

The Pathogenic Diagnosis in Pediatric Diabetology: Next Generation Sequencing and Precision Therapy
 ,
, 
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Case Report
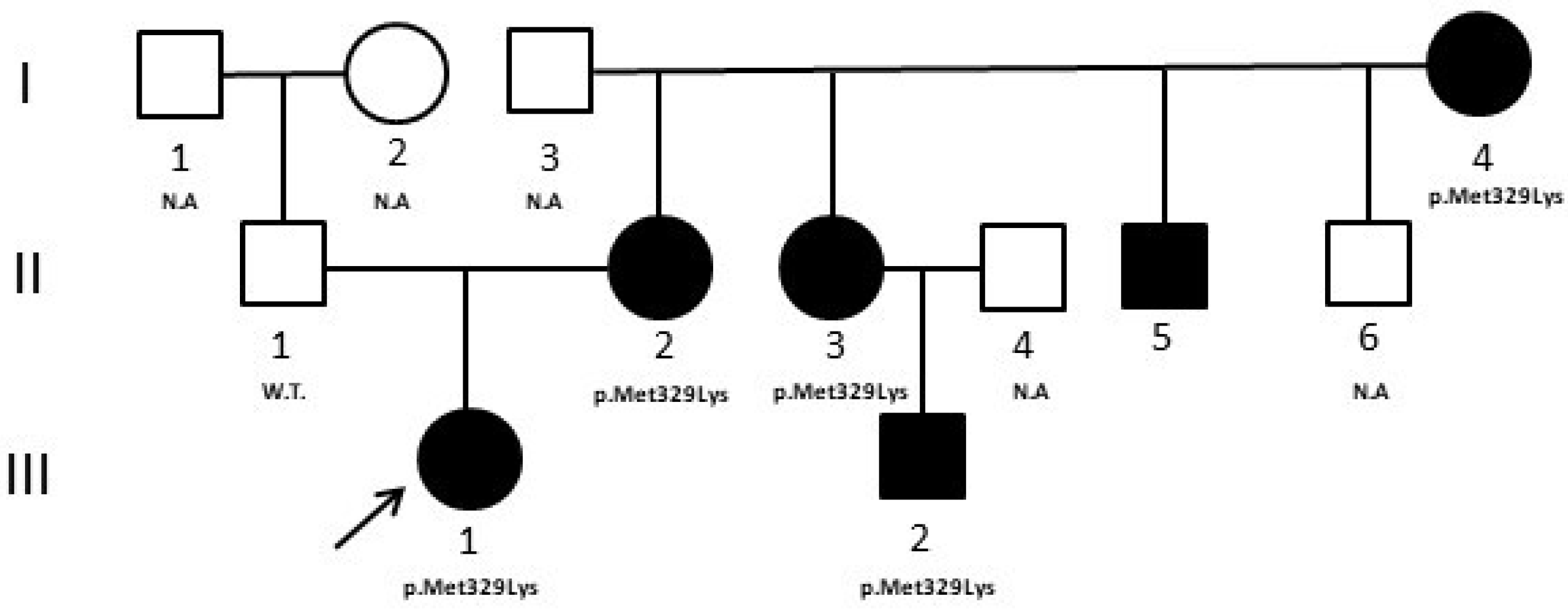
3.1. Case 1
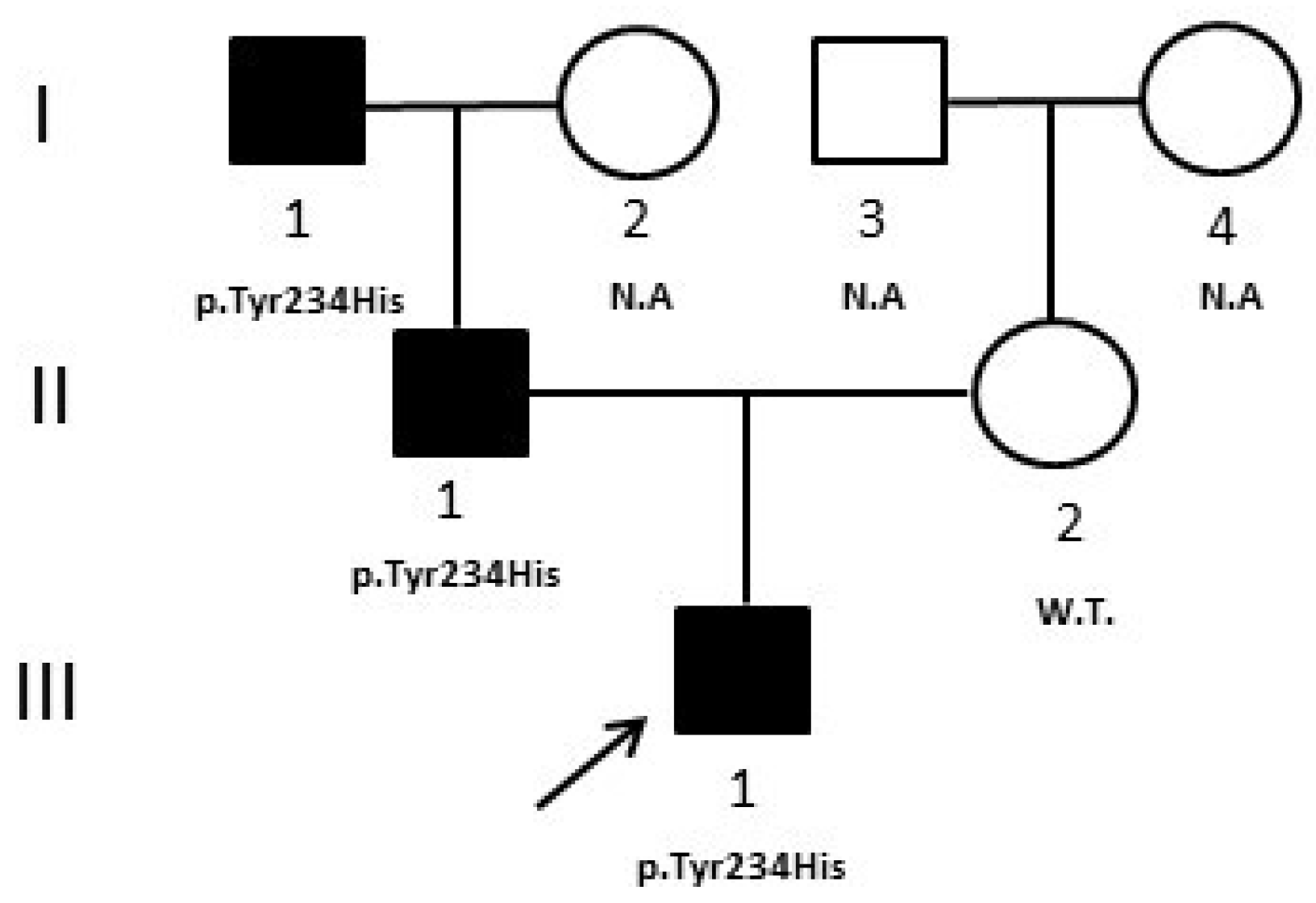
3.2. Case 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iafusco, D.; Zanfardino, A.; Bonfanti, R.; Rabbone, I.; Tinto, N.; Iafusco, F.; Meola, S.; Gicchino, M.F.; Ozen, G.; Casaburo, F.; et al. Congenital Diabetes Mellitus. Minerva Pediatr. 2020, 72, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Bitterman, O.; Tinto, N.; Franzese, A.; Iafusco, F.; Festa, C.; Mozzillo, E.; Napoli, A.; Iafusco, D. Glucokinase Deficit and Birthweight: Does Maternal Hyperglycemia Always Meet Fetal Needs? Acta Diabetol. 2018, 55, 1247–1250. [Google Scholar] [CrossRef] [PubMed]
- Delvecchio, M.; Mozzillo, E.; Salzano, G.; Iafusco, D.; Frontino, G.; Patera, P.I.; Rabbone, I.; Cherubini, V.; Grasso, V.; Tinto, N.; et al. Monogenic Diabetes Accounts for 6.3% of Cases Referred to 15 Italian Pediatric Diabetes Centers During 2007 to 2012. J. Clin. Endocrinol. Metab. 2017, 102, 1826–1834. [Google Scholar] [CrossRef] [PubMed]
- Donath, X.; Saint-Martin, C.; Dubois-Laforgue, D.; Rajasingham, R.; Mifsud, F.; Ciangura, C.; Timsit, J.; Bellanné-Chantelot, C.; Monogenic Diabetes Study Group of the Société Francophone du Diabète. Next-Generation Sequencing Identifies Monogenic Diabetes in 16% of Patients with Late Adolescence/Adult-Onset Diabetes Selected on a Clinical Basis: A Cross-Sectional Analysis. BMC Med. 2019, 17, 132. [Google Scholar] [CrossRef] [PubMed]
- Maturity-Onset Diabetes of the Young (MODY): How Many Cases Are We Missing?—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/20499044/ (accessed on 8 February 2022).
- Moran, A.; Pillay, K.; Becker, D.; Granados, A.; Hameed, S.; Acerini, C.L. ISPAD Clinical Practice Consensus Guidelines 2018: Management of Cystic Fibrosis-Related Diabetes in Children and Adolescents. Pediatr. Diabetes 2018, 19 (Suppl. S27), 64–74. [Google Scholar] [CrossRef]
- Iafusco, F.; Maione, G.; Mazzaccara, C.; Di Candia, F.; Mozzillo, E.; Franzese, A.; Tinto, N. NGS Analysis Revealed Digenic Heterozygous GCK and HNF1A Variants in a Child with Mild Hyperglycemia: A Case Report. Diagnostics 2021, 11, 1164. [Google Scholar] [CrossRef]
- Forlani, G.; Zucchini, S.; Di Rocco, A.; Di Luzio, R.; Scipione, M.; Marasco, E.; Romeo, G.; Marchesini, G.; Mantovani, V. Double Heterozygous Mutations Involving Both HNF1A/MODY3 and HNF4A/MODY1 Genes: A Case Report. Diabetes Care 2010, 33, 2336–2338. [Google Scholar] [CrossRef]
- on behalf of the ACMG Laboratory Quality Assurance Committee; Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; et al. Standards and Guidelines for the Interpretation of Sequence Variants: A Joint Consensus Recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–423. [Google Scholar] [CrossRef]
- Bingham, C.; Hattersley, A.T. Renal Cysts and Diabetes Syndrome Resulting from Mutations in Hepatocyte Nuclear Factor-1beta. Nephrol. Dial. Transplant. 2004, 19, 2703–2708. [Google Scholar] [CrossRef]
- Barretta, F.; Mirra, B.; Monda, E.; Caiazza, M.; Lombardo, B.; Tinto, N.; Scudiero, O.; Frisso, G.; Mazzaccara, C. The Hidden Fragility in the Heart of the Athletes: A Review of Genetic Biomarkers. Int. J. Mol. Sci. 2020, 21, 6682. [Google Scholar] [CrossRef]
- Hattersley, A.T.; Patel, K.A. Precision Diabetes: Learning from Monogenic Diabetes. Diabetologia 2017, 60, 769–777. [Google Scholar] [CrossRef]
- Zmysłowska, A.; Jakiel, P.; Gadzalska, K.; Majos, A.; Płoszaj, T.; Ben-Skowronek, I.; Deja, G.; Glowinska-Olszewska, B.; Jarosz-Chobot, P.; Klonowska, B.; et al. Next- Generation Sequencing Is an Effective Method for Diagnosing Patients with Different Forms of Monogenic Diabetes. Diabetes Res. Clin. Pract. 2022, 183, 109154. [Google Scholar] [CrossRef]
- Iafusco, F.; Meola, S.; Pecoraro, C.; Mazzaccara, C.; Iafusco, D.; Tinto, N. Prenatal Diagnosis of HNF1b Mutation Allows Recognition of Neonatal Dysglycemia. Acta Diabetol. 2021, 58, 393–395. [Google Scholar] [CrossRef]
- Riddle, M.C.; Philipson, L.H.; Rich, S.S.; Carlsson, A.; Franks, P.W.; Greeley, S.A.W.; Nolan, J.J.; Pearson, E.R.; Zeitler, P.S.; Hattersley, A.T. Monogenic Diabetes: From Genetic Insights to Population-Based Precision in Care. Reflections From a Diabetes Care Editors’ Expert Forum. Diabetes Care 2020, 43, 3117–3128. [Google Scholar] [CrossRef]
- Delvecchio, M.; Pastore, C.; Giordano, P. Treatment Options for MODY Patients: A Systematic Review of Literature. Diabetes Ther. 2020, 11, 1667–1685. [Google Scholar] [CrossRef]
- Iafusco, F.; De Sanctis, P.; Pirozzi, D.; Capone, S.; Lombardo, B.; Gambale, A.; Confetto, S.; Zanfardino, A.; Iolascon, A.; Pastore, L.; et al. Molecular Diagnosis of MODY3 Permitted to Reveal a de Novo 12q24.31 Deletion and to Explain a Complex Phenotype in a Young Diabetic Patient. Clin. Chem. Lab. Med. 2019, 57, e306–e310. [Google Scholar] [CrossRef]
- Delvecchio, M.; Salzano, G.; Bonura, C.; Cauvin, V.; Cherubini, V.; d’Annunzio, G.; Franzese, A.; Giglio, S.; Grasso, V.; Graziani, V.; et al. Can HbA1c Combined with Fasting Plasma Glucose Help to Assess Priority for GCK-MODY vs HNF1A-MODY Genetic Testing? Acta Diabetol. 2018, 55, 981–983. [Google Scholar] [CrossRef]
- Prisco, F.; Iafusco, D.; Franzese, A.; Sulli, N.; Barbetti, F. MODY 2 Presenting as Neonatal Hyperglycaemia: A Need to Reshape the Definition of “Neonatal Diabetes”? Diabetologia 2000, 43, 1331–1332. [Google Scholar] [CrossRef]
- Capuano, M.; Garcia-Herrero, C.M.; Tinto, N.; Carluccio, C.; Capobianco, V.; Coto, I.; Cola, A.; Iafusco, D.; Franzese, A.; Zagari, A.; et al. Glucokinase (GCK) Mutations and Their Characterization in MODY2 Children of Southern Italy. PLoS ONE 2012, 7, e38906. [Google Scholar] [CrossRef]
- Tinto, N.; Zagari, A.; Capuano, M.; De Simone, A.; Capobianco, V.; Daniele, G.; Giugliano, M.; Spadaro, R.; Franzese, A.; Sacchetti, L. Glucokinase Gene Mutations: Structural and Genotype-Phenotype Analyses in MODY Children from South Italy. PLoS ONE 2008, 3, e1870. [Google Scholar] [CrossRef]
- Pinelli, M.; Acquaviva, F.; Barbetti, F.; Caredda, E.; Cocozza, S.; Delvecchio, M.; Mozzillo, E.; Pirozzi, D.; Prisco, F.; Rabbone, I.; et al. Identification of Candidate Children for Maturity-Onset Diabetes of the Young Type 2 (MODY2) Gene Testing: A Seven-Item Clinical Flowchart (7-IF). PLoS ONE 2013, 8, e79933. [Google Scholar] [CrossRef] [PubMed]
- Maltoni, G.; Zucchini, S.; Scipione, M.; Mantovani, V.; Salardi, S.; Cicognani, A. Onset of Type 1 Diabetes Mellitus in Two Patients with Maturity Onset Diabetes of the Young. Pediatr. Diabetes 2012, 13, 208–212. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maione, G.; Iafusco, F.; Zanfardino, A.; Piscopo, A.; Ozen, G.; Iafusco, D.; Tinto, N. The Pathogenic Diagnosis in Pediatric Diabetology: Next Generation Sequencing and Precision Therapy. Medicina 2023, 59, 310. https://doi.org/10.3390/medicina59020310
Maione G, Iafusco F, Zanfardino A, Piscopo A, Ozen G, Iafusco D, Tinto N. The Pathogenic Diagnosis in Pediatric Diabetology: Next Generation Sequencing and Precision Therapy. Medicina. 2023; 59(2):310. https://doi.org/10.3390/medicina59020310
Chicago/Turabian StyleMaione, Giovanna, Fernanda Iafusco, Angela Zanfardino, Alessia Piscopo, Gulsum Ozen, Dario Iafusco, and Nadia Tinto. 2023. "The Pathogenic Diagnosis in Pediatric Diabetology: Next Generation Sequencing and Precision Therapy" Medicina 59, no. 2: 310. https://doi.org/10.3390/medicina59020310
APA StyleMaione, G., Iafusco, F., Zanfardino, A., Piscopo, A., Ozen, G., Iafusco, D., & Tinto, N. (2023). The Pathogenic Diagnosis in Pediatric Diabetology: Next Generation Sequencing and Precision Therapy. Medicina, 59(2), 310. https://doi.org/10.3390/medicina59020310