
Comparing the Efficacy of Intra-Articular Single Platelet-Rich Plasma(PRP) versus Novel Crosslinked Hyaluronic Acid for Early-Stage Knee Osteoarthritis: A Prospective, Double-Blind, Randomized Controlled Trial

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Randomization and Masking
2.3. PRP and HA Preparation
2.4. Outcome Assessment
2.5. Statistical Analysis
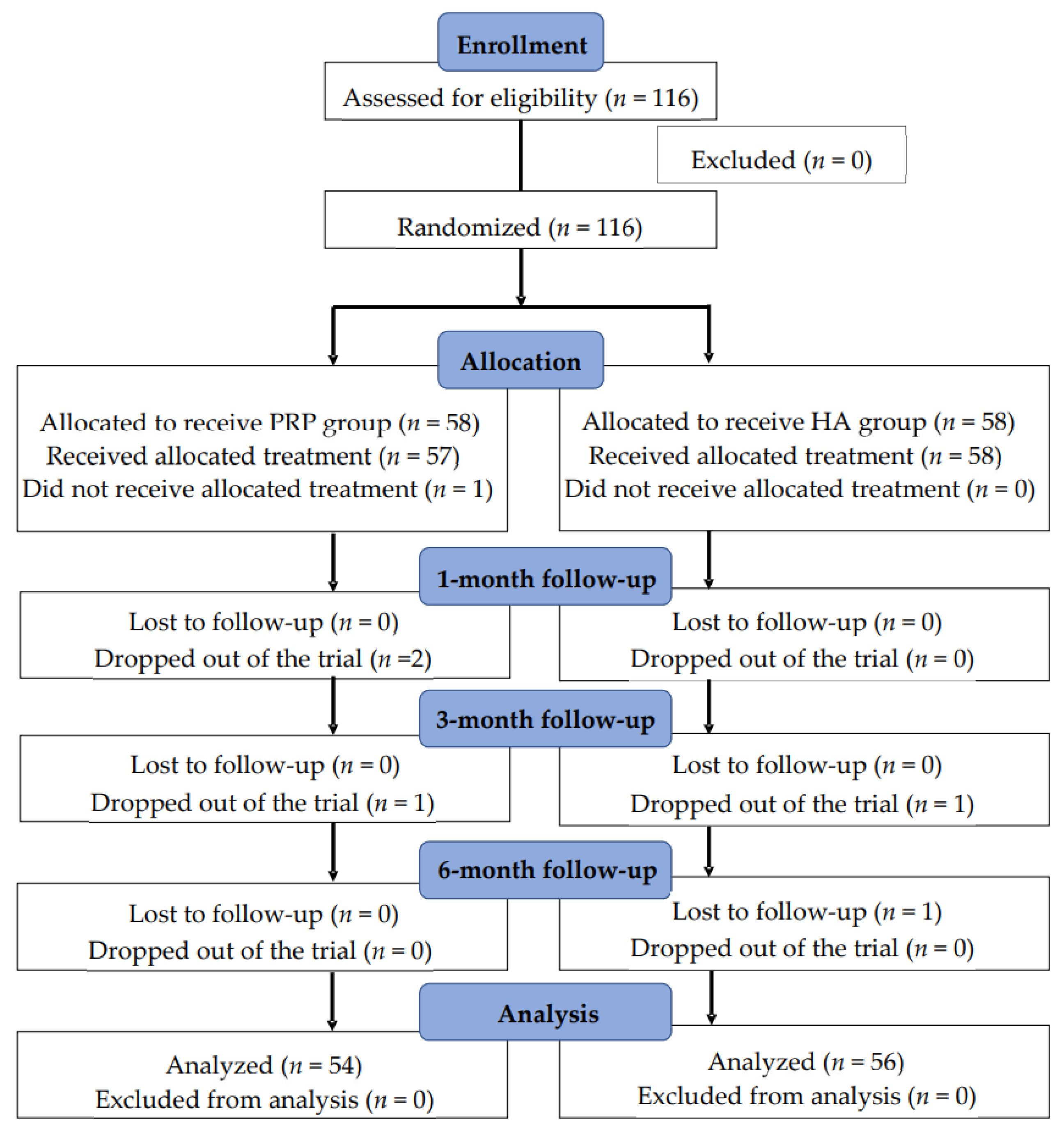
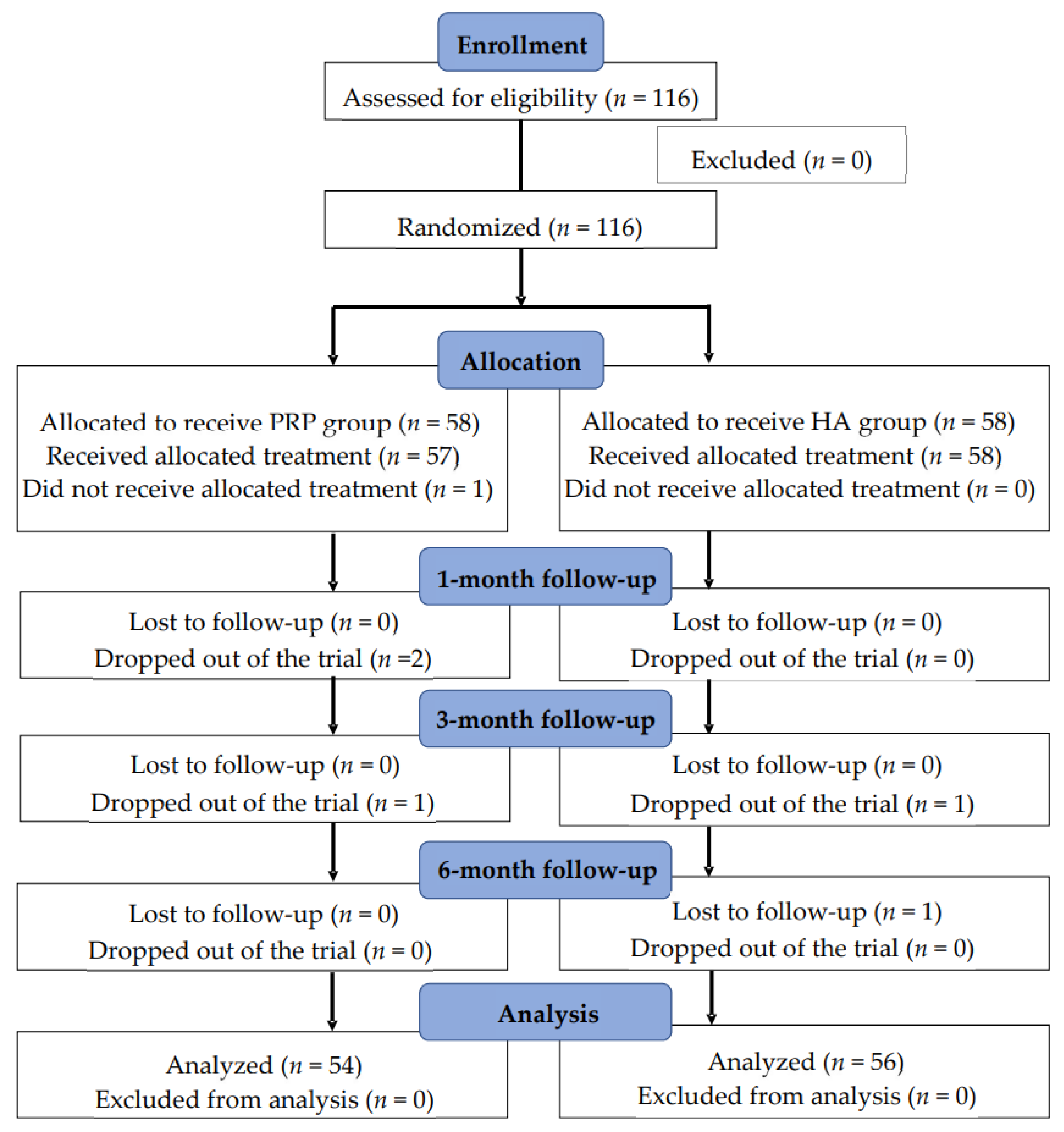
3. Results
3.1. PRP Group
3.2. HA Group
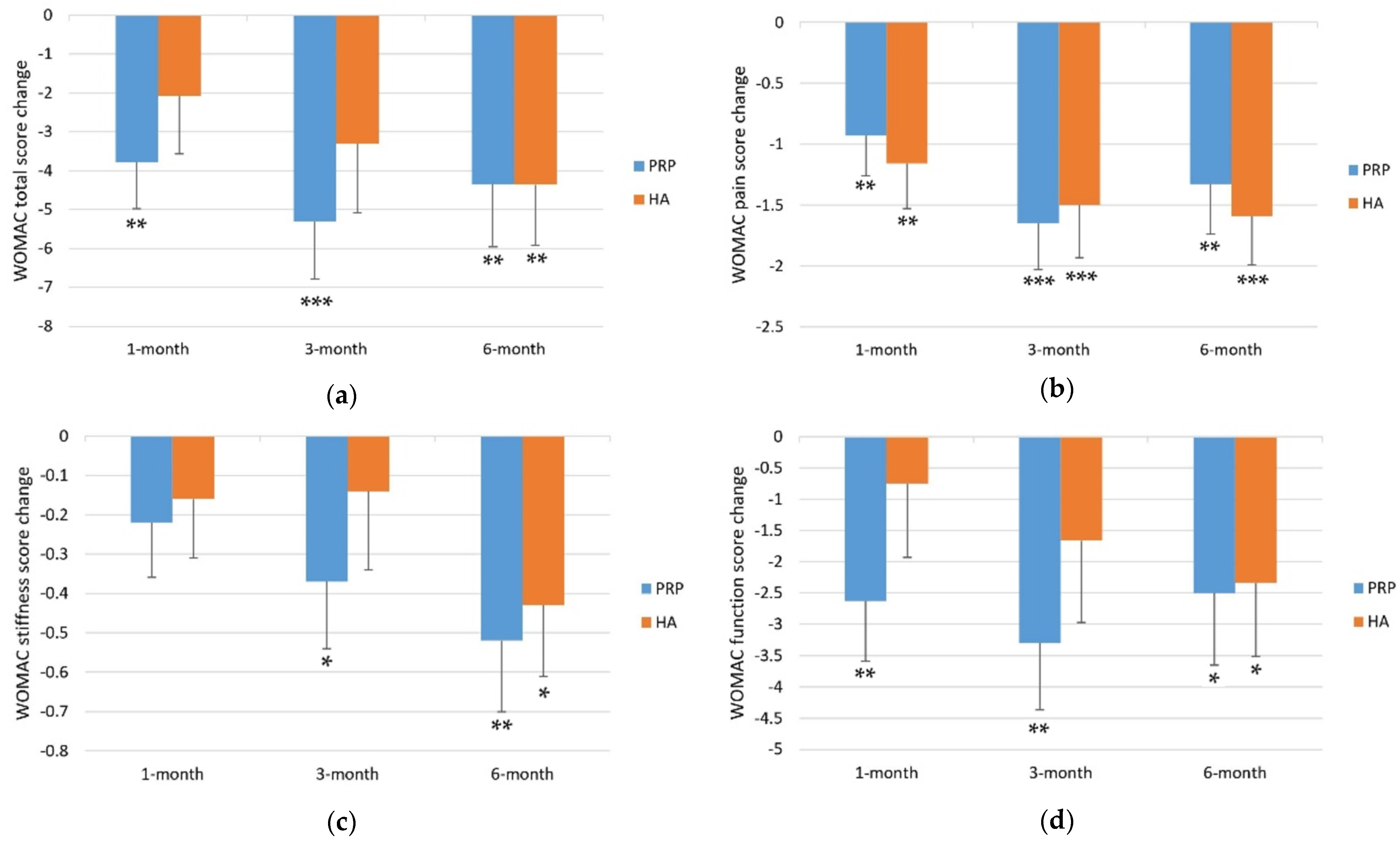
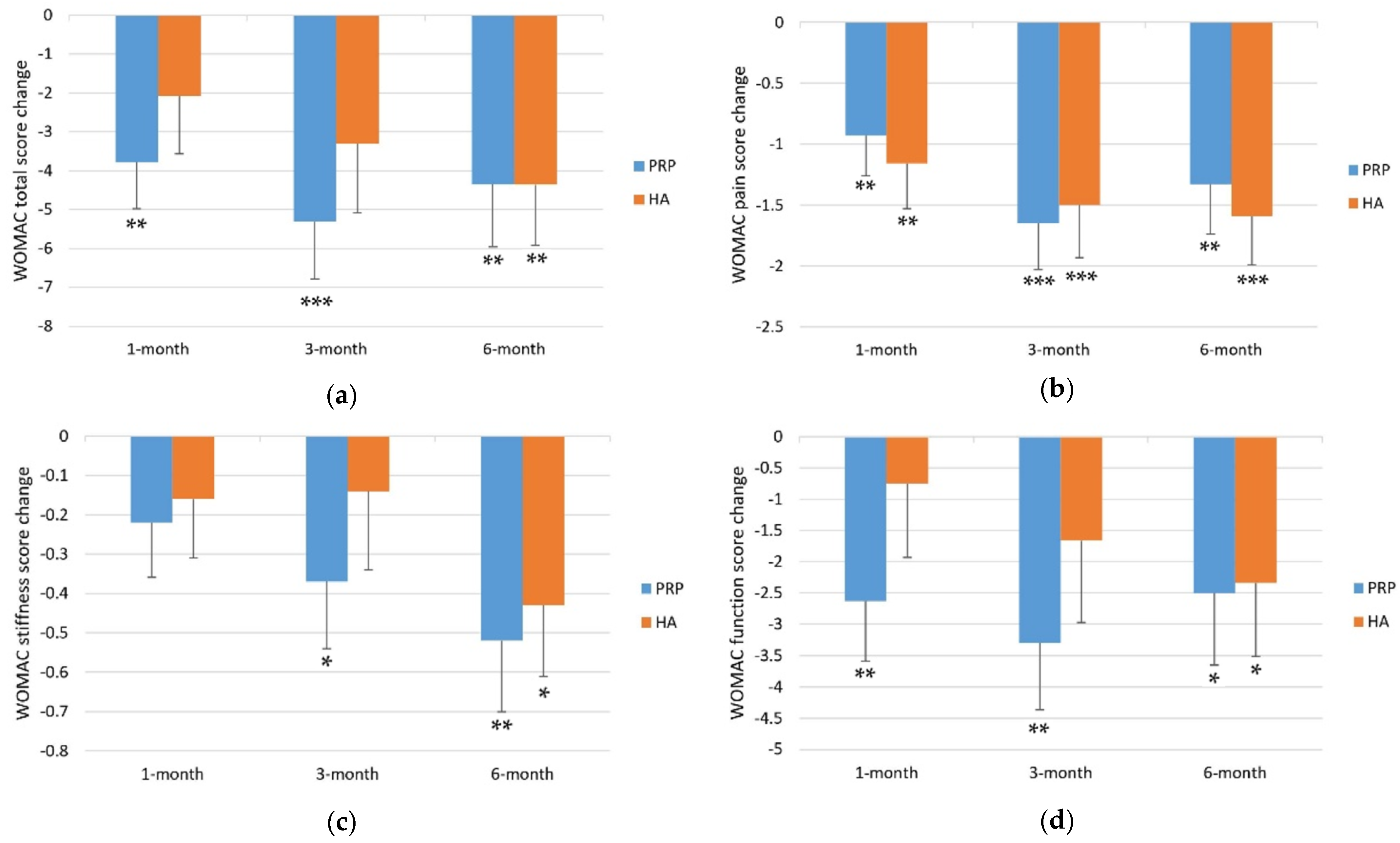
3.3. PRP vs. HA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malemud, C.J. Biologic basis of osteoarthritis: State of the evidence. Curr. Opin. Rheumatol. 2015, 27, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Berenbaum, F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthr. Cartil. 2013, 21, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scanzello, C.R.; Goldring, S.R. The role of synovitis in osteoarthritis pathogenesis. Bone 2012, 51, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felson, D.T.; Lawrence, R.C.; Dieppe, P.A.; Hirsch, R.; Helmick, C.G.; Jordan, J.M.; Kington, R.S.; Lane, N.E.; Nevitt, M.C.; Zhang, Y.; et al. Osteoarthritis: New insights. Part 1: The disease and its risk factors. Ann. Intern. Med. 2000, 133, 635–646. [Google Scholar] [CrossRef]
- Jüni, P.; Hari, R.; Rutjes, A.W.; Fischer, R.; Silletta, M.G.; Reichenbach, S.; da Costa, B.R. Intra-articular corticosteroid for knee osteoarthritis. Cochrane Database Syst. Rev. 2015, Cd005328. [Google Scholar] [CrossRef] [Green Version]
- Blagojevic, M.; Jinks, C.; Jeffery, A.; Jordan, K.P. Risk factors for onset of osteoarthritis of the knee in older adults: A systematic review and meta-analysis. Osteoarthr. Cartil. 2010, 18, 24–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Aziem, A.A.; Soliman, E.S.; Mosaad, D.M.; Draz, A.H. Effect of a physiotherapy rehabilitation program on knee osteoarthritis in patients with different pain intensities. J. Phys. Ther. Sci. 2018, 30, 307–312. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.R.; Deshpande, B.R.; Collins, J.E.; Katz, J.N.; Losina, E. Comparative pain reduction of oral non-steroidal anti-inflammatory drugs and opioids for knee osteoarthritis: Systematic analytic review. Osteoarthr. Cartil. 2016, 24, 962–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Southworth, T.M.; Naveen, N.B.; Tauro, T.M.; Leong, N.L.; Cole, B.J. The Use of Platelet-Rich Plasma in Symptomatic Knee Osteoarthritis. J. Knee Surg. 2019, 32, 37–45. [Google Scholar] [CrossRef]
- Zeng, C.; Lane, N.E.; Hunter, D.J.; Wei, J.; Choi, H.K.; McAlindon, T.E.; Li, H.; Lu, N.; Lei, G.; Zhang, Y. Intra-articular corticosteroids and the risk of knee osteoarthritis progression: Results from the Osteoarthritis Initiative. Osteoarthr. Cartil. 2019, 27, 855–862. [Google Scholar] [CrossRef]
- Mishra, A.; Harmon, K.; Woodall, J.; Vieira, A. Sports medicine applications of platelet rich plasma. Curr. Pharm. Biotechnol. 2012, 13, 1185–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, N.T.; Schultz, G.S. Growth factors and wound healing: Biochemical properties of growth factors and their receptors. Am. J. Surg. 1993, 165, 728–737. [Google Scholar] [CrossRef]
- Cugat, R.; Cuscó, X.; Seijas, R.; Álvarez, P.; Steinbacher, G.; Ares, O.; Wang-Saegusa, A.; García-Balletbó, M. Biologic enhancement of cartilage repair: The role of platelet-rich plasma and other commercially available growth factors. Arthroscopy 2015, 31, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.; Hackel, J.; Niazi, F.; Shaw, P.; Nicholls, M. Efficacy and safety of repeated courses of hyaluronic acid injections for knee osteoarthritis: A systematic review. Semin. Arthritis Rheum. 2018, 48, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Rayegani, S.M.; Raeissadat, S.A.; Taheri, M.S.; Babaee, M.; Bahrami, M.H.; Eliaspour, D.; Ghorbani, E. Does intra articular platelet rich plasma injection improve function, pain and quality of life in patients with osteoarthritis of the knee? A randomized clinical trial. Orthop. Rev. 2014, 6, 5405. [Google Scholar] [CrossRef] [Green Version]
- Vaquerizo, V.; Plasencia, M.; Arribas, I.; Seijas, R.; Padilla, S.; Orive, G.; Anitua, E. Comparison of intra-articular injections of plasma rich in growth factors (PRGF-Endoret) versus Durolane hyaluronic acid in the treatment of patients with symptomatic osteoarthritis: A randomized controlled trial. Arthroscopy 2013, 29, 1635–1643. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Di Martino, A.; Di Matteo, B.; Merli, M.L.; Cenacchi, A.; Fornasari, P.M.; Marcacci, M. Platelet-rich plasma vs hyaluronic acid to treat knee degenerative pathology: Study design and preliminary results of a randomized controlled trial. BMC Musculoskelet. Disord. 2012, 13, 229. [Google Scholar] [CrossRef] [Green Version]
- Di Martino, A.; Di Matteo, B.; Papio, T.; Tentoni, F.; Selleri, F.; Cenacchi, A.; Kon, E.; Filardo, G. Platelet-Rich Plasma Versus Hyaluronic Acid Injections for the Treatment of Knee Osteoarthritis: Results at 5 Years of a Double-Blind, Randomized Controlled Trial. Am. J. Sports Med. 2019, 47, 347–354. [Google Scholar] [CrossRef]
- Sánchez, M.; Anitua, E.; Azofra, J.; Aguirre, J.J.; Andia, I. Intra-articular injection of an autologous preparation rich in growth factors for the treatment of knee OA: A retrospective cohort study. Clin. Exp. Rheumatol. 2008, 26, 910–913. [Google Scholar]
- Sánchez, M.; Jorquera, C.; Sánchez, P.; Beitia, M.; García-Cano, B.; Guadilla, J.; Delgado, D. Platelet-rich plasma injections delay the need for knee arthroplasty: A retrospective study and survival analysis. Int. Orthop. 2021, 45, 401–410. [Google Scholar] [CrossRef]
- Anitua, E.; Sánchez, M.; Aguirre, J.J.; Prado, R.; Padilla, S.; Orive, G. Efficacy and safety of plasma rich in growth factors intra-articular infiltrations in the treatment of knee osteoarthritis. Arthroscopy 2014, 30, 1006–1017. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Huang, H.; Pan, J.; Lin, J.; Zeng, L.; Liang, G.; Yang, W.; Liu, J. Meta-analysis Comparing Platelet-Rich Plasma vs Hyaluronic Acid Injection in Patients with Knee Osteoarthritis. Pain Med. 2019, 20, 1418–1429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Wang, C.; You, D.; Zhao, S.; Zhu, Z.; Xu, M. Platelet-rich plasma versus hyaluronic acid in the treatment of knee osteoarthritis: A meta-analysis. Medicine 2020, 99, e19388. [Google Scholar] [CrossRef] [PubMed]
- Belk, J.W.; Kraeutler, M.J.; Houck, D.A.; Goodrich, J.A.; Dragoo, J.L.; McCarty, E.C. Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Am. J. Sports Med. 2021, 49, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Chen, H.; Zhao, L.; Huang, W. Platelet-Rich Plasma Versus Hyaluronic Acid in the Treatment of Knee Osteoarthritis: A Meta-analysis of 26 Randomized Controlled Trials. Arthroscopy 2021, 37, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, M.; Fiz, N.; Azofra, J.; Usabiaga, J.; Aduriz Recalde, E.; Garcia Gutierrez, A.; Albillos, J.; Gárate, R.; Aguirre, J.J.; Padilla, S.; et al. A randomized clinical trial evaluating plasma rich in growth factors (PRGF-Endoret) versus hyaluronic acid in the short-term treatment of symptomatic knee osteoarthritis. Arthroscopy 2012, 28, 1070–1078. [Google Scholar] [CrossRef]
- Sun, S.F.; Hsu, C.W.; Lin, H.S.; Liou, I.H.; Chen, Y.H.; Hung, C.L. Comparison of Single Intra-Articular Injection of Novel Hyaluronan (HYA-JOINT Plus) with Synvisc-One for Knee Osteoarthritis: A Randomized, Controlled, Double-Blind Trial of Efficacy and Safety. J. Bone Jt. Surg. Am. 2017, 99, 462–471. [Google Scholar] [CrossRef]
- Tuan, S.; Liou, I.; Su, H.; Tsai, Y.; Chen, G.; Sun, S. Improvement of self-reported functional scores and thickening of quadriceps and femoral intercondylar cartilage under ultrasonography after single intra-articular injection of a novel cross-linked hyaluronic acid in the treatment of knee osteoarthritis. J. Back Musculoskelet. Rehabil. 2018, 31, 709–718. [Google Scholar] [CrossRef]
- Sun, S.F.; Lin, G.C.; Hsu, C.W.; Lin, H.S.; Liou, I.S.; Wu, S.Y. Comparing efficacy of intraarticular single crosslinked Hyaluronan (HYAJOINT Plus) and platelet-rich plasma (PRP) versus PRP alone for treating knee osteoarthritis. Sci. Rep. 2021, 11, 140. [Google Scholar] [CrossRef]
- Thumboo, J.; Chew, L.H.; Soh, C.H. Validation of the Western Ontario and Mcmaster University osteoarthritis index in Asians with osteoarthritis in Singapore. Osteoarthr. Cartil. 2001, 9, 440–446. [Google Scholar] [CrossRef] [Green Version]
- Nicholls, M.; Shaw, P.; Niazi, F.; Bhandari, M.; Bedi, A. The Impact of Excluding Patients with End-Stage Knee Disease in Intra-Articular Hyaluronic Acid Trials: A Systematic Review and Meta-Analysis. Adv. Ther. 2019, 36, 147–161. [Google Scholar] [CrossRef] [Green Version]
- Hawker, G.A. The Challenge of Pain for Patients with OA. HSS J 2012, 8, 42–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ettinger, W.H., Jr.; Burns, R.; Messier, S.P.; Applegate, W.; Rejeski, W.J.; Morgan, T.; Shumaker, S.; Berry, M.J.; O’Toole, M.; Monu, J.; et al. A randomized trial comparing aerobic exercise and resistance exercise with a health education program in older adults with knee osteoarthritis. The Fitness Arthritis and Seniors Trial (FAST). JAMA 1997, 277, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Angst, F.; Aeschlimann, A.; Stucki, G. Smallest detectable and minimal clinically important differences of rehabilitation intervention with their implications for required sample sizes using WOMAC and SF-36 quality of life measurement instruments in patients with osteoarthritis of the lower extremities. Arthritis Rheumatol. 2001, 45, 384–391. [Google Scholar] [CrossRef]
- Filardo, G.; Di Matteo, B.; Di Martino, A.; Merli, M.L.; Cenacchi, A.; Fornasari, P.; Marcacci, M.; Kon, E. Platelet-Rich Plasma Intra-articular Knee Injections Show No Superiority Versus Viscosupplementation: A Randomized Controlled Trial. Am. J. Sports Med. 2015, 43, 1575–1582. [Google Scholar] [CrossRef]
- Paterson, K.L.; Nicholls, M.; Bennell, K.L.; Bates, D. Intra-articular injection of photo-activated platelet-rich plasma in patients with knee osteoarthritis: A double-blind, randomized controlled pilot study. BMC Musculoskelet. Disord. 2016, 17, 67. [Google Scholar] [CrossRef] [Green Version]
- Riboh, J.C.; Saltzman, B.M.; Yanke, A.B.; Fortier, L.; Cole, B.J. Effect of Leukocyte Concentration on the Efficacy of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis. Am. J. Sports Med. 2016, 44, 792–800. [Google Scholar] [CrossRef]
- Vilchez-Cavazos, F.; Millán-Alanís, J.M.; Blázquez-Saldaña, J.; Álvarez-Villalobos, N.; Peña-Martínez, V.M.; Acosta-Olivo, C.A.; Simental-Mendía, M. Comparison of the Clinical Effectiveness of Single Versus Multiple Injections of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2019, 7, 2325967119887116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spaková, T.; Rosocha, J.; Lacko, M.; Harvanová, D.; Gharaibeh, A. Treatment of knee joint osteoarthritis with autologous platelet-rich plasma in comparison with hyaluronic acid. Am. J. Phys. Med. Rehabil. 2012, 91, 411–417. [Google Scholar] [CrossRef]
- Patel, S.; Dhillon, M.S.; Aggarwal, S.; Marwaha, N.; Jain, A. Treatment with platelet-rich plasma is more effective than placebo for knee osteoarthritis: A prospective, double-blind, randomized trial. Am. J. Sports Med. 2013, 41, 356–364. [Google Scholar] [CrossRef]
- Martini, L.I.; Via, A.G.; Fossati, C.; Randelli, F.; Randelli, P.; Cucchi, D. Single Platelet-Rich Plasma Injection for Early Stage of Osteoarthritis of the Knee. Joints 2017, 5, 2–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buendía-López, D.; Medina-Quirós, M.; Fernández-Villacañas Marín, M. Clinical and radiographic comparison of a single LP-PRP injection, a single hyaluronic acid injection and daily NSAID administration with a 52-week follow-up: A randomized controlled trial. J. Orthop. Traumatol. 2018, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Colen, S.; van den Bekerom, M.P.; Mulier, M.; Haverkamp, D. Hyaluronic acid in the treatment of knee osteoarthritis: A systematic review and meta-analysis with emphasis on the efficacy of different products. BioDrugs 2012, 26, 257–268. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| PRP Group (n = 54) | HA Group (n = 56) | p-Value | |
|---|---|---|---|
| Age (year) | 61.87 ± 5.46 | 63.00 ± 5.33 | 0.274 a |
| Gender | 0.445 b | ||
| Male, n (%) | 12 (22.2%) | 16 (28.6%) | |
| Female, n (%) | 42 (77.8%) | 40 (71.4%) | |
| BMI | 24.07 ± 3.35 | 24.02 ± 2.39 | 0.937 a |
| K–L grade | 0.055 b | ||
| I | 29 (53.7%) | 40 (71.4%) | |
| II | 25 (46.3%) | 16 (28.6%) | |
| Treatment Side | 0.686 b | ||
| Right | 23 | 26 | |
| Left | 31 | 30 | |
| WOMAC score | |||
| Pain | 4.20 ± 0.42 | 4.38 ± 0.43 | 0.776 a |
| Stiffness | 1.89 ± 0.19 | 1.73 ± 0.21 | 0.575 a |
| Function | 12.65 ± 1.38 | 12.13 ± 1.27 | 0.780 a |
| Total | 18.74 ± 1.85 | 18.23 ± 1.80 | 0.844 a |
| PRP Group (n = 54) | HA Group (n = 56) | p-Value | |
|---|---|---|---|
| WOMAC at 1-month follow-up | |||
| Pain | 3.28 ± 0.37 | 3.21 ± 0.39 | 0.907 a |
| Stiffness | 1.67 ± 0.19 | 1.57 ± 0.19 | 0.722 a |
| Function | 10.02 ± 1.15 | 11.38 ± 1.54 | 0.483 a |
| Total | 14.96 ± 1.60 | 16.16 ± 2.04 | 0.646 a |
| WOMAC at 3-month follow-up | |||
| Pain | 2.56 ± 0.32 | 2.88 ± 0.41 | 0.545 a |
| Stiffness | 1.52 ± 0.16 | 1.59 ± 0.21 | 0.791 a |
| Function | 9.35 ± 1.03 | 10.46 ± 1.59 | 0.562 a |
| Total | 13.43 ± 1.42 | 14.93 ± 2.17 | 0.567 a |
| WOMAC at 6-month follow-up | |||
| Pain | 2.87 ± 0.35 | 2.79 ± 0.38 | 0.872 a |
| Stiffness | 1.37 ± 0.17 | 1.30 ± 0.16 | 0.774 a |
| Function | 10.15 ± 1.12 | 9.79 ± 1.44 | 0.843 a |
| Total | 14.39 ± 1.56 | 13.88 ± 1.91 | 0.836 a |
| PRP Group (n = 54) | p-Value a (Pre vs. Post) | HA Group (n = 56) | p-Value b (Pre vs. Post) | p-Value c | |
|---|---|---|---|---|---|
| WOMAC at 1-month follow-up | |||||
| Pain | −0.93 ± 0.33 | 0.005 ** | −1.16 ± 0.37 | 0.002 ** | 0.634 |
| Stiffness | −0.22 ± 0.14 | 0.107 | −0.16 ± 0.15 | 0.281 | 0.762 |
| Function | −2.63 ± 0.96 | 0.006 ** | −0.75 ± 1.18 | 0.523 | 0.214 |
| Total | −3.78 ± 1.20 | 0.001 ** | −2.07 ± 1.50 | 0.163 | 0.369 |
| WOMAC at 3-month follow-up | |||||
| Pain | −1.65 ± 0.38 | <0.001 *** | −1.50 ± 0.43 | <0.001 *** | 0.793 |
| Stiffness | −0.37 ± 0.17 | 0.026 * | −0.14 ± 0.20 | 0.467 | 0.376 |
| Function | −3.30 ± 1.07 | 0.002 ** | −1.66 ± 1.31 | 0.200 | 0.329 |
| Total | −5.31 ± 1.48 | <0.001 *** | −3.30 ± 1.78 | 0.061 | 0.380 |
| WOMAC at 6-month follow-up | |||||
| Pain | −1.33 ± 0.41 | 0.001 ** | −1.59 ± 0.40 | <0.001 *** | 0.651 |
| Stiffness | −0.52 ± 0.18 | 0.004 ** | −0.43 ± 0.18 | 0.013 * | 0.719 |
| Function | −2.50 ± 1.15 | 0.029 * | −2.34 ± 1.17 | 0.044 * | 0.921 |
| Total | −4.35 ± 1.61 | 0.006 ** | −4.36 ± 1.56 | 0.005 ** | 0.998 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-C.; Lee, C.-L.; Chen, Y.-J.; Tien, Y.-C.; Lin, S.-Y.; Chen, C.-H.; Chou, P.P.-H.; Huang, H.-T. Comparing the Efficacy of Intra-Articular Single Platelet-Rich Plasma(PRP) versus Novel Crosslinked Hyaluronic Acid for Early-Stage Knee Osteoarthritis: A Prospective, Double-Blind, Randomized Controlled Trial. Medicina 2022, 58, 1028. https://doi.org/10.3390/medicina58081028
Wang Y-C, Lee C-L, Chen Y-J, Tien Y-C, Lin S-Y, Chen C-H, Chou PP-H, Huang H-T. Comparing the Efficacy of Intra-Articular Single Platelet-Rich Plasma(PRP) versus Novel Crosslinked Hyaluronic Acid for Early-Stage Knee Osteoarthritis: A Prospective, Double-Blind, Randomized Controlled Trial. Medicina. 2022; 58(8):1028. https://doi.org/10.3390/medicina58081028
Chicago/Turabian StyleWang, Ying-Chun, Chia-Ling Lee, Yu-Jen Chen, Yin-Chun Tien, Sung-Yen Lin, Chung-Hwan Chen, Paul Pei-Hsi Chou, and Hsuan-Ti Huang. 2022. "Comparing the Efficacy of Intra-Articular Single Platelet-Rich Plasma(PRP) versus Novel Crosslinked Hyaluronic Acid for Early-Stage Knee Osteoarthritis: A Prospective, Double-Blind, Randomized Controlled Trial" Medicina 58, no. 8: 1028. https://doi.org/10.3390/medicina58081028
APA StyleWang, Y.-C., Lee, C.-L., Chen, Y.-J., Tien, Y.-C., Lin, S.-Y., Chen, C.-H., Chou, P. P.-H., & Huang, H.-T. (2022). Comparing the Efficacy of Intra-Articular Single Platelet-Rich Plasma(PRP) versus Novel Crosslinked Hyaluronic Acid for Early-Stage Knee Osteoarthritis: A Prospective, Double-Blind, Randomized Controlled Trial. Medicina, 58(8), 1028. https://doi.org/10.3390/medicina58081028