
Intermittent Fasting and Reduction of Inflammatory Response in a Patient with Ulcerative Colitis

 , ,
, ,
Abstract
1. Introduction
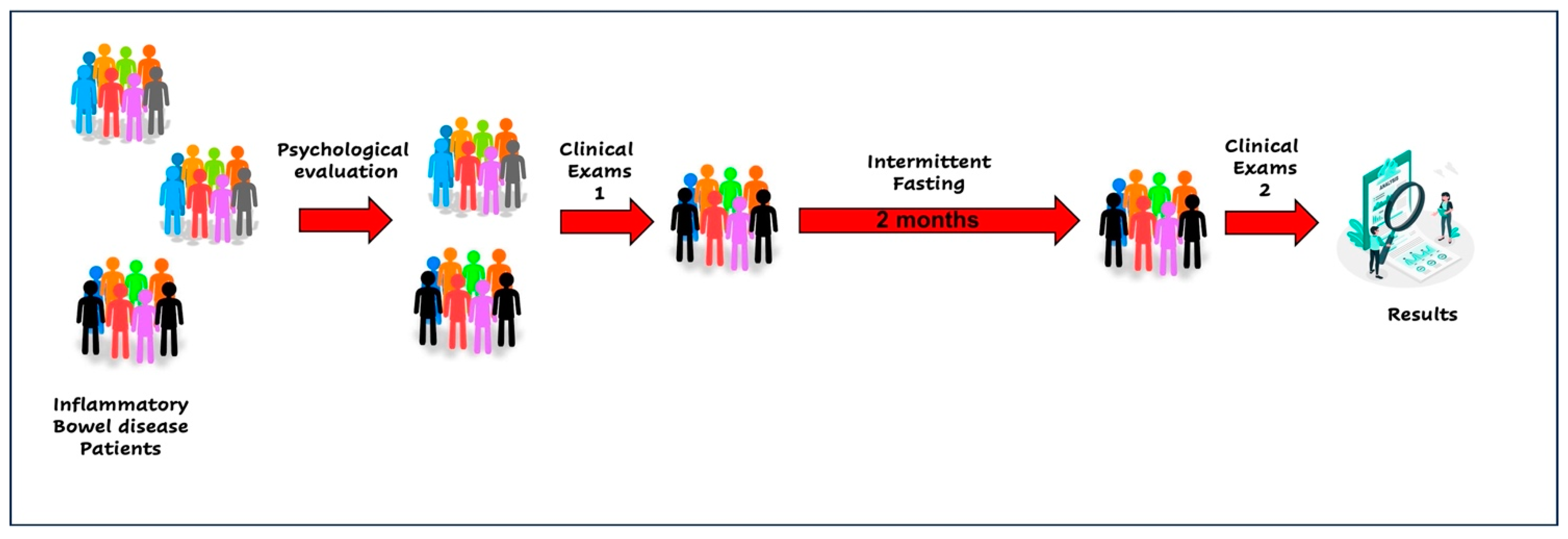
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ungaro, R.; Mehandru, S.; Allen, P.B.; Peyrin-Biroulet, L.; Colombel, J.F. Ulcerative colitis. Lancet 2017, 389, 1756–1770. [Google Scholar] [CrossRef]
- Veauthier, B.; Hornecker, J.R. Crohn’s Disease: Diagnosis and Management. Am. Fam. Physician 2018, 98, 661–669. [Google Scholar] [PubMed]
- Pagnini, C.; Pizarro, T.T.; Cominelli, F. Novel Pharmacological Therapy in Inflammatory Bowel Diseases: Beyond Anti-Tumor Necrosis Factor. Front. Pharmacol. 2019, 10, 671. [Google Scholar] [CrossRef]
- Alfredsson, J.; Wick, M.J. Mechanism of fibrosis and stricture formation in Crohn’s disease. Scand. J. Immunol. 2020, 92, e12990. [Google Scholar] [CrossRef] [PubMed]
- Dansinger, M.L.; Gleason, J.A.; Griffith, J.L.; Selker, H.P.; Schaefer, E.J. Comparison of the Atkins, Ornish, Weight Watchers, and Zone diets for weight loss and heart disease risk reduction: A randomized trial. JAMA 2005, 293, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Mandi, Y.; Stone, T.W.; Guillemin, G.J.; Vecsei, L.; Williams, R.O. Editorial: Multiple Implications of the Kynurenine Pathway in Inflammatory Diseases: Diagnostic and Therapeutic Applications. Front. Immunol. 2022, 13, 860867. [Google Scholar] [CrossRef]
- Wu, J.; Man, D.; Shi, D.; Wu, W.; Wang, S.; Wang, K.; Li, Y.; Yang, L.; Bian, X.; Wang, Q.; et al. Intermittent Fasting Alleviates Risk Markers in a Murine Model of Ulcerative Colitis by Modulating the Gut Microbiome and Metabolome. Nutrients 2022, 14, 5311. [Google Scholar] [CrossRef]
- Mushtaq, R.; Akram, A.; Mushtaq, R.; Khwaja, S.; Ahmed, S. The role of inflammatory markers following Ramadan Fasting. Pak. J. Med. Sci. 2019, 35, 77–81. [Google Scholar] [CrossRef]
- Rahbar, A.R.; Safavi, E.; Rooholamini, M.; Jaafari, F.; Darvishi, S.; Rahbar, A. Effects of intermittent fasting during ramadan on insulin-like growth factor-1, interleukin 2, and lipid profile in healthy muslims. Int. J. Prev. Med. 2019, 10, 7. [Google Scholar] [CrossRef]
- Bhutani, S.; Klempel, M.C.; Kroeger, C.M.; Trepanowski, J.F.; Varady, K.A. Alternate day fasting and endurance exercise combine to reduce body weight and favorably alter plasma lipids in obese humans. Obesity 2013, 21, 1370–1379. [Google Scholar] [CrossRef]
- Eshghinia, S.; Mohammadzadeh, F. The effects of modified alternate-day fasting diet on weight loss and CAD risk factors in overweight and obese women. J. Diabetes Metab. Disord. 2013, 12, 4. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Brandhorst, S.; Shelehchi, M.; Mirzaei, H.; Cheng, C.W.; Budniak, J.; Groshen, S.; Mack, W.J.; Guen, E.; Di Biase, S.; et al. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and cardiovascular disease. Sci. Transl. Med. 2017, 9, eaai8700. [Google Scholar] [CrossRef] [PubMed]
- McNally, A.; Hill, G.R.; Sparwasser, T.; Thomas, R.; Steptoe, R.J. CD4+CD25+ regulatory T cells control CD8+ T-cell effector differentiation by modulating IL-2 homeostasis. Proc. Natl. Acad. Sci. USA 2011, 108, 7529–7534. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Chen, L.; Bai, M.; Wang, S.; Ye, X.; Lin, Y.; Luo, X.; Li, Z.; Zhang, L.; Zhu, X.; et al. Time-restricted feeding ameliorates dextran sulfate sodium-induced colitis via reducing intestinal inflammation. Front. Nutr. 2022, 9, 1043783. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.; Tung, N.; Casanova-Acebes, M.; Chang, C.; Cantoni, C.; Zhang, D.; Wirtz, T.H.; Naik, S.; Rose, S.A.; Brocker, C.N.; et al. Dietary Intake Regulates the Circulating Inflammatory Monocyte Pool. Cell 2019, 178, 1102–1114.e17. [Google Scholar] [CrossRef] [PubMed]
- Cignarella, F.; Cantoni, C.; Ghezzi, L.; Salter, A.; Dorsett, Y.; Chen, L.; Phillips, D.; Weinstock, G.M.; Fontana, L.; Cross, A.H.; et al. Intermittent Fasting Confers Protection in CNS Autoimmunity by Altering the Gut Mi-crobiota. Cell Metab. 2018, 27, 1222–1235.e6. [Google Scholar] [CrossRef]
- Zhang, X.; Zou, Q.; Zhao, B.; Zhang, J.; Zhao, W.; Li, Y.; Liu, R.; Liu, X.; Liu, Z. Effects of alternate-day fasting, time-restricted fasting and intermittent energy restriction DSS-induced on colitis and behavioral disorders. Redox Biol. 2020, 32, 101535, Erratum in Redox Biol. 2021, 44, 101955. [Google Scholar] [CrossRef] [PubMed]
- Negm, M.; Bahaa, A.; Farrag, A.; Lithy, R.M.; Badary, H.A.; Essam, M.; Kamel, S.; Sakr, M.A.B.D.; El Aaty, W.; Shamkh, M.; et al. Effect of Ramadan intermittent fasting on inflammatory markers, disease severity, depression, and quality of life in patients with inflammatory bowel diseases: A prospective cohort study. BMC Gastroenterol. 2022, 22, 203. [Google Scholar] [CrossRef]
- Tavakkoli, H.; Haghdani, S.; Emami, M.H.; Adilipour, H.; Tavakkoli, M.; Tavakkoli, M. Ramadan fasting and inflammatory bowel disease. Indian. J. Gastroenterol. 2008, 27, 239–241. [Google Scholar]
- Aksungar, F.B.; Topkaya, A.E.; Akyildiz, M. Interleukin-6, C-reactive protein and biochemical parameters during prolonged intermittent fasting. Ann. Nutr. Metab. 2007, 51, 88–95. [Google Scholar] [CrossRef]
- Calabrese, W.R.; Rudick, M.M.; Simms, L.J.; Clark, L.A. Development and validation of Big Four personality scales for the Schedule for Nonadaptive and Adaptive Personality—Second Edition (SNAP-2). Psychol. Assess. 2012, 24, 751–763. [Google Scholar] [CrossRef]
- Olivares-Tirado, P.; Leyton, G.; Salazar, E. Personality factors and self-perceived health in Chilean elderly population. Health 2013, 5, 86–96. [Google Scholar] [CrossRef]
- Yu, Y.R.; Rodriguez, J.R. Clinical presentation of Crohn’s, ulcerative colitis, and indeterminate colitis: Symptoms, extraintestinal manifestations, and disease phenotypes. Semin. Pediatr. Surg. 2017, 26, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Fritsch, J.; Garces, L.; Quintero, M.A.; Pignac-Kobinger, J.; Santander, A.M.; Fernández, I.; Ban, Y.J.; Kwon, D.; Phillips, M.C.; Knight, K.; et al. Low-fat, high-fiber diet reduces markers of inflammation and dysbiosis and improves quality of life in patients with ulcerative colitis. Clin. Gastroenterol. Hepatol. 2021, 19, 1189–1199.e30. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.M.; Lewis, J.D.; Mayer, E.A.; Plevy, S.E.; Chuang, E.; Rappaport, S.M.; Croitoru, K.; Korzenik, J.R.; Krischer, J.; Hyams, J.S.; et al. Challenges in IBD research: Environmental triggers. Inflamm. Bowel Dis. 2019, 25, S13–S23. [Google Scholar] [CrossRef] [PubMed]
- Navabi, V.S.; Gorrepati, S.; Yadav, J.; Chintanaboina, S.; Maher, P.; Demuth, B.; Stern, A.; Stuart, A.; Tinsley, K.; Clarke, E.D.; et al. Coates, Influences and impact of anxiety and depression in the setting of inflammatory bowel disease. Inflamm. Bowel Dis. 2018, 24, 2303–2308. [Google Scholar] [CrossRef]
- Neuendorf, A.; Harding, N.; Stello, D.; Hanes, H. Wahbeh, Depression and anxiety in patients with Inflammatory Bowel Disease: A systematic review. J. Psychosom. Res. 2016, 87, 70–80. [Google Scholar] [CrossRef]
- Szebeni, G.B.; Veres, A.; Dezsõfi, K.; Rusai, A. Arató,IncreasedexpressionofToll-like receptor (TLR) 2 and TLR4 in the colonic mucosa of children with inflammatory bowel disease. Clin. Exp. Immunol. 2008, 151, 34–41. [Google Scholar] [CrossRef]
- Hu, X.; Xia, K.; Dai, M.; Duan, S. Intermittent fasting modulates the intestinal microbiota and improves obesity and host energy metabolism. Npj Biofilms Microbiomes 2023, 9, 19. [Google Scholar] [CrossRef]
- Bhandage, A.K.; Jin, Z.; Korol, S.V.; Shen, Q.; Pei, Y.; Deng, Q.; Espes, D.; Carlsson, P.O.; Kamali-Moghaddam, M.; Birnir, B. GABA Regulates Release of Inflammatory Cytokines from Peripheral Blood Mononuclear Cells and CD4+ T Cells and Is Immunosuppressive in Type 1 Diabetes. EBioMedicine 2018, 30, 283–294. [Google Scholar] [CrossRef]
- Khan, M.N.; Khan, S.I.; Rana, M.I.; Ayyaz, A.; Khan, M.Y.; Imran, M. Intermittent fasting positively modulates human gut microbial diversity and ameliorates blood lipid profile. Front. Microbiol. 2022, 13, 922727. [Google Scholar] [CrossRef]
- de Souza, C.H.B.; Gioielli, L.A.; Saad, S.M.I. Inulin increases Bifidobacterium animalis Bb-12 in vitro gastrointestinal resistance in margarine. LWT Food Sci. Technol. 2017, 79, 205–212. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, K.E.; Kim, J.K.; Kim, D.H. Suppression of gut dysbiosis by Bifidobacterium longum alleviates cognitive decline in 5XFAD transgenic and aged mice. Sci. Rep. 2019, 9, 11814. [Google Scholar] [CrossRef]
- Flint, H.J.; Duncan, S.H.; Scott, K.P.; Louis, P. Links between diet, gut microbiota composition and gut metabolism. Proc. Nutr. Soc. 2015, 74, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Arpaia, N.; Campbell, C.; Fan, X.; Dikiy, S.; van der Veeken, J.; deRoos, P.; Alexander, Y.R. Metabolites produced by commensal bacteria promote peripheral regulatory T-cell generation. Nature 2013, 504, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Faris, M.A.; Kacimi, S.; Al-Kurd, R.A.; Yasser, K.B. Intermittent fasting during Ramadan attenuates proinflammatory cytokines and immune cells in healthy subjects. Nutr. Res. 2012, 32, 947–955. [Google Scholar] [CrossRef] [PubMed]
- El Mountassir, M.; Benelbarhdadi, I.; Borahma, M.; Ajana, F. Impact of Ramadan on Crohn’s disease. Gastroenterol. Hepatol. Endosc. 2021, 6, 1000217. [Google Scholar] [CrossRef]
- Unalacak, M.; Kara, I.H.; Baltaci, D.; Erdem, O.; Bucaktepe, P.G. Effects of Ramadan fasting on biochemical and hematological parameters and cytokines in healthy and obese individuals. Metab. Syndr. Relat. Disord. 2011, 9, 157–161. [Google Scholar] [CrossRef]
- Widhani, A.; Yunihastuti, E.; Setiati, S.; Witjaksono, F.; Karjadi, T.H. Ramadan fasting reduces high-sensitivity C-reactive protein among HIV-infected patients receiving antiretroviral therapy. Front. Nutr. 2023, 9, 964797. [Google Scholar] [CrossRef]


{kind=link}
| Blood Count | Pre-T | Post-T | |
| Hematocrit | 40.4 | 42.1 | % |
| Hemoglobin | 13.8 | 13.8 | gr/dL |
| Total Leukocytes | 7.4 | 8.6 | 103/mL |
| Platelets | 348 | 359 | 103/mL |
| HSV | 11 | 10 | mm/Hr |
| Coagulation | Pre-T | Post-T | |
| INR | 1 | 1 | |
| Lipidic profile | Pre-T | Post-T | |
| Total Cholesterol | 174 | 169 | mg/dL |
| HDL | 61 | 61 | mg/dL |
| LDL | 90 | 87 | mg/dL |
| TG | 112 | 103 | mg/dL |
| Inflammation | Pre-T | Post-T | |
| Calprotectin | 139 | 51 | mg/Kg |
| CRP | 3.64 | 1.57 | mg/L |
| Glucose | Pre-T | Post-T | |
| Basal | 90 | 95 | mg/dL |
| OGTT | 135 | 119 | mg/dL |
| Liver profile | Pre-T | Post-T | |
| GGT | 10 | 13 | U/L |
| AP | 96 | 91 | U/L |
| GOT/AST | 18 | 17 | U/L |
| GPT/ALT | 19 | 16 | U/L |
| Bilirubin | 0.42 | 0.43 | mg/dL |
| Thyroid | Pre-T | Post-T | |
| TSH | 3.7 | 4.53 | uUI/mL |
| Free T4 | 1.01 | 1.05 | ng/dL |
| Nutritional Recommendations for Intermittent Fasting 10/14 | |
| Feeding time 10 h | |
| intermittent Fasting 14 h | |
| Fasting | |
| During fasting you can drink water and infusions such as tea or chamomile sugarless/sweetener less | |
| During fasting you can´t eat neither drink liquid with sugar or sweetener, coffee, natural juice, or powder juice | |
| Feeding time | |
| Sources | Foods |
| Vit E | Nuts such as almonds, hazelnuts, peanuts Sunflower oil, corn, Spinach, broccoli, kiwi, tomato, mango. |
| Vit C | Paprika Orange Grapefruit, Kiwi, Broccoli Strawberries, Tomato, Sprouts (cabbage, cauliflower, Brussels). |
| Vit D | Cod oil, Egg, Liver, Salmon, tuna, Mushroom (exposed to UV light), Vegetable enriched drinks |
| Vit B-complex | Liver, Spinach, Asparagus, Cabbages, Legumes, Avocado, Chicken, Salmon, Tuna Clams, Trout, Turkey, Beef, fortified vegetable drinks. |
| Antiox | Grape, Tomato, Cocoa, Blueberries, Strawberries, Green tea, Carrot, Maqui, Calafate, Murtilla. |
| Iron | Fortified cereals, Legumes, Seafood, Dark green vegetables, Fortified vegetable drinks, Food of animal origin. |
| Calcium | Dairy and derived products, these products can be whole, semi-skimmed or skimmed according to tolerance. It can also be lactose-free according to tolerance. Cereals like amaranth, Legumes such as beans, chickpeas, tofu, Nuts such as almonds and sesame seeds, Calcium-fortified vegetable drinks. |
| Magnesium | Pumpkin seed, Quinoa, Spinach, Walnuts, almonds, pine nuts, Beans. |
| Natural anti-inflammatories | A good consumption of fruits and vegetables is recommended, avoiding highly processed foods and refined carbohydrates, cakes, cookies, etc. Foods with omega 3 content: Fatty fish such as salmon, tuna, horse mackerel, etc, walnuts, flaxseed, flaxseed oil, olive oil, pumpkin seeds. Promote the consumption of whole foods such as rice, whole wheat bread and noodles, amaranth, quinoa.Spices such as turmeric, ginger, rosemary (according to tolerance). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roco-Videla, Á.; Villota-Arcos, C.; Pino-Astorga, C.; Mendoza-Puga, D.; Bittner-Ortega, M.; Corbeaux-Ascui, T. Intermittent Fasting and Reduction of Inflammatory Response in a Patient with Ulcerative Colitis. Medicina 2023, 59, 1453. https://doi.org/10.3390/medicina59081453
Roco-Videla Á, Villota-Arcos C, Pino-Astorga C, Mendoza-Puga D, Bittner-Ortega M, Corbeaux-Ascui T. Intermittent Fasting and Reduction of Inflammatory Response in a Patient with Ulcerative Colitis. Medicina. 2023; 59(8):1453. https://doi.org/10.3390/medicina59081453
Chicago/Turabian StyleRoco-Videla, Ángel, Claudio Villota-Arcos, Carolina Pino-Astorga, Daniela Mendoza-Puga, Mauricio Bittner-Ortega, and Tatiana Corbeaux-Ascui. 2023. "Intermittent Fasting and Reduction of Inflammatory Response in a Patient with Ulcerative Colitis" Medicina 59, no. 8: 1453. https://doi.org/10.3390/medicina59081453
APA StyleRoco-Videla, Á., Villota-Arcos, C., Pino-Astorga, C., Mendoza-Puga, D., Bittner-Ortega, M., & Corbeaux-Ascui, T. (2023). Intermittent Fasting and Reduction of Inflammatory Response in a Patient with Ulcerative Colitis. Medicina, 59(8), 1453. https://doi.org/10.3390/medicina59081453