
Sustained Remission Off-Treatment (SROT) of TPO-RAs: The Burgos Ten-Step Eltrombopag Tapering Scheme



Abstract
1. Introduction
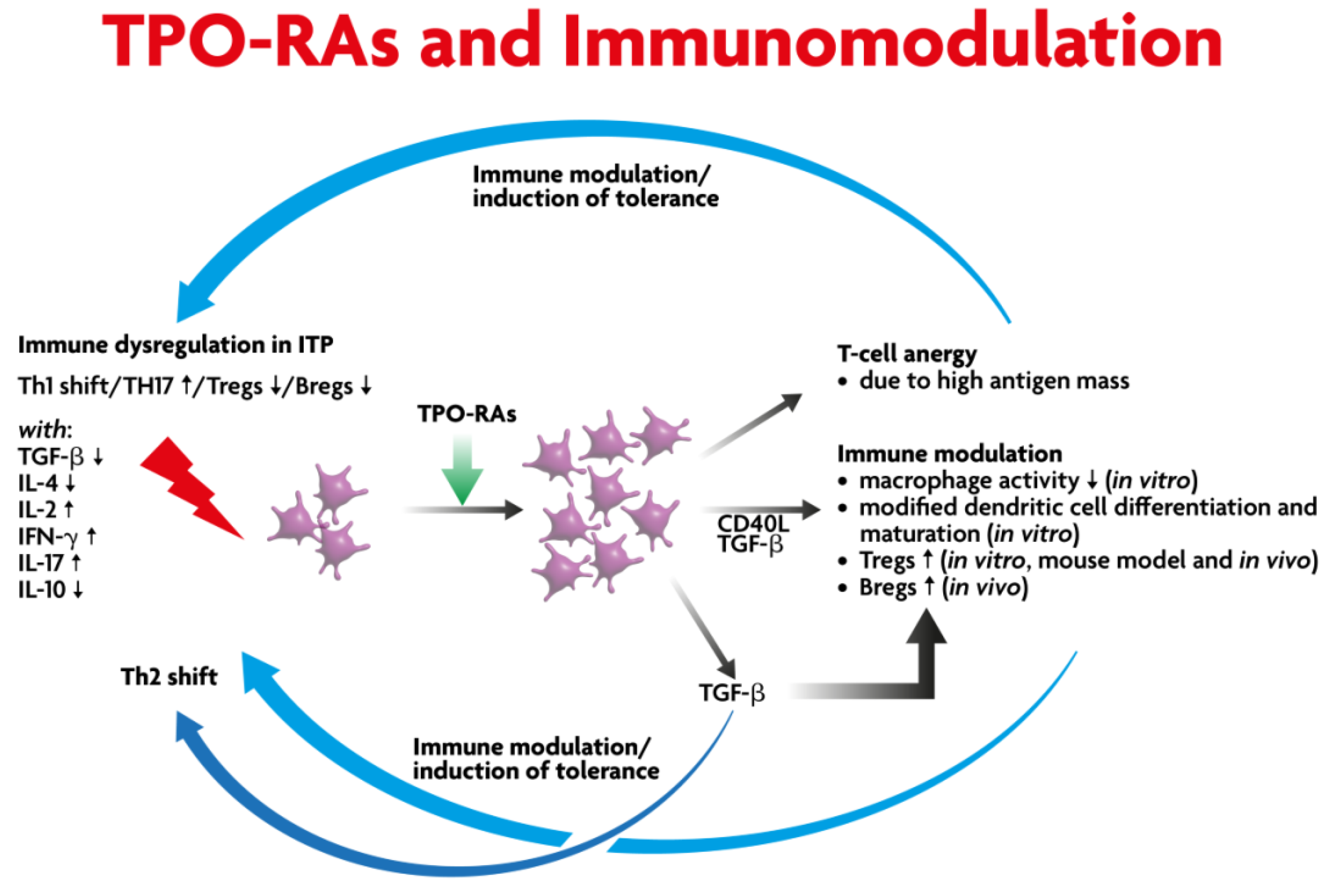
2. Biological Basis for Discontinuation of TPO-RAs
3. Tapering and SROT TPO-RAs: Major Publications, Clinical Approach to TPO-RA Discontinuation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuter, D.J.; Rummel, M.; Boccia, R.; Macik, B.G.; Pabinger, I.; Selleslag, D.; Rodeghiero, F.; Chong, B.H.; Wang, X.; Berger, D.P. Romiplostim or Standard of Care in Patients with Immune Thrombocytopenia. N. Engl. J. Med. 2010, 363, 1889–1899. [Google Scholar] [CrossRef] [PubMed]
- Cheng, G.; Saleh, M.N.; Marcher, C.; Vasey, S.; Mayer, B.; Aivado, M.; Arning, M.; Stone, N.L.; Bussel, J.B. Eltrombopag for management of chronic immune thrombocytopenia (RAISE): A 6-month, randomised, phase 3 study. Lancet 2011, 377, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.S.M.; Saleh, M.N.; Khelif, A.; Salama, A.; Portella, M.S.O.; Burgess, P.; Bussel, J.B. Safety and efficacy of long-term treatment of chronic/persistent ITP with eltrombopag: Final results of the EXTEND study. Blood 2017, 130, 2527–2536. [Google Scholar] [CrossRef]
- Jurczak, W.; Chojnowski, K.; Mayer, J.; Krawczyk, K.; Jamieson, B.D.; Tian, W.; Allen, L.F. Phase 3 randomised study of avatrombopag, a novel thrombopoietin receptor agonist for the treatment of chronic immune thrombocytopenia. Br. J. Haematol. 2018, 183, 479–490. [Google Scholar] [CrossRef]
- Bussel, J.B.; Kuter, D.J.; George, J.N.; McMillan, R.; Aledort, L.M.; Conklin, G.T.; Lichtin, A.E.; Lyons, R.M.; Nieva, J.; Wasser, J.S.; et al. AMG 531, a Thrombopoiesis-Stimulating Protein, for Chronic ITP. N. Engl. J. Med. 2006, 355, 1672–1681. [Google Scholar] [CrossRef] [PubMed]
- Newland, A.; Godeau, B.; Priego, V.; Viallard, J.-F.; Fernández, M.F.L.; Orejudos, A.; Eisen, M. Remission and platelet responses with romiplostim in primary immune thrombocytopenia: Final results from a phase 2 study. Br. J. Haematol. 2015, 172, 262–273. [Google Scholar] [CrossRef]
- Mahévas, M.; Fain, O.; Ebbo, M.; Roudot-Thoraval, F.; Limal, N.; Khellaf, M.; Schleinitz, N.; Bierling, P.; Languille, L.; Godeau, B.; et al. The temporary use of thrombopoietin-receptor agonists may induce a prolonged remission in adult chronic immune thrombocytopenia. Results of a French observational study. Br. J. Haematol. 2014, 165, 865–869. [Google Scholar] [CrossRef]
- González-López, T.J.; Pascual, C.; Álvarez-Román, M.T.; Fernández-Fuertes, F.; Sánchez-González, B.; Caparrós, I.; Jarque, I.; Mingot-Castellano, M.E.; Hernández-Rivas, J.A.; Martín-Salces, M.; et al. Successful discontinuation of eltrombopag after complete remission in patients with primary immune thrombocytopenia. Am. J. Hematol. 2015, 90, E40–E43. [Google Scholar] [CrossRef]
- Lucchini, E.; Palandri, F.; Volpetti, S.; Vianelli, N.; Auteri, G.; Rossi, E.; Patriarca, A.; Carli, G.; Barcellini, W.; Celli, M.; et al. Eltrombopag second-line therapy in adult patients with primary immune thrombocytopenia in an attempt to achieve sustained remission off-treatment: Results of a phase II, multicentre, prospective study. Br. J. Haematol. 2021, 193, 386–396. [Google Scholar] [CrossRef]
- Zaja, F.; Carpenedo, M.; Baratè, C.; Borchiellini, A.; Chiurazzi, F.; Finazzi, G.; Lucchesi, A.; Palandri, F.; Ricco, A.; Santoro, C.; et al. Tapering and discontinuation of thrombopoietin receptor agonists in immune thrombocytopenia: Real-world recommendations. Blood Rev. 2019, 41, 100647. [Google Scholar] [CrossRef]
- Palandri, F.; Rossi, E.; Bartoletti, D.; Ferretti, A.; Ruggeri, M.; Lucchini, E.; Carrai, V.; Barcellini, W.; Patriarca, A.; Rivolti, E.; et al. Real-world use of thrombopoietin receptor agonists in older patients with primary immune thrombocytopenia. Blood 2021, 138, 571–583. [Google Scholar] [CrossRef] [PubMed]
- Mahevas, M.; Guillet, S.; Viallard, J.-F.; Gobert, D.; Malphettes, M.; Cheze, S.; Lefrere, F.; Audia, S.; Bonnotte, B.; Lambotte, O.; et al. Rate of Prolonged Response after Stopping Thrombopoietin-Receptor Agonists Treatment in Primary Immune Thrombocytopenia (ITP): Results from a Nationwide Prospective Multicenter Interventional Study (STOPAGO). Blood 2021, 138, 583. [Google Scholar] [CrossRef]
- Cooper, N.; Ghanima, W.; Vianelli, N.; Valcárcel, D.; Yavaşoğlu, I.; Melikyan, A.; Eduardo Yañez Ruiz, E.; Jens Haenig, J.; James Lee, J.; Joan Maier, J.; et al. Sustained response off treatment in eltrombopag-treated patients with itp who are refractory or relapsed after first-line steroids: Primary analysis of the phase ii taper trial. Hemasphere 2022, 6, 193–194. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Kuter, D.J. Optimal use of thrombopoietin receptor agonists in immune thrombocytopenia. Ther. Adv. Hematol. 2019, 10, 2040620719841735. [Google Scholar] [CrossRef] [PubMed]
- Mingot-Castellano, M.E.; Román, M.T.; Fuertes, L.F.F.; González-López, T.J.; De Castro, J.M.G.; Jarque, I.; López-Fernández, M.F.; Lozano, M.L.; González, B.S.; Ferreiras, D.V.; et al. Management of Adult Patients with Primary Immune Thrombocytopenia (ITP) in Clinical Practice: A Consensus Approach of the Spanish ITP Expert Group. Adv. Hematol. 2019, 2019, 4621416. [Google Scholar] [CrossRef]
- Cooper, N.; Hill, Q.A.; Grainger, J.; Westwood, J.-P.; Bradbury, C.; Provan, D.; Thachil, J.; Ramscar, N.; Roy, A. Tapering and Discontinuation of Thrombopoietin Receptor Agonist Therapy in Patients with Immune Thrombocytopenia: Results from a Modified Delphi Panel. Acta Haematol. 2021, 144, 418–426. [Google Scholar] [CrossRef]
- Carpenedo, M.; Baldacci, E.; Baratè, C.; Borchiellini, A.; Buccisano, F.; Calvaruso, G.; Chiurazzi, F.; Fattizzo, B.; Giuffrida, G.; Rossi, E.; et al. Second-line administration of thrombopoietin receptor agonists in immune thrombocytopenia: Italian Delphi-based consensus recommendations. Ther. Adv. Hematol. 2021, 12, 20406207211048361. [Google Scholar] [CrossRef]
- Wang, B.; Nichol, J.L.; Sullivan, J.T. Pharmacodynamics and pharmacokinetics of AMG 531, a novel thrombopoietin receptor ligand. Clin. Pharmacol. Ther. 2004, 76, 628–638. [Google Scholar] [CrossRef]
- Bao, W.; Bussel, J.B.; Heck, S.; He, W.; Karpoff, M.; Boulad, N.; Yazdanbakhsh, K. Improved regulatory T-cell activity in patients with chronic immune thrombocytopenia treated with thrombopoietic agents. Blood 2010, 116, 4639–4645. [Google Scholar] [CrossRef]
- Schifferli, A.; Kühne, T. Thrombopoietin receptor agonists: A new immune modulatory strategy in immune thrombocytopenia? Semin. Hematol. 2016, 53 (Suppl. S1), S31–S34. [Google Scholar] [CrossRef]
- Liu, X.G.; Liu, S.; Feng, Q.; Liu, X.-N.; Li, G.-S.; Sheng, Z.; Chen, P.; Liu, Y.; Wei, Y.; Dong, X.-Y.; et al. Thrombopoietin receptor agonists shift the balance of Fcγ receptors toward inhibitory receptor IIb on monocytes in ITP. Blood 2016, 128, 852–861. [Google Scholar] [CrossRef] [PubMed]
- Semple, J.W.; Rebetz, J.; Maouia, A.; Kapur, R. An update on the pathophysiology of immune thrombocytopenia. Curr. Opin. Hematol. 2020, 27, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Audia, S.; Mahévas, M.; Nivet, M.; Ouandji, S.; Ciudad, M.; Bonnotte, B. Immune Thrombocytopenia: Recent Advances in Pathogenesis and Treatments. Hemasphere 2021, 5, e574. [Google Scholar] [CrossRef] [PubMed]
- Swinkels, M.; Rijkers, M.; Voorberg, J.; Vidarsson, G.; Leebeek, F.W.G.; Jansen, A.J.G. Emerging Concepts in Immune Thrombocytopenia. Front. Immunol. 2018, 9, 880. [Google Scholar] [CrossRef]
- Zufferey, A.; Kapur, R.; Semple, J.W. Pathogenesis and Therapeutic Mechanisms in Immune Thrombocytopenia (ITP). J. Clin. Med. 2017, 6, 16. [Google Scholar] [CrossRef]
- Semple, J.W.; Milev, Y.; Cosgrave, D.; Mody, M.; Hornstein, A.; Blanchette, V.; Freedman, J. Differences in serum cytokine levels in acute and chronic autoimmune thrombocytopenic purpura: Relationship to platelet phenotype and antiplatelet T-cell reactivity. Blood 1996, 87, 4245–4254. [Google Scholar] [CrossRef]
- Sakakura, M.; Wada, H.; Tawara, I.; Nobori, T.; Sugiyama, T.; Sagawa, N.; Shiku, H. Reduced Cd4+Cd25+ T cells in patients with idiopathic thrombocytopenic purpura. Thromb. Res. 2007, 120, 187–193. [Google Scholar] [CrossRef]
- Stasi, R.; Cooper, N.; Del Poeta, G.; Stipa, E.; Evangelista, M.L.; Abruzzese, E.; Amadori, S. Analysis of regulatory T-cell changes in patients with idiopathic thrombocytopenic purpura receiving B cell–depleting therapy with rituximab. Blood 2008, 112, 1147–1150. [Google Scholar] [CrossRef]
- Yu, J.; Heck, S.; Patel, V.; LeVan, J.; Yu, Y.; Bussel, J.B.; Yazdanbakhsh, K. Defective circulating CD25 regulatory T cells in patients with chronic immune thrombocytopenic purpura. Blood 2008, 112, 1325–1328. [Google Scholar] [CrossRef]
- Olsson, B.; Ridell, B.; Carlsson, L.; Jacobsson, S.; Wadenvik, H. Recruitment of T cells into bone marrow of ITP patients possibly due to elevated expression of VLA-4 and CX3CR1. Blood 2008, 112, 1078–1084. [Google Scholar] [CrossRef]
- Houwerzijl, E.J.; Blom, N.R.; van der Want, J.; Esselink, M.T.; Koornstra, J.J.; Smit, J.W.; Louwes, H.; Vellenga, E.; De Wolf, J.T.M. Ultrastructural study shows morphologic features of apoptosis and para-apoptosis in megakaryocytes from patients with idiopathic thrombocytopenic purpura. Blood 2004, 103, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Kuter, D.J.; Newland, A.; Chong, B.H.; Rodeghiero, F.; Romero, M.T.; Pabinger, I.; Chen, Y.; Wang, K.; Mehta, B.; Eisen, M. Romiplostim in adult patients with newly diagnosed or persistent immune thrombocytopenia (ITP) for up to 1 year and in those with chronic ITP for more than 1 year: A subgroup analysis of integrated data from completed romiplostim studies. Br. J. Haematol. 2019, 185, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.Y.; Flavell, R.A. ‘Yin-Yang’ functions of transforming growth factor-beta and T regulatory cells in immune regulation. Immunol. Rev. 2007, 220, 199–213. [Google Scholar] [CrossRef]
- Nagahama, M.; Nomura, S.; Kanazawa, S.; Ozaki, Y.; Kagawa, H.; Fukuhara, S. Significance of chemokines and soluble CD40 ligand in patients with autoimmune thrombocytopenic purpura. Eur. J. Haematol. 2002, 69, 303–308. [Google Scholar] [CrossRef]
- Guilliams, M.; Bruhns, P.; Saeys, Y.; Hammad, H.; Lambrecht, B.N. The function of Fcγ receptors in dendritic cells and macrophages. Nat. Rev. Immunol. 2014, 14, 94–108. [Google Scholar] [CrossRef] [PubMed]
- Directrices de diagnóstico, tratamiento y seguimiento de la PTI. Recomendaciones del Grupo de Trabajo de la SEHH y GEPTI. Año 2020. Available online: https://www.gepti.es/images/stories/recursos/2022/02/GUIA-PTI-2021.pdf (accessed on 7 February 2023).
- Schifferli, A.; Rüfer, A.; Rovo, A.; Cantoni, N.; Holbro, A.; Favre, G.; Faeth, H.; Pereira, R.R.; Wieland, A.; Dirks, J.; et al. Immunomodulation with Romiplostim in Young Adult Primary Immune Thrombocytopenia (ITP) As Second-Line Strategy (iROM-study). Blood 2021, 138, 3149. [Google Scholar] [CrossRef]
- Novartis. Revolade (eltrombopag) [prescribing information]. Official EMA datasheet, 2020. Available online: https://cima.aemps.es/cima/dochtml/ft/10612005/FichaTecnica_10612005.html (accessed on 7 February 2023).
- Moulis, G.; Bagheri, H.; Sailler, L.; Jonville-Bera, A.P.; Weber, E.; Guy, C.; Petitpain, N.; Laroche, M.L.; Favrelière, S.; Béné, J.; et al. Are adverse drug reaction patterns different between romiplostim and eltrombopag? 2009–2013 French PharmacoVigilance assessment. Eur. J. Intern. Med. 2014, 25, 777–780. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Kuter, D.J. Antiplatelet Antibody Testing in Immune Thrombocytopenia and Evans Syndrome: Longitudinal Serologic Evolution and Relation to Clinical Features. Blood 2018, 132, 1137. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Rosovsky, R.P.; Leaf, R.S.K.; Smith, D.B.; Goodarzi, K.; Fogerty, A.E.; Sykes, D.B.; Kuter, D.J. A modern reassessment of glycoprotein-specific direct platelet autoantibody testing in immune thrombocytopenia. Blood Adv. 2019, 4, 9–18. [Google Scholar] [CrossRef]
- Hollenhorst, M.A.; Al-Samkari, H.; Kuter, D.J. Markers of autoimmunity in immune thrombocytopenia: Prevalence and prognostic significance. Blood Adv. 2019, 3, 3515–3521. [Google Scholar] [CrossRef]


{kind=link}
| Number of Patients Primarily Treated (n) | SROT Rate | Follow-Up Time (Months) | Type of TPO-RA Used | Median Number of Previous Treatments | Mean Time of TPO-RA Treatment before Tapering | Median Minimum Platelet Count at Tapering Initiation | Biological Investigation to Support Tapering (Yes/No) | |
|---|---|---|---|---|---|---|---|---|
| Newland A, et al. (2016) [6] | 98 | 21.3% (16/75) | 6 months | Romiplostim | One | ≤12 months | ≥50 × 109/L | No |
| Mahévas M, et al. (2014) [7] | 54 | 50% (14/28) | 13.5 months | Romiplostim and/or Eltrombopag | Six | 5 years | ≥300 × 109/L | No |
| González-López TJ, et al. (2015) [8] | 260 | 53.1% (26/49) | 9 months | Eltrombopag | Four | 46.5 months | ≥100 × 109/L | No |
| Lucchini E, et al. (2021) [9] | 51 | 25% (13/51) | 24 weeks | Eltrombopag | One | 6 months | ≥30 × 109/L | Yes |
| Palandri, et al. (2021) [11] | 390 | 16.5% (62/384) | 9.6 years | Romiplostim or Eltrombopag | Not available | 0.9 years | Not available | No |
| Mahevas M, et al. (2021) [12] | 49 | 56.2% (27/48) | 6 months | Romiplostim or Eltrombopag | Two | 1.6 years | 291 × 109/L | Yes |
| Cooper N, et al. (2022) [13] | 105 | 41.9% (44/105) | 2 years | Eltrombopag | One | 4 months | ≥70 × 109/L | No |
| First step (7 days-treatment) | 50–50–25–50–50–25–50 (mg per day) |
| Second step (7 days-treatment) | 50–25–25–50–25–25–50 (mg per day) |
| Third step (7 days-treatment) | 25/24 hs (mg per day) |
| Fourth step (7 days-treatment) | 25–25–0–25–25–0–25 (mg per day) |
| Fifth step (7 days-treatment) | 25–0–0–25–0–0–25 (mg per day) |
| Sixth step (7 days-treatment) | 25–0–0–0–25–0–0 (mg per day) |
| Seventh step (7 days-treatment) | 25–0–0–0–0–12.5–0 (mg per day) |
| Eighth step (7 days-treatment) | 25–0–0–0–0–0–0 (mg per day) |
| Ninth step (7 days-treatment) | 12.5–0–0–0–0–0–0 (mg per day) |
| Tenth step (7 days-treatment) | No TPO-RA treatment |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-López, T.J.; Provan, D. Sustained Remission Off-Treatment (SROT) of TPO-RAs: The Burgos Ten-Step Eltrombopag Tapering Scheme. Medicina 2023, 59, 659. https://doi.org/10.3390/medicina59040659
González-López TJ, Provan D. Sustained Remission Off-Treatment (SROT) of TPO-RAs: The Burgos Ten-Step Eltrombopag Tapering Scheme. Medicina. 2023; 59(4):659. https://doi.org/10.3390/medicina59040659
Chicago/Turabian StyleGonzález-López, Tomás José, and Drew Provan. 2023. "Sustained Remission Off-Treatment (SROT) of TPO-RAs: The Burgos Ten-Step Eltrombopag Tapering Scheme" Medicina 59, no. 4: 659. https://doi.org/10.3390/medicina59040659
APA StyleGonzález-López, T. J., & Provan, D. (2023). Sustained Remission Off-Treatment (SROT) of TPO-RAs: The Burgos Ten-Step Eltrombopag Tapering Scheme. Medicina, 59(4), 659. https://doi.org/10.3390/medicina59040659