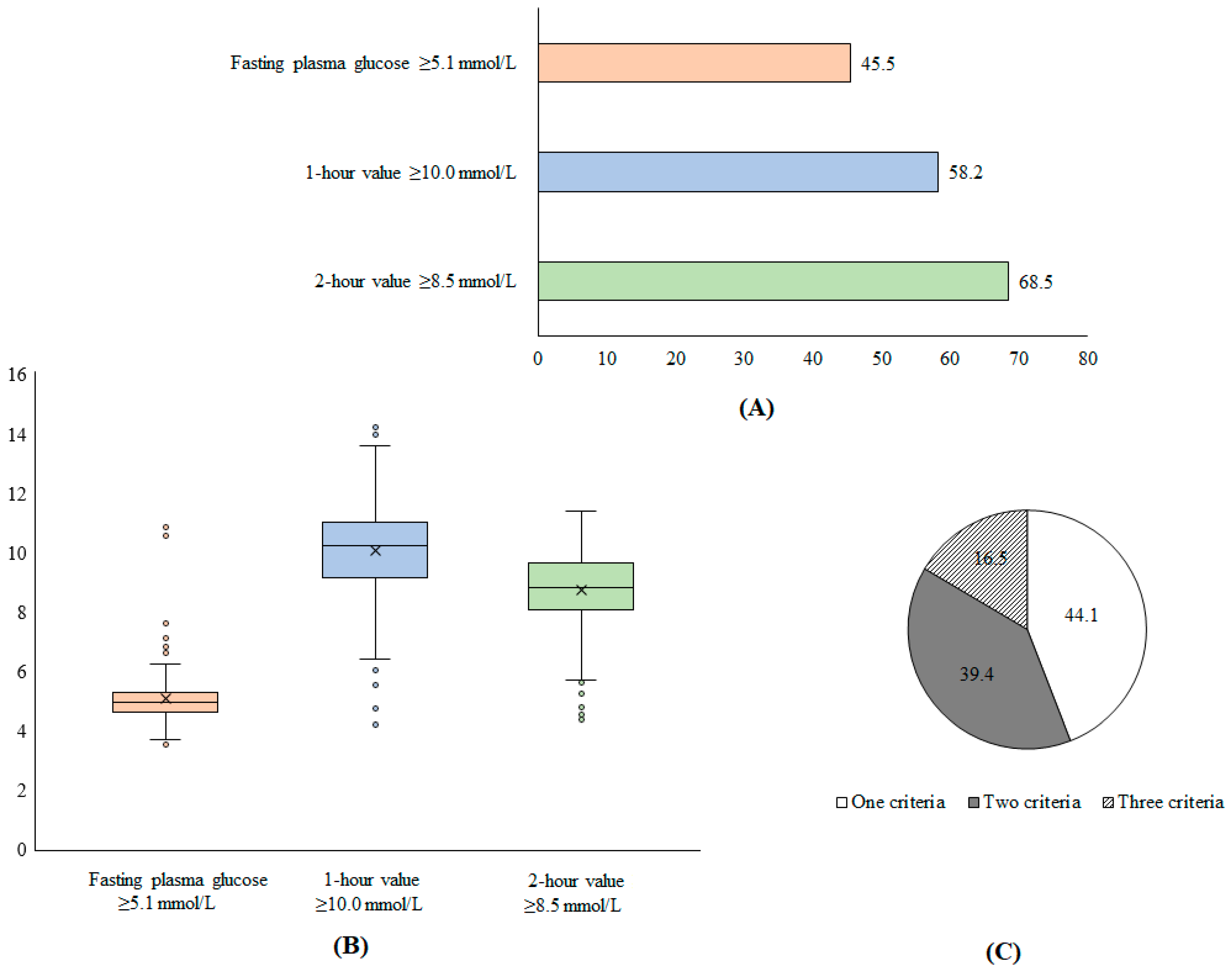
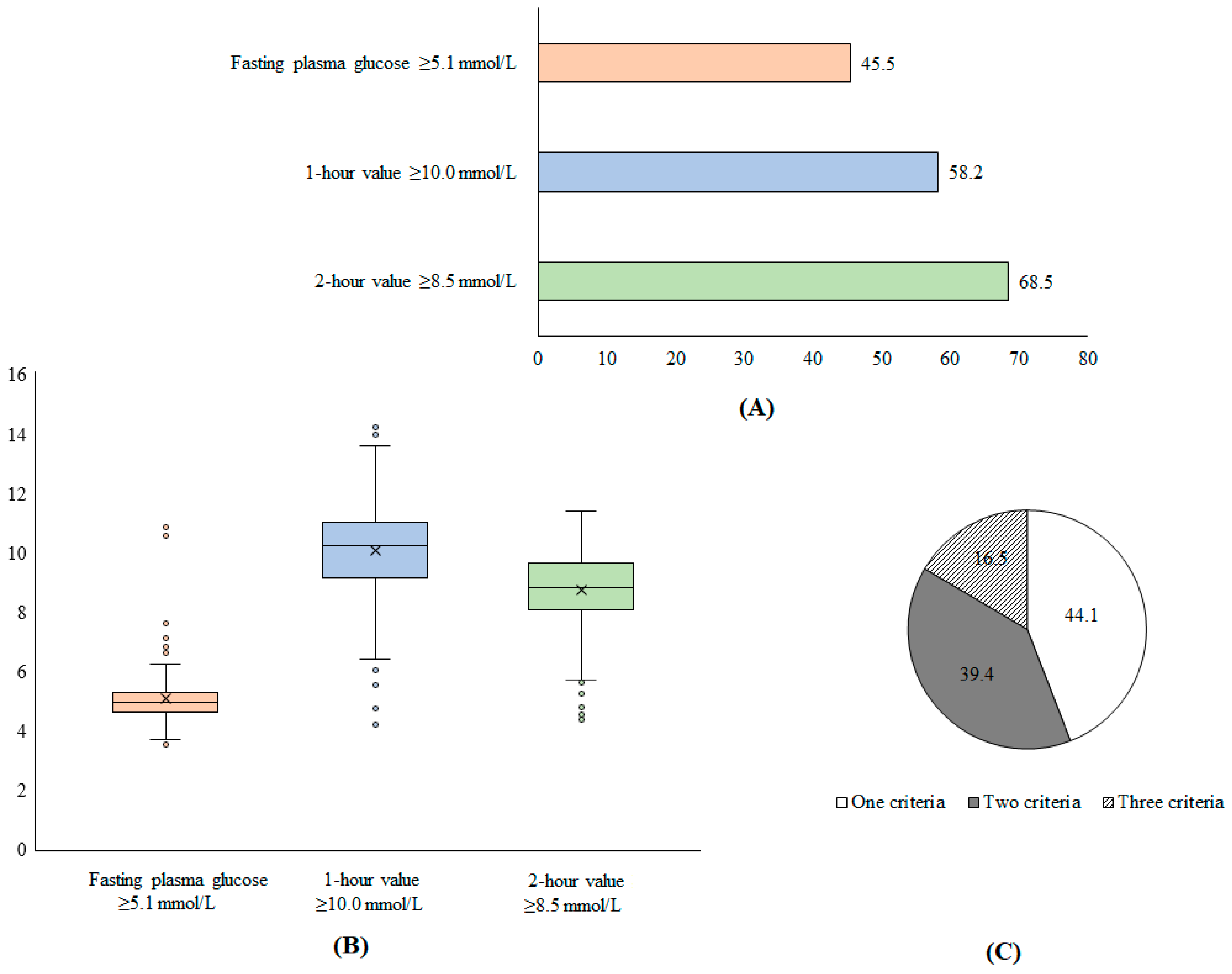
2.3. Diagnostic Criteria
2.4. Lifestyle Intervention
2.5. Evaluation of Intervention Effectiveness
2.6. Data Analysis
3. Results
3.1. Characteristics of Participants
3.2. Effectiveness of Lifestyle Changes in Glycemic Control among Pregnant with GDM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]
- Bellamy, L.; Casas, J.-P.; Hingorani, A.D.; Williams, D. Type 2 Diabetes Mellitus after Gestational Diabetes: A Systematic Review and Meta-Analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Doğan, H.; Demir Çaltekin, M. Plantar Sensation, Proprioception, and Balance Levels in Pregnant Women with Gestational Diabetes Mellitus. Clin. Biomech. 2023, 107, 106016. [Google Scholar] [CrossRef]
- Lin, X.; Yang, T.; Zhang, X.; Wei, W. Lifestyle Intervention to Prevent Gestational Diabetes Mellitus and Adverse Maternal Outcomes among Pregnant Women at High Risk for Gestational Diabetes Mellitus. J. Int. Med. Res. 2020, 48, 0300060520979130. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, L.; Poulsen, C.W.; Kampmann, U.; Smedegaard, S.B.; Ovesen, P.G.; Fuglsang, J. Diet and Healthy Lifestyle in the Management of Gestational Diabetes Mellitus. Nutrients 2020, 12, 3050. [Google Scholar] [CrossRef] [PubMed]
- Zakaria, H.; Abusanana, S.; Mussa, B.M.; Al Dhaheri, A.S.; Stojanovska, L.; Mohamad, M.N.; Saleh, S.T.; Ali, H.I.; Cheikh Ismail, L. The Role of Lifestyle Interventions in the Prevention and Treatment of Gestational Diabetes Mellitus. Medicina 2023, 59, 287. [Google Scholar] [CrossRef] [PubMed]
- Farrar, D.; Simmonds, M.; Bryant, M.; Sheldon, T.A.; Tuffnell, D.; Golder, S.; Dunne, F.; Lawlor, D.A. Hyperglycaemia and Risk of Adverse Perinatal Outcomes: Systematic Review and Meta-Analysis. BMJ 2016, 354, i4694. [Google Scholar] [CrossRef]
- Moses, R.G.; Barker, M.; Winter, M.; Petocz, P.; Brand-Miller, J.C. Can a Low–Glycemic Index Diet Reduce the Need for Insulin in Gestational Diabetes Mellitus? Diabetes Care 2009, 32, 996–1000. [Google Scholar] [CrossRef]
- Cremona, A.; O’Gorman, C.; Cotter, A.; Saunders, J.; Donnelly, A. Effect of Exercise Modality on Markers of Insulin Sensitivity and Blood Glucose Control in Pregnancies Complicated with Gestational Diabetes Mellitus: A Systematic Review. Obes. Sci. Pract. 2018, 4, 455–467. [Google Scholar] [CrossRef]
- Barakat, R.; Cordero, Y.; Coteron, J.; Luaces, M.; Montejo, R. Exercise during Pregnancy Improves Maternal Glucose Screen at 24-28 Weeks: A Randomised Controlled Trial. Br. J. Sports Med. 2012, 46, 656–661. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Physical Activity and Exercise During Pregnancy and the Postpartum Period: ACOG Committee Opinion, Number 804. Obstet. Gynecol. 2020, 135, e178–e188. [Google Scholar] [CrossRef]
- Lin, L.; Lin, J.; Yan, J. Interactive Affection of Pre-Pregnancy Overweight or Obesity, Excessive Gestational Weight Gain and Glucose Tolerance Test Characteristics on Adverse Pregnancy Outcomes Among Women with Gestational Diabetes Mellitus. Front. Endocrinol. 2022, 13, 942271. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-W.; Soh, S.E.; Tint, M.-T.; Loy, S.L.; Yap, F.; Tan, K.H.; Lee, Y.S.; Shek, L.P.-C.; Godfrey, K.M.; Gluckman, P.D.; et al. Combined Analysis of Gestational Diabetes and Maternal Weight Status from Pre-Pregnancy through Post-Delivery in Future Development of Type 2 Diabetes. Sci. Rep. 2021, 11, 5021. [Google Scholar] [CrossRef] [PubMed]
- Simmons, D.; Devlieger, R.; van Assche, A.; Jans, G.; Galjaard, S.; Corcoy, R.; Adelantado, J.M.; Dunne, F.; Desoye, G.; Harreiter, J.; et al. Effect of Physical Activity and/or Healthy Eating on GDM Risk: The DALI Lifestyle Study. J. Clin. Endocrinol. Metab. 2017, 102, 903–913. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.R.; Lipscombe, L.L.; Feig, D.S.; Lowe, J.M. Missed Opportunities for Type 2 Diabetes Testing Following Gestational Diabetes: A Population-Based Cohort Study. BJOG 2011, 118, 1484–1490. [Google Scholar] [CrossRef]
- Ministry of Health. Hướng dẫn Quốc Gia Dự Phòng Và Kiểm Soát Đái Tháo Đường Thai Kỳ (National Guidelines for the Prevention and Control of Gestational Diabetes). Available online: http://canhgiacduoc.org.vn/SiteData/3/UserFiles/HDQD%20VE%20DAI%20THAO%20DUONG%20THAI%20KY.pdf (accessed on 11 April 2023).
- Vietnam Society of Endocrinology—Diabetes. Khuyến Cáo Về Chẩn Đoán Và Điều Trị Bệnh Đái Tháo Đường (Recommendations for Diagnosis and Treatment of Diabetes). Available online: https://daithaoduong.kcb.vn/huong-dan-chan-doan-va-dieu-tri (accessed on 11 April 2023).
- American Diabetes Association. 13. Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes—2018. Diabetes Care 2017, 41, S137–S143. [Google Scholar] [CrossRef]
- American Diabetes Association. 14. Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S183–S192. [Google Scholar] [CrossRef]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful Selection of Variables in Logistic Regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef]
- Lende, M.; Rijhsinghani, A. Gestational Diabetes: Overview with Emphasis on Medical Management. Int. J. Environ. Res. Public Health 2020, 17, 9573. [Google Scholar] [CrossRef]
- Gadgil, M.D.; Ehrlich, S.F.; Zhu, Y.; Brown, S.D.; Hedderson, M.M.; Crites, Y.; Ferrara, A. Dietary Quality and Glycemic Control Among Women with Gestational Diabetes Mellitus. J. Womens Health 2019, 28, 178–184. [Google Scholar] [CrossRef]
- Charokopou, M.; Sabater, F.J.; Townsend, R.; Roudaut, M.; McEwan, P.; Verheggen, B.G. Methods Applied in Cost-Effectiveness Models for Treatment Strategies in Type 2 Diabetes Mellitus and Their Use in Health Technology Assessments: A Systematic Review of the Literature from 2008 to 2013. Curr. Med. Res. Opin. 2016, 32, 207–218. [Google Scholar] [CrossRef]
- Sami, W.; Ansari, T.; Butt, N.S.; Hamid, M.R.A. Effect of Diet on Type 2 Diabetes Mellitus: A Review. Int. J. Health Sci. 2017, 11, 65–71. [Google Scholar]
- McFarland, K.F.; Case, C.A. The Relationship of Maternal Age on Gestational Diabetes. Diabetes Care 1985, 8, 598–600. [Google Scholar] [CrossRef] [PubMed]
- Pu, J.; Zhao, B.; Wang, E.J.; Nimbal, V.; Osmundson, S.; Kunz, L.; Popat, R.A.; Chung, S.; Palaniappan, L.P. Racial/Ethnic Differences in Gestational Diabetes Prevalence and Contribution of Common Risk Factors. Paediatr. Perinat. Epidemiol. 2015, 29, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Cavazos-Rehg, P.A.; Krauss, M.J.; Spitznagel, E.L.; Bommarito, K.; Madden, T.; Olsen, M.A.; Subramaniam, H.; Peipert, J.F.; Jean Bierut, L. Maternal Age and Risk of Labor and Delivery Complications. Matern. Child Health J. 2015, 19, 1202–1211. [Google Scholar] [CrossRef]
- Zhang, C.; Rawal, S.; Chong, Y.S. Risk Factors for Gestational Diabetes: Is Prevention Possible? Diabetologia 2016, 59, 1385–1390. [Google Scholar] [CrossRef]
- Zhang, M.; Zhou, Y.; Zhong, J.; Wang, K.; Ding, Y.; Li, L. Current Guidelines on the Management of Gestational Diabetes Mellitus: A Content Analysis and Appraisal. BMC Pregnancy Childbirth 2019, 19, 200. [Google Scholar] [CrossRef]
- Goveia, P.; Cañon-Montañez, W.; Santos, D.d.P.; Lopes, G.W.; Ma, R.C.W.; Duncan, B.B.; Ziegelman, P.K.; Schmidt, M.I. Lifestyle Intervention for the Prevention of Diabetes in Women with Previous Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2018, 9, 583. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | Unsuccessful Glycemic Control Group | Successful Glycemic Control Group | Total | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Age | <35 | 16 | 43.2 | 132 | 75.0 | 148 | 69.5 | <0.0001 |
| ≥35 | 21 | 56.8 | 44 | 25.0 | 65 | 30.5 | ||
| Education level | ≤High school | 15 | 40.5 | 61 | 34.7 | 76 | 35.7 | 0.50 |
| >High school | 22 | 59.5 | 115 | 65.3 | 137 | 64.3 | ||
| Occupation | Housewife, farmer, small business | 13 | 35.1 | 48 | 27.3 | 61 | 28.6 | 0.56 |
| Worker | 10 | 27.0 | 41 | 23.3 | 51 | 23.9 | ||
| State officials | 6 | 16.2 | 24 | 13.6 | 30 | 14.1 | ||
| Private officer | 6 | 16.2 | 52 | 29.5 | 58 | 27.2 | ||
| Others | 2 | 5.4 | 11 | 6.3 | 13 | 6.1 | ||
| Chronic diseases | No | 33 | 89.2 | 161 | 91.5 | 194 | 91.1 | 0.66 |
| Yes | 4 | 10.8 | 15 | 8.5 | 19 | 8.9 | ||
| Pre-pregnancy body mass index | <25 | 28 | 75.7 | 171 | 97.2 | 199 | 93.4 | <0.0001 |
| ≥25 | 9 | 24.3 | 5 | 2.8 | 14 | 6.6 | ||
| Diabetes mellitus in family | No | 36 | 97.3 | 172 | 97.7 | 208 | 97.7 | 0.88 |
| Yes | 1 | 2.7 | 4 | 2.3 | 5 | 2.3 | ||
| History of pregnant | First | 11 | 29.7 | 72 | 40.9 | 83 | 39.0 | 0.21 |
| ≥Second | 26 | 70.3 | 104 | 59.1 | 130 | 61.0 | ||
| Pregnancy method | Nature | 26 | 70.3 | 155 | 88.1 | 181 | 85.0 | 0.01 |
| IVF | 11 | 29.7 | 21 | 11.9 | 32 | 15.0 | ||
| Number of criteria for GDM diagnosis | 1 | 14 | 37.8 | 80 | 45.5 | 94 | 44.1 | 0.02 |
| 2 | 11 | 29.7 | 73 | 41.5 | 84 | 39.4 | ||
| 3 | 12 | 32.4 | 23 | 13.1 | 35 | 16.4 | ||
| Characteristics | Univariate Analysis | Multivariate Analysis * | |||||
|---|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | ||
| Age | ≥35 | reference | reference | ||||
| <35 | 3.94 | 1.89–8.20 | <0.001 | 3.22 | 1.45–7.14 | 0.004 | |
| Education level | >High school | reference | |||||
| ≤High school | 0.78 | 0.38–1.61 | 0.50 | ||||
| Occupation | Housewife, farmer, small business | reference | reference | ||||
| Worker | 1.11 | 0.44–2.80 | 0.82 | 0.84 | 0.28–2.50 | 0.76 | |
| State officials | 1.08 | 0.37–3.20 | 0.89 | 0.87 | 0.24–3.11 | 0.83 | |
| Private officer | 2.35 | 0.83–6.67 | 0.11 | 1.40 | 0.43–4.52 | 0.58 | |
| Others | 1.49 | 0.29–7.58 | 0.63 | 1.04 | 0.17–6.24 | 0.96 | |
| Chronic diseases | Yes | ||||||
| No | 1.30 | 0.40–4.17 | 0.66 | ||||
| Pre-pregnancy body mass index | ≥25 | reference | reference | ||||
| <25 | 10.99 | 3.43–35.20 | <0.001 | 10.84 | 3.08–38.18 | <0.001 | |
| Diabetes mellitus in family | Yes | reference | |||||
| No | 1.19 | 0.13–11.00 | 0.88 | ||||
| History of pregnant | ≥Second | reference | reference | ||||
| First | 0.61 | 0.28–1.32 | 0.21 | 1.17 | 0.46–2.96 | 0.74 | |
| Pregnancy method | IVF | reference | reference | ||||
| Nature | 3.12 | 1.35–7.23 | 0.01 | 2.21 | 0.88–5.56 | 0.09 | |
| Number of criteria for GD diagnosis | 3 | reference | reference | ||||
| 2 | 3.46 | 1.35–8.89 | 0.01 | 3.78 | 1.35–10.55 | 0.01 | |
| 1 | 2.98 | 1.21–7.33 | 0.02 | 3.03 | 1.11–8.25 | 0.03 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, D.C.; Vu, T.B.; Tran, T.N.; Nguyen, T.L.; Nguyen, T.B.; Nguyen, D.C.; Hoang, V.T. The Effectiveness of Lifestyle Changes in Glycemic Control among Pregnant Women with Gestational Diabetes Mellitus. Medicina 2023, 59, 1587. https://doi.org/10.3390/medicina59091587
Le DC, Vu TB, Tran TN, Nguyen TL, Nguyen TB, Nguyen DC, Hoang VT. The Effectiveness of Lifestyle Changes in Glycemic Control among Pregnant Women with Gestational Diabetes Mellitus. Medicina. 2023; 59(9):1587. https://doi.org/10.3390/medicina59091587
Chicago/Turabian StyleLe, Duc Cuong, Thanh Binh Vu, Thi Nuong Tran, Thi Ly Nguyen, Thanh Binh Nguyen, Duy Cuong Nguyen, and Van Thuan Hoang. 2023. "The Effectiveness of Lifestyle Changes in Glycemic Control among Pregnant Women with Gestational Diabetes Mellitus" Medicina 59, no. 9: 1587. https://doi.org/10.3390/medicina59091587
APA StyleLe, D. C., Vu, T. B., Tran, T. N., Nguyen, T. L., Nguyen, T. B., Nguyen, D. C., & Hoang, V. T. (2023). The Effectiveness of Lifestyle Changes in Glycemic Control among Pregnant Women with Gestational Diabetes Mellitus. Medicina, 59(9), 1587. https://doi.org/10.3390/medicina59091587