
Incidence of Lower Extremity Amputation in Romania: A Nationwide 5-Year Cohort Study, 2015–2019


 ,
,
Abstract
1. Introduction
2. Objectives
3. Materials and Methods
3.1. Inclusion and Exclusion Criteria
3.1.1. Definitions
3.1.2. Statistical Analysis
4. Results
4.1. General Characteristics
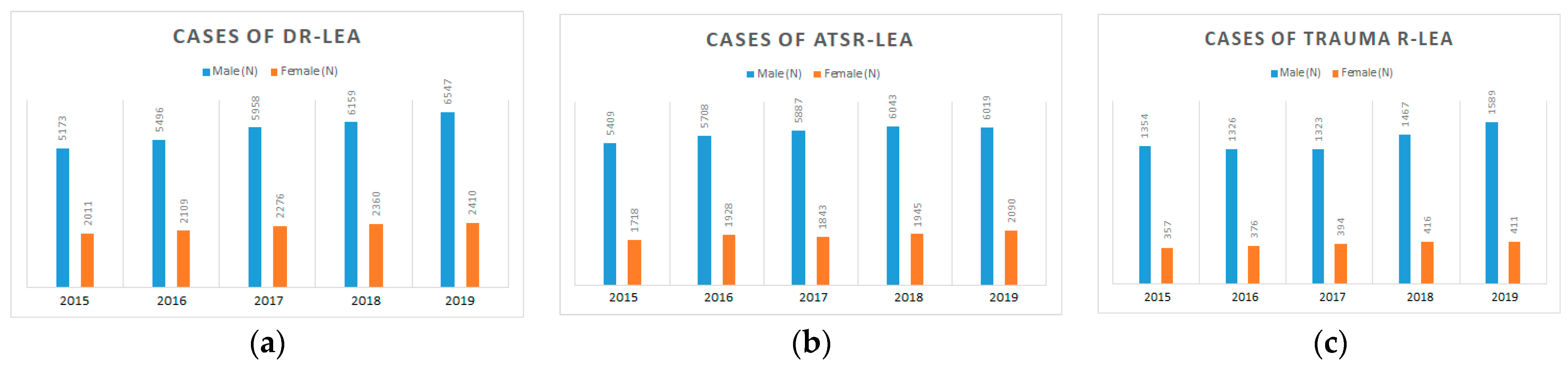
4.2. LEAs and Sex Distribution
4.3. LEAs and Age Distribution
4.4. Diabetes-Related LEAs
4.5. Minor Amputations in Patients with Diabetes
4.6. Major Amputations in Patients with Diabetes
4.7. ATS-Related LEAs
4.8. Trauma-Related LEAs
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.A.; Williams, L.J.; Mensah, G.A.; et al. Comparison of Global Estimates of Prevalence and Risk Factors for Peripheral Artery Disease in 2000 and 2010: A Systematic Review and Analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef] [PubMed]
- Frykberg, R.G.; Zgonis, T.; Armstrong, D.G.; Driver, V.R.; Giurini, J.M.; Kravitz, S.R.; Landsman, A.S.; Lavery, L.A.; Moore, J.C.; Schuberth, J.M.; et al. Diabetic Foot Disorders. A Clinical Practice Guideline (2006 Revision). J. Foot Ankle Surg. 2006, 45 (Suppl. S5), S1–S66. [Google Scholar] [CrossRef] [PubMed]
- IDF Diabetes Atlas 8th Edition—Feel4Diabetes. Available online: https://feel4diabetes-study.eu/idf-diabetes-atlas-8th-edition/ (accessed on 16 March 2022).
- IDF Diabetes Atlas 2021|IDF Diabetes Atlas. Available online: https://diabetesatlas.org/atlas/tenth-edition/ (accessed on 16 March 2022).
- Moxey, P.W.; Gogalniceanu, P.; Hinchliffe, R.J.; Loftus, I.M.; Jones, K.J.; Thompson, M.M.; Holt, P.J. Lower Extremity Amputations—A Review of Global Variability in Incidence. Diabet. Med. 2011, 28, 1144–1153. [Google Scholar] [CrossRef]
- Gakidou, E.; Afshin, A.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Aboyans, V.; et al. Global, Regional, and National Comparative Risk Assessment of 84 Behavioural, Environmental and Occupational, and Metabolic Risks or Clusters of Risks, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef]
- Tentolouris, N.; Al-Sabbagh, S.; Walker, M.G.; Boulton, A.J.M.; Jude, E.B. Mortality in Diabetic and Nondiabetic Patients after Amputations Performed from 1990 to 1995: A 5-Year Follow-up Study. Diabetes Care 2004, 27, 1598–1604. [Google Scholar] [CrossRef]
- Liu, R.; Petersen, B.J.; Rothenberg, G.M.; Armstrong, D.G. Lower Extremity Reamputation in People with Diabetes: A Systematic Review and Meta-Analysis. BMJ Open Diabetes Res. Care 2021, 9, e002325. [Google Scholar] [CrossRef] [PubMed]
- Kanade, R.; Van Deursen, R.; Burton, J.; Davies, V.; Harding, K.; Price, P. Re-Amputation Occurrence in the Diabetic Population in South Wales, UK. Int. Wound J. 2007, 4, 344–352. [Google Scholar] [CrossRef]
- Jude, E.B.; Oyibo, S.O.; Chalmers, N.; Boulton, A.J.M. Peripheral Arterial Disease in Diabetic and Nondiabetic Patients: A Comparison of Severity and Outcome. Diabetes Care 2001, 24, 1433–1437. [Google Scholar] [CrossRef]
- Newhall, K.; Spangler, E.; Dzebisashvili, N.; Goodman, D.C.; Goodney, P. Amputation Rates for Patients with Diabetes and Peripheral Arterial Disease: The Effects of Race and Region. Ann. Vasc. Surg. 2016, 30, 292–298.e1. [Google Scholar] [CrossRef]
- Members. Available online: https://www.idf.org/our-network/regions-members/europe/members/154-romania.html (accessed on 2 July 2020).
- Mota, M.; Popa, S.G.; Mota, E.; Mitrea, A.; Catrinoiu, D.; Cheta, D.M.; Guja, C.; Hancu, N.; Ionescu-Tirgoviste, C.; Lichiardopol, R.; et al. Prevalence of Diabetes Mellitus and Prediabetes in the Adult Romanian Population: PREDATORR Study. J. Diabetes 2016, 8, 336–344. [Google Scholar] [CrossRef]
- Veresiu, I.A.; Iancu, S.S.; Bondor, C. Trends in Diabetes-Related Lower Extremities Amputations in Romania-A Five Year Nationwide Evaluation. Diabetes Res. Clin. Pract. 2015, 109, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Vamos, E.P.; Bottle, A.; Edmonds, M.E.; Valabhji, J.; Majeed, A.; Millett, C. Changes in the Incidence of Lower Extremity Amputations in Individuals with and without Diabetes in England between 2004 and 2008. Diabetes Care 2010, 33, 2592–2597. [Google Scholar] [CrossRef] [PubMed]
- Rezultate 2011—Institutul Național de Statistică. Available online: https://www.recensamantromania.ro/rpl-2011/rezultate-2011/ (accessed on 17 January 2022).
- Populaţia Rezidentă * La 1 Ianuarie 2020. 2021, No. 222, 2020–2021. Available online: https://insse.ro/cms/ro/content/populaţia-rezidentă-la-1-ianuarie-2021-şi-migraţia-internaţională-în-anul-2020 (accessed on 17 January 2022).
- Behrendt, C.A.; Sigvant, B.; Szeberin, Z.; Beiles, B.; Eldrup, N.; Thomson, I.A.; Venermo, M.; Altreuther, M.; Menyhei, G.; Nordanstig, J.; et al. International Variations in Amputation Practice: A VASCUNET Report. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 391–399. [Google Scholar] [CrossRef]
- Kolossváry, E.; Ferenci, T.; Kováts, T.; Kovács, L.; Járai, Z.; Menyhei, G.; Farkas, K. Trends in Major Lower Limb Amputation Related to Peripheral Arterial Disease in Hungary: A Nationwide Study (2004–2012). Eur. J. Vasc. Endovasc. Surg. 2015, 50, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Walter, N.; Alt, V.; Rupp, M. Lower Limb Amputation Rates in Germany. Medicina 2022, 58, 101. [Google Scholar] [CrossRef]
- Greenfield, S.; Nicolucci, A.; Mattke, S. Selecting Indicators for the Quality of Diabetes Care at the Health Systems Level in OECD Countries; Organisation for Economic Co-operation and Development: Paris, France, 2004. [Google Scholar]
- Rasmussen, B.S.B.; Yderstraede, K.B.; Carstensen, B.; Skov, O.; Beck-Nielsen, H. Substantial Reduction in the Number of Amputations among Patients with Diabetes: A Cohort Study over 16 Years. Diabetologia 2016, 59, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Kreutzburg, T.; Peters, F.; Rieß, H.C.; Hischke, S.; Marschall, U.; Kriston, L.; L’Hoest, H.; Sedrakyan, A.; Debus, E.S.; Behrendt, C.A. Editor’s Choice—Comorbidity Patterns Among Patients with Peripheral Arterial Occlusive Disease in Germany: A Trend Analysis of Health Insurance Claims Data. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 59–66. [Google Scholar] [CrossRef]
- Rodríguez Pérez, M.D.C.; Chines, C.; Pedrero García, A.J.; Sousa, D.; Cuevas Fernández, F.J.; Marcelino-Rodríguez, I.; Domínguez Coello, S.; Cabrera De León, A. Major Amputations in Type 2 Diabetes between 2001 and 2015 in Spain: Regional Differences. BMC Public Health 2020, 20, 54. [Google Scholar] [CrossRef]
- Icks, A.; Haastert, B.; Trautner, C.; Giani, G.; Glaeske, G.; Hoffmann, F. Incidence of Lower-Limb Amputations in the Diabetic Compared to the Non-Diabetic Population. Findings from Nationwide Insurance Data, Germany, 2005–2007. Exp. Clin. Endocrinol. Diabetes 2009, 117, 500–504. [Google Scholar] [CrossRef]
- Kröger, K.; Berg, C.; Santosa, F.; Malyar, N.; Reinecke, H. Lower Limb Amputation in Germany—An Analysis of Data from the German Federal Statistical Office between 2005 and 2014. Dtsch. Arztebl. Int. 2017, 114, 130–136. [Google Scholar] [CrossRef]
- Lopez-De-andres, A.; Jimenez-Garcia, R.; Hernandez-Barrera, V.; de Miguel-Diez, J.; de Miguel-Yanes, J.M.; Omaña-Palanco, R.; Carabantes-Alarcon, D. Trends of Non-Traumatic Lower-Extremity Amputation and Type 2 Diabetes: Spain, 2001–2019. J. Clin. Med. 2022, 11, 1246. [Google Scholar] [CrossRef] [PubMed]
- Holman, N.; Young, R.J.; Jeffcoate, W.J. Variation in the Recorded Incidence of Amputation of the Lower Limb in England. Diabetologia 2012, 55, 1919–1925. [Google Scholar] [CrossRef] [PubMed]
- Buckley, C.M.; O’Farrell, A.; Canavan, R.J.; Lynch, A.D.; de la Harpe, D.V.; Bradley, C.P.; Perry, I.J. Trends in the Incidence of Lower Extremity Amputations in People with and without Diabetes over a Five-Year Period in the Republic of Ireland. PLoS ONE 2012, 7, e41492. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, M.E.; Almdal, T.P.; Færch, K. Reduced Incidence of Lower-Extremity Amputations in a Danish Diabetes Population from 2000 to 2011. Diabetic. Med. 2014, 31, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.S.; Petersen, J.; Kirketerp-Møller, K.; Poulsen, I.; Andersen, O. Progression of Disease Preceding Lower Extremity Amputation in Denmark: A Longitudinal Registry Study of Diagnoses, Use of Medication and Healthcare Services 14 Years Prior to Amputation. BMJ Open 2017, 7, 16030. [Google Scholar] [CrossRef]
- Jonasson, J.M.; Ye, W.; Sparén, P.; Apelqvist, J.; Nyrén, O.; Brismar, K. Risks of Nontraumatic Lower-Extremity Amputations in Patients with Type 1 Diabetes: A Population-Based Cohort Study in Sweden. Diabetes Care 2008, 31, 1536–1540. [Google Scholar] [CrossRef]
- Witsø, E.; Lium, A.; Lydersen, S. Lower Limb Amputations in Trondheim, Norway: A 40% Reduction in Diabetic Major Lower-Limb Amputations from 1996 to 2006. Acta Orthop. 2010, 81, 737. [Google Scholar] [CrossRef]
- Geiss, L.S.; Li, Y.; Hora, I.; Albright, A.; Rolka, D.; Gregg, E.W. Resurgence of Diabetes-Related Nontraumatic Lower-Extremity Amputation in the Young and Middle-Aged Adult U.S. Population. Diabetes Care 2019, 42, 50–54. [Google Scholar] [CrossRef]
- Huang, E.S.; Laiteerapong, N.; Liu, J.Y.; John, P.M.; Moffet, H.H.; Karter, A.J. Rates of Complications and Mortality in Older Diabetes Patients: The Diabetes and Aging Study. JAMA Int. Med. 2014, 174, 251. [Google Scholar] [CrossRef]
- Harding, J.L.; Andes, L.J.; Rolka, D.B.; Imperatore, G.; Gregg, E.W.; Li, Y.; Albright, A. National and State-Level Trends in Nontraumatic Lower-Extremity Amputation Among U.S. Medicare Beneficiaries With Diabetes, 2000–2017. Diabetes Care 2020, 43, 2453–2459. [Google Scholar] [CrossRef]
- Déruaz-Luyet, A.; Raabe, C.; Garry, E.M.; Brodovicz, K.G.; Lavery, L.A. Incidence of Lower Extremity Amputations among Patients with Type 1 and Type 2 Diabetes in the United States from 2010 to 2014. Diabetes Obes. Metab. 2020, 22, 1132. [Google Scholar] [CrossRef]
- Imam, B.; Miller, W.C.; Finlayson, H.C.; Eng, J.J.; Jarus, T. Incidence of Lower Limb Amputation in Canada. Can. J. Public. Health 2017, 108, e374–e380. [Google Scholar] [CrossRef] [PubMed]
- Pran, L.; Harnanan, D.; Baijoo, S.; Short, A.; Cave, C.; Maharaj, R.; Cawich, S.O.; Naraynsingh, V. Major Lower Limb Amputations: Recognizing Pitfalls. Cureus 2021, 13, e16972. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.E.; Kenealy, T.; Garrett, M.; Bramley, D.; Drury, P.L.; Elley, C.R. Ethnicity and Risk of Lower Limb Amputation in People with Type 2 Diabetes: A Prospective Cohort Study. Diabet. Med. 2016, 33, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Dillingham, T.R.; Pezzin, L.E.; MacKenzie, E.J. Racial Differences in the Incidence of Limb Loss Secondary to Peripheral Vascular Disease: A Population-Based Study. Arch. Phys. Med. Rehabil. 2002, 83, 1252–1257. [Google Scholar] [CrossRef]
- Ikonen, T.S.; Sund, R.; Venermo, M.; Winell, K. Fewer Major Amputations Among Individuals With Diabetes in Finland in 1997–2007: A Population-Based Study. Diabetes Care 2010, 33, 2598. [Google Scholar] [CrossRef]
- Narres, M.; Kvitkina, T.; Claessen, H.; Droste, S.; Schuster, B.; Morbach, S.; Rümenapf, G.; Van Acker, K.; Icks, A. Incidence of Lower Extremity Amputations in the Diabetic Compared with the Non-Diabetic Population: A Systematic Review. PLoS ONE 2017, 12, e0182081. [Google Scholar] [CrossRef]
- van Houtum, W.H.; Lavery, L.A. Regional Variation in the Incidence of Diabetes-Related Amputations in The Netherlands. Diabetes Res. Clin. Pract. 1996, 31, 125–132. [Google Scholar] [CrossRef]
- ANALIZA DE SITUAŢIE. Available online: https://insp.gov.ro/download/cnepss/stare-de-sanatate/determinantii_starii_de_sanatate/tutunul/Analiza-de-situatie-ZNT-2019.pdf (accessed on 17 January 2022).
- Margolis, D.J.; Allen-Taylor, L.; Hoffstad, O.; Berlin, J.A. Diabetic Neuropathic Foot Ulcers and Amputation. Wound Repair. Regen. 2005, 13, 230–236. [Google Scholar] [CrossRef]
- Boulton, A.J.M. The Pathway to Foot Ulceration in Diabetes. Med. Clin. N. Am. 2013, 97, 775–790. [Google Scholar] [CrossRef]
- Apelqvist, J.; Bakker, K.; van Houtum, W.H.; Schaper, N.C. Practical Guidelines on the Management and Prevention of the Diabetic Foot: Based upon the International Consensus on the Diabetic Foot (2007) Prepared by the International Working Group on the Diabetic Foot. Diabetes Metab. Res. Rev. 2008, 24 (Suppl. S1), S181–S187. [Google Scholar] [CrossRef] [PubMed]
- Trautner, C.; Haastert, B.; Mauckner, P.; Gätcke, L.M.; Giani, G. Reduced Incidence of Lower-Limb Amputations in the Diabetic Population of a German City, 1990–2005: Results of the Leverkusen Amputation Reduction Study (LARS). Diabetes Care 2007, 30, 2633–2637. [Google Scholar] [CrossRef] [PubMed]
- Schaper, N.C.; Andros, G.; Apelqvist, J.; Bakker, K.; Lammer, J.; Lepantalo, M.; Mills, J.L.; Reekers, J.; Shearman, C.P.; Zierler, R.E.; et al. Diagnosis and Treatment of Peripheral Arterial Disease in Diabetic Patients with a Foot Ulcer. A Progress Report of the International Working Group on the Diabetic Foot. Diabetes Metab. Res. Rev. 2012, 28 (Suppl. S1), 218–224. [Google Scholar] [CrossRef] [PubMed]
- Hinchliffe, R.J.; Andros, G.; Apelqvist, J.; Bakker, K.; Fiedrichs, S.; Lammer, J.; Lepantalo, M.; Mills, J.L.; Reekers, J.; Shearman, C.P.; et al. A Systematic Review of the Effectiveness of Revascularization of the Ulcerated Foot in Patients with Diabetes and Peripheral Arterial Disease. Diabetes Metab. Res. Rev. 2012, 28 (Suppl. S1), 179–217. [Google Scholar] [CrossRef]
- Ahmad, N.; Thomas, G.N.; Gill, P.; Chan, C.; Torella, F. Lower Limb Amputation in England: Prevalence, Regional Variation and Relationship with Revascularisation, Deprivation and Risk Factors. A Retrospective Review of Hospital Data. J. R. Soc. Med. 2014, 107, 483–489. [Google Scholar] [CrossRef]
- Jeffcoate, W.J.; Van Houtum, W.H. Amputation as a Marker of the Quality of Foot Care in Diabetes. Diabetologia 2004, 47, 2051–2058. [Google Scholar] [CrossRef]
- National Diabetes Audit—2013–2014 and 2014–2015: Report 1, Care Processes and Treatment Targets—NHS Digital. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/national-diabetes-audit/national-diabetes-audit-2013-2014-and-2014-2015-report-1-care-processes-and-treatment-targets (accessed on 18 April 2022).


{kind=link}
| Years | 2015 | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|---|
| General population | 19,875,542 | 19,760,585 | 19,643,949 | 19,533,481 | 19,425,873 |
| Diabetic Population | 999,192 | 186,9136 | 1,785,300 | 1,161,330 | 1,704,560 |
| IDF Diabetes | 1,278,300 | 1,278,300 | 1,278,300 | 1,278,300 | 1,278,300 |
| 2015 | 2016 | 2017 | 2018 | 2019 | Total | |
|---|---|---|---|---|---|---|
| Number of cases with LEA (N) | 16,022 | 16,943 | 17,681 | 18,390 | 19,066 | 88,102 |
| Men N (%) | 11,936 (74.5%) | 12,530 (73.95%) | 13,168 (74.48%) | 13,669 (74.33%) | 14,155 (74.24%) | 65,458 (74.30%) |
| Underlying disease N (%) | ||||||
| DM | 7184 (44.84%) | 7605 (44.89%) | 8234 (46.57%) | 8519 (46.32%) | 8957 (46.98%) | 40,499 (45.97%) |
| ATS | 7127 (44.48%) | 7636 (45.07%) | 7730 (43.72%) | 7988 (43.44%) | 8109 (42.53%) | 38,590 (43.80%) |
| Trauma | 1711 (10.68%) | 1702 (10.05%) | 1717 (9.71%) | 1883 (10.24%) | 2000 (10.49%) | 9013 (10.23%) |
| Incidence of LEA per 105 population | 80.61 | 85.74 | 90.01 | 94.15 | 98.15 | 89.68 |
| DM | 36.14 | 38.49 | 41.92 | 43.61 | 46.11 | 41.22 |
| ATS | 35.85 | 38.64 | 39.35 | 40.89 | 41.74 | 39.28 |
| Trauma | 8.60 | 8.61 | 8.74 | 9.63 | 10.29 | 9.18 |
| Amputation type N (%) | ||||||
| Minor | 9573 (59.75%) | 10,254 (60.52%) | 10,911 (61.71%) | 11,281 (61.34%) | 12,010 (62.99%) | 54,029 (61.33%) |
| Major | 6449 (40.25%) | 6689 (39.48%) | 6770 (38.29%) | 7109 (38.66%) | 7056 (37.01%) | 34,073 (38.67%) |
| Minor-to-major ratio | 1.48 | 1.53 | 1.61 | 1.59 | 1.70 | 1.59 |
| Amputation type among DR-LEA N (%) | ||||||
| Minor | 5024 (69.93%) | 5374 (70.66%) | 5865 (71.23%) | 6056 (71.09%) | 6488 (72.43%) | 28,807 (71.13%) |
| Major | 2160 (30.07%) | 2231 (29.34%) | 2369 (28.77%) | 2463 (28.91%) | 2469 (27.57%) | 11,692 (28.87%) |
| Incidence of DR-LEA per 105 Population with DM | 718.98 | 406.87 | 461.21 | 733.56 | 525.47 | 569.22 |
| Minor | 502.81 | 287.51 | 328.52 | 521.47 | 380.63 | 404.19 |
| Major | 216.17 | 119.36 | 132.69 | 212.08 | 144.85 | 165.03 |
| Incidence of DR-LEA per 105 general population | ||||||
| Minor | 25.28 | 27.20 | 29.86 | 31.00 | 33.40 | 29.32 |
| Major | 10.87 | 11.29 | 12.06 | 12.61 | 12.71 | 11.90 |
| Incidence of ATSR-LEA per 105 general population | ||||||
| Minor | 18.33 | 20.46 | 21.30 | 21.76 | 22.96 | 20.95 |
| Major | 17.52 | 18.18 | 18.05 | 19.14 | 18.78 | 18.33 |
| Incidence of TR-LEA per 105 general population | ||||||
| Minor | 4.55 | 4.24 | 4.39 | 4.99 | 5.47 | 4.72 |
| Major | 4.06 | 4.38 | 4.35 | 4.65 | 4.83 | 4.45 |
| Male/female ratio among DR-LEA | 2.57 | 2.61 | 2.62 | 2.61 | 2.72 | 2.63 |
| Minor | 2.97 | 2.90 | 2.83 | 2.88 | 2.95 | 2.90 |
| Major | 1.90 | 2.06 | 2.18 | 2.08 | 2.21 | 2.09 |
| Male/female ratio among ATSR-LEA | 3.15 | 2.96 | 3.19 | 3.11 | 2.88 | 3.05 |
| Minor | 3.45 | 3.16 | 3.39 | 3.29 | 3.03 | 3.25 |
| Major | 2.87 | 2.76 | 2.98 | 2.91 | 2.72 | 2.85 |
| Male/female ratio among TR-LEA | 3.79 | 3.53 | 3.36 | 3.53 | 3.87 | 3.61 |
| Minor | 3.46 | 3.41 | 3.38 | 3.69 | 3.60 | 3.51 |
| Major | 4.23 | 3.65 | 3.34 | 3.37 | 4.21 | 3.73 |
| Number of Nontraumatic-LEA N | 14,311 | 15,241 | 15,964 | 16,507 | 17,066 | 79,089 |
| Minor | 8668 | 9417 | 10,049 | 10,306 | 10,948 | 49,388 |
| Major | 5643 | 5824 | 5915 | 6201 | 6118 | 29,701 |
| Incidence of Nontraumatic-LEA per 105 General population | 72.00 | 77.13 | 81.27 | 84.51 | 87.85 | 80.51 |
| Minor | 43.61 | 47.66 | 51.16 | 52.76 | 56.36 | 50.27 |
| Major | 28.39 | 29.47 | 30.11 | 31.75 | 31.49 | 30.23 |
| 2015 | 2016 | 2017 | 2018 | 2019 | Total | |
|---|---|---|---|---|---|---|
| Type 1 DM | 1307 (18.19%) | 1203 (15.82%) | 1102 (13.38%) | 1021 (11.99%) | 973 (10.86%) | 5606 (13.84%) |
| Minor | 949 | 871 | 814 | 787 | 746 | 4167 |
| Major | 358 | 332 | 288 | 234 | 227 | 1439 |
| Type 2 DM | 5638 (78.48%) | 6164 (81.05%) | 6883 (83.59%) | 7267 (85.30%) | 7725 (86.25%) | 33,677 (83.16%) |
| Minor | 3903 | 4341 | 4879 | 5104 | 5552 | 23779 |
| Major | 1735 | 1823 | 2004 | 2163 | 2173 | 9898 |
| Other DM | 239 (3.33%) | 238 (3.13%) | 249 (3.02%) | 231 (2.71%) | 259 (2.89%) | 1216 (3%) |
| Minor | 172 | 162 | 172 | 165 | 190 | 861 |
| Major | 67 | 76 | 77 | 66 | 69 | 355 |
| Incidence of DR-LEAs per DM population | ||||||
| Type 1 DM | 6.58 | 6.09 | 5.61 | 5.23 | 5.01 | 5.71 |
| Minor | 4.77 | 4.41 | 4.14 | 4.03 | 3.84 | 4.24 |
| Major | 1.80 | 1.68 | 1.47 | 1.20 | 1.17 | 1.46 |
| Type 2 DM | 28.37 | 31.19 | 35.04 | 37.20 | 39.77 | 34.28 |
| Minor | 19.64 | 21.97 | 24.84 | 26.13 | 28.58 | 24.23 |
| Major | 8.73 | 9.23 | 10.20 | 11.07 | 11.19 | 10.08 |
| Other DM | 1.2 | 1.2 | 1.27 | 1.18 | 1.33 | 1.24 |
| Minor | 0.87 | 0.82 | 0.88 | 0.84 | 0.98 | 0.88 |
| Major | 0.34 | 0.38 | 0.39 | 0.34 | 0.36 | 0.36 |
| Minor/major ratio among DR-LEAs | ||||||
| Total | 2.33 | 2.41 | 2.48 | 2.46 | 2.63 | 2.46 |
| Female | 1.70 | 1.89 | 2.06 | 1.95 | 2.14 | 1.95 |
| Male | 2.65 | 2.66 | 2.67 | 2.70 | 2.85 | 2.71 |
| Type 1 DM | 2.65 | 2.62 | 2.83 | 3.36 | 3.29 | 2.90 |
| Type 2 DM | 2.25 | 2.38 | 2.43 | 2.36 | 2.55 | 2.40 |
| Other types of DM | 2.57 | 2.13 | 2.23 | 2.50 | 2.75 | 2.43 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rusu, E.; Coman, H.; Coșoreanu, A.; Militaru, A.-M.; Popescu-Vâlceanu, H.-C.; Teodoru, I.; Mihai, D.-A.; Elian, V.; Gavan, N.A.; Radulian, G. Incidence of Lower Extremity Amputation in Romania: A Nationwide 5-Year Cohort Study, 2015–2019. Medicina 2023, 59, 1199. https://doi.org/10.3390/medicina59071199
Rusu E, Coman H, Coșoreanu A, Militaru A-M, Popescu-Vâlceanu H-C, Teodoru I, Mihai D-A, Elian V, Gavan NA, Radulian G. Incidence of Lower Extremity Amputation in Romania: A Nationwide 5-Year Cohort Study, 2015–2019. Medicina. 2023; 59(7):1199. https://doi.org/10.3390/medicina59071199
Chicago/Turabian StyleRusu, Emilia, Horațiu Coman, Andrada Coșoreanu, Ana-Maria Militaru, Horațiu-Cristian Popescu-Vâlceanu, Ileana Teodoru, Doina-Andrada Mihai, Viviana Elian, Norina Alinta Gavan, and Gabriela Radulian. 2023. "Incidence of Lower Extremity Amputation in Romania: A Nationwide 5-Year Cohort Study, 2015–2019" Medicina 59, no. 7: 1199. https://doi.org/10.3390/medicina59071199
APA StyleRusu, E., Coman, H., Coșoreanu, A., Militaru, A.-M., Popescu-Vâlceanu, H.-C., Teodoru, I., Mihai, D.-A., Elian, V., Gavan, N. A., & Radulian, G. (2023). Incidence of Lower Extremity Amputation in Romania: A Nationwide 5-Year Cohort Study, 2015–2019. Medicina, 59(7), 1199. https://doi.org/10.3390/medicina59071199