
Recent Advancement of Medical Patch for Transdermal Drug Delivery




Abstract

1. Introduction
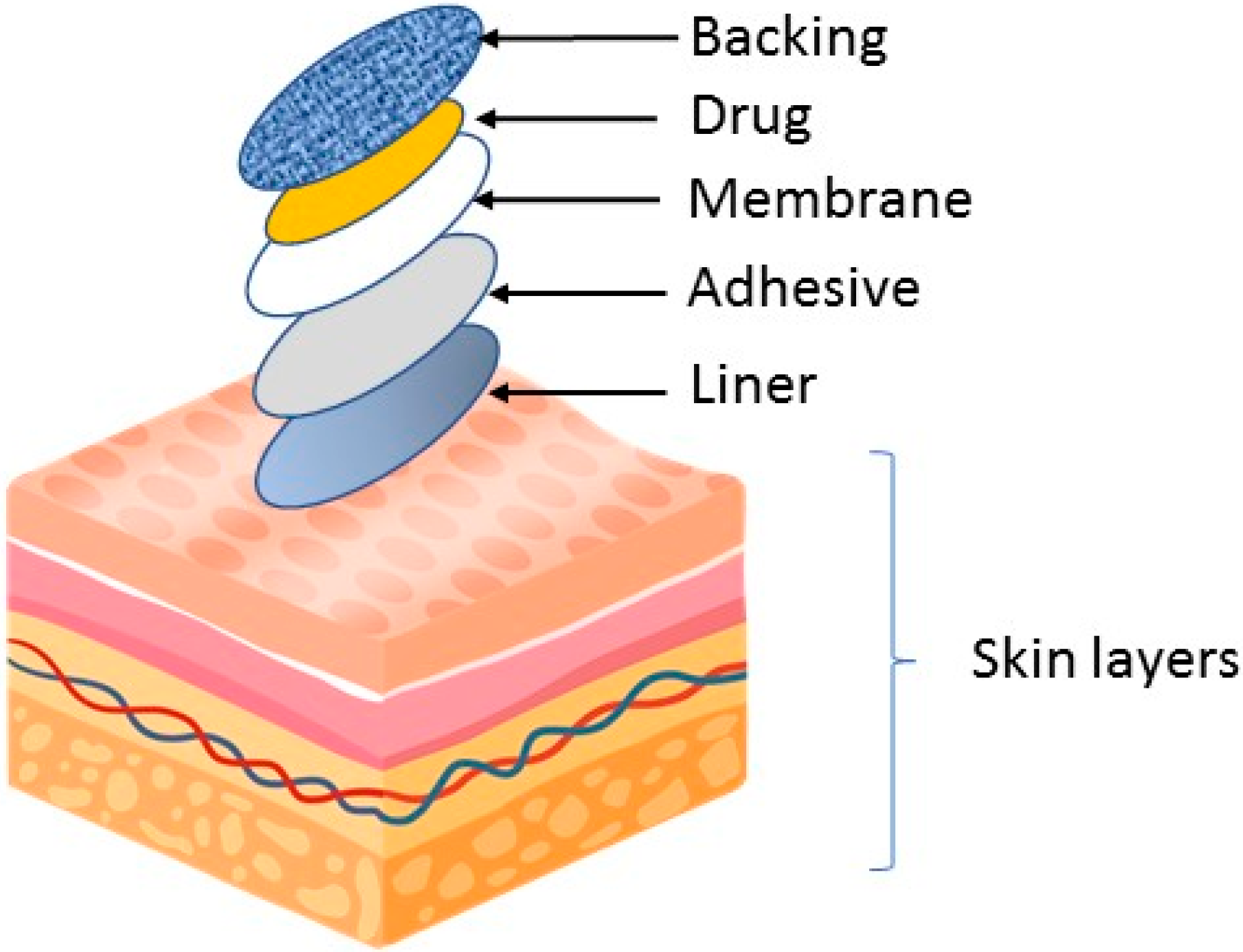
2. Transdermal Patch Design
3. Basic Component of Transdermal Patch
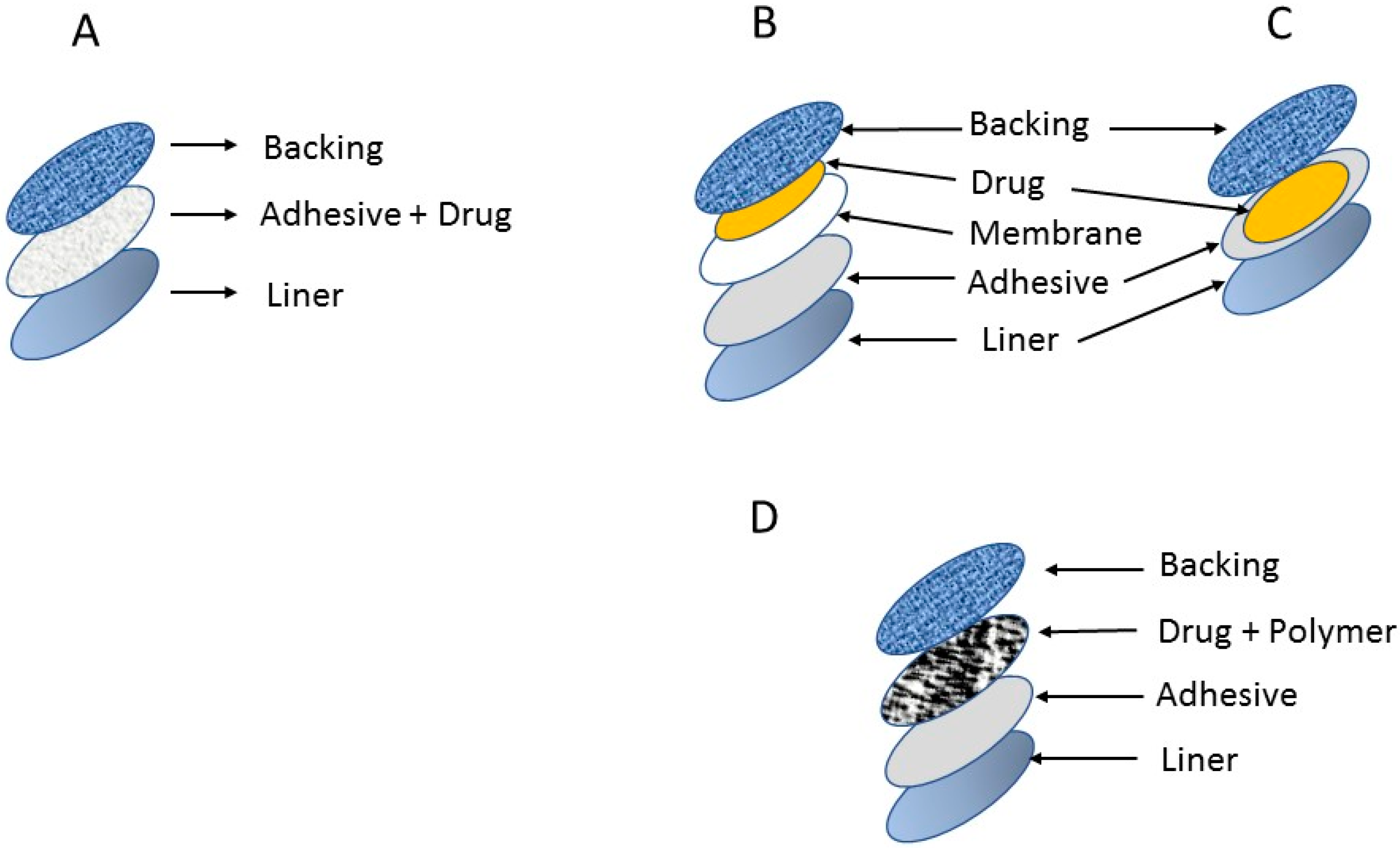
4. Types of Transdermal Patches
4.1. Drug-in-Adhesive System
4.2. Reservoir System
4.3. Matrix System
4.4. Micro-Reservoir System
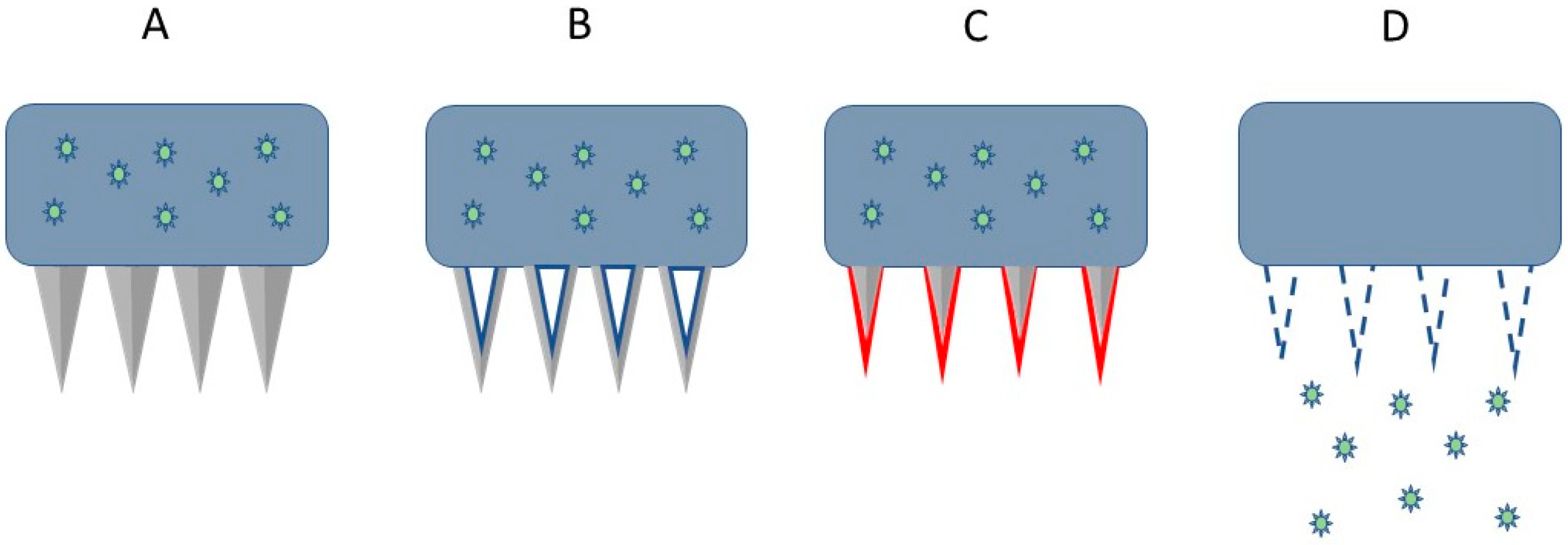
5. Microneedle-Based Patches
- Solid Microneedles: These are the simplest type of microneedles, consisting of solid needles that penetrate the skin to create tiny channels. Solid microneedles are commonly used for drug delivery and cosmetic treatments.
- Hollow Microneedles: These microneedles have a hollow core that allows for the delivery of fluids or drugs into the skin. Hollow microneedles are often used for transdermal drug delivery and sampling of interstitial fluid.
- Coated Microneedles: These microneedles have a coating that dissolves upon penetration of the skin, allowing for the release of drugs or other substances. Coated microneedles are often used for transdermal drug delivery.
- Dissolving Microneedles: These microneedles are made of materials that dissolve in the skin, allowing for the controlled release of drugs or other substances. Dissolving microneedles are often used for vaccines and other drug delivery applications.
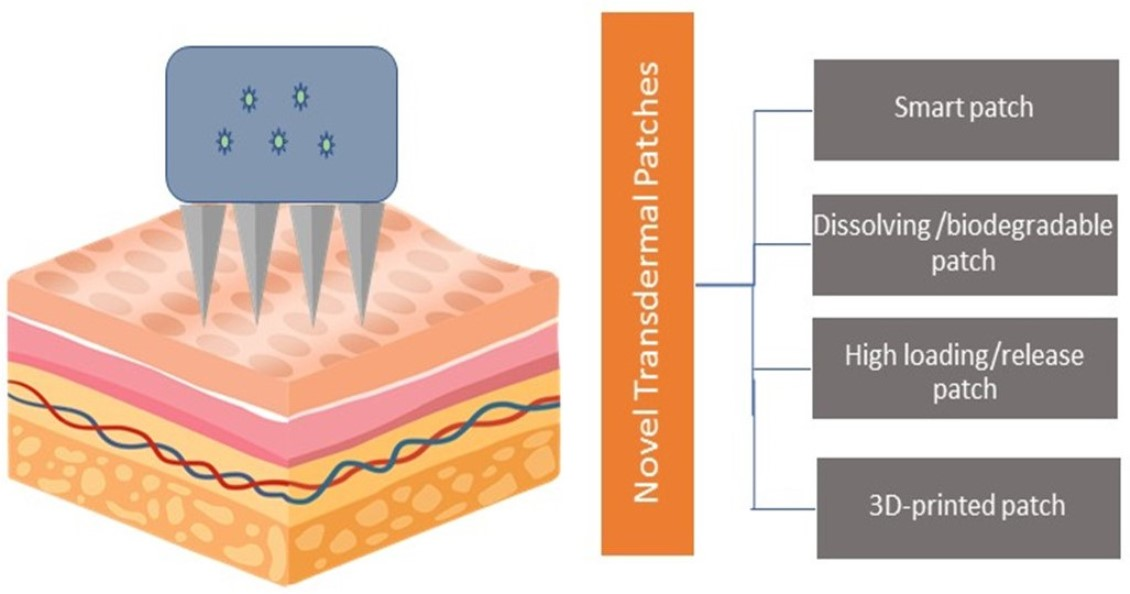
6. Recent Advancement of Transdermal Patch
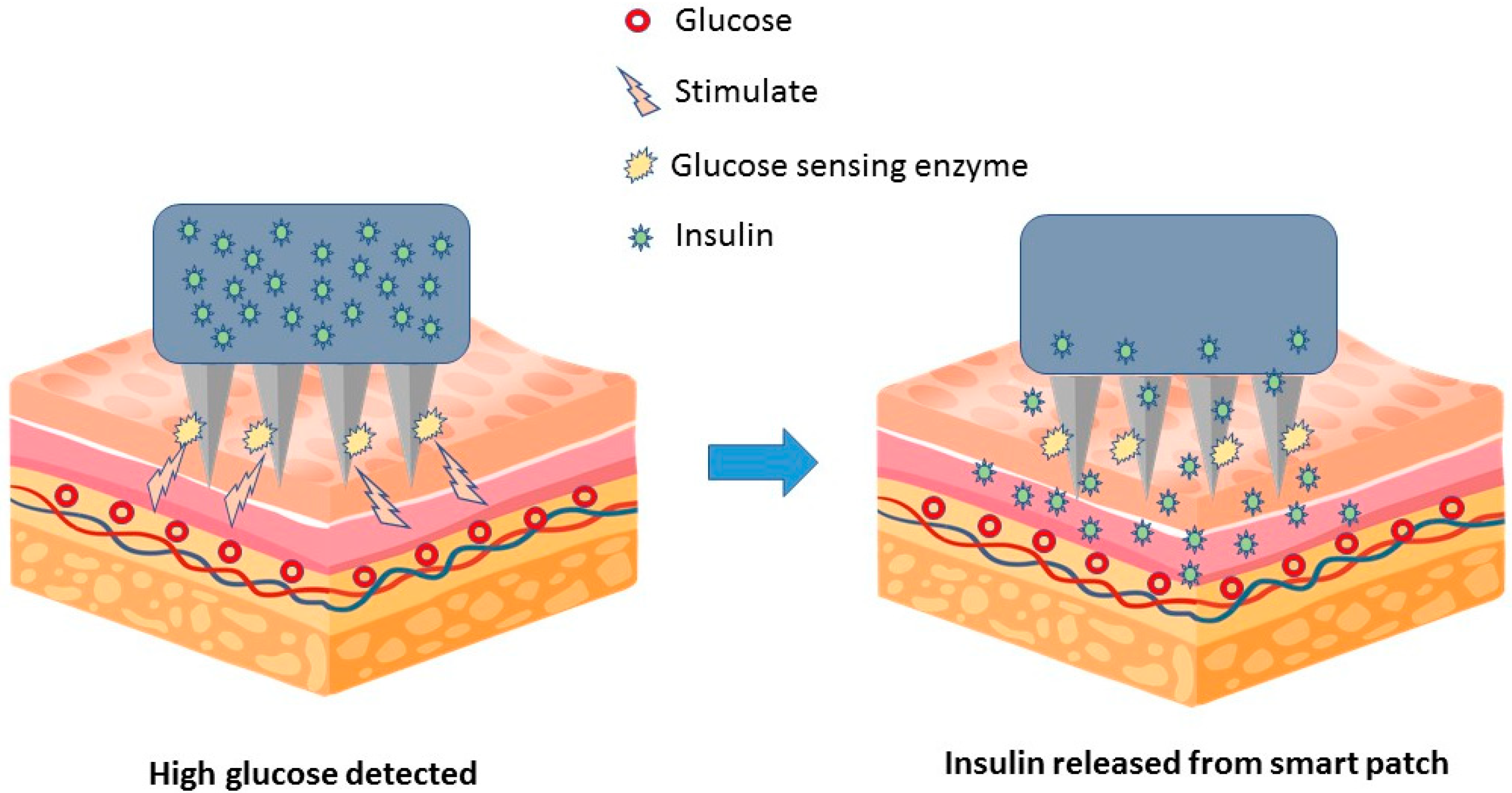
6.1. Smart Patches
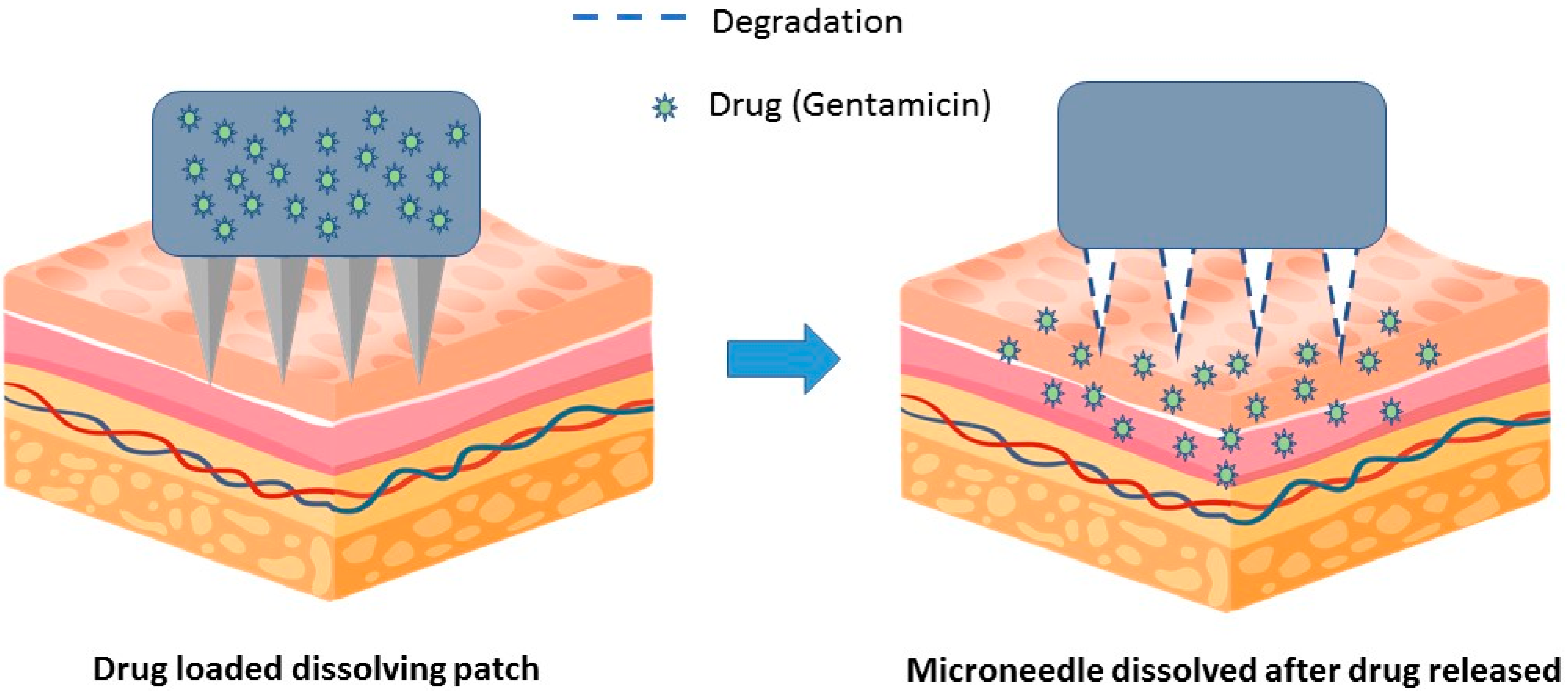
6.2. Dissolving/Degradable Patches
6.3. Three-Dimensional (3D)-Printed Patches
6.4. High Loading/Release Patches
7. Potential Application of Transdermal Patches
7.1. Transdermal Patches for Patches for Vaccination
7.2. Transdermal Patches for Gene Therapy
7.3. Transdermal Patches for Insulin Delivery
7.4. Transdermal Patches for Cardiovascular Diseases
7.5. Transdermal Patches for Hormonal Deficiencies and Contraception
7.6. Transdermal Patches for Central Nervus System (CNS) Disorder
7.7. Transdermal Patches for Infectious Diseases
8. Conclusions and Future Challenges
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chien, Y.W.; Liu, J.C. Transdermal drug delivery systems. J. Biomater. Appl. 1986, 1, 183–206. [Google Scholar] [CrossRef]
- Lasagna, L.; Greenblatt, D.J. More than skin deep: Transdermal drug-delivery systems. N. Engl. J. Med. 1986, 314, 1638–1639. [Google Scholar] [CrossRef]
- Berner, B.; John, V.A. Pharmacokinetic characterisation of transdermal delivery systems. Clin. Pharmacokinet. 1994, 26, 121–134. [Google Scholar] [CrossRef]
- Kopper, N.W.; Gudeman, J.; Thompson, D.J. Transdermal hormone therapy in postmenopausal women: A review of metabolic effects and drug delivery technologies. Drug Des. Dev. Ther. 2009, 2, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Kumar, L.; Verma, S.; Singh, M.; Chalotra, T.; Utreja, P. Advanced Drug Delivery Systems for Transdermal Delivery of Non-Steroidal Anti-Inflammatory Drugs: A Review. Curr. Drug Deliv. 2018, 15, 1087–1099. [Google Scholar] [CrossRef] [PubMed]
- Thirunavukkarasu, A.; Nithya, R.; Jeyanthi, J. Transdermal drug delivery systems for the effective management of type 2 diabetes mellitus: A review. Diabetes Res. Clin. Pract. 2022, 194, 109996. [Google Scholar] [CrossRef]
- Al Hanbali, O.A.; Khan, H.M.S.; Sarfraz, M.; Arafat, M.; Ijaz, S.; Hameed, A. Transdermal patches: Design and current approaches to painless drug delivery. Acta Pharm. 2019, 69, 197–215. [Google Scholar] [CrossRef] [PubMed]
- Musselman, M.; Faden, J.; Citrome, L. Asenapine: An atypical antipsychotic with atypical formulations. Ther. Adv. Psychopharmacol. 2021, 11, 20451253211035269. [Google Scholar] [CrossRef]
- Suzuki, K.; Castelli, M.; Komaroff, M.; Starling, B.; Terahara, T.; Citrome, L. Pharmacokinetic Profile of the Asenapine Transdermal System (HP-3070). J. Clin. Psychopharmacol. 2021, 41, 286–294. [Google Scholar] [CrossRef]
- Yamashita, T.; Ikeda, T.; Akita, Y. Comparison of heart rate reduction effect and safety between bisoprolol transdermal patch and bisoprolol fumarate oral formulation in Japanese patients with persistent/permanent atrial fibrillation (BISONO-AF study). J. Cardiol. 2019, 73, 386–393. [Google Scholar] [CrossRef]
- Transdermal buprenorphine (Butrans) for chronic pain. Med. Lett. Drugs Ther. 2011, 53, 31–32.
- James, I.G.; O’Brien, C.M.; McDonald, C.J. A randomized, double-blind, double-dummy comparison of the efficacy and tolerability of low-dose transdermal buprenorphine (BuTrans seven-day patches) with buprenorphine sublingual tablets (Temgesic) in patients with osteoarthritis pain. J. Pain Symptom Manag. 2010, 40, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Smyth, M.; Haupt, T.S.; Gregoire, M.C. Retrospective Review of the Use of Transdermal Buprenorphine Patches (Butrans) in a Pediatric Population. J. Palliat. Med. 2020, 23, 1094–1097. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.M.; Shi, X.X.; Yang, S.W.; Qian, Q.F.; Huang, Y.; Xie, Y.Q.; Ou, P. Efficacy of clonidine transdermal patch in treatment of moderate to severe tic disorders in children. Chin. J. Contemp. Pediatr. 2017, 19, 786–789. [Google Scholar] [CrossRef]
- Kang, H.; Zhang, Y.F.; Jiao, F.Y.; Guo, X.Y.; Gao, X.M. Efficacy of clonidine transdermal patch for treatment of Tourette’s syndrome in children. Chin. J. Contemp. Pediatr. 2009, 11, 537–539. [Google Scholar]
- Ke, G.M.; Wang, L.; Xue, H.Y.; Lu, W.L.; Zhang, X.; Zhang, Q.; Guo, H.Y. In vitro and in vivo characterization of a newly developed clonidine transdermal patch for treatment of attention deficit hyperactivity disorder in children. Biol. Pharm. Bull. 2005, 28, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Song, P.P.; Jiang, L.; Li, X.J.; Hong, S.Q.; Li, S.Z.; Hu, Y. The Efficacy and Tolerability of the Clonidine Transdermal Patch in the Treatment for Children with Tic Disorders: A Prospective, Open, Single-Group, Self-Controlled Study. Front. Neurol. 2017, 8, 32. [Google Scholar] [CrossRef]
- Antihypertensive Patch Italian Study (APIS) Investigators. One year efficacy and tolerability of clonidine administered by the transdermal route in patients with mild to moderate essential hypertension-A multicentre open label study. Clin. Auton. Res. 1993, 3, 379–383. [Google Scholar] [CrossRef]
- Cutler, A.J.; Suzuki, K.; Starling, B.; Balakrishnan, K.; Komaroff, M.; Castelli, M.; Meeves, S.; Childress, A.C. Efficacy and safety of dextroamphetamine transdermal system for the treatment of attention-deficit/hyperactivity disorder in children and adolescents: Results from a pivotal phase 2 study. J. Child Adolesc. Psychopharmacol. 2022, 32, 89. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Choi, H.Y.; Lim, H.S.; Lee, S.H.; Jeon, H.S.; Hong, D.; Kim, S.S.; Choi, Y.K.; Bae, K.S. Single dose pharmacokinetics of the novel transdermal donepezil patch in healthy volunteers. Drug Des. Dev. Ther. 2015, 9, 1419–1426. [Google Scholar] [CrossRef]
- Yoon, S.K.; Bae, K.S.; Hong, D.H.; Kim, S.S.; Choi, Y.K.; Lim, H.S. Pharmacokinetic evaluation by modeling and simulation analysis of a donepezil patch formulation in healthy male volunteers. Drug Des. Devel. Ther. 2020, 14, 1729. [Google Scholar] [CrossRef]
- Aguirre, W.; Chedraui, P.; Mendoza, J.; Ruilova, I. Gabapentin vs. low-dose transdermal estradiol for treating post-menopausal women with moderate to very severe hot flushes. Gynecol. Endocrinol. 2010, 26, 333–337. [Google Scholar] [CrossRef]
- Clemente, C.; Caruso, M.G.; Berloco, P.; Buonsante, A.; Giannandrea, B.; Di Leo, A. alpha-Tocopherol and beta-carotene serum levels in post-menopausal women treated with transdermal estradiol and oral medroxyprogesterone acetate. Horm. Metab. Res. 1996, 28, 558–561. [Google Scholar] [CrossRef]
- Zieman, M. The introduction of a transdermal hormonal contraceptive (Ortho Evra/Evra). Fertil. Steril. 2002, 77, S1–S2. [Google Scholar] [CrossRef]
- Zieman, M.; Guillebaud, J.; Weisberg, E.; Shangold, G.A.; Fisher, A.C.; Creasy, G.W. Contraceptive efficacy and cycle control with the Ortho Evra/Evra transdermal system: The analysis of pooled data. Fertil. Steril. 2002, 77, S13–S18. [Google Scholar] [CrossRef] [PubMed]
- Baumrucker, S.J. Duragesic (transdermal fentanyl) in hospice care. Am. J. Hosp. Palliat. Care 1996, 13, 13–15. [Google Scholar] [CrossRef] [PubMed]
- Abramowicz, M.; Zuccotti, G.; Pflomm, J.M.; Daron, S.M.; Houst, B.M.; Zanone, C.E.; Dalton, V.K.; Epstein, E.J.; Hirsch, J.; Juurlink, D.N. A granisetron patch (sancuso). Med. Lett. Drugs Ther. 2008, 50, 103–104; quiz p. 102 following 104. [Google Scholar]
- Howell, J.; Smeets, J.; Drenth, H.J.; Gill, D. Pharmacokinetics of a granisetron transdermal system for the treatment of chemotherapy-induced nausea and vomiting. J. Oncol. Pharm. Pract. 2009, 15, 223–231. [Google Scholar] [CrossRef]
- Le, T.N.; Adler, M.T.; Ouillette, H.; Berens, P.; Smith, J.A. Observational Case Series Evaluation of the Granisetron Transdermal Patch System (Sancuso) for the Management of Nausea/Vomiting of Pregnancy. Am. J. Perinatol. 2017, 34, 851–855. [Google Scholar] [CrossRef]
- Badoi, D.; Crauciuc, E.; Rusu, L.; Luca, V. Therapy with climara in surgical menopause. Rev. Med. Chir. Soc. Med. Nat. Iasi 2012, 116, 828–833. [Google Scholar]
- Taggart, W.; Dandekar, K.; Ellman, H.; Notelovitz, M. The effect of site of application on the transcutaneous absorption of 17-beta estradiol from a transdermal delivery system (Climara). Menopause 2000, 7, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Desai, M.J.; Siriki, R.; Wang, D. Treatment of pain in Dercum’s disease with Lidoderm (lidocaine 5% patch): A case report. Pain Med. 2008, 9, 1224–1226. [Google Scholar] [CrossRef] [PubMed]
- Karmarkar, A.; Lieberman, I. Management of complex regional pain syndrome type II using lidoderm 5% patches. Br. J. Anaesth. 2007, 98, 261–262. [Google Scholar] [CrossRef] [PubMed]
- Wokovich, A.M.; Shen, M.; Doub, W.H.; Machado, S.G.; Buhse, L.F. Evaluating elevated release liner adhesion of a transdermal drug delivery system (TDDS): A study of Daytrana methylphenidate transdermal system. Drug Dev. Ind. Pharm. 2011, 37, 1217–1224. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.K.; Lan, T.H.; Wu, B.J. A double-blind randomized clinical trial of different doses of transdermal nicotine patch for smoking reduction and cessation in long-term hospitalized schizophrenic patients. Eur. Arch. Psychiatry Clin. Neurosci. 2013, 263, 75–82. [Google Scholar] [CrossRef]
- Perng, R.P.; Hsieh, W.C.; Chen, Y.M.; Lu, C.C.; Chiang, S.J. Randomized, double-blind, placebo-controlled study of transdermal nicotine patch for smoking cessation. J. Formos. Med. Assoc. 1998, 97, 547–551. [Google Scholar]
- Rich, J.D. Transdermal nicotine patch for smoking cessation. N. Engl. J. Med. 1992, 326, 344–345. [Google Scholar]
- Dahlstrom, C.G.; Rasmussen, K.; Bagger, J.P.; Henningsen, P.; Haghfelt, T. Transdermal nitroglycerin (Transiderm-Nitro) in the treatment of unstable angina pectoris. Dan. Med. Bull. 1986, 33, 265–267. [Google Scholar]
- Greco, R.; D’Alterio, D.; Schiattarella, M.; Boccia, A.; Greco, L.; Marsico, F. Efficacy of a new transdermal nitroglycerin patch (Deponit 10) for stable angina pectoris. Am. J. Cardiol. 1988, 61, 44E–51E. [Google Scholar] [CrossRef]
- Mammen, M.V.; Tripathi, M.; Chandola, H.C.; Tyagi, A.; Bais, P.S.; Sanjeev, O.P. Comparison of Enhancement of Analgesic Effect of Intrathecal Neostigmine by Intrathecal Clonidine and Transdermal Nitroglycerin Patch on Bupivacaine Spinal Anesthesia. Anesth. Essays Res. 2017, 11, 993–997. [Google Scholar] [CrossRef]
- Savonitto, S.; Motolese, M.; Agabiti-Rosei, E. Antianginal effect of transdermal nitroglycerin and oral nitrates given for 24 hours a day in 2,456 patients with stable angina pectoris. The Italian Multicenter Study. Int. J. Clin. Pharmacol. Ther. 1995, 33, 194–203. [Google Scholar] [PubMed]
- Archer, D.F.; Furst, K.; Tipping, D.; Dain, M.P.; Vandepol, C. A randomized comparison of continuous combined transdermal delivery of estradiol-norethindrone acetate and estradiol alone for menopause. CombiPatch Study Group. Obstet. Gynecol. 1999, 94, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Dull, P. Transdermal oxybutynin (oxytrol) for urinary incontinence. Am. Fam. Physician 2004, 70, 2351–2352. [Google Scholar]
- Ho, C. Transdermally-delivered oxybutynin (Oxytrol(R) for overactive bladder. Issues Emerg. Health Technol. 2001, 24, 1–4. [Google Scholar]
- Kurz, A.; Farlow, M.; Lefevre, G. Pharmacokinetics of a novel transdermal rivastigmine patch for the treatment of Alzheimer’s disease: A review. Int. J. Clin. Pract. 2009, 63, 799–805. [Google Scholar] [CrossRef]
- Lefevre, G.; Pommier, F.; Sedek, G.; Allison, M.; Huang, H.L.; Kiese, B.; Ho, Y.Y.; Appel-Dingemanse, S. Pharmacokinetics and bioavailability of the novel rivastigmine transdermal patch versus rivastigmine oral solution in healthy elderly subjects. J. Clin. Pharmacol. 2008, 48, 246–252. [Google Scholar] [CrossRef]
- Chatsis, V. Rotigotine transdermal patches (Neupro) for the treatment of Parkinson’s disease. Issues Emerg. Health Technol. 2008, 112, 1–6. [Google Scholar]
- Jessen, L.; Kovalick, L.J.; Azzaro, A.J. The selegiline transdermal system (emsam): A therapeutic option for the treatment of major depressive disorder. P T Peer-Rev. J. Formul. Manag. 2008, 33, 212–246. [Google Scholar]
- Johnson, P.; Hansen, D.; Matarazzo, D.; Petterson, L.; Swisher, C.; Trappolini, A. Transderm Scop for prevention of motion sickness. N. Engl. J. Med. 1984, 311, 468–469. [Google Scholar] [CrossRef]
- Swaminathan, S.K.; Strasinger, C.; Kelchen, M.; Carr, J.; Ye, W.; Wokovich, A.; Ghosh, P.; Rajagopal, S.; Ueda, K.; Fisher, J.; et al. Determination of Rate and Extent of Scopolamine Release from Transderm Scop(R) Transdermal Drug Delivery Systems in Healthy Human Adults. AAPS PharmSciTech 2020, 21, 117. [Google Scholar] [CrossRef]
- Bhasin, S.; Storer, T.W.; Asbel-Sethi, N.; Kilbourne, A.; Hays, R.; Sinha-Hikim, I.; Shen, R.; Arver, S.; Beall, G. Effects of testosterone replacement with a nongenital, transdermal system, Androderm, in human immunodeficiency virus-infected men with low testosterone levels. J. Clin. Endocrinol. Metab. 1998, 83, 3155–3162. [Google Scholar] [CrossRef] [PubMed]
- De Sanctis, V.; Vullo, C.; Urso, L.; Rigolin, F.; Cavallini, A.; Caramelli, K.; Daugherty, C.; Mazer, N. Clinical experience using the Androderm testosterone transdermal system in hypogonadal adolescents and young men with beta-thalassemia major. J. Pediatr. Endocrinol. Metab. 1998, 11 (Suppl. 3), 891–900. [Google Scholar] [PubMed]
- Buch, A.; Shen, L.; Kelly, S.; Sahota, R.; Brezovic, C.; Bixler, C.; Powell, J. Steady-state bioavailability of estradiol from two matrix transdermal delivery systems, Alora and Climara. Menopause 1998, 5, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Rozenbaum, H.; Birkhauser, M.; De Nooyer, C.; Lambotte, R.; Pornel, B.; Schneider, H.; Studd, J. Comparison of two estradiol transdermal systems (Oesclim 50 and Estraderm TTS 50). I. Tolerability, adhesion and efficacy. Maturitas 1996, 25, 161–173. [Google Scholar] [CrossRef]
- Youngkin, E.Q. Estrogen replacement therapy and the estraderm transdermal system. Nurse Pract. 1990, 15, 19–26, 31. [Google Scholar] [CrossRef]
- Wokovich, A.M.; Prodduturi, S.; Doub, W.H.; Hussain, A.S.; Buhse, L.F. Transdermal drug delivery system (TDDS) adhesion as a critical safety, efficacy and quality attribute. Eur. J. Pharm. Biopharm. 2006, 64, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.C.; Park, J.H.; Prausnitz, M.R. Microneedles for drug and vaccine delivery. Adv. Drug Deliv. Rev. 2012, 64, 1547–1568. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Z.; Huo, M.R.; Zhou, J.P.; Zhou, Y.Q.; Hao, B.H.; Liu, T.; Zhang, Y. Super-short solid silicon microneedles for transdermal drug delivery applications. Int. J. Pharm. 2010, 389, 122–129. [Google Scholar] [CrossRef]
- Permana, A.D.; Tekko, I.A.; McCrudden, M.T.C.; Anjani, Q.K.; Ramadon, D.; McCarthy, H.O.; Donnelly, R.F. Solid lipid nanoparticle-based dissolving microneedles: A promising intradermal lymph targeting drug delivery system with potential for enhanced treatment of lymphatic filariasis. J. Control. Release 2019, 316, 34–52. [Google Scholar] [CrossRef]
- Cheung, K.; Das, D.B. Microneedles for drug delivery: Trends and progress. Drug Deliv. 2016, 23, 2338–2354. [Google Scholar] [CrossRef]
- Ita, K. Transdermal Delivery of Drugs with Microneedles-Potential and Challenges. Pharmaceutics 2015, 7, 90–105. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, M.W.; Tayyaba, S.; Nisar, A.; Afzulpurkar, N.; Bodhale, D.W.; Lomas, T.; Poyai, A.; Tuantranont, A. Design, fabrication and analysis of silicon hollow microneedles for transdermal drug delivery system for treatment of hemodynamic dysfunctions. Cardiovasc. Eng. 2010, 10, 91–108. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, C.; Sebastian, R.; Tjulkins, F.; Whelan, D.; Bocchino, A.; Hu, Y.; O’Brien, J.; Scully, J.; Hegarty, M.; Blake, A.; et al. Hollow silicon microneedles, fabricated using combined wet and dry etching techniques, for transdermal delivery and diagnostics. Int. J. Pharm. 2023, 637, 122888. [Google Scholar] [CrossRef]
- Ma, Y.; Gill, H.S. Coating solid dispersions on microneedles via a molten dip-coating method: Development and in vitro evaluation for transdermal delivery of a water-insoluble drug. J. Pharm. Sci. 2014, 103, 3621–3630. [Google Scholar] [CrossRef]
- Chen, B.Z.; He, M.C.; Zhang, X.P.; Fei, W.M.; Cui, Y.; Guo, X.D. A novel method for fabrication of coated microneedles with homogeneous and controllable drug dosage for transdermal drug delivery. Drug Deliv. Transl. Res. 2022, 12, 2730–2739. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Chen, B.Z.; Wang, Q.L.; Jin, X.; Guo, X.D. Fabrication of coated polymer microneedles for transdermal drug delivery. J. Control. Release 2017, 265, 14–21. [Google Scholar] [CrossRef]
- Gill, H.S.; Prausnitz, M.R. Coated microneedles for transdermal delivery. J. Control. Release 2007, 117, 227–237. [Google Scholar] [CrossRef]
- Dalvi, M.; Kharat, P.; Thakor, P.; Bhavana, V.; Singh, S.B.; Mehra, N.K. Panorama of dissolving microneedles for transdermal drug delivery. Life Sci. 2021, 284, 119877. [Google Scholar] [CrossRef]
- Dillon, C.; Hughes, H.; O’Reilly, N.J.; McLoughlin, P. Formulation and characterisation of dissolving microneedles for the transdermal delivery of therapeutic peptides. Int. J. Pharm. 2017, 526, 125–136. [Google Scholar] [CrossRef]
- Ita, K. Dissolving microneedles for transdermal drug delivery: Advances and challenges. Biomed. Pharmacother. 2017, 93, 1116–1127. [Google Scholar] [CrossRef]
- Lee, J.W.; Park, J.H.; Prausnitz, M.R. Dissolving microneedles for transdermal drug delivery. Biomaterials 2008, 29, 2113–2124. [Google Scholar] [CrossRef] [PubMed]
- Invernale, M.A.; Tang, B.C.; York, R.L.; Le, L.; Hou, D.Y.; Anderson, D.G. Microneedle electrodes toward an amperometric glucose-sensing smart patch. Adv. Healthc. Mater. 2014, 3, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Veiseh, O.; Langer, R. Diabetes: A smart insulin patch. Nature 2015, 524, 39–40. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Zhang, Y.; Ye, Y.; DiSanto, R.; Sun, W.; Ranson, D.; Ligler, F.S.; Buse, J.B.; Gu, Z. Microneedle-array patches loaded with hypoxia-sensitive vesicles provide fast glucose-responsive insulin delivery. Proc. Natl. Acad. Sci. USA 2015, 112, 8260–8265. [Google Scholar] [CrossRef] [PubMed]
- Iversen, M.; Monisha, M.; Agarwala, S. Flexible, Wearable and Fully-printed Smart Patch for pH and Hydration Sensing in Wounds. Int. J. Bioprinting 2022, 8, 447. [Google Scholar] [CrossRef]
- Liu, H.; Li, Z.; Che, S.; Feng, Y.; Guan, L.; Yang, X.; Zhao, Y.; Wang, J.; Zvyagin, A.V.; Yang, B.; et al. A smart hydrogel patch with high transparency, adhesiveness and hemostasis for all-round treatment and glucose monitoring of diabetic foot ulcers. J. Mater. Chem. B 2022, 10, 5804–5817. [Google Scholar] [CrossRef]
- Gilpin, V.; Surandhiran, D.; Scott, C.; Devine, A.; Cundell, J.H.; Gill, C.I.R.; Pourshahidi, L.K.; Davis, J. Lasered Graphene Microheaters Modified with Phase-Change Composites: New Approach to Smart Patch Drug Delivery. Micromachines 2022, 13, 1132. [Google Scholar] [CrossRef]
- Rodgers, A.M.; McCrudden, M.T.C.; Courtenay, A.J.; Kearney, M.C.; Edwards, K.L.; Ingram, R.J.; Bengoechea, J.; Donnelly, R.F. Control of Klebsiella pneumoniae Infection in Mice by Using Dissolving Microarray Patches Containing Gentamicin. Antimicrob. Agents Chemother. 2019, 63, e02612-18. [Google Scholar] [CrossRef]
- Lee, I.C.; Lin, W.M.; Shu, J.C.; Tsai, S.W.; Chen, C.H.; Tsai, M.T. Formulation of two-layer dissolving polymeric microneedle patches for insulin transdermal delivery in diabetic mice. J. Biomed. Mater. Res. Part A 2017, 105, 84–93. [Google Scholar] [CrossRef]
- Kim, H.; Seong, K.Y.; Lee, J.H.; Park, W.; Yang, S.Y.; Hahn, S.K. Biodegradable Microneedle Patch Delivering Antigenic Peptide-Hyaluronate Conjugate for Cancer Immunotherapy. ACS Biomater. Sci. Eng. 2019, 5, 5150–5158. [Google Scholar] [CrossRef]
- Li, Y.; Liu, F.; Su, C.; Yu, B.; Liu, D.; Chen, H.J.; Lin, D.A.; Yang, C.; Zhou, L.; Wu, Q.; et al. Biodegradable Therapeutic Microneedle Patch for Rapid Antihypertensive Treatment. ACS Appl. Mater. Interfaces 2019, 11, 30575–30584. [Google Scholar] [CrossRef] [PubMed]
- Adli, S.A.; Ali, F.; Azmi, A.S.; Anuar, H.; Nasir, N.A.M.; Hasham, R.; Idris, M.K.H. Development of Biodegradable Cosmetic Patch Using a Polylactic Acid/Phycocyanin-Alginate Composite. Polymers 2020, 12, 1669. [Google Scholar] [CrossRef] [PubMed]
- Economidou, S.N.; Pissinato Pere, C.P.; Okereke, M.; Douroumis, D. Optimisation of Design and Manufacturing Parameters of 3D Printed Solid Microneedles for Improved Strength, Sharpness, and Drug Delivery. Micromachines 2021, 12, 117. [Google Scholar] [CrossRef]
- Jang, M.J.; Bae, S.K.; Jung, Y.S.; Kim, J.C.; Kim, J.S.; Park, S.K.; Suh, J.S.; Yi, S.J.; Ahn, S.H.; Lim, J.O. Enhanced wound healing using a 3D printed VEGF-mimicking peptide incorporated hydrogel patch in a pig model. Biomed. Mater. 2021, 16, 045013. [Google Scholar] [CrossRef]
- Caudill, C.; Perry, J.L.; Iliadis, K.; Tessema, A.T.; Lee, B.J.; Mecham, B.S.; Tian, S.; DeSimone, J.M. Transdermal vaccination via 3D-printed microneedles induces potent humoral and cellular immunity. Proc. Natl. Acad. Sci. USA 2021, 118, e2102595118. [Google Scholar] [CrossRef] [PubMed]
- Yadav, V.; Sharma, P.K.; Murty, U.S.; Mohan, N.H.; Thomas, R.; Dwivedy, S.K.; Banerjee, S. 3D printed hollow microneedles array using stereolithography for efficient transdermal delivery of rifampicin. Int. J. Pharm. 2021, 605, 120815. [Google Scholar] [CrossRef]
- Maurizii, G.; Moroni, S.; Khorshid, S.; Aluigi, A.; Tiboni, M.; Casettari, L. 3D-printed EVA-based patches manufactured by direct powder extrusion for personalized transdermal therapies. Int. J. Pharm. 2023, 635, 122720. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Kathuria, H.; Amir, M.H.B.; Zhang, X.; Duong, H.T.T.; Ho, P.C.; Kang, L. High resolution photopolymer for 3D printing of personalised microneedle for transdermal delivery of anti-wrinkle small peptide. J. Control. Release 2021, 329, 907–918. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Liu, C.; Song, Y.; Ruan, J.; Quan, P.; Fang, L. High drug-loading and controlled-release hydroxyphenyl-polyacrylate adhesive for transdermal patch. J. Control. Release 2023, 353, 475–489. [Google Scholar] [CrossRef]
- Yang, D.; Liu, C.; Piao, H.; Quan, P.; Fang, L. Enhanced Drug Loading in the Drug-in-Adhesive Transdermal Patch Utilizing a Drug-Ionic Liquid Strategy: Insight into the Role of Ionic Hydrogen Bonding. Mol. Pharm. 2021, 18, 1157–1166. [Google Scholar] [CrossRef]
- Yang, D.; Liu, C.; Quan, P.; Fang, L. Molecular mechanism of high capacity-high release transdermal drug delivery patch with carboxyl acrylate polymer: Roles of ion-ion repulsion and hydrogen bond. Int. J. Pharm. 2020, 585, 119376. [Google Scholar] [CrossRef]
- Choi, I.J.; Cha, H.R.; Hwang, S.J.; Baek, S.K.; Lee, J.M.; Choi, S.O. Live Vaccinia Virus-Coated Microneedle Array Patches for Smallpox Vaccination and Stockpiling. Pharmaceutics 2021, 13, 209. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.P.; Koutsonanos, D.G.; Del Pilar Martin, M.; Lee, J.W.; Zarnitsyn, V.; Choi, S.O.; Murthy, N.; Compans, R.W.; Skountzou, I.; Prausnitz, M.R. Dissolving polymer microneedle patches for influenza vaccination. Nat. Med. 2010, 16, 915–920. [Google Scholar] [CrossRef]
- Singh, P.; Muhammad, I.; Nelson, N.E.; Tran, K.T.M.; Vinikoor, T.; Chorsi, M.T.; D’Orio, E.; Nguyen, T.D. Transdermal delivery for gene therapy. Drug Deliv. Transl. Res. 2022, 12, 2613–2633. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Li, X.; Zhang, P.; Wang, Y. Rapidly dissolving microneedle patch for synergistic gene and photothermal therapy of subcutaneous tumor. J. Mater. Chem. B 2020, 8, 4331–4339. [Google Scholar] [CrossRef]
- Islam, M.R.; Uddin, S.; Chowdhury, M.R.; Wakabayashi, R.; Moniruzzaman, M.; Goto, M. Insulin Transdermal Delivery System for Diabetes Treatment Using a Biocompatible Ionic Liquid-Based Microemulsion. ACS Appl. Mater. Interfaces 2021, 13, 42461–42472. [Google Scholar] [CrossRef]
- Jorge, L.R.; Harada, L.K.; Silva, E.C.; Campos, W.F.; Moreli, F.C.; Shimamoto, G.; Pereira, J.F.B.; Oliveira, J.M., Jr.; Tubino, M.; Vila, M.; et al. Non-invasive Transdermal Delivery of Human Insulin Using Ionic Liquids: In vitro Studies. Front. Pharmacol. 2020, 11, 243. [Google Scholar] [CrossRef]
- Lin, X.; Choi, D.; Hong, J. Insulin particles as building blocks for controlled insulin release multilayer nano-films. Mater. Sci. Eng. C Mater. Biol. Appl. 2015, 54, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Maciel, V.B.V.; Yoshida, C.M.P.; Pereira, S.; Goycoolea, F.M.; Franco, T.T. Electrostatic Self-Assembled Chitosan-Pectin Nano- and Microparticles for Insulin Delivery. Molecules 2017, 22, 1707. [Google Scholar] [CrossRef]
- Tanner, E.E.L.; Ibsen, K.N.; Mitragotri, S. Transdermal insulin delivery using choline-based ionic liquids (CAGE). J. Control. Release 2018, 286, 137–144. [Google Scholar] [CrossRef]
- Sugumar, V.; Ang, K.P.; Alshanon, A.F.; Sethi, G.; Yong, P.V.C.; Looi, C.Y.; Wong, W.F. A Comprehensive Review of the Evolution of Insulin Development and Its Delivery Method. Pharmaceutics 2022, 14, 1406. [Google Scholar] [CrossRef] [PubMed]
- Seong, K.Y.; Seo, M.S.; Hwang, D.Y.; O’Cearbhaill, E.D.; Sreenan, S.; Karp, J.M.; Yang, S.Y. A self-adherent, bullet-shaped microneedle patch for controlled transdermal delivery of insulin. J. Control. Release 2017, 265, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, R.; Stachnik, J.M.; Echizen, H. Clinical pharmacokinetics of drugs in patients with heart failure: An update (part 1, drugs administered intravenously). Clin. Pharmacokinet. 2013, 52, 169–185. [Google Scholar] [CrossRef]
- Lainscak, M.; Vitale, C.; Seferovic, P.; Spoletini, I.; Cvan Trobec, K.; Rosano, G.M. Pharmacokinetics and pharmacodynamics of cardiovascular drugs in chronic heart failure. Int. J. Cardiol. 2016, 224, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Mangoni, A.A.; Jarmuzewska, E.A. The influence of heart failure on the pharmacokinetics of cardiovascular and non-cardiovascular drugs: A critical appraisal of the evidence. Br. J. Clin. Pharmacol. 2019, 85, 20–36. [Google Scholar] [CrossRef]
- Ahad, A.; Aqil, M.; Kohli, K.; Sultana, Y.; Mujeeb, M.; Ali, A. Interactions between novel terpenes and main components of rat and human skin: Mechanistic view for transdermal delivery of propranolol hydrochloride. Curr. Drug Deliv. 2011, 8, 213–224. [Google Scholar] [CrossRef]
- Corbo, M.; Liu, J.C.; Chien, Y.W. Bioavailability of propranolol following oral and transdermal administration in rabbits. J. Pharm. Sci. 1990, 79, 584–587. [Google Scholar] [CrossRef]
- Matsuoka, H.; Kuwajima, I.; Shimada, K.; Mitamura, H.; Saruta, T. Comparison of efficacy and safety between bisoprolol transdermal patch (TY-0201) and bisoprolol fumarate oral formulation in Japanese patients with grade I or II essential hypertension: Randomized, double-blind, placebo-controlled study. J. Clin. Hypertens. 2013, 15, 806–814. [Google Scholar] [CrossRef]
- Hara, T.; Yagi, S.; Akaike, M.; Sata, M. Transdermal patch of bisoprolol for the treatment of hypertension complicated with aortic dissection. Int. J. Cardiol. 2015, 198, 220–221. [Google Scholar] [CrossRef]
- Shinohara, M.; Fujino, T.; Koike, H.; Kitahara, K.; Kinoshita, T.; Yuzawa, H.; Suzuki, T.; Fukunaga, S.; Kobayashi, K.; Aoki, J.; et al. Assessment of a novel transdermal selective beta1-blocker, the bisoprolol patch, for treating frequent premature ventricular contractions in patients without structural heart disease. J. Cardiol. 2017, 70, 212–219. [Google Scholar] [CrossRef]
- Kiuchi, S.; Hisatake, S.; Kabuki, T.; Oka, T.; Dobashi, S.; Fujii, T.; Sano, T.; Ikeda, T. Bisoprolol transdermal patch improves orthostatic hypotension in patients with chronic heart failure and hypertension. Clin. Exp. Hypertens. 2020, 42, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Yasui, T.; Oka, T.; Shioyama, W.; Oboshi, M.; Fujita, M. Bisoprolol transdermal patch treatment for patients with atrial fibrillation after noncardiac surgery: A single-center retrospective study of 61 patients. SAGE Open Med. 2020, 8, 7817. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Sonoo, T.; Nakano, H.; Naraba, H.; Hashimoto, H.; Nakamura, K. The influence of edema on the bisoprolol blood concentration after bisoprolol dermal patch application: A case-control study. Medicine 2021, 100, e27354. [Google Scholar] [CrossRef] [PubMed]
- Onesti, G.; Bock, K.D.; Heimsoth, V.; Kim, K.E.; Merguet, P. Clonidine: A new antihypertensive agent. Am. J. Cardiol. 1971, 28, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Groom, M.J.; Cortese, S. Current Pharmacological Treatments for ADHD. Curr. Top. Behav. Neurosci. 2022, 57, 19–50. [Google Scholar] [CrossRef] [PubMed]
- Gossop, M. Clonidine and the treatment of the opiate withdrawal syndrome. Drug Alcohol Depend. 1988, 21, 253–259. [Google Scholar] [CrossRef]
- Popli, S.; Stroka, G.; Ing, T.S.; Daugirdas, J.T.; Norusis, M.J.; Hano, J.E.; Gandhi, V.C. Transdermal clonidine for hypertensive patients. Clin. Ther. 1983, 5, 624–628. [Google Scholar]
- Elliott, W.J.; Prisant, L.M. Drug delivery systems for antihypertensive agents. Blood Press. Monit. 1997, 2, 53–60. [Google Scholar] [CrossRef]
- Fujimura, A.; Ebihara, A.; Ohashi, K.; Shiga, T.; Kumagai, Y.; Nakashima, H.; Kotegawa, T. Comparison of the pharmacokinetics, pharmacodynamics, and safety of oral (Catapres) and transdermal (M-5041T) clonidine in healthy subjects. J. Clin. Pharmacol. 1994, 34, 260–265. [Google Scholar] [CrossRef]
- Thakur, R.; Anwer, M.K.; Shams, M.S.; Ali, A.; Khar, R.K.; Shakeel, F.; Taha, E.I. Proniosomal transdermal therapeutic system of losartan potassium: Development and pharmacokinetic evaluation. J. Drug Target. 2009, 17, 442–449. [Google Scholar] [CrossRef]
- Marsh, N.; Marsh, A. A short history of nitroglycerine and nitric oxide in pharmacology and physiology. Clin. Exp. Pharmacol. Physiol. 2000, 27, 313–319. [Google Scholar] [CrossRef]
- Nicholls, M. Nitric oxide discovery Nobel Prize winners. Eur. Heart J. 2019, 40, 1747–1749. [Google Scholar] [CrossRef] [PubMed]
- Noonan, P.K.; Gonzalez, M.A.; Ruggirello, D.; Tomlinson, J.; Babcock-Atkinson, E.; Ray, M.; Golub, A.; Cohen, A. Relative bioavailability of a new transdermal nitroglycerin delivery system. J. Pharm. Sci. 1986, 75, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Balfour, J.A.; Heel, R.C. Transdermal estradiol. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic efficacy in the treatment of menopausal complaints. Drugs 1990, 40, 561–582. [Google Scholar] [CrossRef]
- Le Roux, Y.; Borg, M.L.; Sibille, M.; Thebault, J.; Renoux, A.; Douin, M.J.; Djebbar, F.; Dain, M.P. Bioavailability Study of Menorest(R), a New Estrogen Transdermal Delivery System, Compared with a Transdermal Reservoir System. Clin. Drug Investig. 1995, 10, 172–178. [Google Scholar] [CrossRef]
- Marty, J.P. Menorest: Technical development and pharmacokinetic profile. Eur. J. Obstet. Gynecol. Reprod. Biol. 1996, 64, S29–S33. [Google Scholar] [CrossRef]
- Muller, P.; Botta, L.; Ezzet, F. Bioavailability of estradiol from a new matrix and a conventional reservoir-type transdermal therapeutic system. Eur. J. Clin. Pharmacol. 1996, 51, 327–330. [Google Scholar] [CrossRef]
- Reginster, J.Y.; Albert, A.; Deroisy, R.; Colette, J.; Vrijens, B.; Blacker, C.; Brion, N.; Caulin, F.; Mayolle, C.; Regnard, A.; et al. Plasma estradiol concentrations and pharmacokinetics following transdermal application of Menorest 50 or Systen (Evorel) 50. Maturitas 1997, 27, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Andersson, T.L.; Stehle, B.; Davidsson, B.; Hoglund, P. Bioavailability of estradiol from two matrix transdermal delivery systems: Menorest and Climara. Maturitas 2000, 34, 57–64. [Google Scholar] [CrossRef]
- Zhang, H.; Cui, D.; Wang, B.; Han, Y.H.; Balimane, P.; Yang, Z.; Sinz, M.; Rodrigues, A.D. Pharmacokinetic drug interactions involving 17alpha-ethinylestradiol: A new look at an old drug. Clin. Pharmacokinet. 2007, 46, 133–157. [Google Scholar] [CrossRef]
- Abrams, L.S.; Skee, D.M.; Natarajan, J.; Wong, F.A.; Anderson, G.D. Pharmacokinetics of a contraceptive patch (Evra/Ortho Evra) containing norelgestromin and ethinyloestradiol at four application sites. Br. J. Clin. Pharmacol. 2002, 53, 141–146. [Google Scholar] [CrossRef]
- Dittrich, R.; Parker, L.; Rosen, J.B.; Shangold, G.; Creasy, G.W.; Fisher, A.C.; Ortho Evra/Evra 001 Study, G. Transdermal contraception: Evaluation of three transdermal norelgestromin/ethinyl estradiol doses in a randomized, multicenter, dose-response study. Am. J. Obstet. Gynecol. 2002, 186, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Bhasin, S.; Brito, J.P.; Cunningham, G.R.; Hayes, F.J.; Hodis, H.N.; Matsumoto, A.M.; Snyder, P.J.; Swerdloff, R.S.; Wu, F.C.; Yialamas, M.A. Testosterone Therapy in Men with Hypogonadism: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2018, 103, 1715–1744. [Google Scholar] [CrossRef] [PubMed]
- Dobs, A.S.; Meikle, A.W.; Arver, S.; Sanders, S.W.; Caramelli, K.E.; Mazer, N.A. Pharmacokinetics, efficacy, and safety of a permeation-enhanced testosterone transdermal system in comparison with bi-weekly injections of testosterone enanthate for the treatment of hypogonadal men. J. Clin. Endocrinol. Metab. 1999, 84, 3469–3478. [Google Scholar] [CrossRef] [PubMed]
- Raynaud, J.P.; Aumonier, C.; Gualano, V.; Betea, D.; Beckers, A. Pharmacokinetic study of a new testosterone-in-adhesive matrix patch applied every 2 days to hypogonadal men. J. Steroid Biochem. Mol. Biol. 2008, 109, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Priano, L.; Gasco, M.R.; Mauro, A. Transdermal treatment options for neurological disorders: Impact on the elderly. Drugs Aging 2006, 23, 357–375. [Google Scholar] [CrossRef]
- Verghese, C.; Abdijadid, S. Methylphenidate. In StatPearls; NCBI Bookshelf: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kimko, H.C.; Cross, J.T.; Abernethy, D.R. Pharmacokinetics and clinical effectiveness of methylphenidate. Clin. Pharmacokinet. 1999, 37, 457–470. [Google Scholar] [CrossRef] [PubMed]
- Pierce, D.; Dixon, C.M.; Wigal, S.B.; McGough, J.J. Pharmacokinetics of methylphenidate transdermal system (MTS): Results from a laboratory classroom study. J. Child Adolesc. Psychopharmacol. 2008, 18, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Frampton, J.E. Rotigotine Transdermal Patch: A Review in Parkinson’s Disease. CNS Drugs 2019, 33, 707–718. [Google Scholar] [CrossRef]
- Elshoff, J.P.; Braun, M.; Andreas, J.O.; Middle, M.; Cawello, W. Steady-state plasma concentration profile of transdermal rotigotine: An integrated analysis of three, open-label, randomized, phase I multiple dose studies. Clin. Ther. 2012, 34, 966–978. [Google Scholar] [CrossRef]
- Elshoff, J.P.; Cawello, W.; Andreas, J.O.; Mathy, F.X.; Braun, M. An update on pharmacological, pharmacokinetic properties and drug-drug interactions of rotigotine transdermal system in Parkinson’s disease and restless legs syndrome. Drugs 2015, 75, 487–501. [Google Scholar] [CrossRef] [PubMed]
- Chrisp, P.; Mammen, G.J.; Sorkin, E.M. Selegiline. A review of its pharmacology, symptomatic benefits and protective potential in Parkinson’s disease. Drugs Aging 1991, 1, 228–248. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, I. Clinical pharmacokinetics and pharmacodynamics of selegiline. An update. Clin. Pharmacokinet. 1997, 33, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.S.; Hochadel, T.J.; Morales, R.J.; Rohatagi, S.; DeWitt, K.E.; Watson, S.K.; DiSanto, A.R. Pharmacokinetics and safety of a selegiline transdermal system relative to single-dose oral administration in the elderly. Am. J. Ther. 1996, 3, 688–698. [Google Scholar] [CrossRef]
- Frampton, J.E.; Plosker, G.L. Selegiline transdermal system: In the treatment of major depressive disorder. Drugs 2007, 67, 257–265. [Google Scholar] [CrossRef]
- Birks, J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database Syst. Rev. 2006, 2006, CD005593. [Google Scholar] [CrossRef]
- Marucci, G.; Buccioni, M.; Ben, D.D.; Lambertucci, C.; Volpini, R.; Amenta, F. Efficacy of acetylcholinesterase inhibitors in Alzheimer’s disease. Neuropharmacology 2021, 190, 108352. [Google Scholar] [CrossRef]
- Rogers, S.L.; Friedhoff, L.T. Pharmacokinetic and pharmacodynamic profile of donepezil HCl following single oral doses. Br. J. Clin. Pharmacol. 1998, 46 (Suppl. 1), 1–6. [Google Scholar] [CrossRef]
- Bickel, U.; Thomsen, T.; Weber, W.; Fischer, J.P.; Bachus, R.; Nitz, M.; Kewitz, H. Pharmacokinetics of galanthamine in humans and corresponding cholinesterase inhibition. Clin. Pharmacol. Ther. 1991, 50, 420–428. [Google Scholar] [CrossRef]
- Farlow, M.R. Clinical pharmacokinetics of galantamine. Clin. Pharmacokinet. 2003, 42, 1383–1392. [Google Scholar] [CrossRef]
- Ameen, D.; Michniak-Kohn, B. Development and in vitro evaluation of pressure sensitive adhesive patch for the transdermal delivery of galantamine: Effect of penetration enhancers and crystallization inhibition. Eur. J. Pharm. Biopharm. 2019, 139, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Nasrollahzadeh, M.; Ganji, F.; Taghizadeh, S.M.; Vasheghani-Farahani, E.; Mohiti-Asli, M. Drug in adhesive transdermal patch containing antibiotic-loaded solid lipid nanoparticles. J. Biosci. Bioeng. 2022, 134, 471–476. [Google Scholar] [CrossRef]
- Altun, E.; Yuca, E.; Ekren, N.; Kalaskar, D.M.; Ficai, D.; Dolete, G.; Ficai, A.; Gunduz, O. Kinetic Release Studies of Antibiotic Patches for Local Transdermal Delivery. Pharmaceutics 2021, 13, 613. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Vora, L.K.; Kelly, S.A.; Li, L.; Larraneta, E.; McCarthy, H.O.; Donnelly, R.F. Hydrogel-forming microarray patch mediated transdermal delivery of tetracycline hydrochloride. J. Control. Release 2023, 356, 196–204. [Google Scholar] [CrossRef]
- Ramadon, D.; Permana, A.D.; Courtenay, A.J.; McCrudden, M.T.C.; Tekko, I.A.; McAlister, E.; Anjani, Q.K.; Utomo, E.; McCarthy, H.O.; Donnelly, R.F. Development, Evaluation, and Pharmacokinetic Assessment of Polymeric Microarray Patches for Transdermal Delivery of Vancomycin Hydrochloride. Mol. Pharm. 2020, 17, 3353–3368. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Advantages | Disadvantages |
|---|---|
| Continuous dosing, multi-day treatment | Limited type of medication |
| Bypass the digestive system | Skin irritation |
| Avoid first-pass metabolism | Inconsistent absorption |
| Can be terminated anytime | Patch failure |
| Less invasive | Limited dosing option |
| Drugs | Indication | Product Name | Duration of Application | Reference |
|---|---|---|---|---|
| Asenapine | Mania, bipolar disorder | Secuado® | 24 h | [8,9] |
| Bisoprolol | Atrial fibrillation | Bisono® | 24 h | [10] |
| Buprenorphine | Management of pain | Butrans® | 7 days | [11,12,13] |
| Clonidine | Hypertension, Tic disorder, Tourette syndrome, Attention deficit hyperactivity disorder (ADHD) | Catapres-TTS® | 7 days | [14,15,16,17,18] |
| Dextroamphetamine | ADHD | Xelstrym® | Up to 9 h | [19] |
| Donepezil | Alzheimer disease | Adlarity® | 7 days | [20,21] |
| Estrogen | Postmenstrual syndrome | Fematrix® | 7 days | [22,23] |
| Ethinyl Estradiol | Prevent pregnancy | Ortho Evra® | 7 days | [24,25] |
| Fentanyl | Moderate/severe pain | Duragesic® | 72 hours | [26] |
| Granisetron | Anti-emetic | Sancuso® | Up to 7 days | [27,28,29] |
| Levonorgestrel, Estradiol | Postmenstrual syndrome | Climara Pro® | 7 days | [30,31] |
| Lidocaine | Treatment of pain | Lidoderm® Dermalid® | up to 3 times daily for no more than 12 hours | [32,33] |
| Methylphenidate | ADHD | Daytrana® | Up to 9 days | [34] |
| Nicotine | Smoking cessation | Habitrol®, Nicoderm® Nicoderm CQ® Nicorette® | 24 h 16 h | [35,36,37] |
| Nitroglycerin | Angina pectoris Relieve pain after surgery | Minitran® Nitro-dur® | 12–14 h | [38,39,40,41] |
| Norethindrone Estradiol | Symptoms of menopause | Combipatch® | 3–4 days | [42] |
| Oxybutynin | Overactive bladder | Oxytrol® | 3–4 days | [43,44] |
| Rivastigmine | Alzheimer disease | Exelon® | 24 h | [45,46] |
| Rotigotine | Parkinson’s disease | Neupro® | 24 h | [47] |
| Selegiline | Depression | Emsam® | 24 h | [48] |
| Scopolamine | Motion sickness | Transderm-scop® | 72 h | [49,50] |
| Testosterone | Hypogonadism in males | Androderm® | 24 h | [51,52] |
| 17-β-Estradiol | Postmenstrual syndrome and osteoporosis | Alora® Climara® Estraderm® Vivelle-Dot ® Vivella® Menostar® Minivelle® | 3–4 days 7 days 3–4 days 3–4 days 3–4 days 7 days 3–4 days | [53,54,55] |
| Type | Material | Structure | Use | Dose | Delivery Rate | References |
|---|---|---|---|---|---|---|
| Solid | Silicon, Metal, Polymer | Simple | Can be reuse | Small dose | Fast | [57,58,59] |
| Hollow | Silicon | Simple | Can be reuse | Large dose | Fast | [60,61,62,63] |
| Coated | Polymer, Sugar, Lipids | Complex | Single | More precise dosing | Fast | [64,65,66,67] |
| Dissolving | Polymer | Complex | Single | More precise dosing | Slow | [68,69,70,71] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, W.F.; Ang, K.P.; Sethi, G.; Looi, C.Y. Recent Advancement of Medical Patch for Transdermal Drug Delivery. Medicina 2023, 59, 778. https://doi.org/10.3390/medicina59040778
Wong WF, Ang KP, Sethi G, Looi CY. Recent Advancement of Medical Patch for Transdermal Drug Delivery. Medicina. 2023; 59(4):778. https://doi.org/10.3390/medicina59040778
Chicago/Turabian StyleWong, Won Fen, Kuan Ping Ang, Gautam Sethi, and Chung Yeng Looi. 2023. "Recent Advancement of Medical Patch for Transdermal Drug Delivery" Medicina 59, no. 4: 778. https://doi.org/10.3390/medicina59040778
APA StyleWong, W. F., Ang, K. P., Sethi, G., & Looi, C. Y. (2023). Recent Advancement of Medical Patch for Transdermal Drug Delivery. Medicina, 59(4), 778. https://doi.org/10.3390/medicina59040778