
Artificial Intelligence and Neurosurgery: Tracking Antiplatelet Response Patterns for Endovascular Intervention


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Indications for Antiplatelet Therapy
3.1.1. Stents
3.1.2. WEB Embolization
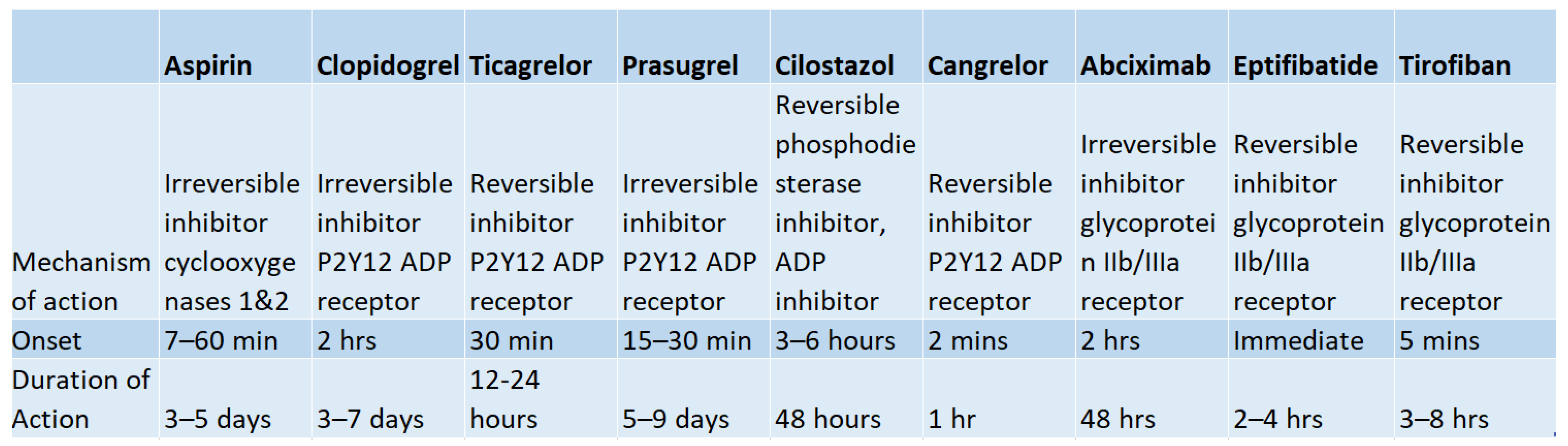
4. Antiplatelet Regimens
4.1. Aspirin
4.2. Clopidogrel
4.3. Aspirin and Clopidogrel
4.4. Clopidogrel Non-Responders
4.5. Aspirin and Ticagrelor
4.6. Alternative Agents
4.6.1. Prasugrel
4.6.2. Cilostazol
4.6.3. Abciximab, Eptifibatide, and Tirofiban
5. Antiplatelet Therapy Monitoring
5.1. PRU Monitoring
5.2. Thromboelastography (TEG) Platelet Mapping
6. Bridging Medications
6.1. Cangrelor
6.2. Tirofiban
7. Use of AI to Monitor Antiplatelet Therapy
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thachil, J. Antiplatelet therapy—A summary for the general physicians. Clin. Med. 2016, 16, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Passacquale, G.; Sharma, P.; Perera, D.; Ferro, A. Antiplatelet therapy in cardiovascular disease: Current status and future directions. Br. J. Clin. Pharmacol. 2022, 88, 2686–2699. [Google Scholar] [CrossRef] [PubMed]
- Patrono, C.; Morais, J.; Baigent, C.; Collet, J.P.; Fitzgerald, D.; Halvorsen, S.; Rocca, B.; Siegbehan, A.; Storey, R.F.; Vilahur, G. Antiplatelet agents for the treatment and prevention of coronary atherothrombosis. J. Am. Coll. Cardiol. 2017, 70, 1760–1776. [Google Scholar] [CrossRef] [PubMed]
- Montinari, M.R.; Minelli, S.; De Caterina, R. The first 3500 years of aspirin history from its roots–A concise summary. Vasc. Pharmacol. 2019, 113, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, X.; Yu, Y.; Han, R. Continuation versus discontinuation of aspirin-based antiplatelet therapy for perioperative bleeding and ischaemic events in adults undergoing neurosurgery: Protocol for a systematic review and meta-analysis. BMJ Open 2021, 11, e046741. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.; Galper, B.Z.; Cohen, D.J.; Yeh, R.W.; Mauri, L. Balancing the risks of bleeding and stent thrombosis: A decision analytic model to compare durations of dual antiplatelet therapy after drug-eluting stents. Am. Heart J. 2015, 169, 222–233.e5. [Google Scholar] [CrossRef] [PubMed]
- Gurajala, I.; Gopinath, R. Perioperative management of patient with intracoronary stent presenting for noncardiac surgery. Ann. Card. Anaesth. 2016, 19, 122–131. [Google Scholar] [CrossRef]
- Faught, R.W.; Satti, S.R.; Hurst, R.W.; Pukenas, B.A.; Smith, M.J. Heterogeneous practice patterns regarding antiplatelet medications for neuroendovascular stenting in the USA: A multicenter survey. J. NeuroInterv. Surg. 2014, 6, 774–779. [Google Scholar] [CrossRef]
- Tonetti, D.A.; Jankowitz, B.T.; Gross, B.A. Antiplatelet therapy in flow diversion. Neurosurgery 2020, 86 (Suppl. 1), S47–S52. [Google Scholar] [CrossRef]
- Fiorella, D.; Thiabolt, L.; Albuquerque, F.C.; Deshmukh, V.R.; McDougall, C.G.; Rasmussen, P.A. Antiplatelet therapy in neuroendovascular therapeutics. Neurosurg. Clin. N. Am. 2005, 16, 517–540. [Google Scholar] [CrossRef]
- Kim, K.S.; Fraser, J.F.; Grupke, S.; Cook, A.M. Management of antiplatelet therapy in patients undergoing neuroendovascular procedures. J. Neurosurg. 2018, 129, 890–905. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Yoshimura, S.; Milot, G.; Fiehler, J.; Jayaraman, M.; Dorn, F.; Taylor, A.; Liu, J.; Albuquerque, F.; Jensen, M.E.; et al. Considerations for Antiplatelet Management of Carotid Stenting in the Setting of Mechanical Thrombectomy: A Delphi Consensus Statement. AJNR Am. J. Neuroradiol. 2020, 41, 2274–2279. [Google Scholar] [CrossRef] [PubMed]
- Ryu, C.W.; Park, S.; Shin, H.S.; Koh, J.S. Complications in Stent-Assisted Endovascular Therapy of Ruptured Intracranial Aneurysms and Relevance to Antiplatelet Administration: A Systematic Review. AJNR Am. J. Neuroradiol. 2015, 36, 1682–1688. [Google Scholar] [CrossRef] [PubMed]
- Yi, H.J.; Shin, D.S.; Kim, B.T.; Lee, D.H.; Sung, J.H. Comparison of Neuroform Atlas Stent-Assisted Coiling and Coiling Alone in Ruptured Intracranial Aneurysms: A Propensity Score Matching Analysis. Neurosurgery 2023, 92, 607–614. [Google Scholar] [CrossRef]
- Hwang, G.; Jung, C.; Park, S.Q.; Kang, H.S.; Lee, S.H.; Oh, C.W.; Chung, Y.S.; Han, M.H.; Kwon, O.K. Thromboembolic complications of elective coil embolization of unruptured aneurysms: The effect of oral antiplatelet preparation on periprocedural thromboembolic complication. Neurosurgery 2010, 67, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Delgado Almandoz, J.E.; Kadkhodayan, Y.; Crandall, B.M.; Scholz, J.M.; Fease, J.L.; Tubman, D.E. Variability in initial response to standard clopidogrel therapy, delayed conversion to clopidogrel hyper-response, and associated thromboembolic and hemorrhagic complications in patients undergoing endovascular treatment of unruptured cerebral aneurysms. J. Neurointerv. Surg. 2014, 6, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Layton, K.F.; Cloft, H.J.; Gray, L.A.; Lewis, D.A.; Kallmes, D.F. Balloon-assisted coiling of intracranial aneurysms: Evaluation of local thrombus formation and symptomatic thromboembolic complications. AJNR Am. J. Neuroradiol. 2007, 28, 1172–1175. [Google Scholar] [CrossRef]
- Podlasek, A.; Al Sultan, A.A.; Assis, Z.; Kashani, N.; Goyal, M.; Almekhlafi, M.A. Outcome of intracranial flow diversion according to the antiplatelet regimen used: A systematic review and meta-analysis. J. Neurointerv. Surg. 2020, 12, 148–155. [Google Scholar] [CrossRef]
- Kilburg, C.; Taussky, P.; Kalani, M.Y.; Park, M.S. Novel use of flow diversion for the treatment of aneurysms associated with arteriovenous malformations. Neurosurg. Focus 2017, 42, E7. [Google Scholar] [CrossRef]
- Beaty, N.B.; Campos, J.K.; Colby, G.P.; Lin, L.M.; Bender, M.T.; Xu, R.; Coon, A.L. Pipeline Flex Embolization of Flow-Related Aneurysms Associated with Arteriovenous Malformations: A Case Report. Interv. Neurol. 2018, 7, 164–170. [Google Scholar] [CrossRef]
- Phuc, D.D.; Thuan, D.D.; Dai, P.D.; Duc, D.M.; Anh, N.Q.; Nga, N.T.; Toi, C.D.; Phuong, D.V.; Mai, D.T. Surpass Flow-Diverter in the Treatment of Two Wide-Neck Aneurysms in the Scheme of an Arteriovenous Malformation Patient: A Case Study. Open Access Maced. J. Med. Sci. 2019, 7, 4316–4318. [Google Scholar] [CrossRef] [PubMed]
- Hou, K.; Xu, K.; Chen, X.; Wang, Y.; Li, K.; Yu, J. Endovascular treatment for the flow-related aneurysm originating from an anterior inferior cerebellar artery supplying the cerebellar arteriovenous malformation. Interv. Neuroradiol. J. Peritherapeutic Neuroradiol. Surg. Proced. Relat. Neurosci. 2020, 26, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Schirmer, C.M.; Bulsara, K.R.; Al-Mufti, F.; Haranhalli, N.; Thibault, L.; Hetts, S.W. SNIS Standards and Guidelines Committee. Antiplatelets and antithrombotics in neurointerventional procedures: Guideline update. J. Neurointerv. Surg. 2023, 1–10. [Google Scholar] [CrossRef]
- Alexander, M.J.; Zauner, A.; Chaloupka, J.C.; Baxter, B.; Callison, R.C.; Gupta, R.; Song, S.S.; Yu, W.; WEAVE Trial Sites and Interventionalists. WEAVE Trial: Final Results in 152 On-Label Patients. Stroke 2019, 50, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Pierot, L.; Spelle, L.; Molyneux, A.; Byrne, J. WEBCAST and French Observatory Investigators: Clinical and anatomical follow-up in patients with aneurysms treated with the WEB device: 1-year follow-up report in the cumulated population of 2 prospective, multicenter series (WEBCAST and French Observatory). Neurosurgery 2016, 78, 133–141. [Google Scholar] [PubMed]
- Pierot, L.; Liebig, T.; Sychra, V.; Kadziolka, K.; Dorn, F.; Strasilla, C.; Kabbasch, C.; Klisch, J. Intrasaccular flow-disruption treatment of intracranial aneurysms: Preliminary results of a multicenter clinical study. Am. J. Neuroradiol. 2012, 33, 1232–1238. [Google Scholar] [CrossRef] [PubMed]
- Hurst, R. Response to letter to the editor: Antiplatelet therapy and the WEB II device. Neuroradiol. J. 2014, 27, 370. [Google Scholar] [CrossRef]
- Angiolillo, D.J. The evolution of antiplatelet therapy in the treatment of acute coronary syndromes: From aspirin to the present day. Drugs 2012, 72, 2087–2116. [Google Scholar] [CrossRef]
- Franchi, F.; Angiolillo, D.J. Novel antiplatelet agents in acute coronary syndrome. Nat. Rev. Cardiol. 2015, 12, 30–47. [Google Scholar] [CrossRef]
- Lee, M.; Saver, J.L.; Hong, K.S.; Rao, N.M.; Wu, Y.L.; Ovbiagele, B. Risk–benefit profile of long-term dual-versus single-antiplatelet therapy among patients with ischemic stroke: A systematic review and meta-analysis. Ann. Intern. Med. 2013, 159, 463–470. [Google Scholar] [CrossRef]
- Diener, H.C.; Bogousslavsky, J.; Brass, L.M.; Cimminiello, C.; Csiba, L.; Kaste, M.; Rupprecht, H.J. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): Randomised, double-blind, placebo-controlled trial. Lancet 2004, 364, 331–337. [Google Scholar] [CrossRef] [PubMed]
- sPs3 Investigators. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. N. Engl. J. Med. 2012, 367, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Fox, K.A.; Hacke, W.; Berger, P.B.; Black, H.R.; Boden, W.E.; Cacoub, P.; Cohen, E.A.; Creager, M.A.; Topol, E.J.; et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N. Engl. J. Med. 2006, 354, 1706–1717. [Google Scholar] [CrossRef] [PubMed]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Wilson, J.A.; et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef] [PubMed]
- Floyd, C.N.; Ferro, A. Antiplatelet drug resistance: Molecular insights and clinical implications. Prostaglandins Other Lipid Mediat. 2015, 120, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Pandey, C.P.; Misra, A.; Negi, M.P.S.; Kanuri, B.N.; Chhonker, Y.S.; Bhatta, R.S.; Narain, V.S.; Dikshit, M. Aspirin & clopidogrel non-responsiveness & its association with genetic polymorphisms in patients with myocardial infarction. Indian J. Med. Res. 2019, 150, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.J.; Bernardo, E.; Sabaté, M.; Jimenez-Quevedo, P.; Costa, M.A.; Palazuelos, J.; Hernández-Antolin, R.; Moreno, R.; Escaned, J.; Alfonso, F.; et al. Impact of platelet reactivity on cardiovascular outcomes in patients with type 2 diabetes mellitus and coronary artery disease. J. Am. Coll. Cardiol. 2007, 50, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- Ulehlova, J.; Slavik, L.; Kucerova, J.; Krcova, V.; Vaclavik, J.; Indrak, K. Genetic polymorphisms of platelet receptors in patients with acute myocardial infarction and resistance to antiplatelet therapy. Genet. Test. Mol. Biomark. 2014, 18, 599–604. [Google Scholar] [CrossRef]
- Simon, T.; Verstuyft, C.; Mary-Krause, M.; Quteineh, L.; Drouet, E.; Méneveau, N.; Becquemont, L. Genetic determinants of response to clopidogrel and cardiovascular events. N. Engl. J. Med. 2009, 360, 363–375. [Google Scholar] [CrossRef]
- Yi, X.; Wang, C.; Liu, P.; Fu, C.; Lin, J.; Chen, Y. Antiplatelet drug resistance is associated with early neurological deterioration in acute minor ischemic stroke in the Chinese population. J. Neurol. 2016, 263, 1612–1619. [Google Scholar] [CrossRef]
- Borchert, R.J.; Simonato, D.; Hickman, C.R.; Fuschi, M.; Thibault, L.; Henkes, H.; Fiorella, D.; Tan, B.Y.; Yeo, L.L.; Makalanda, H.L.D.; et al. P2Y12 inhibitors for the neurointerventionalist. Interv. Neuroradiol. J. Peritherapeutic Neuroradiol. Surg. Proced. Relat. Neurosci. 2022, 28, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Narata, A.P.; Amelot, A.; Bibi, R.; Herbreteau, D.; Angoulvant, D.; Gruel, Y.; Janot, K. Dual Antiplatelet Therapy Combining Aspirin and Ticagrelor for Intracranial Stenting Procedures: A Retrospective Single Center Study of 154 Consecutive Patients with Unruptured Aneurysms. Neurosurgery 2019, 84, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Harrington, R.A.; et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Tomaniak, M.; Chichareon, P.; Onuma, Y.; Deliargyris, E.N.; Takahashi, K.; Kogame, N.; Modolo, R.; Chang, C.C.; Rademaker-Havinga, T.; Storey, R.F.; et al. Benefit and Risks of Aspirin in Addition to Ticagrelor in Acute Coronary Syndromes: A Post Hoc Analysis of the Randomized GLOBAL LEADERS Trial. JAMA Cardiol. 2019, 4, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- Dobesh, P.P.; Oestreich, J.H. Ticagrelor: Pharmacokinetics, pharmacodynamics, clinical efficacy, and safety. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2014, 34, 1077–1090. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Chen, W.; Pan, Y.; Yan, H.; Meng, X.; Liu, L.; Wang, Y.; Wang, Y. Effect of ticagrelor versus clopidogrel on platelet reactivity measured by thrombelastography in patients with minor stroke or TIA. Aging 2020, 12, 20085–20094. [Google Scholar] [CrossRef] [PubMed]
- Akbari, S.H.; Reynolds, M.R.; Kadkhodayan, Y.; Cross, D.T., 3rd; Moran, C.J. Hemorrhagic complications after prasugrel (Effient) therapy for vascular neurointerventional procedures. J. Neurointerv. Surg. 2013, 5, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, Y.; Katayama, Y.; Uchiyama, S.; Yamaguchi, T.; Handa, S.; Matsuoka, K.; Ohashi, Y.; Tanahashi, N.; Yamamoto, H.; Hamada, C.; et al. Cilostazol for prevention of secondary stroke (CSPS 2): An aspirin-controlled, double-blind, randomised non-inferiority trial. Lancet Neurol. 2010, 9, 959–968. [Google Scholar] [CrossRef]
- Toyoda, K.; Uchiyama, S.; Yamaguchi, T.; Easton, J.D.; Kimura, K.; Hoshino, H.; Sakai, N.; Okada, Y.; Tanaka, K.; Kumagai, N.; et al. Dual antiplatelet therapy using cilostazol for secondary prevention in patients with high-risk ischaemic stroke in Japan: A multicentre, open-label, randomised controlled trial. Lancet Neurol. 2019, 18, 539–548. [Google Scholar] [CrossRef]
- Hoshino, H.; Toyoda, K.; Omae, K.; Ishida, N.; Uchiyama, S.; Kimura, K.; Sakai, N.; Okada, Y.; Tanaka, K.; Origasa, H.; et al. Dual Antiplatelet Therapy Using Cilostazol with Aspirin or Clopidogrel: Subanalysis of the CSPS.com Trial. Stroke 2021, 52, 3430–3439. [Google Scholar] [CrossRef]
- Topol, E.J.; Byzova, T.V.; Plow, E.F. Platelet GPIIb-IIIa blockers. Lancet 1999, 353, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Muñiz-Lozano, A.; Rollini, F.; Franchi, F.; Angiolillo, D.J. Update on platelet glycoprotein IIb/IIIa inhibitors: Recommendations for clinical practice. Ther. Adv. Cardiovasc. Dis. 2013, 7, 197–213. [Google Scholar] [CrossRef] [PubMed]
- Anton-Martin, P.; Matherne, E.; Kramer, J.; Joseph, N.; Rayburn, M. Cangrelor Dosing and Monitoring for Prevention of Acute Systemic-to-Pulmonary Artery Shunt Thrombosis in Neonates. J. Pediatr. Pharmacol. Ther. 2022, 27, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.C.; Behan, M.W.; Heptinstall, S. Inhibition of ADP-induced intracellular Ca2+ responses and platelet aggregation by the P2Y12 receptor antagonists AR-C69931MX and clopidogrel is enhanced by prostaglandin E1. Cell Calcium. 2004, 35, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Malinin, A.; Pokov, A.; Spergling, M.; Defranco, A.; Schwartz, K.; Schwartz, D.; Mahmud, E.; Atar, D.; Serebruany, V. Monitoring platelet inhibition after clopidogrel with the VerifyNow-P2Y12(R) rapid analyzer: The VERIfy Thrombosis risk ASsessment (VERITAS) study. Thromb Res. 2007, 119, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Almandoz, J.D.; Crandall, B.M.; Scholz, J.M.; Fease, J.L.; Anderson, R.E.; Kadkhodayan, Y.; Tubman, D.E. Last-recorded P2Y12 reaction units value is strongly associated with thromboembolic and hemorrhagic complications occurring up to 6 months after treatment in patients with cerebral aneurysms treated with the pipeline embolization device. Am. J. Neuroradiol. 2014, 35, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Higashiguchi, S.; Sadato, A.; Nakahara, I.; Matsumoto, S.; Hayakawa, M.; Adachi, K.; Hasebe, A.; Suyama, Y.; Omi, T.; Yamashiro, K.; et al. Reduction of thromboembolic complications during the endovascular treatment of unruptured aneurysms by employing a tailored dual antiplatelet regimen using aspirin and prasugrel. J. Neurointerv. Surg. 2021, 13, 1044–1048. [Google Scholar] [CrossRef] [PubMed]
- Volod, O.; Arabia, F.A.; Lam, L.D.; Runge, A.; Cheng, C.; Czer, L.S.C. Platelet Mapping by Thromboelastography and Whole Blood Aggregometry in Adult Patients Supported by Mechanical Circulatory Support Device on Aspirin Therapy. J. Extra-Corpor. Technol. 2020, 52, 13–21. [Google Scholar] [CrossRef]
- Volod, O.; Arabia, A.F.; Lam, L.D.; Runge, A.; Cheng, C.; Czer, L.S.C. Evaluation of the TEG® platelet mapping™ assay in blood donors. Thromb. J. 2007, 5, 3. [Google Scholar] [CrossRef]
- Van Tuyl, J.S.; Newsome, A.S.; Hollis, I.B. Perioperative bridging with glycoprotein IIb/IIIa inhibitors versus cangrelor: Balancing efficacy and safety. Ann. Pharmacother. 2019, 53, 726–737. [Google Scholar] [CrossRef]
- Entezami, P.; Holden, D.N.; Boulos, A.S.; Paul, A.R.; Field, N.C.; Nourollahzadeh, E.; Dalfino, J.C. Cangrelor dose titration using platelet function testing during cerebrovascular stent placement. Interv. Neuroradiol. 2021, 27, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Siebler, M.; Hennerici, M.G.; Schneider, D.; von Reutern, G.M.; Seitz, R.J.; Röther, J.; Witte, O.W.; Hamann, G.; Junghans, U.; Fiebach, J.B.; et al. Safety of Tirofiban in acute Ischemic Stroke: The SaTIS trial. Stroke 2011, 42, 2388–2392. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Lin, L.; Zhang, M.; Wu, Y.; Liu, C.; Li, X.; Huang, S.; Liang, C.; Wang, Y.; Feng, W.; et al. Safety and preliminary efficacy of early tirofiban treatment after alteplase in acute ischemic stroke patients. Stroke 2016, 47, 2649–2651. [Google Scholar] [CrossRef]
- Wu, C.; Wu, D.; Chen, J.; Li, C.; Ji, X. Why not intravenous thrombolysis in patients with recurrent stroke within 3 months? Aging Dis. 2018, 9, 309. [Google Scholar] [CrossRef] [PubMed]
- Kellert, L.; Hametner, C.; Rohde, S.; Bendszus, M.; Hacke, W.; Ringleb, P.; Stampfl, S. Endovascular stroke therapy: Tirofiban is associated with risk of fatal intracerebral hemorrhage and poor outcome. Stroke 2013, 44, 1453–1455. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.H.; Jeong, H.W.; Kim, S.T.; Kim, E.G. Adjuvant Tirofiban Injection Through Deployed Solitaire Stent as a Rescue Technique After failed Mechanical Thrombectomy in Acute Stroke. Neurointervention 2015, 10, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Geng, X.; Gao, J.; Hussain, M.; Moon, S.J.; Du, H.; Ding, Y. Intravenous Administration of Standard Dose Tirofiban after Mechanical Arterial Recanalization is Safe and Relatively Effective in Acute Ischemic Stroke. Aging Dis. 2019, 10, 1049–1057. [Google Scholar] [CrossRef]
- Ciccone, A.; Motto, C.; Abraha, I.; Cozzolino, F.; Santilli, I. Glycoprotein IIb–IIIa inhibitors for acute ischaemic stroke. Cochrane Database Syst. Rev. 2014, 45, e155–e156. [Google Scholar] [CrossRef]
- Kraft, P.; Schuhmann, M.K.; Fluri, F.; Lorenz, K.; Zernecke, A.; Stoll, G.; Nieswandt, B.; Kleinschnitz, C. Efficacy and Safety of Platelet Glycoprotein Receptor Blockade in Aged and Comorbid Mice with Acute Experimental Stroke. Stroke 2015, 46, 3502–3506. [Google Scholar] [CrossRef]
- King, S.; Short, M.; Harmon, C. Glycoprotein IIb/IIIa inhibitors: The resurgence of tirofiban. Vasc. Pharmacol. 2016, 78, 10–16. [Google Scholar] [CrossRef]
- Alshawabkeh, L.I.; Prasad, A.; Lenkovsky, F.; Makary, L.F.; Kandil, E.S.; Weideman, R.A.; Kelly, K.C.; Rangan, B.V.; Banerjee, S.; Brilakis, E.S. Outcomes of a preoperative “bridging” strategy with glycoprotein IIb/IIIa inhibitors to prevent perioperative stent thrombosis in patients with drug-eluting stents who undergo surgery necessitating interruption of thienopyridine administration. EuroInterv. J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2013, 9, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Savonitto, S.; D’Urbano, M.; Caracciolo, M.; Barlocco, F.; Mariani, G.; Nichelatti, M.; Klugmann, S.; De Servi, S. Urgent surgery in patients with a recently implanted coronary drug-eluting stent: A phase II study of ‘bridging’ antiplatelet therapy with tirofiban during temporary withdrawal of clopidogrel. Br. J. Anaesth. 2010, 104, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Rasmy, L.; Xiang, Y.; Feng, J.; Du, J.; Aguilar, D.; Dhoble, A.; Wang, Q.; Niu, S.; Hu, X.; et al. AI-aided dynamic prediction of bleeding and ischemic risk after coronary stenting and subsequent DAPT. bioRxiv 2022. [Google Scholar] [CrossRef]
- Fan, J.; Ma, X.; Wu, L.; Zhang, F.; Yu, X.; Zeng, W. Light Gradient Boosting Machine: An efficient soft computing model for estimating daily reference evapotranspiration with local and external meteorological data. Agric. Water Manag. 2019, 225, 105758. [Google Scholar] [CrossRef]
- Tolles, J.; Meurer, W.J. Logistic regression: Relating patient characteristics to outcomes. JAMA 2016, 316, 533–534. [Google Scholar] [CrossRef] [PubMed]
- Svetnik, V.; Liaw, A.; Tong, C.; Culberson, J.C.; Sheridan, R.P.; Feuston, B.P. Random forest: A classification and regression tool for compound classification and QSAR modeling. J. Chem. Inf. Comput. Sci. 2003, 43, 1947–1958. [Google Scholar] [CrossRef]
- Cho, K.; Van Merriënboer, B.; Gulcehre, C.; Bahdanau, D.; Bougares, F.; Schwenk, H.; Bengio, Y. Learning phrase representations using RNN encoder-decoder for statistical machine translation. arXiv 2014, arXiv:1406.1078. [Google Scholar]
- Choi, E.; Bahadori, M.T.; Kulas, J.A.; Schuetz, A.; Stewart, W.F.; Sun, J. RETAIN: An interpretable predictive model for healthcare using reverse time attention mechanism. Adv. Neural Inf. Process. Syst. 2016, 29, 3512–3520. [Google Scholar]
- Rasmy, L.; Wu, Y.; Wang, N.; Geng, X.; Zheng, W.J.; Wang, F.; Wu, H.; Xu, H.; Zhi, D. A study of generalizability of recurrent neural network-based predictive models for heart failure onset risk using a large and heterogeneous EHR data set. J. Biomed. Inform. 2018, 84, 11–16. [Google Scholar] [CrossRef]
- Fernández-Ruiz, I. Machine learning predicts risk in ACS. Nat. Rev. Cardiol. 2021, 18, 230. [Google Scholar] [CrossRef]
- D’Ascenzo, F.; De Filippo, O.; Gallone, G.; Mittone, G.; Deriu, M.A.; Iannaccone, M.; Ariza-Solé, A.; Liebetrau, C.; Manzano-Fernández, S.; Quadri, G.; et al. Machine learning-based prediction of adverse events following an acute coronary syndrome (PRAISE): A modelling study of pooled datasets. Lancet 2021, 397, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Jaja, B.N.; Cusimano, M.D.; Etminan, N.; Hanggi, D.; Hasan, D.; Ilodigwe, D.; Lantigua, H.; Le Roux, P.L.; Lo, B.; Macdonald, R.L.; et al. Clinical prediction models for aneurysmal subarachnoid hemorrhage: A systematic review. Neurocritical Care 2013, 18, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Risselada, R.; Lingsma, H.F.; Bauer-Mehren, A.; Friedrich, C.M.; Molyneux, A.J.; Kerr, R.S.C.; Yarnold, K.J.; Sneade, M.; Steyerberg, E.W.; Sturkenboom, M.C.J.M. Prediction of 60 day case-fatality after aneurysmal subarachnoid haemorrhage: Results from the International Subarachnoid Aneurysm Trial (ISAT). Eur. J. Epidemiol. 2010, 25, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Abulhasan, Y.B.; Alabdulraheem, N.; Simoneau, G.; Angle, M.R.; Teitelbaum, J. Mortality after spontaneous subarachnoid hemorrhage: Causality and validation of a prediction model. World Neurosurg. 2018, 112, e799–e811. [Google Scholar] [CrossRef] [PubMed]
- Zeiler, F.A.; Lo, B.W.Y.; Akoth, E.; Silvaggio, J.; Kaufmann, A.M.; Teitelbaum, J.; West, M. Predicting outcome in subarachnoid hemorrhage (SAH) utilizing the Full Outline of UnResponsiveness (FOUR) score. Neurocritical Care 2017, 27, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Hostettler, I.C.; Sebök, M.; Ambler, G.; Muroi, C.; Prömmel, P.; Neidert, M.C.; Cristoph, M.; Johannes, K.; Pangalu, A.; Germans, M.R. Validation and Optimization of barrow neurological institute score in prediction of adverse events and functional outcome after subarachnoid hemorrhage—Creation of the HATCH (Hemorrhage, Age, Treatment, Clinical State, Hydrocephalus) Score. Neurosurgery 2020, 88, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Jaja, B.N.R.; Saposnik, G.; Lingsma, H.F.; Macdonald, E.; Thorpe, K.E.; Mamdani, M.; Steyerberg, E.W.; Molyneux, A.; Manoel, A.L.O.; Schatlo, B.; et al. Development and validation of outcome prediction models for aneurysmal subarachnoid haemorrhage: The SAHIT multinational cohort study. BMJ 2018, 360, j5745. [Google Scholar] [CrossRef]
- Witsch, J.; Frey, H.P.; Patel, S.; Park, S.; Lahiri, S.; Schmidt, J.M.; Agarwal, S.; Falo, M.C.; Velazquez, A.; Claassen, J.; et al. Prognostication of long-term outcomes after subarachnoid hemorrhage: The FRESH score. Ann. Neurol. 2016, 80, 46–58. [Google Scholar] [CrossRef]
- Van Donkelaar, C.E.; Bakker, N.A.; Birks, J.; Veeger, N.J.; Metzemaekers, J.D.; Molyneux, A.J.; Groen, R.J.M.; van Dijk, J.M.C. Prediction of outcome after aneurysmal subarachnoid hemorrhage: Development and validation of the SAFIRE grading scale. Stroke 2019, 50, 837–844. [Google Scholar] [CrossRef]
- Katsuki, M.; Kawamura, S.; Koh, A. Easily Created Prediction Model Using Automated Artificial Intelligence Framework (Prediction One, Sony Network Communications Inc., Tokyo, Japan) for Subarachnoid Hemorrhage Outcomes Treated by Coiling and Delayed Cerebral Ischemia. Cureus 2021, 13, e15695. [Google Scholar] [CrossRef]
- Rubbert, C.; Patil, K.R.; Beseoglu, K.; Mathys, C.; May, R.; Kaschner, M.G.; Sigl, B.; Teichert, N.A.; Boos, J.; Caspers, J.; et al. Prediction of outcome after aneurysmal subarachnoid haemorrhage using data from patient admission. Eur. Radiol. 2018, 28, 4949–4958. [Google Scholar] [CrossRef] [PubMed]
- De Toledo, P.; Rios, P.M.; Ledezma, A.; Sanchis, A.; Alen, J.F.; Lagares, A. Predicting the outcome of patients with subarachnoid hemorrhage using machine learning techniques. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 794–801. [Google Scholar] [CrossRef] [PubMed]
- De Jong, G.; Aquarius, R.; Sanaan, B.; Bartels, R.H.; Grotenhuis, J.A.; Henssen, D.J.; Boogaarts, H.D. Prediction models in aneurysmal subarachnoid hemorrhage: Forecasting clinical outcome with artificial intelligence. Neurosurgery 2021, 88, E427–E434. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Zhang, J.; Shan, B.; He, M.; Xu, J. XGBoost Machine Learning Algorithm for Prediction of Outcome in Aneurysmal Subarachnoid Hemorrhage. Neuropsychiatr. Dis. Treat. 2022, 18, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.M.; Kistler, J.P.; Davis, J.M. Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning. Neurosurgery 1980, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Frontera, J.A.; Claassen, J.; Schmidt, J.M.; Wartenberg, K.E.; Temes, R.; Connolly, E.S.; Macdonald, R.; Loch, R.; Mayer, S.A. Prediction of symptomatic vasospasm after subarachnoid hemorrhage: The modified fisher scale. Neurosurgery 2006, 59, 21–27. [Google Scholar] [PubMed]
- Ahn, S.H.; Savarraj, J.P.; Pervez, M.; Jones, W.; Park, J.; Jeon, S.B.; Choi, H.A. The subarachnoid hemorrhage early brain edema score predicts delayed cerebral ischemia and clinical outcomes. Neurosurgery 2018, 83, 137–145. [Google Scholar] [CrossRef]
- Claassen, J.; Carhuapoma, J.R.; Kreiter, K.T.; Du, E.Y.; Connolly, E.S.; Mayer, S.A. Global cerebral edema after subarachnoid hemorrhage: Frequency, predictors, and impact on outcome. Stroke 2002, 33, 1225–1232. [Google Scholar] [CrossRef]
- De Oliveira Manoel, A.L.; Jaja, B.N.; Germans, M.R.; Yan, H.; Qian, W.; Kouzmina, E.; Marotta, T.R.; Turkel-Parrella, D.; Schweizer, T.A.; Macdonald, R.L.; et al. The VASOGRADE: A simple grading scale for prediction of delayed cerebral ischemia after subarachnoid hemorrhage. Stroke 2015, 46, 1826–1831. [Google Scholar] [CrossRef]
- Fang, Y.; Lu, J.; Zheng, J.; Wu, H.; Araujo, C.; Reis, C.; Lenahan, C.; Zhu, S.; Chen, S.; Zhang, J. Comparison of aneurysmal subarachnoid hemorrhage grading scores in patients with aneurysm clipping and coiling. Sci. Rep. 2020, 10, 1–9. [Google Scholar]
- Savarraj, J.P.; Hergenroeder, G.W.; Zhu, L.; Chang, T.; Park, S.; Megjhani, M.; Vahidy, F.S.; Zhao, Z.; Kitagawa, R.S.; Choi, H.A. Machine learning to predict delayed cerebral ischemia and outcomes in subarachnoid hemorrhage. Neurology 2021, 96, e553–e562. [Google Scholar] [CrossRef] [PubMed]
- Ramos, L.A.; van der Steen, W.E.; Barros, R.S.; Majoie, C.B.; van den Berg, R.; Verbaan, D.; Marquering, H.A. Machine learning improves prediction of delayed cerebral ischemia in patients with subarachnoid hemorrhage. J. Neurointerv. Surg. 2019, 11, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Megjhani, M.; Terilli, K.; Weiss, M.; Savarraj, J.; Chen, L.H.; Alkhachroum, A.; Roh, D.J.; Agarwai, S.; Connolly Jr, E.S.; Park, S.; et al. Dynamic detection of delayed cerebral ischemia: A study in 3 centers. Stroke 2021, 52, 1370–1379. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Megjhani, M.; Frey, H.P.; Grave, E.; Wiggins, C.; Terilli, K.L.; Roh, D.J.; Velazquez, A.; Agarwal, S.; Elhadad, N.; et al. Predicting delayed cerebral ischemia after subarachnoid hemorrhage using physiological time series data. J. Clin. Monit. Comput. 2019, 33, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Taghavi, R.M.; Zhu, G.; Wintermark, M.; Kuraitis, G.M.; Sussman, E.S.; Pulli, B.; Biniam, B.; Ostmeier, S.; Steinberg, G.K.; Heit, J.J. Prediction of delayed cerebral ischemia after cerebral aneurysm rupture using explainable machine learning approach. Interv. Neuroradiol. J. Peritherapeutic Neuroradiol. Surg. Proced. Relat. Neurosci. 2023. [Google Scholar] [CrossRef] [PubMed]
- Greving, J.P.; Wermer, M.J.; Brown, R.D., Jr.; Morita, A.; Juvela, S.; Yonekura, M.; Ishibashi, T.; Torner, J.C.; Nakayama, T.; Algra, A.; et al. Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms: A pooled analysis of six prospective cohort studies. Lancet Neurol. 2014, 13, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Greving, J.P.; Wermer, M.J.H.; Brown, R.D.; Morita, A.; Juvela, S.; Yonekura, M.; Ishibashi, T.; Torner, J.C.; Nakayama, T.; Rinkel, G.J.E.; et al. ELAPSS score for prediction of risk of growth of unruptured intracranial aneurysms. Neurology 2017, 88, 1600–1606. [Google Scholar] [CrossRef]
- Backes, D.; Rinkel, G.J.; Greving, J.P.; Velthuis, B.K.; Murayama, Y.; Takao, H.; Ishibashi, T.; Igase, M.; Terbrugge, K.G.; Agid, R.; et al. The unruptured intracranial aneurysm treatment score: A multidisciplinary consensus. Neurology 2015, 85, 881–889. [Google Scholar] [CrossRef]
- Staartjes, V.E.; Sebök, M.; Blum, P.G.; Serra, C.; Germans, M.R.; Krayenbühl, N.; Regli, L.; Esposito, G. Development of machine learning-based preoperative predictive analytics for unruptured intracranial aneurysm surgery: A pilot study. Acta Neurochir. 2020, 162, 2759–2765. [Google Scholar] [CrossRef]
- Zanaty, M.; Park, B.J.; Seaman, S.C.; Cliffton, W.E.; Woodiwiss, T.; Piscopo, A.; Howard, M.A.; Abode-Iyamah, K. Predicting Chronic Subdural Hematoma Recurrence and Stroke Outcomes While withholding Antiplatelet and Anticoagulant Agents. Front. Neurol. 2020, 10, 1401. [Google Scholar] [CrossRef]
- Labovitz, D.L.; Shafner, L.; Reyes Gil, M.; Virmani, D.; Hanina, A. Using Artificial Intelligence to Reduce the Risk of Nonadherence in Patients on Anticoagulation Therapy. Stroke 2017, 48, 1416–1419. [Google Scholar] [CrossRef] [PubMed]
- Babel, A.; Taneja, R.; Mondello Malvestiti, F.; Monaco, A.; Donde, S. Artificial intelligence solutions to increase medication adherence in patients with non-communicable diseases. Front. Digit. Health 2021, 3, 669869. [Google Scholar] [CrossRef] [PubMed]
- Mofatteh, M. Neurosurgery and artificial intelligence. AIMS Neurosci. 2021, 8, 477–495. [Google Scholar] [CrossRef] [PubMed]
- Bellini, V.; Valente, M.; Del Rio, P.; Bignami, E. Artificial intelligence in thoracic surgery: A narrative review. J. Thorac. Dis. 2021, 13, 6963–6975. [Google Scholar] [CrossRef] [PubMed]
- Deo, R.C. Machine Learning in Medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, J.; Jahangir, K.; Mashkoor, Y.; Sultana, N.; Mehmood, D.; Ashraf, M.; Hafeez, M.H. The future of artificial intelligence in neurosurgery: A narrative review. Surg. Neurol. Int. 2022, 13, 536. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year of Publication | Predictive Model Used | Condition Studied | Results |
|---|---|---|---|---|
| Li et al.; Fan et al. [73,74] | 2022, 2019 | light gradient boosting machine | Risks of ischemic/bleeding events for patients who had undergone DES implantation | AUC of 0.82 for ischemia and 0.77 for bleeding |
| Li et al.; Tolles et al. [73,75] | 2022, 2016 | Logistic regression | Risks of ischemic/bleeding events for patients who had undergone DES implantation | AUC of 0.82 for ischemia and 0.77 for bleeding |
| Li et al.; Svetnik et al. [73,76] | 2022, 2003 | Random forest | Risks of ischemic/bleeding events for patients who had undergone DES implantation | AUC of 0.82 for ischemia and 0.77 for bleeding |
| Li et al.; Cho et al. [73,77] | 2022, 2004 | Random forest | Risks of ischemic/bleeding events for patients who had undergone DES implantation | AUC of 0.82 for ischemia and 0.77 for bleeding |
| Li et al.; Choi et al. [73,78] | 2022, 2016 | RETAIN | Risks of ischemic/bleeding events for patients who had undergone DES implantation | AUC of 0.82 for ischemia and 0.77 for bleeding |
| D’Ascenzo [81] | 2021 | PRAISE | ACS syndrome outcomes | AUC for the 1-year risk of MI of 0.74 in the internal validation cohort and 0.81 in the external validation cohort and an AUC for the 1-year risk of major bleeding of 0.70 in the internal validation cohort and 0.86 in external validation cohort |
| Jaja et al.; Risselada et al.; Abulhasan et al.; Zeiler et al.; Hostettler et al.; Jaja et al.; Witsch et al.; van Donkelaar et al., 2019 [82,83,84,85,86,87,88,89] | 2013, 2010, 2018; 2017, 2020, 2018; 2016, 2019 | Statistical methods | SAH outcomes | 0.70–0.90 |
| Rubbert et al. [91] | 2018 | Random forests | SAH outcomes | 71% accuracy |
| De Toledo et al. [92] | 2009 | Random forests | SAH outcomes | 0.84 AUC |
| Katsuki et al.; de Jong et al.; Wang et al. [90,93,94] | 2020, 2021, 2022 | Deep learning | SAH outcomes | Approximately 0.90 AUC |
| Ramos et al. [102] | 2019 | Machine learning | SAH outcomes | AUC 0.74 |
| Meghjani et al. [103] | 2021 | L2-regularized logistic regression, random forest, and support vector machines models | SAH outcomes | AUC 0.83 |
| De Jong et al. [93] | 2021 | feedforward artificial neural networks (ffANNs) | SAH outcomes | AUC 0.72 |
| Park et al. [104] | 2019 | Random kernel | SAH outcomes | AUC 0.77 |
| Savarraj et al. [101] | 2021 | Machine learning | SAH outcomes | AUC 0.75 |
| Taghavi et al. [105] | 2023 | Random Forest | SAH outcomes | AUC 0.780 |
| Staartjes et al. [109] | 2020 | Machine learning models | UIA outcomes | AUC 0.63–0.77 |
| Zanaty et al. [110] | 2020 | Machine learning models | Recurrence of cSDH | AUC of 0.91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saigal, K.; Patel, A.B.; Lucke-Wold, B. Artificial Intelligence and Neurosurgery: Tracking Antiplatelet Response Patterns for Endovascular Intervention. Medicina 2023, 59, 1714. https://doi.org/10.3390/medicina59101714
Saigal K, Patel AB, Lucke-Wold B. Artificial Intelligence and Neurosurgery: Tracking Antiplatelet Response Patterns for Endovascular Intervention. Medicina. 2023; 59(10):1714. https://doi.org/10.3390/medicina59101714
Chicago/Turabian StyleSaigal, Khushi, Anmol Bharat Patel, and Brandon Lucke-Wold. 2023. "Artificial Intelligence and Neurosurgery: Tracking Antiplatelet Response Patterns for Endovascular Intervention" Medicina 59, no. 10: 1714. https://doi.org/10.3390/medicina59101714
APA StyleSaigal, K., Patel, A. B., & Lucke-Wold, B. (2023). Artificial Intelligence and Neurosurgery: Tracking Antiplatelet Response Patterns for Endovascular Intervention. Medicina, 59(10), 1714. https://doi.org/10.3390/medicina59101714