1. Introduction
It has been well documented that intravitreal injections of anti-vascular endothelial growth factor (anti-VEGF) drugs lead to functional and anatomical improvements of eyes with neovascular age-related macular degeneration (nAMD). Because of their effectiveness, anti-VEGF treatments have become the first-line treatment for nAMD; however, the treatment has several weaknesses including its lack of effect on exudations and the need for frequent intravitreal injections.
Thus, new anti-VEGF drugs have been developed that have stronger effects on exudations and longer-lasting effects. One of these newly developed anti-VEGF agents is brolucizumab (Beovu; Novartis Pharma AG, Basel, Switzerland) which is a humanized single-chain antibody fragment that inhibits the binding of VEGF-A to the VEGF receptor. It was approved for use in Japan in 2020. Its lower molecular weight compared to other commercially available anti-VEGF drugs allows it to be used at a higher molar concentration which then has greater therapeutic effects. However, several post-marketing cases of visual acuity reduction caused by severe intraocular inflammation (IOI) and retinal vasculitis and/or retinal artery occlusion (RAO) have been reported after intravitreal injection of brolucizumab (IVBr) [
1]. The Safety Review Committee (SRC) reported that IOI in any form was identified in 50 of 1088 study eyes of patients treated with brolucizumab (4.6%) during the HAWK and HARRIER trials. Of these 50 eyes with IOI, 36 eyes had concomitant retinal vasculitis (3.3%), of which 23 had concomitant retinal vascular occlusion (2.1%) [
2]. These studies reported that an early diagnosis and appropriate treatments were necessary to treat the IOI successfully. Because the detection of IOI is usually made by complaints from patients of a worsening of the vision, it is imperative that patients know the symptoms associated with IOI. Once the diagnosis of IOI is confirmed, initiation of corticosteroid therapy is recommended. Based on the severity of inflammation, clinicians may consider the most potent topical corticosteroid from the locally available options. If necessary, topical therapy may be supplemented with sub-tenon, intravitreal, and systemic corticosteroids. Treatment can be tapered once the inflammation is under control [
2].
We reported a case of IOI that developed after IVBr for nAMD that had a delay in beginning the treatment because of the lack of reporting a reduction in the vision due to the patient’s cognitive dysfunction.
2. Case Presentation
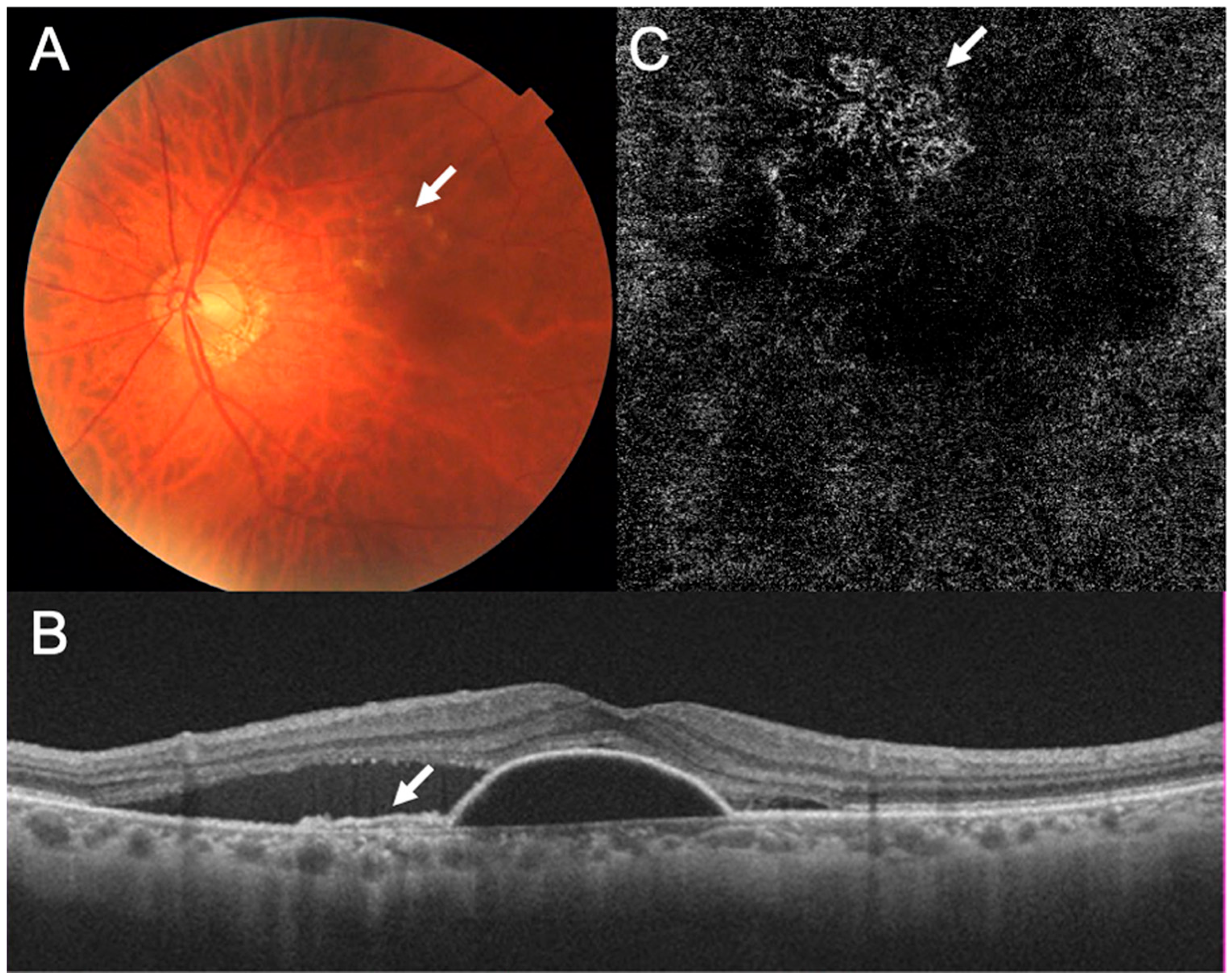
A 79-year-old Japanese man was referred to our hospital with a complaint of visual disturbances in both eyes. His decimal best-corrected visual acuity (BCVA) was 0.9 in his right eye and 1.0 in his left eye. The intraocular pressure (IOP) was 13 mmHg in both eyes. Slit-lamp examinations showed no abnormalities except for mild cataracts in both eyes. Ophthalmoscopy showed mild abnormalities in the retinal pigment epithelium, but the presence of hard exudates and serous retinal detachment in his left eye (
Figure 1A). Optical coherence tomography (OCT) showed the double-layer sign indicating that the patient had type 1 macular neovascularization (MNV), serous retinal pigment epithelial detachment (PED), and subretinal fluid (SRF) in his left eye (
Figure 1B). Optical coherence tomography angiography (OCTA) showed macular neovascularization (MNV) located in the area corresponding to the area of the RPE abnormalities (
Figure 1C). Based on these findings, he was diagnosed with nAMD in the left eye, and we began treatment with intravitreal injections of aflibercept (IVA).
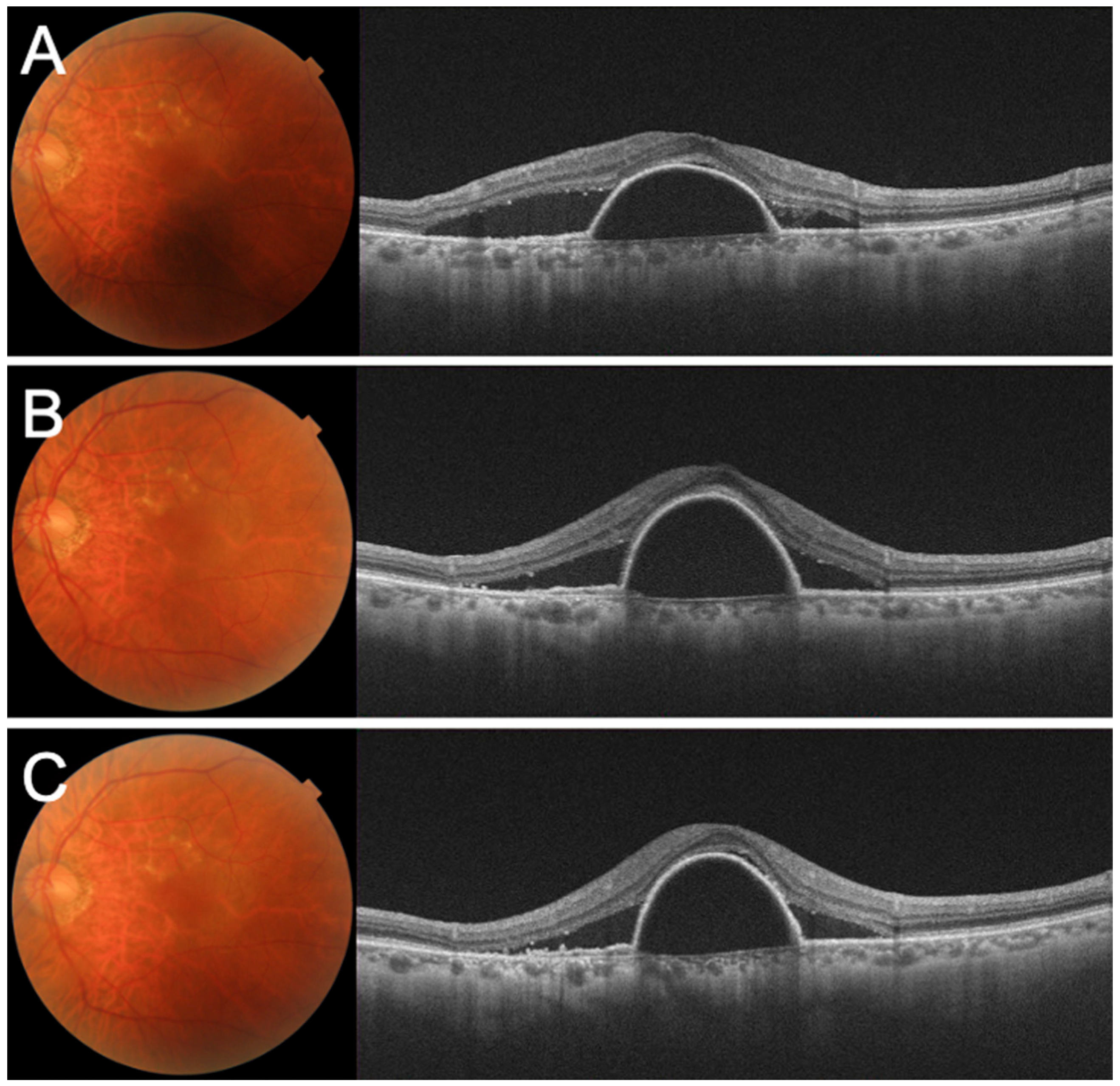
Despite the three-monthly IVA injections, the serous PED and SRF remained, and the BCVA gradually decreased to 0.1 (
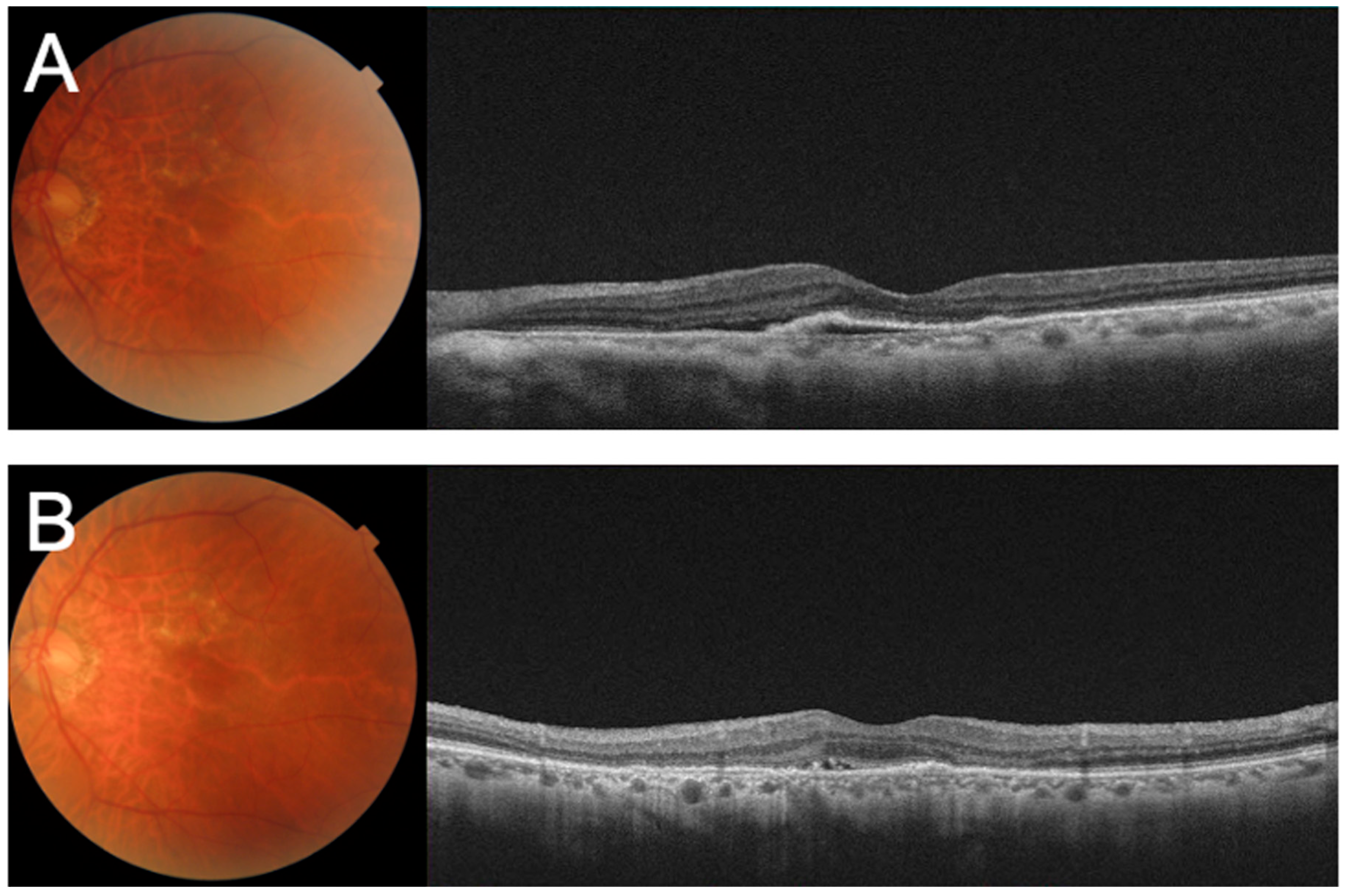
Figure 2A–C). We concluded that his left eye was refractory to aflibercept and switched his treatment to brolucizumab. After there monthly IVBr injections, the decimal BCVA improved to 0.3, and OCT showed that the serous PED and SRF had been resolved (
Figure 3A,B). He was then instructed to be aware of symptoms associated with IOI.
Three weeks after his third IVBr injection, he was referred to our hospital with a complaint of decreased vision in his left eye. The reduced vision had been noted two weeks earlier by the patient, but he failed to report it.
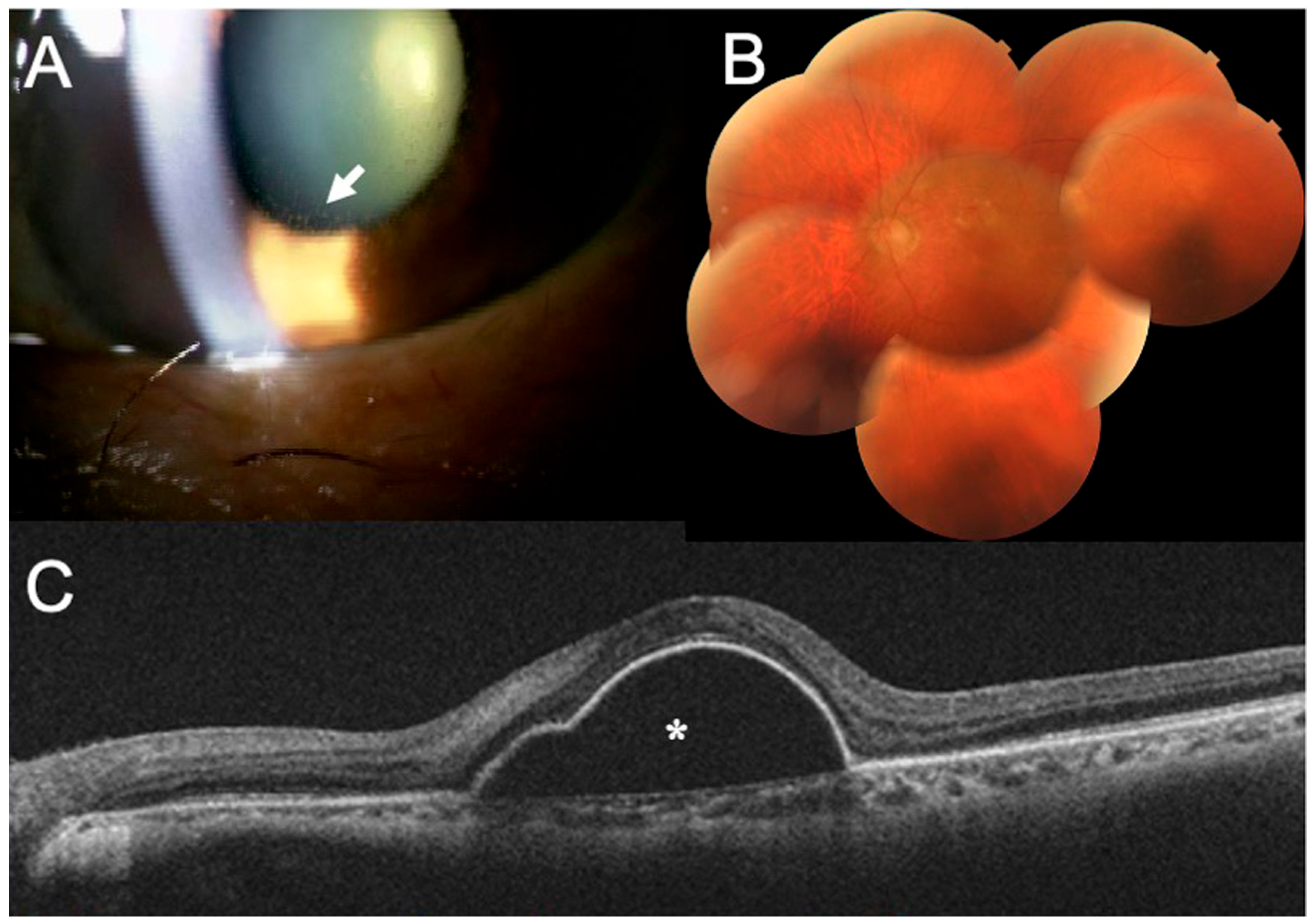
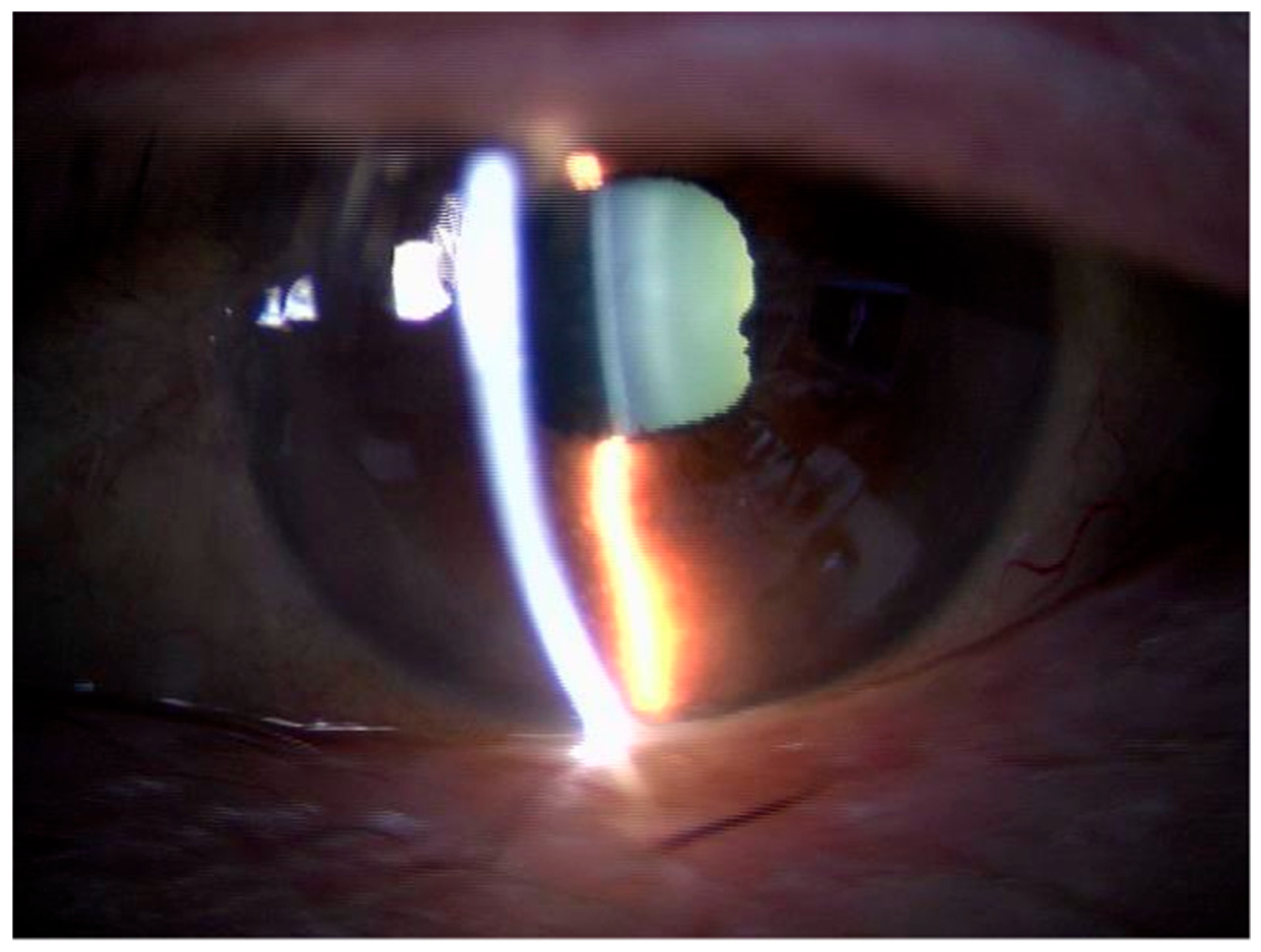
Our examination showed that his BCVA had decreased to 0.02, and the IOP increased to 43 mmHg in his left eye. Slit-lamp examination showed keratic precipitates in his left eye (
Figure 4A), and ophthalmoscopy showed an absence of retinal vasculitis in his left eye (
Figure 4B). However, OCT revealed the recurrence of the serous PED (
Figure 4C).
Because the left eye showed signs of IOI mainly in the anterior chamber, we began treating the IOI and ocular hypertension with an intravenous infusion of D-mannitol, 250 mg of oral acetazolamide 2/day supplemented with topical brinzolamide, timolol M-maleate, betamethasone, and latanoprost. The IOP normalized two weeks later, but his symptoms were unchanged with the BCVA in the left eye remaining at 0.02. However, the IOP was normal and no keratic precipitates were visible (
Figure 5). These treatments improved the inflammation, but the BCVA remained reduced. We suggest that the lack of a complete recovery of the BCVA was caused by both the recurrence of serous PED and the delay in treating the IOI.
Because we remembered that we had to explain the cause of his symptoms and the importance of early treatments repeatedly, we suspected that the patient had some degree of cognitive dysfunction. To assess his cognitive functionality quantitatively, the Mini-Mental State Examination (MMSE) was performed. A score of 27 points or higher is normal for this examination. His MMSE score was 20, and he was classified as highly suspicious of having dementia.
He did not wish to continue with additional treatments for his nAMD, so we followed him without any treatment.
3. Discussion
Brolucizumab is an anti-VEGF agent that was launched in 2019 for the treatment of nAMD. Brolucizumab was reported to be well tolerated; however, the incidence of IOI was higher with brolucizumab than with aflibercept. In 2020, the American Society of Retina Specialists circulated safety updates reporting on the development of retinal vasculitis (RV) in patients treated with brolucizumab. Some of these cases were reported to develop occlusive RV with an associated reduction in vision. The post-marketing report stated that the rate of RV and/or retinal vascular occlusion (RVO) was approximately 15.1 per 10,000 injections [
3]. It was also reported that severe vision reduction could develop secondary to retinal arteriolar occlusions after multiple IVBr injections [
4]. Therefore, retinal specialists have emphasized the need for early diagnosis and for prompt and appropriate treatment of the IOI to minimize the risk of the progression of these adverse events [
5]. For inflammation confined to the anterior chamber, frequent administration of potent topical corticosteroids may be adequate to control the inflammation. If a posterior segment inflammation is detected or even suspected, intravitreal, sub-tenon, or systemic corticosteroids should be administered [
3].
Anti-VEGF injections for nAMD have other serious ocular side-effects including endophthalmitis, retinal detachment, and vitreous hemorrhage. Therefore, patients are usually well-informed on the treatment protocols, and consent must be obtained before the first dose is injected. However, before initiating or switching to brolucizumab, the risk of an RO and vision reduction should be explained to the patient more carefully than at the start of anti-VEGF therapy. In addition, patients should be informed of the signs and symptoms associated with IOI, and the importance of immediately returning to the clinic if such signs and symptoms develop [
3]. However, not all nAMD patients comprehend the explanations about the treatment protocol or complications.
A meta-analysis combining both unadjusted and adjusted outcomes showed that dementia and Alzheimer’s disease (AD) were significantly associated with an increased risk of AMD [
6]. In the same way, patients with AMD were significantly associated with the development of AD or senile dementia compared with the controls [
7]. Johnson et al. first identified amyloid β-peptide (Aβ), the major proinflammatory component of senile plaques in AD, in the drusen of eyes with AMD. This indicated that amyloid β-peptide may play a fundamental role in the activation of complement-mediated events during drusen formation [
7]. Similar to its role in AD, Aβ in the drusen may lead to the progression of AD by causing oxidative stress, uncontrolled inflammation, and imbalanced angiogenesis. Such commonly shared pathways in AMD and AD could explain the association of AMD and AD. A previous meta-analysis has indicated that vision impairment is associated with an increased risk of dementia. The lack of physical and social activities in the visually impaired elderly may predispose them to cognitive decline [
8].
Several methods have been used to assess the relationship between dementia and AMD. The mini-mental state examination (MMSE) is the most widely used short cognitive screening test because it is quick and easy to administer in a clinical setting. The MMSE evaluates cognitive function by scoring the degree of memory retained, calculations, languages, and disorientation based on the answers to 11 questions. The maximum MMSE score is 30 points, and patients scoring less than 26 are classified as having mild cognitive impairment, and those scoring less than 21 are classified as having suspected dementia. Rong et al. compared the cognitive function scores between AMD patients and control subjects using various examinations including MMSE [
6]. The results showed that patients with AMD had significantly lower MMSE summary scores than the controls, suggesting the possibility of subclinical dementia. In our case, we diagnosed his left eye as refractory to aflibercept and switched the treatment to brolucizumab. Before starting the treatment, we explained the complications and treatment schedule of the anti-VEGF therapy. Since the patient, like other nAMD patients, did not question our explanations, we assumed that he fully understood the anti-VEGF treatment. In fact, he was treated with aflibercept according to the plan.
Before starting the brolucizumab, we carefully explained to him the risk of IOI and vision loss after IVBr. We informed the patient on the symptoms associated with IOI after IVBr and the importance of immediately returning to the clinic if he experienced such symptoms. Unfortunately, no family members were present at the time of the explanation. Although it appeared that he understood our explanation well, he came to our clinic two weeks after he became aware of a reduction in vision in his left eye. Although the inflammation improved with the topical steroids, initiating treatment for the IOI required time, and the vision did not recover to earlier levels. We suspected that he did not return because of the patient’s cognitive impairment as demonstrated by his MMSE score of 20.
Our findings demonstrated the importance of determining the cognitive function of patients with suspected cognitive reduction before starting treatment and explain the sign and symptoms of IOI to the family members as well as the patient. For patients with suspected dementia, it has been considered that more frequent follow-up visits should be made to detect the IOI and RO as early as possible. In addition, to reduce the development of IOI following IVBr, prophylactic sub-tenon injections of triamcinolone acetonide (STTA) should also be considered [
1].


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}