
The Top Three Burning Questions in Total Hip Arthroplasty


 ,
, {kind=link}
Abstract
1. Introduction
2. Significance of Present Review: Discussing three Burning Topics/Questions in THA
- Are new technologies (robotic or navigated systems) better than conventional THA?
- How important is spinopelvic mobility for THA?
- Is fast-track THA surgery beneficial and who is the ideal candidate for it?
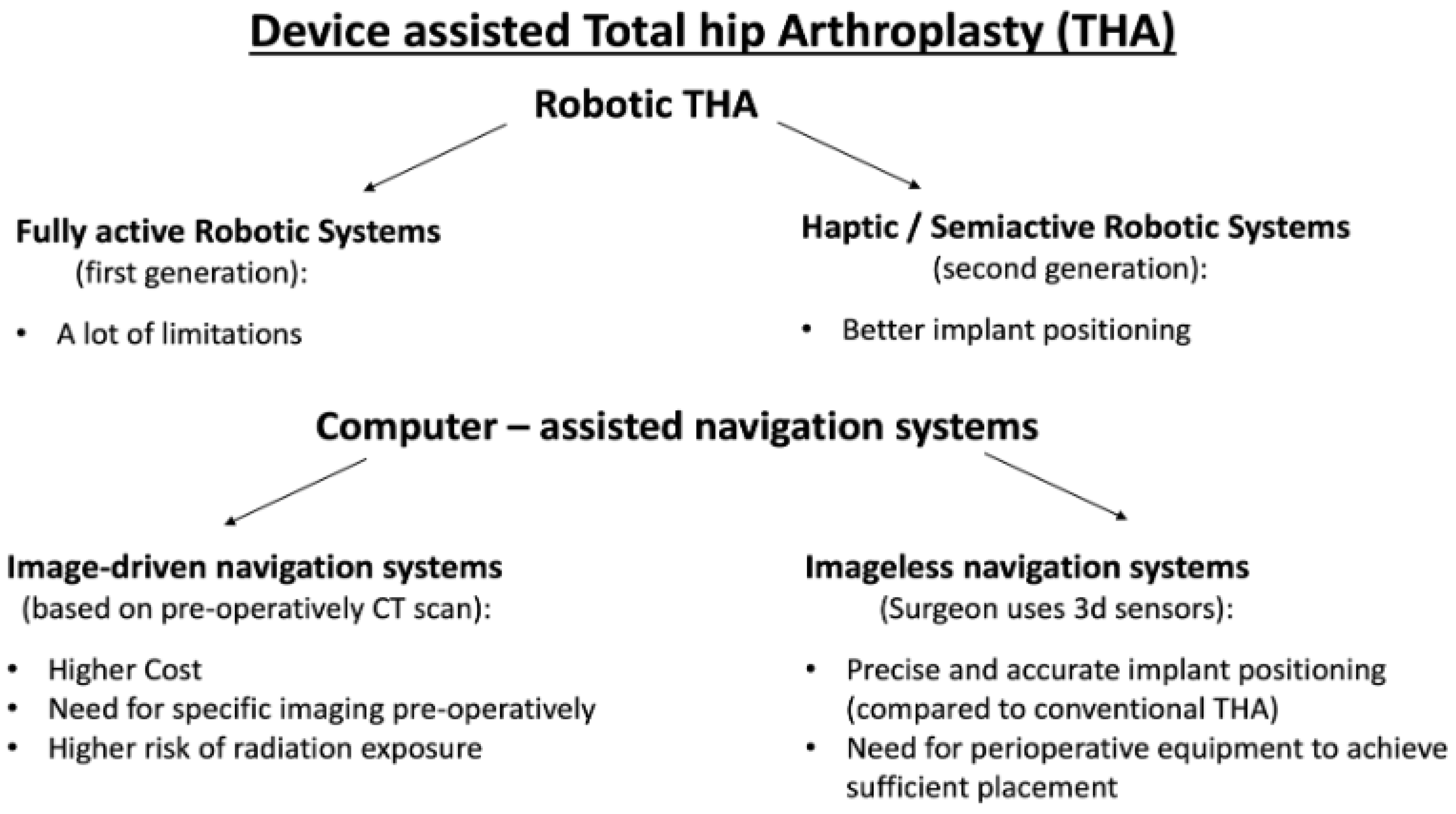
3. Device-Assisted THA Versus Conventional THA
- A.
- Robotic Systems in THA
- B.
- Semiactive Robotic Systems
- C.
- Navigation Systems in THA
4. Spinopelvic Mobility
5. Fast-Track Protocols in THA
6. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Law, W.A. Post-operative study of vitallium mould arthroplasty of the hip joint. J. Bone Joint Surg. Br. 1948, 30B, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Smith-Petersen, M.N. The classic: Evolution of mould arthroplasty of the hip joint by M. N. Smith-Petersen, J. Bone Joint Surg. 30B:L:59, 1948. Clin. Orthop. Relat. Res. 1978, 134, 5–11. [Google Scholar]
- Charnley, J. Anchorage of the femoral head prosthesis to the shaft of the femur. J. Bone Joint Surg. 1960, 42-B, 28–30. [Google Scholar] [CrossRef]
- Charnley, J. ARTHROPLASTY OF THE HIP A New Operation. Lancet 1961, 277, 1129–1132. [Google Scholar] [CrossRef] [PubMed]
- Shon, W.Y.; Park, B.-Y.; R, R.N.; Park, P.S.; Im, J.T.; Yun, H.H. Total Hip Arthroplasty: Past, Present, and Future. What Has Been Achieved? Hip Pelvis 2019, 31, 179–189. [Google Scholar] [CrossRef]
- Learmonth, I.D.; Young, C.; Rorabeck, C. The operation of the century: Total hip replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef]
- Mart, J.-P.S.; Goh, E.L.; Shah, Z. Robotics in total hip arthroplasty: A review of the evolution, application and evidence base. EFORT Open Rev. 2020, 5, 866–873. [Google Scholar] [CrossRef]
- Han, P.-F.; Chen, C.-L.; Zhang, Z.-L.; Han, Y.-C.; Wei, L.; Li, P.-C.; Wei, X.-C. Robotics-assisted versus conventional manual approaches for total hip arthroplasty: A systematic review and meta-analysis of comparative studies. Int. J. Med Robot. Comput Assist. Surg. 2019, 15, e1990. [Google Scholar] [CrossRef]
- Brady, A.W.; Tatka, J.; Fagotti, L.; Kemler, B.R.; Fossum, B.W. Accuracy and Reliability of Software Navigation for Acetabular Component Placement in THA: An In Vitro Validation Study. Medicina 2022, 58, 663. [Google Scholar] [CrossRef]
- Nakamura, N.; Sugano, N.; Nishii, T.; Kakimoto, A.; Miki, H. A Comparison between Robotic-assisted and Manual Implantation of Cementless Total Hip Arthroplasty. Clin. Orthop. Relat. Res. 2010, 468, 1072–1081. [Google Scholar] [CrossRef]
- Nakamura, N.; Sugano, N.; Sakai, T.; Nakahara, I. Does Robotic Milling For Stem Implantation in Cementless THA Result in Improved Outcomes Scores or Survivorship Compared with Hand Rasping? Results of a Randomized Trial at 10 Years. Clin. Orthop. Relat. Res. 2018, 476, 2169–2173. [Google Scholar] [CrossRef]
- Bargar, W.L.; Parise, C.A.; Hankins, A.; Marlen, N.A.; Campanelli, V.; Netravali, N.A. Fourteen Year Follow-Up of Randomized Clinical Trials of Active Robotic-Assisted Total Hip Arthroplasty. J. Arthroplast. 2018, 33, 810–814. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Xiong, J.; Wang, P.; Zhu, S.; Qi, W.; Peng, H.; Yu, L.; Qian, W. Robotic-assisted compared with conventional total hip arthroplasty: Systematic review and meta-analysis. Hear 2018, 94, 335–341. [Google Scholar] [CrossRef]
- Domb, B.G.; Chen, J.W.; Lall, A.C.; Perets, I.; Maldonado, D.R. Minimum 5-Year Outcomes of Robotic-assisted Primary Total Hip Arthroplasty With a Nested Comparison Against Manual Primary Total Hip Arthroplasty: A Propensity Score–Matched Study. J. Am. Acad. Orthop. Surg. 2020, 28, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Bukowski, B.R.; Anderson, P.; Khlopas, A.; Chughtai, M.; A Mont, M.; Illgen, R.I.L. Improved Functional Outcomes with Robotic Compared with Manual Total Hip Arthroplasty. Surg. Technol. Online 2016, 29, 303–308. [Google Scholar]
- Kort, N.; Stirling, P.; Pilot, P.; Müller, J.H. Clinical and surgical outcomes of robot-assisted versus conventional total hip arthroplasty: A systematic overview of meta-analyses. EFORT Open Rev. 2021, 6, 1157–1165. [Google Scholar] [CrossRef]
- Shaw, J.H.; Rahman, T.M.; Wesemann, L.D.; Jiang, C.Z.; Lindsay-Rivera, K.G.; Davis, J.J. Comparison of Postoperative Instability and Acetabular Cup Positioning in Robotic-Assisted Versus Traditional Total Hip Arthroplasty. J. Arthroplast. 2022, 37, S881–S889. [Google Scholar] [CrossRef]
- Guo, D.; Li, X.; Ma, S.; Zhao, Y.; Qi, C.; Xue, Y. Total Hip Arthroplasty with Robotic Arm Assistance for Precise Cup Positioning: A Case-Control Study. Orthop. Surg. 2022, 14, 1498–1505. [Google Scholar] [CrossRef] [PubMed]
- Fontalis, A.; Kayani, B.; Thompson, J.W.; Plastow, R.; Haddad, F.S. Robotic total hip arthroplasty: Past, present and future. Orthop. Trauma 2022, 36, 6–13. [Google Scholar] [CrossRef]
- Kayani, B.; Konan, S.; Ayuob, A.; Ayyad, S.; Haddad, F.S. The current role of robotics in total hip arthroplasty. EFORT Open Rev. 2019, 4, 618–625. [Google Scholar] [CrossRef]
- Caldora, P.; D’Urso, A.; Banchetti, R.; Arniani, S.; Colcelli, D.; Ciampalini, L.; Guastafierro, P.; Lup, D. Blood transfusion, hospital stay and learning curve in robotic assisted total hip arthroplasty. J. Biol. Regul. Homeost Agents 2020, 34 (Suppl. 3), 37–49, Congress of the Italian Orthopaedic Research Society. [Google Scholar] [PubMed]
- Remily, E.A.; Nabet, A.; Sax, O.C.; Douglas, S.J.; Pervaiz, S.S.; Delanois, R.E. Impact of Robotic Assisted Surgery on Outcomes in Total Hip Arthroplasty. Arthroplast. Today 2021, 9, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Kelley, T.C.; Swank, M.L. Role of Navigation in Total Hip Arthroplasty. J. Bone Joint. Surg Am. 2009, 91 (Suppl. 1), 153–158. [Google Scholar] [CrossRef] [PubMed]
- Kurmis, A.P. Advanced, Imageless Navigation in Contemporary THA: Optimising Acetabular Component Placement. In Arthroplasty—Advanced Techniques and Future Perspectives; IntechOpen: London, UK, 2022. [Google Scholar] [CrossRef]
- Zurmühle, C.A.; Zickmantel, B.; Christen, M.; Christen, B.; Zheng, G.; Schwab, J.M.; Tannast, M.; Steppacher, S.D. Image-Less THA Cup Navigation in Clinical Routine Setup: Individual Adjustments, Accuracy, Precision, and Robustness. Med. Kauicinas Lith. 2022, 58, 832. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, R.; Marchie, A.; Farrokhyar, F.; Mahomed, N. Computer navigation in total hip replacement: A meta-analysis. Int. Orthop. 2009, 33, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Lass, R.; Kubista, B.; Olischar, B.; Frantal, S.; Windhager, R.; Giurea, A. Total Hip Arthroplasty Using Imageless Computer-Assisted Hip Navigation: A prospective randomized study. J. Arthroplast. 2014, 29, 786–791. [Google Scholar] [CrossRef]
- Lass, R.; Olischar, B.; Kubista, B.; Waldhoer, T.; Giurea, A.; Windhager, R. Total Hip Arthroplasty Using Imageless Computer-Assisted Navigation—2-Year Follow-Up of a Prospective Randomized Study. J. Clin. Med. 2020, 9, 1620. [Google Scholar] [CrossRef]
- Snijders, T.; Van Gaalen, S.; De Gast, A. Precision and accuracy of imageless navigation versus freehand implantation of total hip arthroplasty: A systematic review and meta-analysis. Int. J. Med Robot. Comput. Assist. Surg. 2017, 13, e1843. [Google Scholar] [CrossRef]
- Maillot, C.; Harman, C.; Villet, L.; Cobb, J.; Rivière, C. Modern cup alignment techniques in total hip arthroplasty: A systematic review. Orthop. Traumatol. Surg. Res. 2019, 105, 907–913. [Google Scholar] [CrossRef]
- Migliorini, F.; Cuozzo, F.; Oliva, F.; Eschweiler, J.; Hildebrand, F.; Maffulli, N. Imageless navigation for primary total hip arthroplasty: A meta-analysis study. J. Orthop. Traumatol. Off. J. Ital. Soc. Orthop. Traumatol. 2022, 23, 1–11. [Google Scholar] [CrossRef]
- Singh, V.; Realyvasquez, J.; Simcox, T.; Rozell, J.C.; Schwarzkopf, R.; Davidovitch, R.I. Robotics Versus Navigation Versus Conventional Total Hip Arthroplasty: Does the Use of Technology Yield Superior Outcomes? J. Arthroplast. 2021, 36, 2801–2807. [Google Scholar] [CrossRef] [PubMed]
- Sweet, M.C.; Borrelli, G.J.; Manawar, S.S.; Miladore, N. Comparison of Outcomes After Robotic-Assisted or Conventional Total Hip Arthroplasty at a Minimum 2-Year Follow-up: A Systematic Review. JBJS Rev. 2021, 9. [Google Scholar] [CrossRef]
- Ogilvie, A.; Kim, W.J.; Asirvatham, R.D.; Fontalis, A.; Putzeys, P.; Haddad, F.S. Robotic-Arm-Assisted Total Hip Arthroplasty: A Review of the Workflow, Outcomes and Its Role in Addressing the Challenge of Spinopelvic Imbalance. Medicina 2022, 58, 1616. [Google Scholar] [CrossRef] [PubMed]
- Lum, Z.C.; Coury, J.G.; Cohen, J.L.; Dorr, L.D. The Current Knowledge on Spinopelvic Mobility. J. Arthroplast. 2018, 33, 291–296. [Google Scholar] [CrossRef]
- Eddine, T.A.; Migaud, H.; Chantelot, C.; Cotten, A.; Fontaine, C.; Duquennoy, A. Variations of pelvic anteversion in the lying and standing positions analysis of 24 control subjects and implications for CT measurement of position of a prosthetic cup. Surg. Radiol. Anat. 2001, 23, 105–110. [Google Scholar] [CrossRef]
- Phan, D.; Bederman, S.S.; Schwarzkopf, R. The influence of sagittal spinal deformity on anteversion of the acetabular component in total hip arthroplasty. Bone Jt. J. 2015, 97-B, 1017–1023. [Google Scholar] [CrossRef]
- Esposito, C.I.; Miller, T.T.; Kim, H.J.; Barlow, B.T.; Wright, T.M.; Padgett, D.E.; Jerabek, S.A.; Mayman, D.J. Does Degenerative Lumbar Spine Disease Influence Femoroacetabular Flexion in Patients Undergoing Total Hip Arthroplasty? Clin. Orthop. Relat. Res. 2016, 474, 1788–1797. [Google Scholar] [CrossRef]
- Malkani, A.L.; Garber, A.T.; Ong, K.L.; Dimar, J.R.; Baykal, D.; Glassman, S.D.; Cochran, A.R.; Berry, D.J. Total Hip Arthroplasty in Patients With Previous Lumbar Fusion Surgery: Are There More Dislocations and Revisions? J. Arthroplast. 2018, 33, 1189–1193. [Google Scholar] [CrossRef]
- Rajaee, S.S.; Bae, H.W.; Kanim, L.E.; Delamarter, R.B. Spinal Fusion in the United States: Analysis of trends from 1998 to 2008. Spine 2012, 37, 67–76. [Google Scholar] [CrossRef]
- Buckland, A.J.; Vigdorchik, J.; Schwab, F.J.; Errico, T.; Lafage, R.; Ames, C.; Bess, S.; Smith, J.; Mundis, G.M.; Lafage, V. Acetabular Anteversion Changes Due to Spinal Deformity Correction: Bridging the Gap Between Hip and Spine Surgeons. J. Bone Joint. Surg. Am. 2015, 97, 1913–1920. [Google Scholar] [CrossRef] [PubMed]
- Barrey, C.; Roussouly, P.; Le Huec, J.-C.; D’Acunzi, G.; Perrin, G. Compensatory mechanisms contributing to keep the sagittal balance of the spine. Eur. Spine J. 2013, 22 (Suppl. 6), s834–s841. [Google Scholar] [CrossRef] [PubMed]
- Ochi, H.; Baba, T.; Homma, Y.; Matsumoto, M.; Nojiri, H.; Kaneko, K. Importance of the spinopelvic factors on the pelvic inclination from standing to sitting before total hip arthroplasty. Eur. Spine J. 2016, 25, 3699–3706. [Google Scholar] [CrossRef] [PubMed]
- Eftekhary, N.; Shimmin, A.; Lazennec, J.Y.; Buckland, A.; Schwarzkopf, R.; Dorr, L.D.; Mayman, D.; Padgett, D.; Vigdorchik, J. A systematic approach to the hip-spine relationship and its applications to total hip arthroplasty. Bone Jt. J. 2019, 101-B, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Bozic, K.J.; Kurtz, S.M.; Lau, E.; Ong, K.; Vail, T.P.; Berry, D.J. The Epidemiology of Revision Total Hip Arthroplasty in the United States. J. Bone Joint Surg Am. 2009, 91, 128–133. [Google Scholar] [CrossRef]
- Abdel, M.P.; von Roth, P.; Jennings, M.T.; Hanssen, A.D.; Pagnano, M.W. What Safe Zone? The Vast Majority of Dislocated THAs Are Within the Lewinnek Safe Zone for Acetabular Component Position. Clin. Orthop. Relat. Res. 2016, 474, 386–391. [Google Scholar] [CrossRef]
- Esposito, C.I.; Gladnick, B.P.; Lee, Y.-Y.; Lyman, S.; Wright, T.M.; Mayman, D.J.; Padgett, D.E. Cup Position Alone Does Not Predict Risk of Dislocation After Hip Arthroplasty. J. Arthroplast. 2015, 30, 109–113. [Google Scholar] [CrossRef]
- Lewinnek, G.E.; Lewis, J.L.; Tarr, R.; Compere, C.L.; Zimmerman, J.R. Dislocations after total hip-replacement arthroplasties. J. Bone Jt. Surg.-Am. Vol. 1978, 60, 217–220. [Google Scholar] [CrossRef]
- Heckmann, N.; McKnight, B.; Stefl, M.; Trasolini, N.A.; Ike, H.; Dorr, L.D. Late Dislocation Following Total Hip Arthroplasty: Spinopelvic Imbalance as a Causative Factor. J. Bone Jt. Surg. 2018, 100, 1845–1853. [Google Scholar] [CrossRef]
- Vigdorchik, J.; Eftekhary, N.; Elbuluk, A.; Abdel, M.P.; Buckland, A.; Schwarzkopf, R.S.; Jerabek, S.A.; Mayman, D.J. Evaluation of the spine is critical in the workup of recurrent instability after total hip arthroplasty. Bone Jt. J. 2019, 101-B, 817–823. [Google Scholar] [CrossRef]
- Bedard, N.A.; Martin, C.T.; Slaven, S.E.; Pugely, A.J.; Mendoza-Lattes, S.A.; Callaghan, J.J. Abnormally High Dislocation Rates of Total Hip Arthroplasty After Spinal Deformity Surgery. J. Arthroplast. 2016, 31, 2884–2885. [Google Scholar] [CrossRef]
- Buckland, A.J.; Puvanesarajah, V.; Vigdorchik, J.; Schwarzkopf, R.; Jain, A.; Klineberg, E.O.; Hart, R.A.; Callaghan, J.J.; Hassanzadeh, H. Dislocation of a primary total hip arthroplasty is more common in patients with a lumbar spinal fusion. Bone Jt. J. 2017, 99-B, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Loh, J.L.M.; Jiang, L.; Chong, H.C.; Yeo, S.J.; Lo, N.N. Effect of Spinal Fusion Surgery on Total Hip Arthroplasty Outcomes: A Matched Comparison Study. J. Arthroplast. 2017, 32, 2457–2461. [Google Scholar] [CrossRef] [PubMed]
- Sing, D.C.; Barry, J.J.; Aguilar, T.U.; Theologis, A.A.; Patterson, J.T.; Tay, B.K.; Vail, T.P.; Hansen, E.N. Prior Lumbar Spinal Arthrodesis Increases Risk of Prosthetic-Related Complication in Total Hip Arthroplasty. J. Arthroplast. 2016, 31, 227–232.e1. [Google Scholar] [CrossRef]
- Gausden, E.B.; Parhar, H.S.; Popper, J.E.; Sculco, P.K.; Rush, B.N. Risk Factors for Early Dislocation Following Primary Elective Total Hip Arthroplasty. J. Arthroplast. 2018, 33, 1567–1571.e2. [Google Scholar] [CrossRef]
- An, V.V.; Phan, K.; Sivakumar, B.S.; Mobbs, R.J.; Bruce, W.J. Prior Lumbar Spinal Fusion is Associated With an Increased Risk of Dislocation and Revision in Total Hip Arthroplasty: A Meta-Analysis. J. Arthroplast. 2018, 33, 297–300. [Google Scholar] [CrossRef]
- Perfetti, D.C.; Schwarzkopf, R.; Buckland, A.; Paulino, C.B.; Vigdorchik, J. Prosthetic Dislocation and Revision After Primary Total Hip Arthroplasty in Lumbar Fusion Patients: A Propensity Score Matched-Pair Analysis. J. Arthroplast. 2017, 32, 1635–1640.e1. [Google Scholar] [CrossRef] [PubMed]
- Onggo, J.R.; Nambiar, M.; Onggo, J.D.; Phan, K.; Ambikaipalan, A.; Babazadeh, S.; Hau, R. Clinical outcomes and complication profile of total hip arthroplasty after lumbar spine fusion: A meta-analysis and systematic review. Eur. Spine J. 2019, 29, 282–294. [Google Scholar] [CrossRef] [PubMed]
- Malkani, A.L.; Himschoot, K.J.; Ong, K.L.; Lau, E.C.; Baykal, D.; Dimar, J.R.; Glassman, S.D.; Berry, D.J. Does Timing of Primary Total Hip Arthroplasty Prior to or After Lumbar Spine Fusion Have an Effect on Dislocation and Revision Rates? J. Arthroplast. 2019, 34, 907–911. [Google Scholar] [CrossRef]
- Bala, A.; Chona, D.V.; Amanatullah, D.F.; Hu, S.S.; Wood, K.B.; Alamin, T.F.; Cheng, I. Timing of Lumbar Spinal Fusion Affects Total Hip Arthroplasty Outcomes. JAAOS Glob. Res. Rev. 2019, 3, e00133. [Google Scholar] [CrossRef] [PubMed]
- Grammatopoulos, G.; Gofton, W.; Jibri, Z.; Coyle, M.; Dobransky, J.; Kreviazuk, C.; Kim, P.R.; Beaulé, P.E. 2018 Frank Stinchfield Award: Spinopelvic Hypermobility Is Associated With an Inferior Outcome After THA: Examining the Effect of Spinal Arthrodesis. Clin. Orthop. Relat. Res. 2018, 477, 310–321. [Google Scholar] [CrossRef] [PubMed]
- Heckmann, N.D.; Lieberman, J.R. Spinopelvic Biomechanics and Total Hip Arthroplasty: A Primer for Clinical Practice. J. Am. Acad. Orthop. Surg. 2021, 29, e888–e903. [Google Scholar] [CrossRef]
- Innmann, M.M.; Merle, C.; Gotterbarm, T.; Ewerbeck, V.; Beaulé, P.E.; Grammatopoulos, G. Can spinopelvic mobility be predicted in patients awaiting total hip arthroplasty? A prospective, diagnostic study of patients with end-stage hip osteoarthritis. Bone Jt. J. 2019, 101-B, 902–909. [Google Scholar] [CrossRef] [PubMed]
- Haffer, H.; Amini, D.A.; Perka, C.; Pumberger, M. The Impact of Spinopelvic Mobility on Arthroplasty: Implications for Hip and Spine Surgeons. J. Clin. Med. 2020, 9, 2569. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of Primary and Revision Hip and Knee Arthroplasty in the United States from 2005 to 2030. J. Bone Joint Surg. Am. 2007, 89, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br. J. Anaesth. 1997, 78, 606–617. [Google Scholar] [CrossRef]
- Kehlet, H. Fast-track hip and knee arthroplasty. Lancet 2013, 381, 1600–1602. [Google Scholar] [CrossRef]
- Hansen, T.B.; Bredtoft, H.K.; Larsen, K. Preoperative physical optimization in fast-track hip and knee arthroplasty. Dan. Med J. 2012, 59, A4381. [Google Scholar] [PubMed]
- Hansen, T.B. Fast track in hip arthroplasty. EFORT Open Rev. 2017, 2, 179–188. [Google Scholar] [CrossRef]
- Husted, H.; Solgaard, S.; Hansen, T.B.; Søballe, K.; Kehlet, H. Care principles at four fast-track arthroplasty departments in Denmark. Dan. Med Bull. 2010, 57, A4166. [Google Scholar]
- Berg, U.; Bülow, E.; Sundberg, M.; Rolfson, O. No increase in readmissions or adverse events after implementation of fast-track program in total hip and knee replacement at 8 Swedish hospitals: An observational before-and-after study of 14,148 total joint replacements 2011–2015. Acta Orthop. 2018, 89, 522–527. [Google Scholar] [CrossRef]
- Khan, S.K.; Malviya, A.; Muller, S.D.; Carluke, I.; Partington, P.F.; Emmerson, K.P.; Reed, M.R. Reduced short-term complications and mortality following Enhanced Recovery primary hip and knee arthroplasty: Results from 6000 consecutive procedures. Acta Orthop. 2014, 85, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.B.; Kehlet, H.; Jørgensen, C.C.; on behalf of the Lundbeck Foundation Center for Fast-track Hip and Knee Replacement Collaborative Group. Myocardial infarction following fast-track total hip and knee arthroplasty—Incidence, time course, and risk factors: A prospective cohort study of 24,862 procedures. Acta Orthop. 2018, 89, 603–609. [Google Scholar] [CrossRef]
- Wainwright, T.W.; Kehlet, H. Fast-track hip and knee arthroplasty—Have we reached the goal? Acta Orthop. 2019, 90, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, M.; Acheson, A.G.; Auerbach, M.; Besser, M.; Habler, O.; Kehlet, H.; Liumbruno, G.M.; Lasocki, S.; Meybohm, P.; Baikady, R.R.; et al. International consensus statement on the peri-operative management of anaemia and iron deficiency. Anaesthesia 2017, 72, 233–247. [Google Scholar] [CrossRef]
- Grosso, M.J.; Neuwirth, A.L.; Boddapati, V.; Shah, R.P.; Cooper, H.J.; Geller, J.A. Decreasing Length of Hospital Stay and Postoperative Complications After Primary Total Hip Arthroplasty: A Decade Analysis From 2006 to 2016. J. Arthroplast. 2019, 34, 422–425. [Google Scholar] [CrossRef]
- Petersen, P.B.; Kehlet, H.; Jørgensen, C.C.; Madsen, F.; Hansen, T.B.; Gromov, K.; Laursen, M.; Hansen, L.T.; Kjærsgaard-Andersen, P.; Solgaard, S.; et al. Improvement in fast-track hip and knee arthroplasty: A prospective multicentre study of 36,935 procedures from 2010 to 2017. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Berg, U.; W-Dahl, A.; Rolfson, O.; Nauclér, E.; Sundberg, M.; Nilsdotter, A. Influence of fast-track programs on patient-reported outcomes in total hip and knee replacement (THR/TKR) at Swedish hospitals 2011–2015: An observational study including 51,169 THR and 8,393 TKR operations. Acta Orthop. 2020, 91, 306–312. [Google Scholar] [CrossRef]
- Joseph, Z.; Calvert, N.; Salmon, M.; Harper, M.; Swann, A.; Tan, R.; Blades, K.; Yates, P. Enhanced recovery principles applied to revision hip and knee arthroplasty leads to better patient outcomes. J. Orthop. 2020, 22, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Lindberg-Larsen, M.; Petersen, P.B.; Corap, Y.; Gromov, K.; Jørgensen, C.C.; Kehlet, H.; Centre for Fast-track Hip and Knee Replacement Collaborative Group. Fast-track revision hip arthroplasty: A multicenter cohort study on 1345 elective aseptic major component revision hip arthroplasties. Acta Orthop. 2022, 93, 341–347. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manouras, L.; Bastian, J.D.; Beckmann, N.A.; Tosounidis, T.H. The Top Three Burning Questions in Total Hip Arthroplasty. Medicina 2023, 59, 655. https://doi.org/10.3390/medicina59040655
Manouras L, Bastian JD, Beckmann NA, Tosounidis TH. The Top Three Burning Questions in Total Hip Arthroplasty. Medicina. 2023; 59(4):655. https://doi.org/10.3390/medicina59040655
Chicago/Turabian StyleManouras, Lefteris, Johannes Dominik Bastian, Nicholas Andreas Beckmann, and Theodoros H. Tosounidis. 2023. "The Top Three Burning Questions in Total Hip Arthroplasty" Medicina 59, no. 4: 655. https://doi.org/10.3390/medicina59040655
APA StyleManouras, L., Bastian, J. D., Beckmann, N. A., & Tosounidis, T. H. (2023). The Top Three Burning Questions in Total Hip Arthroplasty. Medicina, 59(4), 655. https://doi.org/10.3390/medicina59040655