
Antineutrophil Cytoplasmic Antibody-Associated Vasculitis and the Risk of Developing Incidental Tuberculosis: A Population-Based Cohort Study

 , , ,
, , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Design
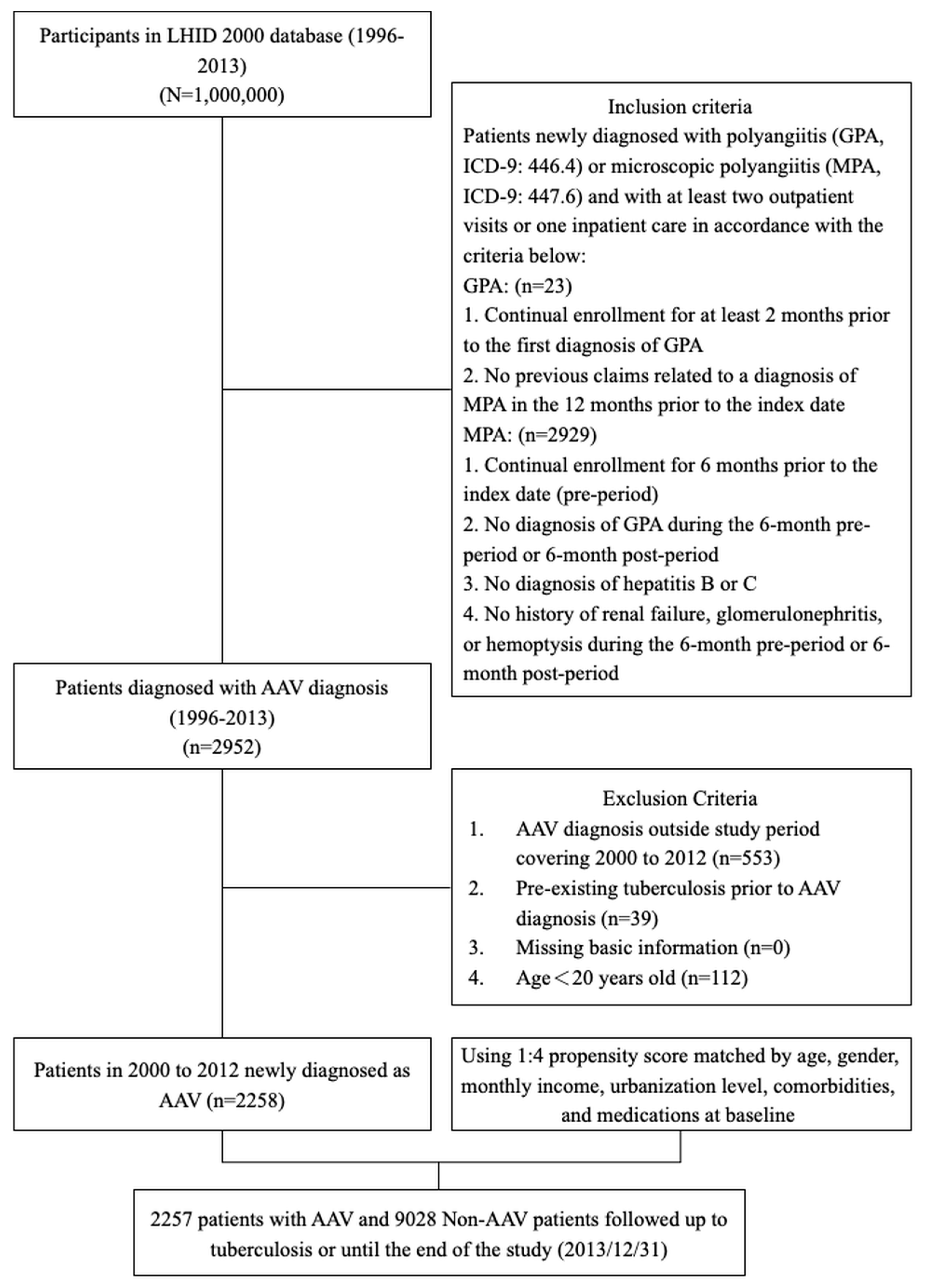
2.3. Selection of Patients with ANCA-Associated Vasculitis
2.4. Matched Cohort Selection
2.5. Variables and Comorbidity
2.6. Outcome Measures
2.7. Statistical Analysis
3. Results
3.1. Baseline Demographic Data
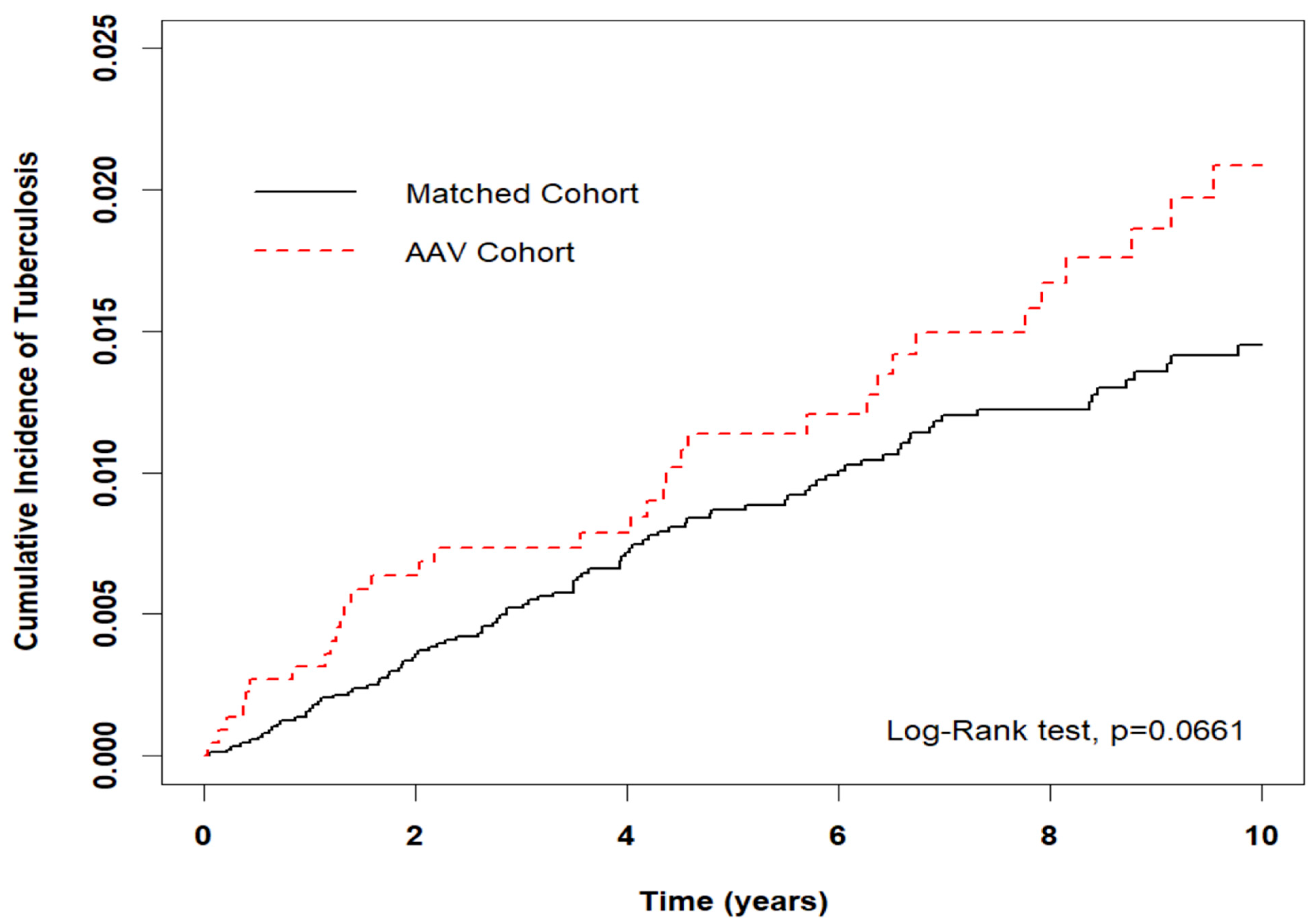
3.2. Risk of Incidental TB in Entire Cohort
3.3. Risk of Incidental TB: Stratification and Interaction Tests
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frieden, T.R.; Brudney, K.F.; Harries, A.D. Global tuberculosis: Perspectives, prospects, and priorities. JAMA 2014, 312, 1393–1394. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Tuberculosis Report; WHO/HTM/TB/2013.11; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Taiwan Centers for Disease Control. Tuberculosis Monitor Data. [Internet]. Available online: https://daily.cdc.gov.tw/stoptb/Indicator.aspx (accessed on 8 February 2021).
- Rathmann, J.; Jayne, D.; Segelmark, M.; Jönsson, G.; Mohammad, A.J. Incidence and predictors of severe infections in ANCA-associated vasculitis: A population-based cohort study. Rheumatology 2021, 60, 2745–2754. [Google Scholar] [CrossRef] [PubMed]
- Flossmann, O.; Berden, A.; de Groot, K.; Hagen, C.; Harper, L.; Heijl, C.; Höglund, P.; Jayne, D.; Luqmani, R.; Mahr, A.; et al. Long-term patient survival in ANCA-associated vasculitis. Ann. Rheum. Dis. 2011, 70, 488–494. [Google Scholar]
- McGregor, J.G.; Negrete-Lopez, R.; Poulton, C.J.; Kidd, J.M.; Katsanos, S.L.; Goetz, L.; Hu, Y.; Nachman, P.H.; Falk, R.J.; Hogan, S.L. Adverse events and infectious burden, microbes and temporal outline from immunosuppressive therapy in antineutrophil cytoplasmic antibody-associated vasculitis with native renal function. Nephrol. Dial. Transplant. 2015, 30 (Suppl. S1), i171–i181. [Google Scholar] [CrossRef] [PubMed]
- Raimundo, K.; Farr, A.M.; Kim, G.; Duna, G. Clinical and Economic Burden of Antineutrophil Cytoplasmic Antibody–associated Vasculitis in the United States. J. Rheumatol. 2015, 42, 2382–2391. [Google Scholar] [CrossRef]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Austin, P.C. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011, 10, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Chander, Y.; Acharya, N.; Naidu, G.; Rathi, M.; Minz, R.; Jain, S.; Behera, D.; Sharma, A. Prevalence of Antineutrophil Cytoplasmic Antibodies and Antinuclear Antibodies in Patients with Pulmonary Tuberculosis: A Tertiary Care Center Experience from North India. J. Assoc. Physicians India 2022, 70, 11–12. [Google Scholar] [CrossRef]
- Kuwabara, G.; Yamada, K.; Tanaka, K.; Nozuchi, S.; Imoto, W.; Shibata, W.; Tohda, M.; Kyoh, S.; Itoh, Y.; Hashimoto, M.; et al. Muscle Biopsy-proven Drug-induced Microscopic Polyangiitis in a Patient with Tuberculosis. Intern. Med. 2023, 62, 129–133. [Google Scholar] [CrossRef]
- Yang, Y.; Thumboo, J.; Tan, B.H.; Tan, T.T.; Fong CH, J.; Ng, H.S.; Fong, K.Y. The risk of tuberculosis in SLE patients from an Asian tertiary hospital. Rheumatol. Int. 2017, 37, 1027–1033. [Google Scholar] [CrossRef]
- Urdahl, K.B.; Shafiani, S.; Ernst, J.D. Initiation and regulation of T-cell responses in tuberculosis. Mucosal Immunol. 2011, 4, 288–293. [Google Scholar] [CrossRef]
- Xu, Y.; Xu, H.; Zhen, Y.; Sang, X.; Wu, H.; Hu, C.; Ma, Z.; Yu, M.; Yi, H. Imbalance of Circulatory T Follicular Helper and T Follicular Regulatory Cells in Patients with ANCA-Associated Vasculitis. Mediat. Inflamm. 2019, 2019, 8421479. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Lee, M.-T.G.; Lee, S.-H.; Lee, S.-H.; Chang, S.-S.; Lee, C.-C. Risk of incidental active tuberculosis and use of corticosteroids. Int. J. Tuberc. Lung Dis. 2015, 19, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Brode, S.K.; Jamieson, F.B.; Ng, R.; Campitelli, M.A.; Kwong, J.C.; Paterson, J.M.; Li, P.; Marchand-Austin, A.; Bombardier, C.; Marras, T.K.; et al. Increased risk of mycobacterial infections associated with anti-rheumatic medications. Thorax 2015, 70, 677–682. [Google Scholar] [CrossRef]
- Mohammad, A.J.; Segelmark, M.; Smith, R.; Englund, M.; Nilsson, J.Å.; Westman, K.; Merkel, P.A.; Jayne, D.R.W. Severe Infection in Antineutrophil Cytoplasmic Antibody-associated Vasculitis. J. Rheumatol. 2017, 44, 1468–1475. [Google Scholar] [CrossRef] [PubMed]
- Nachman, P.H.; Hogan, S.L.; Jennette, J.C.; Falk, R.J. Treatment response and relapse in antineutrophil cytoplasmic autoantibody-associated microscopic polyangiitis and glomerulonephritis. J. Am. Soc. Nephrol. 1996, 7, 33. [Google Scholar] [CrossRef]
- Reinhold-Keller, E.; Herlyn, K.; Wagner-Bastmeyer, R.; Gross, W.L. Stable incidence of primary systemic vasculitides over five years: Results from the German vasculitis register. Arthritis Rheumatol. 2005, 53, 93–99. [Google Scholar] [CrossRef]
- Gonzalez-Gay, M.A.; Garcia-Porrua, C. Systemic vasculitis in adults in northwestern Spain, 1988–1997. Clin. Epidemiol. Asp. Med. 1999, 78, 292–308. [Google Scholar]
- Watts, R.A.; Lane, S.E.; Bentham, G.; Scott, D.G. Epidemiology of systemic vasculitis: A ten-year study in the United Kingdom. Arthritis Rheum. 2000, 43, 414–419. [Google Scholar] [CrossRef]
- Takala, J.H.; Kautiainen, H.; Malmberg, H.; Leirisalo-Repo, M. Incidence of Wegener’s granulomatosis in Finland 1981–2000. Clin. Exp. Rheumatol. 2008, 26, S81–S85. [Google Scholar] [PubMed]
- Berti, A.; Cornec, D.; Crowson, C.S.; Specks, U.; Matteson, E.L. The epidemiology of antineutrophil cytoplasmic autoantibody-associated vasculitis in Olmsted County, Minnesota: A twenty-year US population-based study. Arthritis Rheumatol. 2017, 69, 2338–2350. [Google Scholar] [CrossRef] [PubMed]
- Pierini, F.S.; Scolnik, M.; Scaglioni, V.; Mollerach, F.; Soriano, E.R. Incidence and prevalence of granulomatosis with polyangiitis and microscopic polyangiitis in health management organization in Argentina: A 15-year study. Clin. Rheumatol. 2019, 38, 1935–1940. [Google Scholar] [CrossRef] [PubMed]
- National Health Research Institutes. 2019 Annual Report on Kidney Disease in Taiwan; National Health Research Institutes: Taiwan, China, 2020; pp. 198–203. ISBN 9789865439439. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Variable | AAV | Standardize Mean Difference (SMD) § | ||
|---|---|---|---|---|
| Total | No | Yes | ||
| n = 11,285 | n = 9028 | n = 2257 | ||
| n | n (%)/Mean (SD) | n (%)/Mean (SD) | ||
| Sex | 0.030 | |||
| Female | 6028 | 4795 (53.1) | 1233 (54.6) | |
| Male | 5257 | 4233 (46.9) | 1024 (45.4) | |
| Age at Baseline (years) | 0.081 | |||
| <40 | 2631 | 2055 (22.8) | 576 (25.5) | |
| 40–65 | 5261 | 4202 (46.5) | 1059 (46.9) | |
| ≥65 | 3393 | 2771 (30.7) | 622 (27.6) | |
| Mean (SD) | 54.6 (17.5) | 53.1 (17.0) | 0.086 | |
| Monthly Income (NTD) | 0.072 | |||
| 0–15,840 | 4450 | 3540 (39.2) | 910 (40.3) | |
| 15,841–28,800 | 4939 | 3937 (43.6) | 1002 (44.4) | |
| 28,801–45,800 | 1389 | 1121 (12.4) | 268 (11.9) | |
| >45,800 | 507 | 430 (4.8) | 77 (3.4) | |
| Urbanization | 0.081 | |||
| 1 (highest) | 3540 | 2808 (31.1) | 732 (32.4) | |
| 2 | 3315 | 2693 (29.8) | 622 (27.6) | |
| 3 | 1954 | 1520 (16.8) | 434 (19.2) | |
| 4 | 2476 | 2007 (22.2) | 469 (20.8) | |
| CCI Score | 0.058 | |||
| 0 | 8840 | 7074 (78.4) | 1766 (78.2) | |
| 1 | 1258 | 981 (10.9) | 277 (12.3) | |
| ≥2 | 1187 | 973 (10.8) | 214 (9.5) | |
| Baseline Comorbidity | ||||
| Diabetes | 2396 | 1948 (21.6) | 448 (19.8) | 0.043 |
| Hypertension | 5031 | 4072 (45.1) | 959 (42.5) | 0.053 |
| Hyperlipidemia | 2882 | 2351 (26) | 531 (23.5) | 0.058 |
| Atrial Fibrillation | 230 | 189 (2.1) | 41 (1.8) | 0.020 |
| Valvular heart disease | 720 | 580 (6.4) | 140 (6.2) | 0.009 |
| Parkinsonism | 139 | 110 (1.2) | 29 (1.3) | 0.006 |
| Autoimmune disease | 239 | 179 (2) | 60 (2.7) | 0.045 |
| Characteristics | No. of Events | Crude | Adjusted | ||
|---|---|---|---|---|---|
| (n = 142) | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| AAV | |||||
| No | 104 | Ref. | Ref. | ||
| Yes | 38 | 1.41 (0.98–2.05) | 0.067 | 1.48 (1.02–2.15) | 0.041 |
| Sex | |||||
| Female | 51 | Ref. | Ref. | ||
| Male | 91 | 2.11 (1.50–2.98) | <0.001 | 2.49 (1.70–3.63) | <0.001 |
| Age at Baseline (years) | |||||
| <40 | 8 | Ref. | Ref. | ||
| 40–65 | 41 | 2.57 (1.20–5.47) | 0.015 | 2.75 (1.26–6.02) | 0.012 |
| ≥65 | 93 | 11.26 (5.47–23.19) | <0.001 | 9.10 (4.12–20.06) | <0.001 |
| Monthly Income (NTD) | |||||
| 0–15,840 | 65 | Ref. | Ref. | ||
| 15,841–28,800 | 64 | 0.82 (0.58–1.16) | 0.256 | 0.82 (0.57–1.20) | 0.308 |
| 28,801–45,800 | 11 | 0.49 (0.26–0.93) | 0.029 | 0.67 (0.35–1.31) | 0.243 |
| >45,800 | 2 | 0.24 (0.06–0.98) | 0.047 | 0.34 (0.08–1.43) | 0.141 |
| Urbanization | |||||
| 1 (highest) | 40 | Ref. | Ref. | ||
| 2 | 34 | 0.92 (0.58–1.46) | 0.728 | 0.86 (0.55–1.37) | 0.536 |
| 3 | 27 | 1.23 (0.75–2.00) | 0.410 | 1.14 (0.69–1.87) | 0.610 |
| 4 | 41 | 1.49 (0.97–2.31) | 0.072 | 1.07 (0.67–1.71) | 0.763 |
| CCI Score | |||||
| 0 | 87 | Ref. | Ref. | ||
| 1 | 24 | 2.27 (1.45–3.58) | <0.001 | 1.24 (0.77–2.01) | 0.377 |
| ≥2 | 31 | 3.96 (2.62–5.98) | <0.001 | 1.92 (1.19–3.10) | 0.007 |
| Baseline Comorbidity | |||||
| Diabetes | 40 | 1.68 (1.16–2.42) | 0.006 | 1.14 (0.70–1.86) | 0.600 |
| Hypertension | 88 | 2.37 (1.69–3.32) | <0.001 | 0.91 (0.54–1.55) | 0.735 |
| Hyperlipidemia | 31 | 0.97 (0.65–1.45) | 0.901 | 0.68 (0.42–1.11) | 0.122 |
| Atrial Fibrillation | 1 | 0.53 (0.07–3.82) | 0.531 | 0.21 (0.03–1.57) | 0.129 |
| Valvular heart disease | 8 | 1.16 (0.57–2.37) | 0.684 | 0.74 (0.35–1.54) | 0.420 |
| Parkinsonism | 2 | 1.67 (0.41–6.77) | 0.470 | 0.65 (0.16–2.64) | 0.543 |
| Autoimmune disease | 2 | 0.80 (0.20–3.22) | 0.752 | 1.02 (0.25–4.17) | 0.981 |
| Variables | Matched Cohort | AAV Cohort | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 9028 | n = 2257 | Crude HR | p-Value | Adjusted HR | p-Value | P for Interaction | |||||
| Event | Person-Years | IR | Event | Person-Years | IR | (95% CI) | (95% CI) | ||||
| Overall | 104 | 66,914 | 15.54 | 38 | 17,385 | 21.86 | 1.41 (0.98–2.05) | 0.067 | 1.48 (1.02–2.15) | 0.041 | |
| Sex | 0.001 | ||||||||||
| Female | 28 | 36,191 | 7.74 | 23 | 9579 | 24.01 | 3.10 (1.79–5.39) | <0.001 | 3.24 (1.85–5.67) | <0.001 | |
| Male | 76 | 30,722 | 24.74 | 15 | 7806 | 19.22 | 0.78 (0.45–1.36) | 0.385 | 0.78 (0.45–1.36) | 0.384 | |
| Age at Baseline (years) | 0.707 | ||||||||||
| <40 | 4 | 16,434 | 2.43 | 4 | 4539 | 8.81 | 3.60 (0.90–14.40) | 0.070 | 4.21 (1.00–17.79) | 0.050 | |
| 40–65 | 31 | 33,110 | 9.36 | 10 | 8745 | 11.44 | 1.23 (0.60–2.50) | 0.573 | 1.18 (0.58–2.42) | 0.643 | |
| ≥65 | 69 | 17,370 | 39.72 | 24 | 4101 | 58.52 | 1.47 (0.92–2.34) | 0.103 | 1.44 (0.90–2.30) | 0.128 | |
| CCI Score | 0.597 | ||||||||||
| 0 | 65 | 55,435 | 11.73 | 22 | 14,321 | 15.36 | 1.31 (0.81–2.13) | 0.272 | 1.43 (0.88–2.33) | 0.149 | |
| 1 | 16 | 6400 | 25.00 | 8 | 1979 | 40.42 | 1.62 (0.69–3.79) | 0.266 | 1.74 (0.72–4.23) | 0.220 | |
| ≥2 | 23 | 5079 | 45.29 | 8 | 1085 | 73.76 | 1.62 (0.73–3.63) | 0.237 | 1.53 (0.67–3.53) | 0.316 | |
| Baseline Comorbidity | |||||||||||
| Diabetes | 0.514 | ||||||||||
| No | 76 | 54,278 | 14.00 | 26 | 14,202 | 18.31 | 1.31 (0.84–2.05) | 0.234 | 1.37 (0.87–2.14) | 0.172 | |
| Yes | 28 | 12,636 | 22.16 | 12 | 3183 | 37.70 | 1.77 (0.90–3.47) | 0.100 | 1.94 (0.97–3.90) | 0.062 | |
| Hypertension | 0.435 | ||||||||||
| No | 41 | 39,553 | 10.37 | 13 | 10,602 | 12.26 | 1.18 (0.63–2.21) | 0.599 | 1.22 (0.65–2.29) | 0.538 | |
| Yes | 63 | 27,361 | 23.03 | 25 | 6783 | 36.86 | 1.62 (1.02–2.58) | 0.041 | 1.75 (1.10–2.79) | 0.019 | |
| Hyperlipidemia | 0.286 | ||||||||||
| No | 83 | 51,970 | 15.97 | 28 | 13,870 | 20.19 | 1.27 (0.83–1.95) | 0.276 | 1.33 (0.86–2.04) | 0.200 | |
| Yes | 21 | 14,943 | 14.05 | 10 | 3515 | 28.45 | 2.06 (0.97–4.37) | 0.061 | 2.59 (1.19–5.60) | 0.016 | |
| Follow-Up Period, Year | Matched Cohort | AAV Cohort | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n = 9076 | n = 2269 | Crude HR | p-Value | Adjusted HR | p-Value | |||||
| Event | Person-Years | IR | Event | Person-Years | IR | (95% CI) | (95% CI) | |||
| Years of Follow-up | ||||||||||
| <2 | 31 | 17,415 | 17.80 | 14 | 4355 | 32.15 | 1.81 (0.96–3.39) | 0.067 | 1.91 (1.01–3.60) | 0.046 |
| 2–5 | 37 | 21,473 | 17.23 | 9 | 5467 | 16.46 | 0.96 (0.46–1.98) | 0.900 | 1.03 (0.49–2.14) | 0.941 |
| >5 | 36 | 28,027 | 12.84 | 15 | 7564 | 19.83 | 1.55 (0.85–2.83) | 0.153 | 1.63 (0.88–2.99) | 0.118 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, S.-H.; Li, M.-F.; Ou, S.-H.; Lin, M.-C.; Wang, J.-H.; Lee, P.-T.; Chen, H.-Y. Antineutrophil Cytoplasmic Antibody-Associated Vasculitis and the Risk of Developing Incidental Tuberculosis: A Population-Based Cohort Study. Medicina 2023, 59, 1920. https://doi.org/10.3390/medicina59111920
Chan S-H, Li M-F, Ou S-H, Lin M-C, Wang J-H, Lee P-T, Chen H-Y. Antineutrophil Cytoplasmic Antibody-Associated Vasculitis and the Risk of Developing Incidental Tuberculosis: A Population-Based Cohort Study. Medicina. 2023; 59(11):1920. https://doi.org/10.3390/medicina59111920
Chicago/Turabian StyleChan, Shan-Ho, Ming-Feng Li, Shih-Hsiang Ou, Mei-Chen Lin, Jen-Hung Wang, Po-Tsang Lee, and Hsin-Yu Chen. 2023. "Antineutrophil Cytoplasmic Antibody-Associated Vasculitis and the Risk of Developing Incidental Tuberculosis: A Population-Based Cohort Study" Medicina 59, no. 11: 1920. https://doi.org/10.3390/medicina59111920
APA StyleChan, S.-H., Li, M.-F., Ou, S.-H., Lin, M.-C., Wang, J.-H., Lee, P.-T., & Chen, H.-Y. (2023). Antineutrophil Cytoplasmic Antibody-Associated Vasculitis and the Risk of Developing Incidental Tuberculosis: A Population-Based Cohort Study. Medicina, 59(11), 1920. https://doi.org/10.3390/medicina59111920