

Correlation between Preoperative MRI Parameters and Oswestry Disability Index in Patients with Lumbar Spinal Stenosis: A Retrospective Study

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Imaging Parameters
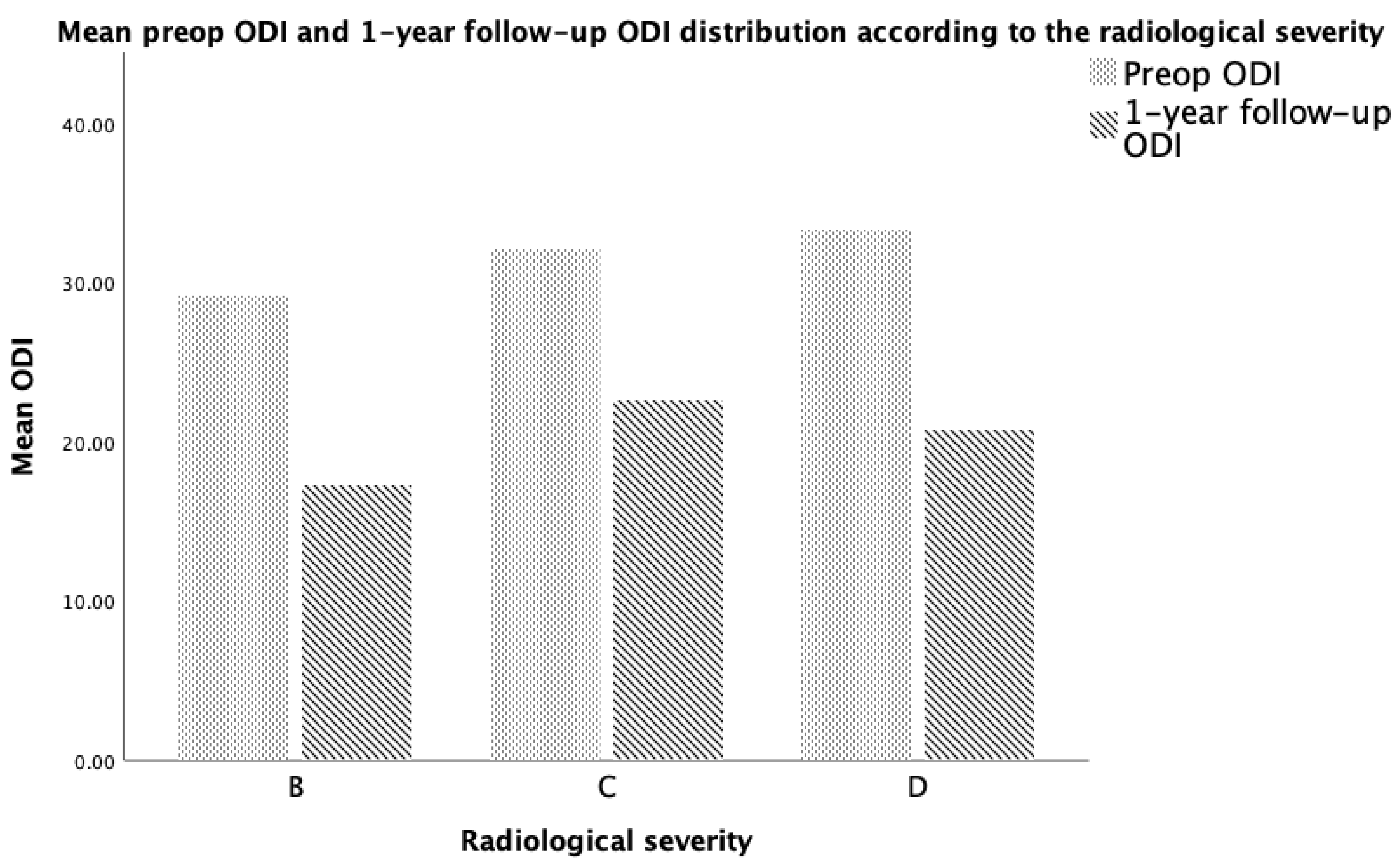
3.2. Patient-Reported Outcome Measure—ODI
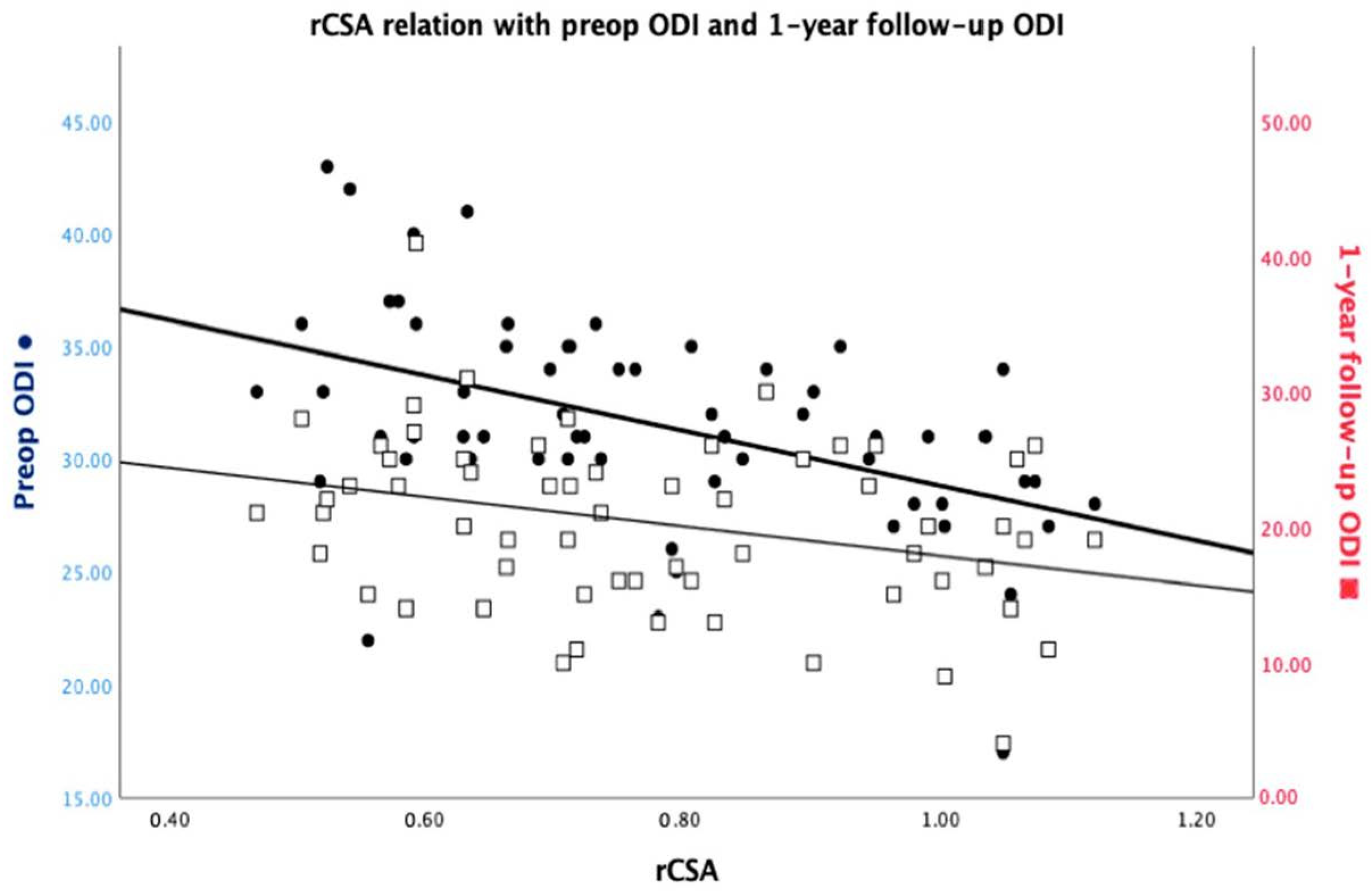
3.3. ODI Functional Score Correlation with Imagistic Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kalichman, L.; Cole, R.; Kim, D.H.; Li, L.; Suri, P.; Guermazi, A.; Hunter, D.J. Spinal stenosis prevalence and association with symptoms: The Framingham Study. Spine J. 2009, 9, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Deyo, R.A.; Mirza, S.K.; Martin, B.I.; Kreuter, W.; Goodman, D.C.; Jarvik, J.G. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA 2010, 303, 1259–1265. [Google Scholar] [CrossRef] [PubMed]
- Maeda, T.; Hashizume, H.; Yoshimura, N.; Oka, H.; Ishimoto, Y.; Nagata, K.; Takami, M.; Tsutsui, S.; Iwasaki, H.; Minamide, A.; et al. Factors associated with lumbar spinal stenosis in a large-scale, population-based cohort: The Wakayama Spine Study. PLoS ONE 2018, 13, e0200208. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, J.N.; Tosteson, T.D.; Lurie, J.D.; Tosteson, A.N.A.; Blood, E.; Hanscom, B.; Herkowitz, H.; Cammisa, F.; Albert, T.; Boden, S.D.; et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N. Engl. J. Med. 2008, 358, 794–810. [Google Scholar] [CrossRef]
- Fairbank, J.C.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2952; discussion 2952. [Google Scholar] [CrossRef]
- Davidson, M.; Keating, J.L. A comparison of five low back disability questionnaires: Reliability and responsiveness. Phys. Ther. 2002, 82, 8–24. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, S.H. Comparative analysis of clinical outcomes in patients with osteoporotic vertebral compression fractures (OVCFs): Conservative treatment versus balloon kyphoplasty. Spine J. 2014, 14, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Teichtahl, A.J.; Urquhart, D.M.; Wang, Y.; Wluka, A.E.; Wijethilake, P.; O’Sullivan, R.; Cicuttini, F.M. Fat infiltration of paraspinal muscles is associated with low back pain, disability, and structural abnormalities in community-based adults. Spine J. 2015, 15, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
- Hodges, P.; Holm, A.K.; Hansson, T.; Holm, S. Rapid atrophy of the lumbar multifidus follows experimental disc or nerve root injury. Spine 2006, 31, 2926–2933. [Google Scholar] [CrossRef]
- Zhang, Y.; Mandelli, F.; Mündermann, A.; Nüesch, C.; Kovacs, B.; Schären, S.; Netzer, C. Association between fatty infiltration of paraspinal muscle, sagittal spinopelvic alignment and stenosis grade in patients with degenerative lumbar spinal stenosis. N. Am. Spine Soc. J. 2021, 5, 100054. [Google Scholar] [CrossRef] [PubMed]
- Tanimoto, Y.; Watanabe, M.; Sun, W.; Sugiura, Y.; Hayashida, I.; Kusabiraki, T.; Tamaki, J. Sarcopenia and falls in community-dwelling elderly subjects in Japan: Defining sarcopenia according to criteria of the European Working Group on Sarcopenia in Older People. Arch. Gerontol. Geriatr. 2014, 59, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Wagner, S.C.; Sebastian, A.S.; McKenzie, J.C.; Butler, J.S.; Kaye, I.D.; Morrissey, P.B.; Vaccaro, A.R.; Kepler, C.K. Severe Lumbar Disability Is Associated with Decreased Psoas Cross-Sectional Area in Degenerative Spondylolisthesis. Glob. Spine J. 2018, 8, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Caprariu, R.; Oprea, M.; Popa, I.; Andrei, D.; Birsasteanu, F.; Poenaru, V.D. Cohort study on the relationship between morphologic parameters of paravertebral muscles, BMI and lumbar lordosis on the severity of lumbar stenosis. Eur. J. Orthop. Surg. Traumatol. 2023, 33, 2435–2443. [Google Scholar] [CrossRef]
- Weishaupt, D.; Zanetti, M.; Boos, N.; Hodler, J. MR imaging and CT in osteoarthritis of the lumbar facet joints. Skelet. Radiol. 1999, 28, 215–219. [Google Scholar] [CrossRef]
- Lohman, C.M.; Tallroth, K.; Kettunen, J.A.; Lindgren, K.A. Comparison of radiologic signs and clinical symptoms of spinal stenosis. Spine 2006, 31, 1834–1840. [Google Scholar] [CrossRef]
- Available online: https://www.aaos.org/globalassets/quality-and-practice-resources/patient-reported-outcome-measures/spine/oswestry-2.pdf (accessed on 16 March 2023).
- Zotti, M.G.T.; Boas, F.V.; Clifton, T.; Piche, M.; Yoon, W.W.; Freeman, B.J.C. Does pre-operative magnetic resonance imaging of the lumbar multifidus muscle predict clinical outcomes following lumbar spinal decompression for symptomatic spinal stenosis? Eur. Spine J. 2017, 26, 2589–2597. [Google Scholar] [CrossRef]
- Maataoui, A.; Vogl, T.J.; Middendorp, M.; Kafchitsas, K.; Khan, M.F. Association between facet joint osteoarthritis and the Oswestry Disability Index. World J. Radiol. 2014, 6, 881–885. [Google Scholar] [CrossRef]
- Sirvanci, M.; Bhatia, M.; Ganiyusufoglu, K.A.; Duran, C.; Tezer, M.; Ozturk, C.; Aydogan, M.; Hamzaoglu, A. Degenerative lumbar spinal stenosis: Correlation with Oswestry Disability Index and MR imaging. Eur. Spine J. 2008, 17, 679–685. [Google Scholar] [CrossRef]
- Carragee, E.J.; Alamin, T.F.; Miller, J.L.; Carragee, J.M. Discographic, MRI and psychosocial determinants of low back pain disability and remission: A prospective study in subjects with benign persistent back pain. Spine J. 2005, 5, 24–35. [Google Scholar] [CrossRef]
- Herno, A.; Airaksinen, O.; Saari, T. Computed tomography after laminectomy for lumbar spinal stenosis. Patients’ pain patterns, walking capacity, and subjective disability had no correlation with computed tomography findings. Spine 1994, 19, 1975–1978. [Google Scholar] [CrossRef] [PubMed]
- Yoshiiwa, T.; Miyazaki, M.; Notani, N.; Ishihara, T.; Kawano, M.; Tsumura, H. Analysis of the Relationship between Ligamentum Flavum Thickening and Lumbar Segmental Instability, Disc Degeneration, and Facet Joint Osteoarthritis in Lumbar Spinal Stenosis. Asian Spine J. 2016, 10, 1132–1140. [Google Scholar] [CrossRef] [PubMed]
- Battié, M.C.; Videman, T.; Gibbons, L.E.; Fisher, L.D.; Manninen, H.; Gill, K. 1995 Volvo Award in clinical sciences. Determinants of lumbar disc degeneration. A study relating lifetime exposures and magnetic resonance imaging findings in identical twins. Spine 1995, 20, 2601–2612. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Wang, T.; Zang, L.; Yuan, S.; Fan, N.; Du, P.; Wu, Q. Quantitative Radiological Characteristics of the Facet Joints in Patients with Lumbar Foraminal Stenosis. J. Pain. Res. 2022, 15, 2363–2371. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.C.; Cha, J.G.; Yoo, J.H.; Kim, H.K.; Kim, H.J.; Shin, B.J. Radiographic grading of facet degeneration, is it reliable?—A comparison of MR or CT grading with histologic grading in lumbar fusion candidates. Spine J. 2012, 12, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.X.; Xiao, L.; Zhao, Q.L.; Liu, C.; Sun, H.Z.; Geng, Y.; Jiang, Y.J. Clinical significance and risk factors of redundant nerve root in patients with lumbar spinal stenosis. Zhongguo Gu Shang 2023, 36, 890–895. (In Chinese) [Google Scholar] [CrossRef] [PubMed]
- Omidi-Kashani, F.; Hasankhani, E.G.; Ashjazadeh, A. Lumbar spinal stenosis: Who should be fused? An updated review. Asian Spine J. 2014, 8, 521–530. [Google Scholar] [CrossRef]
- Kovacs, F.M.; Urrútia, G.; Alarcón, J.D. Surgery versus conservative treatment for symptomatic lumbar spinal stenosis: A systematic review of randomized controlled trials. Spine 2011, 36, E1335–E1351. [Google Scholar] [CrossRef] [PubMed]
- Aghayev, E.; Mannion, A.F.; Fekete, T.F.; Janssen, S.; Goodwin, K.; Zwahlen, M.; Berlemann, U.; Lorenz, T.; Spine Tango Registry Group. Risk Factors for Negative Global Treatment Outcomes in Lumbar Spinal Stenosis Surgery: A Mixed Effects Model Analysis of Data from an International Spine Registry. World Neurosurg. 2020, 136, e270–e283. [Google Scholar] [CrossRef] [PubMed]
- Oprea, M.; Popa, I.; Cimpean, A.M.; Raica, M.; Poenaru, D.V. Microscopic assessment of degenerated intervertebral disc: Clinical implications and possible therapeutic challenge. In Vivo 2015, 29, 95–102. [Google Scholar]
- Verla, T.; Adogwa, O.; Elsamadicy, A.; Moreno, J.R.; Farber, H.; Cheng, J.; Bagley, C.A. Effects of Psoas Muscle Thickness on Outcomes of Lumbar Fusion Surgery. World Neurosurg. 2016, 87, 283–289. [Google Scholar] [CrossRef]
- Urakawa, H.; Sato, K.; Vaishnav, A.S.; Lee, R.; Chaudhary, C.; Mok, J.K.; Virk, S.; Sheha, E.; Katsuura, Y.; Kaito, T.; et al. Preoperative cross-sectional area of psoas muscle correlates with short-term functional outcomes after posterior lumbar surgery. Eur. Spine J. 2023, 32, 2326–2335. [Google Scholar] [CrossRef]
- Echt, M.; Bakare, A.A.; Varela, J.R.; Platt, A.; Abdul Sami, M.; Molenda, J.; Kerolus, M.; Fessler, R.G. Comparison of minimally invasive decompression alone versus minimally invasive short-segment fusion in the setting of adult degenerative lumbar scoliosis: A propensity score-matched analysis. J. Neurosurg. Spine. 2023, 39, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Overdevest, G.M.; Jacobs, W.; Vleggeert-Lankamp, C.; Thomé, C.; Gunzburg, R.; Peul, W. Effectiveness of posterior decompression techniques compared with conventional laminectomy for lumbar stenosis. Cochrane Database Syst. Rev. 2015, 3, CD010036. [Google Scholar] [CrossRef]
- Epstein, N.E. Open laminoforaminotomy: A lost art? Surg. Neurol. Int. 2015, 6 (Suppl. S24), S600–S607. [Google Scholar] [CrossRef] [PubMed]
- Holc, F.; Albani-Forneris, A.; Kido, G.; Beltrame, S.; Petracchi, M.; Gruenberg, M.; Sola, C.; Camino-Willhuber, G. Independent inter and intra-observer agreement of the Schizas’s classification of degenerative lumbar stenosis: Comparison among three levels of surgical training. Rev. Esp. Cir. Ortop. Traumatol. 2023, 67, T175–T180. [Google Scholar] [CrossRef] [PubMed]
- Kuittinen, P.; Sipola, P.; Leinonen, V.; Saari, T.; Sinikallio, S.; Savolainen, S.; Kröger, H.; Turunen, V.; Airaksinen, O.; Aalto, T. Preoperative MRI findings predict two-year postoperative clinical outcome in lumbar spinal stenosis. PLoS ONE 2014, 9, e106404. [Google Scholar] [CrossRef] [PubMed]
- Sigmundsson, F.G.; Kang, X.P.; Jonsson, B.; Stromqvist, B. Prognostic factors in lumbar spinal stenosis surgery. Acta Orthop. 2012, 83, 536–542. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Facet Joint OA | Lumbar Canal Stenosis | ||
|---|---|---|---|
| Weishaupt Grading | No. Cases (Frequency) | Schizas Grading | No. Cases (Frequency) |
| 0 | 0 | A | 0 |
| 1 | 8 (9.3%) | B | 21 (24.4%) |
| 2 | 38 (44.2%) | C | 44 (51.2%) |
| 3 | 40 (46.5%) | D | 21 (24.4%) |
| Imaging Parameters—Descriptive Statistics | ||||
|---|---|---|---|---|
| Min | Max | Mean | Std. Dev. | |
| Age | 32 | 82 | 54.80 | 14.400 |
| rCSA | 0.46 | 1.12 | 0.7734 | 0.18506 |
| TSA | 0.561 | 2.713 | 1.304 | 0.511 |
| NFA | 0.39 | 1.58 | 0.7863 | 0.27302 |
| ODI Mean Score Distribution in Disability Levels | ||||||||
|---|---|---|---|---|---|---|---|---|
| Initial ODI Disability Level | 1-Year Follow-Up ODI Disability Level | |||||||
| Moderate | Severe | Completely | No disability | Mild | Moderate | Severe | Completely | |
| 6 (7%) | 21 (24.4%) | 59 (68.6%) | 1 (1.2%) | 14 (16.3%) | 47 (54.7%) | 23 (26.7%) | 1 (1.2%) | |
| Mean ODI score | 21.50 | 30.48 | 37.27 | 4 | 4.00 | 11.90 | 19.48 | 41.00 |
| Severity | Foramen | rCSA | Initial ODI | 1-year ODI | ||
|---|---|---|---|---|---|---|
| Imagistic severity | Rho | 1.000 | −0.335 ** | −0.012 | 0.327 * | 0.180 |
| NFA | Rho | −0.335 ** | 1.000 | 0.087 | −0.057 | −0.011 |
| rCSA | Rho | −0.012 | 0.087 | 1.000 | −0.498 ** | −0.284 * |
| Initial ODI score | Rho | 0.327 * | −0.057 | −0.498 ** | 1.000 | 0.495 ** |
| 1-year follow-up ODI score | Rho | 0.180 | −0.011 | −0.284 * | 0.495 ** | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caprariu, R.; Oprea, M.D.; Poenaru, D.V.; Andrei, D. Correlation between Preoperative MRI Parameters and Oswestry Disability Index in Patients with Lumbar Spinal Stenosis: A Retrospective Study. Medicina 2023, 59, 2000. https://doi.org/10.3390/medicina59112000
Caprariu R, Oprea MD, Poenaru DV, Andrei D. Correlation between Preoperative MRI Parameters and Oswestry Disability Index in Patients with Lumbar Spinal Stenosis: A Retrospective Study. Medicina. 2023; 59(11):2000. https://doi.org/10.3390/medicina59112000
Chicago/Turabian StyleCaprariu, Radu, Manuel D. Oprea, Dan V. Poenaru, and Diana Andrei. 2023. "Correlation between Preoperative MRI Parameters and Oswestry Disability Index in Patients with Lumbar Spinal Stenosis: A Retrospective Study" Medicina 59, no. 11: 2000. https://doi.org/10.3390/medicina59112000
APA StyleCaprariu, R., Oprea, M. D., Poenaru, D. V., & Andrei, D. (2023). Correlation between Preoperative MRI Parameters and Oswestry Disability Index in Patients with Lumbar Spinal Stenosis: A Retrospective Study. Medicina, 59(11), 2000. https://doi.org/10.3390/medicina59112000