
Efficacy and Safety of Endoscopic Ultrasound-Guided Radiofrequency Ablation for Pancreatic Neuroendocrine Tumors: A Systematic Review and Metanalysis



Abstract
1. Introduction
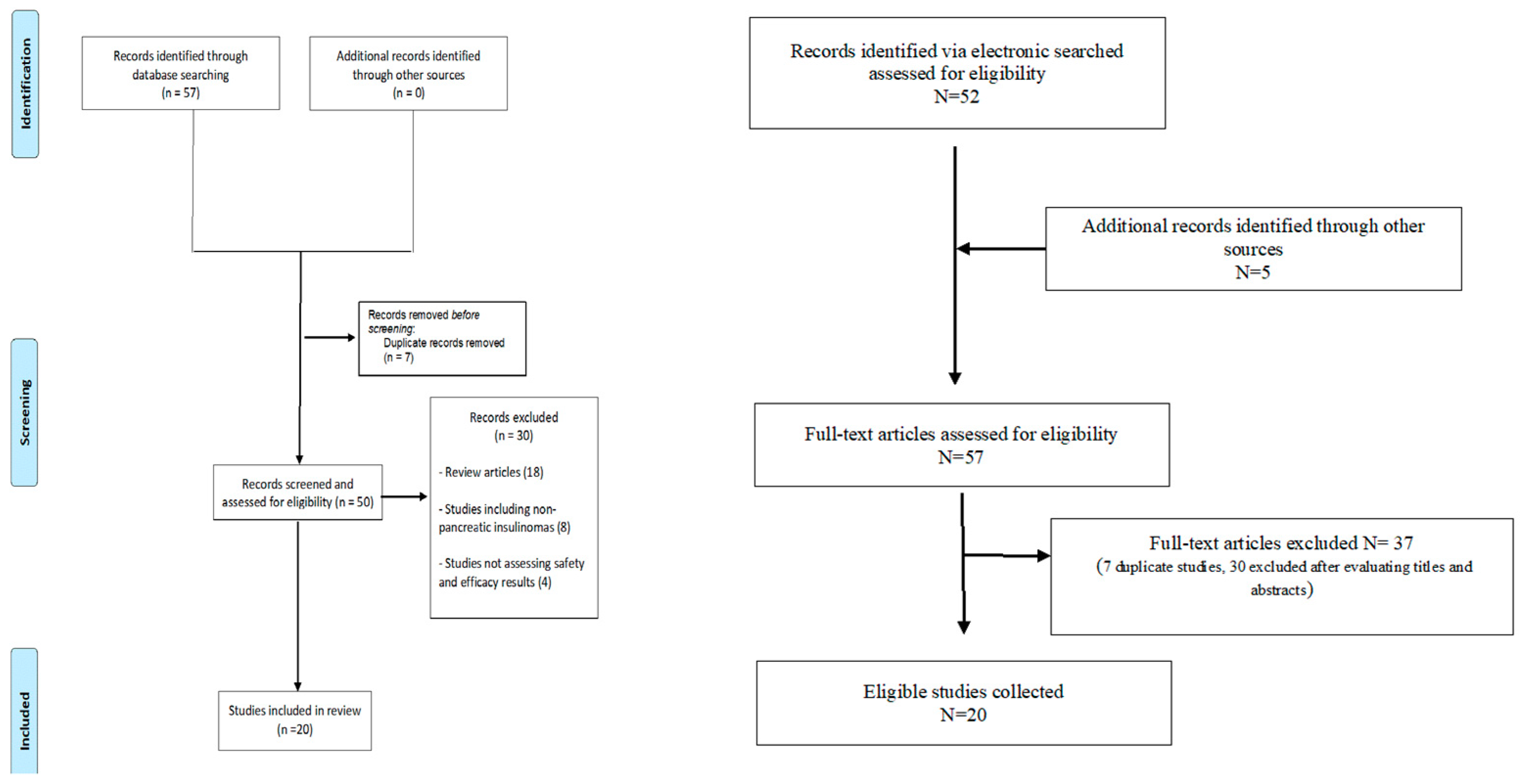
2. Materials and Methods
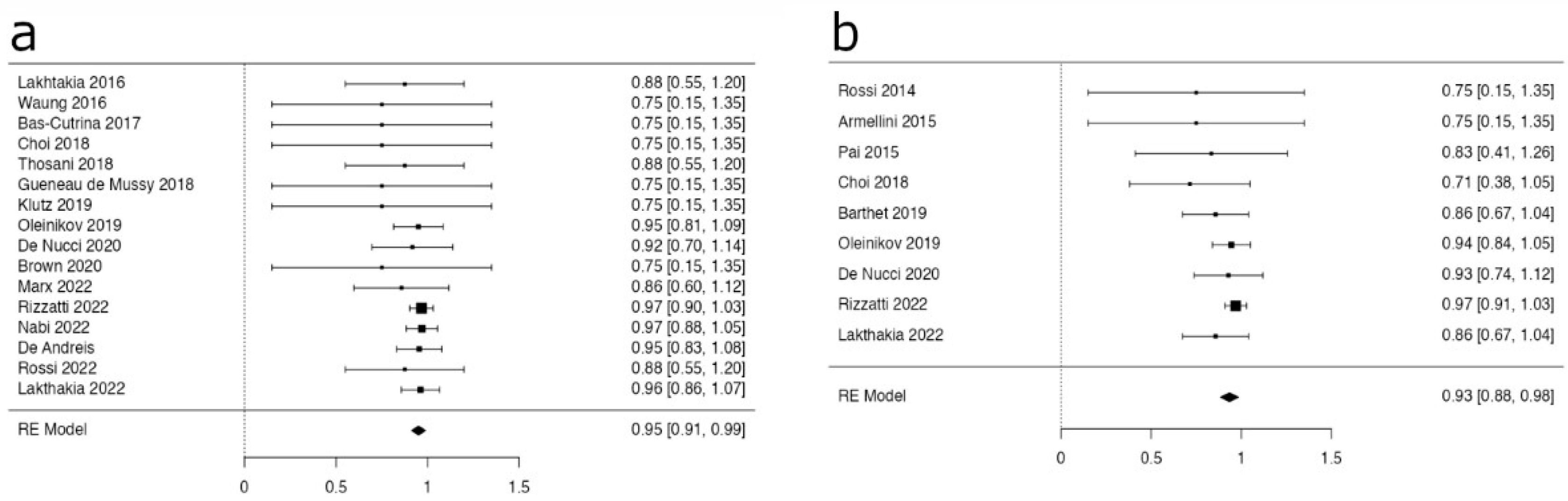
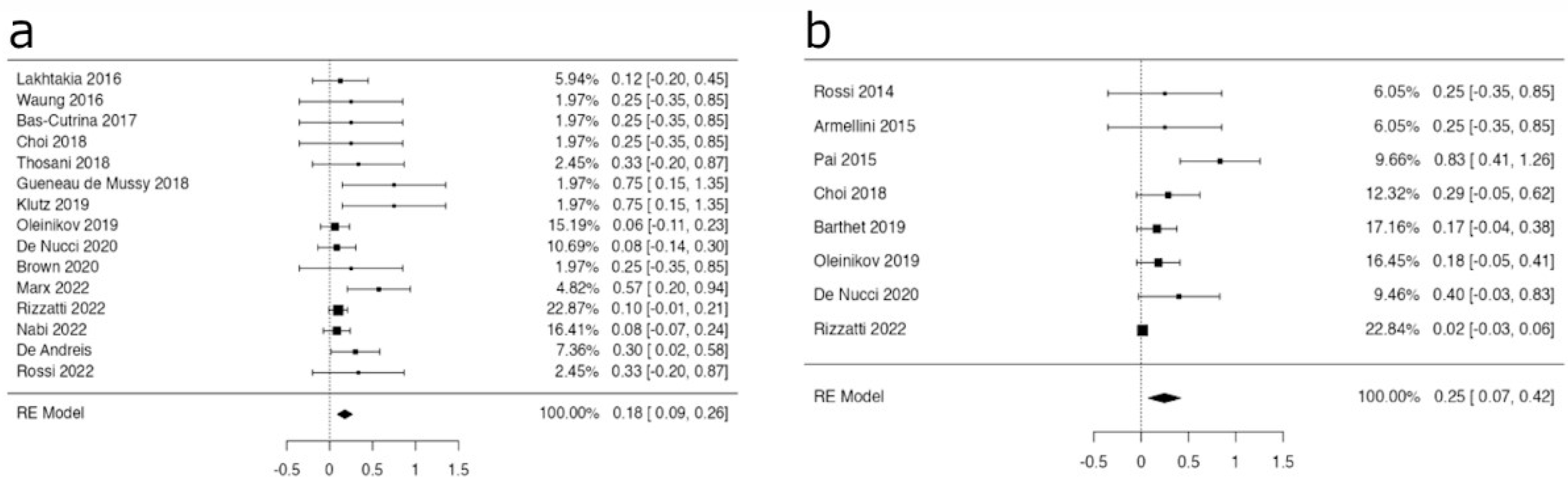
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldberg, S.N. Radiofrequency tumor ablation: Principles and techniques. Eur. J. Ultrasound 2001, 13, 129–147. [Google Scholar] [CrossRef]
- Livraghi, T. Radiofrequency ablation of hepatocellular carcinoma. Surg. Oncol. Clin. N. Am. 2011, 20, 281–299. [Google Scholar] [CrossRef] [PubMed]
- Lakhtakia, S. Therapy of Pancreatic Neuroendocrine Tumors: Fine Needle Intervention including Ethanol and Radiofrequency Ablation. Clin. Endosc. 2017, 50, 546–551. [Google Scholar] [CrossRef]
- Signoretti, M.; Valente, R.; Repici, A.; Delle Fave, G.; Capurso, G.; Carrara, S. Endoscopy-guided ablation of pancreatic lesions: Technical possibilities and clinical outlook. World J. Gastrointest. Endosc. 2017, 16, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Barthet, M.; Giovannini, M.; Lesavre, N.; Boustiere, C.; Napoleon, B.; Koch, S.; Gasmi, M.; Vanbiervliet, G.; Gonzalez, J.M. Endoscopic ultrasound-guided radiofrequency ablation for pancreatic neuroendocrine tumors and pancreatic cystic neoplasms: A prospective multicenter study. Endoscopy 2019, 51, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Crinò, S.F.; D’Onofrio, M.; Bernardoni, L.; Frulloni, L.; Iannelli, M.; Malleo, G.; Paiella, S.; Larghi, A.; Gabbrielli, A. EUS-guided Radiofrequency Ablation (EUS-RFA) of Solid Pancreatic Neoplasm Using an 18-gauge Needle Electrode: Feasibility, Safety, and Technical Success. J. Gastrointest. Liver Dis. 2018, 27, 67–72. [Google Scholar] [CrossRef]
- Girelli, R.; Frigerio, I.; Salvia, R.; Barbi, E.; Tinazzi Martini, P.; Bassi, C. Feasibility and safety of radiofrequency ablation for locally advanced pancreatic cancer. Br. J. Surg. 2010, 97, 220–225. [Google Scholar] [CrossRef]
- D’Onofrio, M.; Crosara, S.; De Robertis, R.; Butturini, G.; Salvia, R.; Paiella, S.; Bassi, C.; Mucelli, R.P. Percutaneous Radiofrequency Ablation of Unresectable Locally Advanced Pancreatic Cancer: Preliminary Results. Technol. Cancer Res. Treat. 2017, 16, 285–294. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 29, n71. [Google Scholar] [CrossRef]
- Cotton, P.B.; Eisen, G.M.; Aabakken, L.; Baron, T.H.; Hutter, M.M.; Jacobson, B.C.; Mergener, K.; Nemcek, A., Jr.; Petersen, B.T.; Petrini, J.L.; et al. A lexicon for endoscopic adverse events: Report of an ASGE workshop. Gastrointest. Endosc. 2010, 71, 446–454. [Google Scholar] [CrossRef]
- Rossi, S.; Viera, F.T.; Ghittoni, G.; Cobianchi, L.; Rosa, L.L.; Siciliani, L.; Bortolotto, C.; Veronese, L.; Vercelli, A.; Gallotti, A.; et al. Radiofrequency ablation of pancreatic neuroendocrine tumors: A pilot study of feasibility; efficacy; and safety. Pancreas 2014, 43, 938–945. [Google Scholar] [CrossRef]
- Pai, M.; Habib, N.; Senturk, H.; Lakhtakia, S.; Reddy, N.; Cicinnati, V.R.; Kaba, I.; Beckebaum, S.; Drymousis, P.; Kahaleh, M.; et al. Endoscopic ultrasound guided radiofrequency ablation; for pancreatic cystic neoplasms and neuroendocrine tumors. World J. Gastrointest. Surg. 2015, 7, 52–59. [Google Scholar] [CrossRef]
- Armellini, E.; Crinò, S.F.; Ballarè, M.; Occhipinti, P. Endoscopic ultrasound-guided radiofrequency ablation of a pancreatic neuroendocrine tumor. Endoscopy 2015, 47 (Suppl. S1), E600–E601. [Google Scholar] [CrossRef] [PubMed]
- Lakhtakia, S.; Ramchandani, M.; Galasso, D.; Gupta, R.; Venugopal, S.; Kalpala, R.; Reddy, D.N. EUS-guided radiofrequency ablation for management of pancreatic insulinoma by using a novel needle electrode (with videos). Gastrointest. Endosc. 2016, 83, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Waung, J.A.; Todd, J.F.; Keane, M.G.; Pereira, S.P. Successful management of a sporadic pancreatic insulinoma by endoscopic ultrasound-guided radiofrequency ablation. Endoscopy 2016, 48 (Suppl. S1), E144–E145. [Google Scholar] [CrossRef]
- Bas-Cutrina, F.; Bargalló, D.; Gornals, J.B. Small pancreatic insulinoma: Successful endoscopic ultrasound-guided radiofrequency ablation in a single session using a 22-G fine needle. Dig. Endosc. 2017, 29, 636–638. [Google Scholar] [CrossRef]
- Choi, J.H.; Seo, D.W.; Song, T.J.; Park, D.H.; Lee, S.S.; Lee, S.K.; Kim, M.H. Endoscopic ultrasound-guided radiofrequency ablation for management of benign solid pancreatic tumors. Endoscopy 2018, 50, 1099–1104. [Google Scholar] [CrossRef]
- Thosani, N.; Sharma, N.R.; Raiman, I.; Thosani, A.J.; Kannadath, B.S.; Guider, G.C.; Raza, A.; Guha, S. Safety and efficacy of endoscopic ultrasound guided radiofrequency ablation (EUS-RFA) in the treatment of pancreatic lesions: A multi-center experience. Gastrointest. Endosc. 2018, 87, AB84. [Google Scholar] [CrossRef]
- Gueneau de Mussy, P.; Lamine, F. A case of benign insulinoma successfully treated with endoscopic ultrasound guided radiofrequency ablation. Endocr. Abstr. 2018, 56, 121. [Google Scholar] [CrossRef]
- Kluz, M.; Staroń, R.; Krupa, Ł.; Partyka, M.; Polkowski, M.; Gutkowski, K. Successful endoscopic ultrasound-guided radiofrequency ablation of a pancreatic insulinoma. Pol. Arch. Intern. Med. 2020, 130, 145–146. [Google Scholar] [CrossRef]
- Oleinikov, K.; Dancour, A.; Epshtein, J.; Benson, A.; Mazeh, H.; Tal, I.; Matalon, S.; Benbassat, C.A.; Livovsky, D.M.; Goldin, E.; et al. Endoscopic Ultrasound-Guided Radiofrequency Ablation: A New Therapeutic Approach for Pancreatic Neuroendocrine Tumors. J. Clin. Endocrinol. Metab. 2019, 104, 2637–2647. [Google Scholar] [CrossRef]
- de Nucci, G.; Imperatore, N.; Mandelli, E.D.; di Nuovo, F.; d’Urbano, C.; Manes, G. Endoscopic ultrasound-guided radiofrequency ablation of pancreatic neuroendocrine tumors: A case series. Endosc. Int. Open. 2020, 8, E1754–E1758. [Google Scholar] [CrossRef]
- Brown, N.G.; Patel, A.A.; Gonda, T.A. Immediate and durable therapeutic response after EUS-guided radiofrequency ablation of a pancreatic insulinoma. VideoGIE 2020, 5, 676–678. [Google Scholar] [CrossRef]
- Marx, M.; Trosic-Ivanisevic, T.; Caillol, F.; Demartines, N.; Schoepfer, A.; Pesenti, C.; Ratone, J.P.; Robert, M.; Giovannini, M.; Godat, S. EUS-guided radiofrequency ablation for pancreatic insulinoma: Experience in 2 tertiary centers. Gastrointest. Endosc. 2022, 95, 1256–1263. [Google Scholar] [CrossRef]
- Rizzatti, G.; de Nucci, G.; Crino’, S.F.; Caillol, F.; Palazzo, L.; Pham, K.D.C.; Larghi, A.; Napolenon, B. Safety and efficacy of endoscopic ultrasound-guided radiofrequency ablation for the treatment of functional and non-functional pancreatic neuroendocrine neoplasms: Preliminary results of a multicentre prospective study. UEG Week 2022 Moderated Posters. United Eur. Gastroenterol. J. 2022, 10 (Suppl. S8), 321–322. [Google Scholar]
- Lakhtakia, S.; Nabi, Z.; Fathima, S.; Basha, J.; Gupta, R.; Reddy, N. Long term outcomes of EUS-guided RFA in pancreatic neuroendocrine tumors: A tertiary care centre experience. UEG Week 2022 Moderated Posters. United Eur. Gastroenterol. J. 2022, 10 (Suppl. S8), 322–323. [Google Scholar]
- Nabi, Z.; Lakhtakia, S.; Fathima, S.; Basha, J.; Gupta, R.; Negashwar Reddy, D. Long-term outcomes of EUS-guided RFA in pancreatic cancer neuroendocrine tumors: A tertiary care centre experience UEG Week 2022 E-Posters. United Eur. Gastroenterol. J. 2022, 10 (Suppl. S8). [Google Scholar]
- Borrelli de Andreis, F.; Boskoski, I.; Mascagni, P.; Bianchi, A.; Schinzari, G.; Annichiarico, E.B.; Quero, G.; Tortora, G.; Alfieri, S.; Gasbarrini, A.; et al. Safety and efficacy of EUS-guided radiofrequency ablation for unresectable pancreatic insulinoma: A single-center experience. Eur. PMC 2022, in press. [Google Scholar]
- Rossi, G.; Petrone, M.C.; Capurso, G.; Partelli, S.; Falconi, M.; Arcidiacono, P.G. Endoscopic ultrasound radiofrequency ablation of pancreatic insulinoma in elderly patients: Three case reports. World J. Clin. Cases 2022, 10, 6514–6519. [Google Scholar] [CrossRef]
- Yoon, W.J.; Brugge, W.R. Endoscopic ultrasonography-guided tumor ablation. Gastrointest. Endosc. Clin. N. Am. 2012, 22, 359–369. [Google Scholar] [CrossRef]
- Goldberg, S.N.; Mallery, S.; Gazelle, G.S.; Brugge, W.R. EUS-guided radiofrequency ablation in the pancreas: Results in a porcine model. Gastrointest. Endosc. 1999, 50, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Varadarajulu, S.; Jhala, N.C.; Drelichman, E.R. EUS-guided radiofrequency ablation with a prototype electrode array system in an animal model (with video). Gastrointest. Endosc. 2009, 70, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Gaidhane, M.; Smith, I.; Ellen, K.; Gatesman, J.; Habib, N.; Foley, P.; Moskaluk, C.; Kahaleh, M. Endoscopic Ultrasound-Guided Radiofrequency Ablation (EUS-RFA) of the Pancreas in a Porcine Model. Gastroenterol. Res. Pract. 2012, 2012, 431451. [Google Scholar] [CrossRef] [PubMed]
- Sethi, A.; Ellrichmann, M.; Dhar, S.; Hadeler, K.G.; Kahle, E.; Seehusen, F.; Klapper, W.; Habib, N.; Fritscher-Ravens, A. Endoscopic ultrasound-guided lymph node ablation with a novel radiofrequency ablation probe: Feasibility study in an acute porcine model. Endoscopy 2014, 46, 411–415. [Google Scholar] [CrossRef]
- Carrara, S.; Arcidiacono, P.G.; Albarello, L.; Addis, A.; Enderle, M.D.; Boemo, C.; Neugebauer, A.; Campagnol, M.; Doglioni, C.; Testoni, P.A. Endoscopic ultrasound-guided application of a new internally gas-cooled radiofrequency ablation probe in the liver and spleen of an animal model: A preliminary study. Endoscopy 2008, 40, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Carrara, S.; Arcidiacono, P.G.; Albarello, L.; Addis, A.; Enderle, M.D.; Boemo, C.; Campagnol, M.; Ambrosi, A.; Doglioni, C.; Testoni, P.A. Endoscopic ultrasound-guided application of a new hybrid cryotherm probe in porcine pancreas: A preliminary study. Endoscopy 2008, 40, 321–326. [Google Scholar] [CrossRef]
- Arcidiacono, P.G.; Carrara, S.; Reni, M.; Petrone, M.C.; Cappio, S.; Balzano, G.; Boemo, C.; Cereda, S.; Nicoletti, R.; Enderle, M.D.; et al. Feasibility and safety of EUS-guided cryothermal ablation in patients with locally advanced pancreatic cancer. Gastrointest Endosc. 2012, 76, 1142–1151. [Google Scholar] [CrossRef]
- Kim, H.J.; Seo, D.W.; Hassanuddin, A.; Kim, S.H.; Chae, H.J.; Jang, J.W.; Park, D.H.; Lee, S.S.; Lee, S.K.; Kim, M.H. EUS-guided radiofrequency ablation of the porcine pancreas. Gastrointest. Endosc. 2012, 76, 1039–1043. [Google Scholar] [CrossRef] [PubMed]
- Song, T.J.; Seo, D.W.; Lakhtakia, S.; Reddy, N.; Oh, D.W.; Park, D.H.; Lee, S.S.; Lee, S.K.; Kim, M.H. Initial experience of EUS-guided radiofrequency ablation of unresectable pancreatic cancer. Gastrointest. Endosc. 2016, 83, 440–443. [Google Scholar] [CrossRef]
- Armellini, E.; Leutner, M.; Stradella, D.; Ballarè, M.; Occhipinti, P. EUS-guided radiofrequency ablation: An option for the extrapancreatic region. Endosc. Ultrasound 2018, 7, 282–283. [Google Scholar] [CrossRef]
- Jiang, T.A.; Deng, Z.; Tian, G.; Zhao, Q.Y.; Wang, W.L. Efficacy and safety of endoscopic ultrasonography-guided interventional treatment for refractory malignant left-sided liver tumors: A case series of 26 patients. Sci. Rep. 2016, 6, 36098. [Google Scholar] [CrossRef]
- Lee, S.H.; Seo, D.W.; Oh, D.; Song, T.J.; Park, D.H.; Lee, S.S.; Kim, M.H. Cushing’s syndrome managed by endoscopic ultrasound-guided radiofrequency ablation of adrenal gland adenoma. Endoscopy 2017, 49, E1–E2. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- Larghi, A.; Rizzatti, G.; Rimbaş, M.; Crino, S.F.; Gasbarrini, A.; Costamagna, G. EUS-guided radiofrequency ablation as an alternative to surgery for pancreatic neuroendocrine neoplasms: Who should we treat? Endosc. Ultrasound 2019, 8, 220–226. [Google Scholar] [CrossRef]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Klöppel, G.; et al. Vienna Consensus Conference participants. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef]
- Rosenberg, A.M.; Friedmann, P.; Del Rivero, J.; Libutti, S.K.; Laird, A.M. Resection versus expectant management of small incidentally discovered nonfunctional pancreatic neuroendocrine tumors. Surgery 2016, 159, 302–309. [Google Scholar] [CrossRef]
- Falconi, M.; Zerbi, A.; Crippa, S.; Balzano, G.; Boninsegna, L.; Capitanio, V.; Bassi, C.; Di Carlo, V.; Pederzoli, P. Parenchyma-preserving resections for small nonfunctioning pancreatic endocrine tumors. Ann. Surg. Oncol. 2010, 17, 1621–1627. [Google Scholar] [CrossRef]
- Falconi, M.; Mantovani, W.; Crippa, S.; Mascetta, G.; Salvia, R.; Pederzoli, P. Pancreatic insufficiency after different resections for benign tumours. Br. J. Surg. 2008, 95, 85–91. [Google Scholar] [CrossRef]
- Aranha, G.V.; Shoup, M. Nonstandard pancreatic resections for unusual lesions. Am. J. Surg. 2005, 189, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Jilesen, A.P.; van Eijck, C.H.; in’t Hof, K.H.; van Dieren, S.; Gouma, D.J.; van Dijkum, E.J. Postoperative Complications; In-Hospital Mortality and 5-Year Survival after Surgical Resection for Patients with a Pancreatic Neuroendocrine Tumor: A Systematic Review. World J. Surg. 2016, 40, 729–748. [Google Scholar] [CrossRef]
- Partelli, S.; Maurizi, A.; Tamburrino, D.; Baldoni, A.; Polenta, V.; Crippa, S.; Falconi, M. GEP-NETS update: A review on surgery of gastro-entero-pancreatic neuroendocrine tumors. Eur. J. Endocrinol. 2014, 171, R153–R162. [Google Scholar] [CrossRef]
- Leyden, S.; Kolarova, T.; Bouvier, C.; Caplin, M.; Conroy, S.; Davies, P.; Dureja, S.; Falconi, M.; Ferolla, P.; Fisher, G.; et al. Unmet needs in the international neuroendocrine tumor (NET) community: Assessment of major gaps from the perspective of patients; patient advocates and NET health care professionals. Int. J. Cancer 2020, 146, 1316–1323. [Google Scholar] [CrossRef]
- Landoni, L.; Marchegiani, G.; Pollini, T.; Cingarlini, S.; D’Onofrio, M.; Capelli, P.; De Robertis, R.; Davì, M.V.; Amodio, A.; Impellizzeri, H.; et al. The Evolution of Surgical Strategies for Pancreatic Neuroendocrine Tumors (Pan-NENs): Time-trend and Outcome Analysis from 587 Consecutive Resections at a High-volume Institution. Ann. Surg. 2019, 269, 725–732. [Google Scholar] [CrossRef]
- Ricci, C.; Partelli, S.; Landoni, L.; Rinzivillo, M.; Ingaldi, C.; Andreasi, V.; Nessi, C.; Muffatti, F.; Fontana, M.; Tamburrino, D.; et al. Sporadic non-functioning pancreatic neuroendocrine tumours: Multicentre analysis. Br. J. Surg. 2021, 108, 811–816. [Google Scholar] [CrossRef]
- Papaefthymiou, A.; Laskaratos, F.M.; Koffas, A.; Manolakis, A.; Gkolfakis, P.; Coda, S.; Sodergren, M.; Suzuki, N.; Toumpanakis, C. State of the Art in Endoscopic Therapy for the Management of Gastroenteropancreatic Neuroendocrine Tumors. Curr. Treat. Options Oncol. 2022, 23, 1014–1034. [Google Scholar] [CrossRef]
- Khanna, L.; Prasad, S.R.; Sunnapwar, A.; Kondapaneni, S.; Dasyam, A.; Tammisetti, V.S.; Salman, U.; Nazarullah, A.; Katabathina, V.S. Pancreatic Neuroendocrine Neoplasms: 2020 Update on Pathologic and Imaging Findings and Classification. Radiographics 2020, 40, 1240–1262. [Google Scholar] [CrossRef]
- Paiella, S.; Landoni, L.; Tebaldi, S.; Zuffante, M.; Salgarello, M.; Cingarlini, S.; D’Onofrio, M.; Parisi, A.; Deiro, G.; Manfrin, E.; et al. Dual-Tracer (68Ga-DOTATOC and 18F-FDG-)-PET/CT Scan and G1-G2 Nonfunctioning Pancreatic Neuroendocrine Tumors: A Single-Center Retrospective Evaluation of 124 Nonmetastatic Resected Cases. Neuroendocrinology 2022, 112, 143–152. [Google Scholar] [CrossRef]
- Crinó, S.F.; Brandolese, A.; Vieceli, F.; Paiella, S.; Conti Bellocchi, M.C.; Manfrin, E.; Bernardoni, L.; Sina, S.; D’Onofrio, M.; Marchegiani, G.; et al. Endoscopic Ultrasound Features Associated with Malignancy and Aggressiveness of Nonhypovascular Solid Pancreatic Lesions: Results from a Prospective Observational Study. Ultraschall Med. 2021, 42, 167–177. [Google Scholar] [CrossRef]
- Paiella, S.; De Pastena, M.; D’Onofrio, M.; Crinò, S.F.; Pan, T.L.; De Robertis, R.; Elio, G.; Martone, E.; Bassi, C.; Salvia, R. Palliative therapy in pancreatic cancer-interventional treatment with radiofrequency ablation/irreversible electroporation. Transl. Gastroenterol. Hepatol. 2018, 3, 80. [Google Scholar] [CrossRef]
- Paiella, S.; Landoni, L.; Rota, R.; Valenti, M.; Elio, G.; Crinò, S.F.; Manfrin, E.; Parisi, A.; Cingarlini, S.; D’Onofrio, M.; et al. Endoscopic ultrasound-guided fine-needle aspiration for the diagnosis and grading of pancreatic neuroendocrine tumors: A retrospective analysis of 110 cases. Endoscopy 2020, 52, 988–994. [Google Scholar] [CrossRef]
- Tacelli, M.; Bina, N.; Crinò, S.F.; Facciorusso, A.; Celsa, C.; Vanni, A.S.; Fantin, A.; Antonini, F.; Falconi, M.; Monica, F.; et al. Reliability of grading preoperative pancreatic neuroendocrine tumors on EUS specimens: A systematic review with meta-analysis of aggregate and individual data. Gastrointest. Endosc. 2022, 96, 898–908.e23. [Google Scholar] [CrossRef]
- Hallet, J.; Law, C.H.; Cukier, M.; Saskin, R.; Liu, N.; Singh, S. Exploring the rising incidence of neuroendocrine tumors: A population-based analysis of epidemiology; metastatic presentation; and outcomes. Cancer 2015, 121, 589–597. [Google Scholar] [CrossRef]
- Melita, G.; Pallio, S.; Tortora, A.; Crinò, S.F.; Macrì, A.; Dionigi, G. Diagnostic and Interventional Role of Endoscopic Ultrasonography for the Management of Pancreatic Neuroendocrine Neoplasms. J. Clin. Med. 2021, 10, 2638. [Google Scholar] [CrossRef]
- Rimbaş, M.; Horumbă, M.; Rizzatti, G.; Crinò, S.F.; Gasbarrini, A.; Costamagna, G.; Larghi, A. Interventional endoscopic ultrasound for pancreatic neuroendocrine neoplasms. Dig. Endosc. 2020, 32, 1031–1041. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Year | Study Design | N of Patients/ N of F-PanNET | Male/ Female | Age | Tumor Size (mean, mm) | Location | Device | N of RFA Sessions /Nodule | Efficacy * | Adverse Events | Follow-Up Months |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lakhtakia [14], 2016 | Retrospective | 3/3 | M | 45 | 19 | H | 19 G, Starmed | 1 | 100 | 0 | 11.5 |
| Waung [15], 2016 | Retrospective | 1/1 | F | 70 | 18 | H | Habib EUS RFA | 3 | 100 | 0 | 10 |
| Bas-Cutrina [16], 2017 | Retrospective | 1/1 | F | 63 | 10 | NR | Habib EUS RFA | 1 | 100 | 0 | 10 |
| Choi [17], 2018 | Prospective | 1/1 | M | 34 | 12 | H | 19G, Starmed | 1 | 100 | 0 | 13 |
| Thosani [18], 2018 | Retrospective | 3/3 | NR | NR | NR | NR | NR | 1.6 ° | 100 | 1 | 5 |
| Gueneau de Mussy [19], 2018 | Retrospective | 1/1 | F | 69 | 12 | T | 19G, Starmed | 1 | 100 | 1 | 2 |
| Klutz [20], 2019 | Retrospective | 1/1 | M | 40 | 9 | H | 19G, Starmed | 1 | 100 | 1 | 6 |
| Oleinikov [21], 2019 | Retrospective | 7/7 | 4M, 3F | 60.4 | 14.9 | H:7, T:2 | 19G, Starmed | 1 | 100 | 0 | 9.7 |
| De Nucci [22], 2020 | Prospective | 5/5 | 2M, 3F | 80 | 12.8 | T | 19 G, Starmed | 1 | 100 | 0 | 12 |
| Brown [23], 2020 | Retrospective | 1/1 | F | 66 | 18 | H | 19 G, Starmed | 1 | 100 | 0 | 8 |
| Marx [24], 2022 | Retrospective | 7/7 | 1M, 6F | 66 | 13.3 | H:1; T:6 | 19 G, Starmed | 1 | 85,7 | 4 | 21 |
| Rizzatti [25], 2022 | Prospective | 30/30 | 10M, 20F | 61.9 | 11.9 | H:12, T:18 | 19 G, Starmed | 25:1; 4:2; 1:3 | 95,8 | 3 | 6 |
| Lakhtakia [26] | Retrospective | 12/12 | NR | NR | NR | NR | 19 G, Starmed | NR | 100 | NR | 31.5 |
| Nabi [27], 2022 | Retrospective | 12/15 | 7M/8F | 46.7 | NR | H:8T:7 | 19 G, Starmed | 1: 10 >1:2 | 100 | 1 | 41 |
| Borrelli deAndreis [28] in press | Retrospective | 10/10 | 7M, 3F | 11.9 | 11,9 | H:3, T:7 | 19 G, Starmed | 9:1,1:2 | 100 | 3 | 3 |
| Rossi [29], 2022 | Retrospective | 3/3 | 2M, 1F | 82.7 | 12 | H:1, T:2 | 19 G, Starmed | 1:2; 2:1 | 100 | 1 | 24 |
| Study, Year | Study Design | N of Patients/ N of NF- PanNETs | Male/ Female | Age | Tumor Size (mean, mm) | Location | Device | N of RFA Sessions per Nodule | Efficacy * | N of Adverse Events | Follow-Up (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Rossi [11], 2014 | Retrospective | 1/1 | M | 72 | 9 | T | Habib EUS RFA | 1 | 100 | 0 | 34 |
| Armellini [13], 2015 | Retrospective | 1/1 | M | 76 | 20 | T | 18 G, Starmed | 1 | 100 | 0 | 1 |
| Pai [12],2015 | Prospective | 2/2 | F | 69.5 | 27.5 | H | Habib EUS RFA | 1:1,1:2 | 100 | 2 | 6 |
| Choi [17], 2018 | Retrospective | 7/7 | 3M, 4F | 56.1 | 20 | H:2, T:5 | 19 G, Starmed | 1:3, 2:2, 3:2 | 75 | 2 | 13 |
| Barthet [5], 2018 | Prospective | 12/14 | 7M, 5F | 59.9 | 13.1 | H:3, T:11 | 19 G, Starmed | NR | 86 | 2 | 12 |
| Oleinikov [21], 2019 | Retrospective | 11/18 | 6M, 5F | 65.8 | 14.2 | H;11, T:7 | 19 G, Starmed | 1 | 94.5 | 2 | 8.7 |
| De Nucci [22], 2020 | Prospective | 5/6 | 3M, 2F | 77.2 | 14.2 | H:3, T:3 | 19 G, Starmed | 1 | 100 | 2 | 12 |
| Rizzatti [25], 2022 | Prospective | 32/32 | 22M, 10F | 70.1 | 14.2 | H:11, T: 21 | 19 G, Starmed | 1:24, 2:7, 3:1 | 96.3 | 0 | 8 |
| Lakthakia [26], 2022 | Retrospective | 14/14 | NR | NR | NR | NR | 19 G, Starmed | NR | 85.7 | NR | 31.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armellini, E.; Facciorusso, A.; Crinò, S.F. Efficacy and Safety of Endoscopic Ultrasound-Guided Radiofrequency Ablation for Pancreatic Neuroendocrine Tumors: A Systematic Review and Metanalysis. Medicina 2023, 59, 359. https://doi.org/10.3390/medicina59020359
Armellini E, Facciorusso A, Crinò SF. Efficacy and Safety of Endoscopic Ultrasound-Guided Radiofrequency Ablation for Pancreatic Neuroendocrine Tumors: A Systematic Review and Metanalysis. Medicina. 2023; 59(2):359. https://doi.org/10.3390/medicina59020359
Chicago/Turabian StyleArmellini, Elia, Antonio Facciorusso, and Stefano Francesco Crinò. 2023. "Efficacy and Safety of Endoscopic Ultrasound-Guided Radiofrequency Ablation for Pancreatic Neuroendocrine Tumors: A Systematic Review and Metanalysis" Medicina 59, no. 2: 359. https://doi.org/10.3390/medicina59020359
APA StyleArmellini, E., Facciorusso, A., & Crinò, S. F. (2023). Efficacy and Safety of Endoscopic Ultrasound-Guided Radiofrequency Ablation for Pancreatic Neuroendocrine Tumors: A Systematic Review and Metanalysis. Medicina, 59(2), 359. https://doi.org/10.3390/medicina59020359