
Reclassification of Treatment Strategy with Fractional Flow Reserve in Cancer Patients with Coronary Artery Disease

 ,
,  , ,
, ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Study Population
2.2. FFR-Guided Treatment and Follow-Up
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iliescu, C.A.; Grines, C.L.; Herrmann, J.; Yang, E.H.; Cilingiroglu, M.; Charitakis, K.; Hakeem, A.; Toutouzas, K.P.; Leesar, M.A.; Marmagkiolis, K. SCAI Expert consensus statement: Evaluation, management, and special considerations of cardio-oncology patients in the cardiac catheterization laboratory (endorsed by the cardiological society of india, and sociedad Latino Americana de Cardiologia intervencionista). Catheter. Cardiovasc. Interv. 2016, 87, E202–E223. [Google Scholar] [PubMed]
- Hamilos, M.; Muller, O.; Cuisset, T.; Ntalianis, A.; Chlouverakis, G.; Sarno, G.; Nelis, O.; Bartunek, J.; Vanderheyden, M.; Wyffels, E.; et al. Long-term clinical outcome after fractional flow reserve-guided treatment in patients with angiographically equivocal left main coronary artery stenosis. Circulation 2009, 120, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.P.; Toth, G.G.; Lai, D.; Zhu, H.; Acar, G.; Agostoni, P.; Appelman, Y.; Arslan, F.; Barbato, E.; Chen, S.L.; et al. Prognostic value of fractional flow reserve: Linking physiologic severity to clinical outcomes. J. Am. Coll. Cardiol. 2014, 64, 1641–1654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, F.M.; Ferrara, A.; Johnson, N.P.; van Nunen, L.X.; Escaned, J.; Albertsson, P.; Erbel, R.; Legrand, V.; Gwon, H.C.; Remkes, W.S.; et al. Deferral vs. performance of percutaneous coronary intervention of functionally non-significant coronary stenosis: 15-year follow-up of the DEFER trial. Eur. Heart J. 2015, 36, 3182–3188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toth, G.G.; Johnson, N.P.; Jeremias, A.; Pellicano, M.; Vranckx, P.; Fearon, W.F.; Barbato, E.; Kern, M.J.; Pijls, N.H.; De Bruyne, B. Standardization of Fractional Flow Reserve Measurements. J. Am. Coll. Cardiol. 2016, 68, 742–753. [Google Scholar] [CrossRef]
- Pijls, N.H.; De Bruyne, B.; Peels, K.; Van Der Voort, P.H.; Bonnier, H.J.; Bartunek, J.K.J.J.; Koolen, J.J. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N. Engl. J. Med. 1996, 334, 1703–1708. [Google Scholar] [CrossRef]
- van Nunen, L.X.; Zimmermann, F.M.; Tonino, P.A.; Barbato, E.; Baumbach, A.; Engstrom, T.; Klauss, V.; MacCarthy, P.A.; Manoharan, G.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet 2015, 386, 1853–1860. [Google Scholar] [CrossRef]
- Falanga, A.; Schieppati, F.; Russo, D. Cancer tissue procoagulant mechanisms and the hypercoagulable state of patients with cancer. Semin. Thromb. Hemost. 2015, 41, 756–764. [Google Scholar] [PubMed]
- Layland, J.; Oldroyd, K.G.; Curzen, N.; Sood, A.; Balachandran, K.; Das, R.; Junejo, S.; Ahmed, N.; Lee, M.M.; Shaukat, A.; et al. Fractional flow reserve vs. angiography in guiding management to optimize outcomes in non-ST-segment elevation myocardial infarction: The British Heart Foundation FAMOUS-NSTEMI randomized trial. Eur. Heart J. 2015, 36, 100–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bruyne, B.; Fearon, W.F.; Pijls, N.H.; Barbato, E.; Tonino, P.; Piroth, Z.; Jagic, N.; Mobius-Winckler, S.; Rioufol, G.; Witt, N.; et al. Fractional flow reserve-guided PCI for stable coronary artery disease. N. Engl. J. Med. 2014, 371, 1208–1217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbato, E.; Toth, G.G.; Johnson, N.P.; Pijls, N.H.; Fearon, W.F.; Tonino, P.A.; Curzen, N.; Piroth, Z.; Rioufol, G.; Juni, P.; et al. A prospective natural history study of coronary atherosclerosis using fractional flow reserve. J. Am. Coll. Cardiol. 2016, 68, 2247–2255. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.M.; Park, D.W.; Shin, E.S.; Koo, B.K.; Nam, C.W.; Doh, J.H.; Kim, J.H.; Chae, I.H.; Yoon, J.H.; Her, S.H.; et al. Fractional flow reserve and cardiac events in coronary artery disease: Data from a prospective IRIS-FFR registry (Interventional Cardiology Research Incooperation Society Fractional Flow Reserve). Circulation 2017, 135, 2241–2251. [Google Scholar] [CrossRef] [PubMed]
- Lugo, L.M.; Ferreiro, J.L. Dual antiplatelet therapy after coronary stent implantation: Individualizing the optimal duration. J. Cardiol. 2018, 72, 94–104. [Google Scholar] [CrossRef] [Green Version]
- De Bruyne, B.; Pijls, N.H.; Kalesan, B.; Barbato, E.; Tonino, P.A.; Piroth, Z.; Jagic, N.; Mobius-Winkler, S.; Rioufol, G.; Witt, N.; et al. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N. Engl. J. Med. 2012, 367, 991–1001. [Google Scholar] [CrossRef] [Green Version]
- Nijhoff, F.; Agostoni, P.; Belkacemi, A.; Nathoe, H.M.; Voskuil, M.; Samim, M.; Doevendans, P.A.; Stella, P.R. Primary percutaneous coronary intervention by drug-eluting balloon angioplasty: The nonrandomized fourth arm of the DEB-AMI (drug-eluting balloon in ST-segment elevation myocardial infarction) trial. Catheter. Cardiovasc. Interv. 2015, 86, S34–S44. [Google Scholar] [CrossRef] [PubMed]
- Iliescu, C.; Balanescu, D.V.; Donisan, T.; Giza, D.E.; Munoz Gonzalez, E.D.; Cilingiroglu, M.; Song, J.; Mukerji, S.S.; Lopez-Mattei, J.C.; Kim, P.Y.; et al. Safety of Diagnostic and Therapeutic Cardiac Catheterization in Cancer Patients with Acute Coronary Syndrome and Chronic Thrombocytopenia. Am. J. Cardiol. 2018, 122, 1465–1470. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | Mean ± SD or Count (%) |
|---|---|
| Age (years) | 64.8 ± 9.92 |
| Female | 16 (28.1%) |
| Male | 41 (71.9%) |
| Cardiovascular risk factors | |
| Hypertension | 41 (71.9%) |
| Hyperlipidemia | 34 (59.6%) |
| Smoking | 25 (43.9%) |
| Family history of coronary artery disease | 12 (21.1%) |
| Malignancy type | |
| Solid | 43 (75.4%) |
| Hematologic | 14 (24.6%) |
| Hemoglobin (g/dL) | 11.8 ± 2 |
| Platelet number (K/µL) | 193.5 ± 78.28 |
| Creatinine (mg/dL) | 1.13 ± 0.94 |
| Coronary lesions | |
| Left anterior descending artery | 39 (68.4%) |
| Left circumflex artery | 3 (5.3%) |
| Left main coronary artery | 4 (7%) |
| Right coronary artery | 10 (17.5%) |
| Ramus | 1 (1.8%) |
| Stenosis severity (%) | 65.88 ± 9.92 |
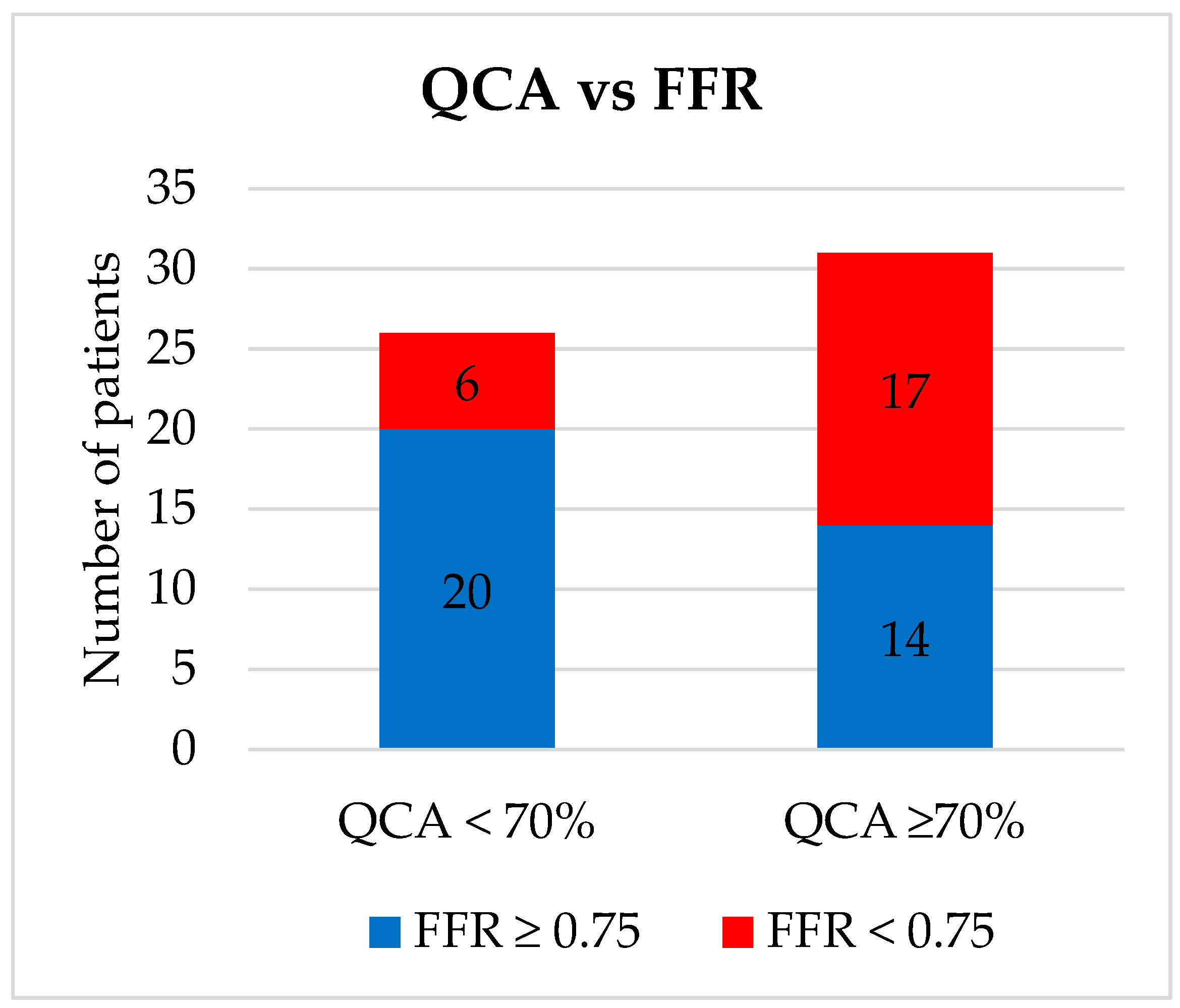
| <70% | 25 (43.9%) |
| ≥70% | 32 (56.1%) |
| Fractional flow reserve | 0.77 ± 0.12 |
| Percutaneous coronary intervention with stenting | |
| No | 34 (59.6%) |
| Yes | 23 (40.4%) |
| Bare-metal stent | 10 (43.5%) |
| Drug-eluting stent | 13 (56.5%) |
| Death within 12 months | 13 (22.8%) |
| Cardiovascular mortality | 1 (1.8%) |
| Survival at 12 Months | Overall Survival | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Alive (N = 44) | Dead (N = 13) | HR (95% CI) | p | Alive (N = 35) | Dead (N = 22) | HR (95% CI) | p | ||
| Age (years) | 64.52 ± 10.71 | 65.76 ± 6.84 | 1.00 | 62.84 ± 10.83 | 67.92 ± 7.47 | 1.03 (0.99–1.08) | 0.11 | ||
| Gender | Female | 10 (22.7%) | 6 (46.2%) | 1.00 | 9 (25.7%) | 7 (31.8%) | 1.00 | ||
| Male | 34 (77.3%) | 7 (53.8%) | 0.38 (0.13–1.13) | 0.08 | 26 (74.3%) | 15 (68.2%) | 0.77 (0.31–1.89) | 0.57 | |
| Hypertension | Yes | 32 (72.7%) | 9 (69.2%) | 0.83 (0.26–2.70) | 0.76 | 24 (68.6%) | 17 (77.3%) | 1.19 (0.44–3.23) | 0.73 |
| Hyperlipidemia | Yes | 27 (61.4%) | 7 (53.8%) | 0.76 (0.25–2.25) | 0.62 | 22 (62.9%) | 12 (54.5%) | 0.78 (0.34-1.80) | 0.56 |
| Smoking | Yes | 20 (45.5%) | 5 (38.5%) | 0.76 (0.25–2.32) | 0.63 | 15 (42.9%) | 10 (45.5%) | 1.16 (0.50–2.69) | 0.73 |
| Family history of coronary artery disease | Yes | 10 (22.7%) | 2 (15.4%) | 0.69 (1.53–3.12) | 0.63 | 9 (25.7%) | 3 (13.6%) | 0.63 (1.88–2.14) | 0.46 |
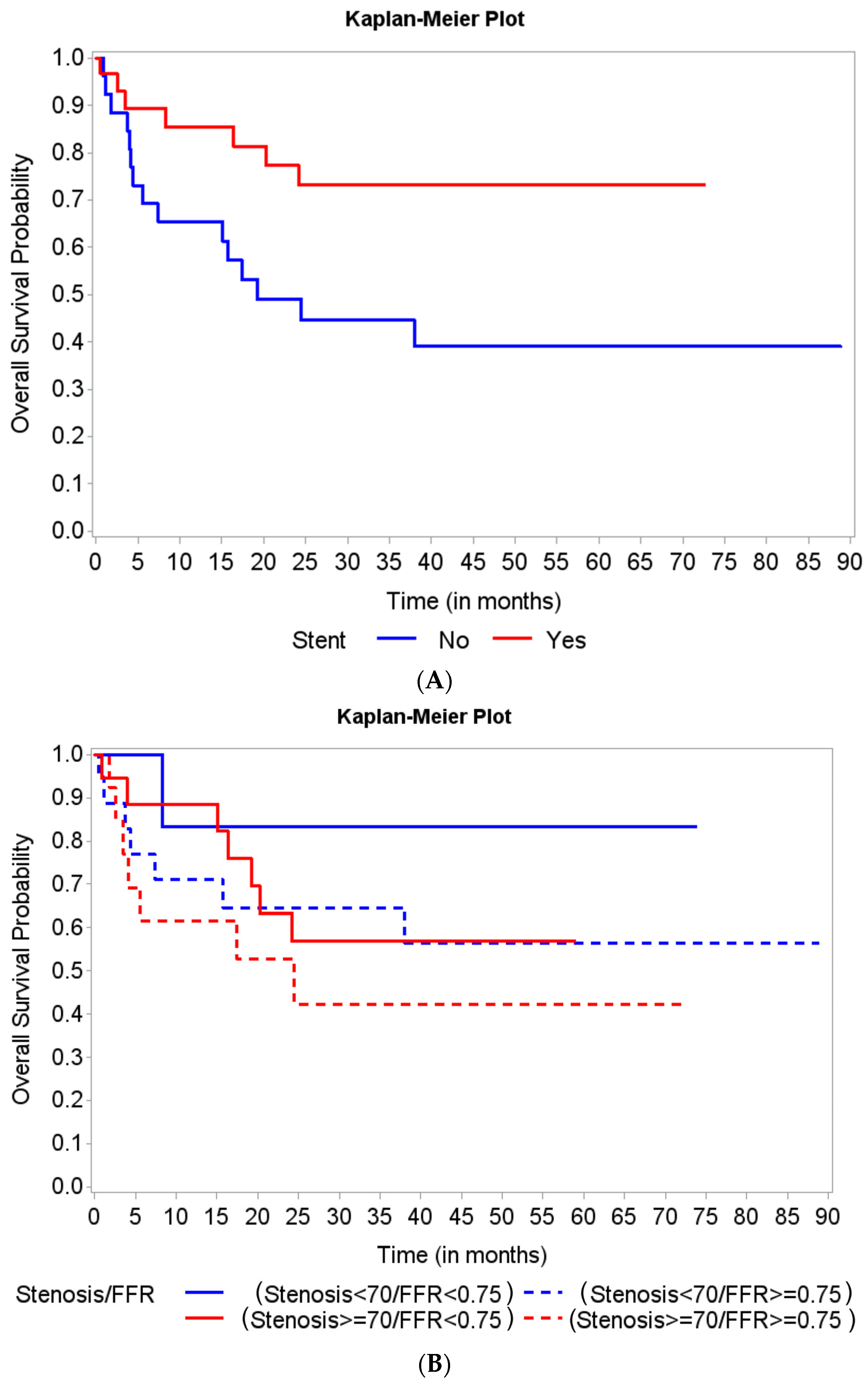
| Stent | Yes | 27 (61.4%) | 4 (30.8%) | 0.34 (0.10–1.09) | 0.07 | 24 (68.6%) | 7 (31.8%) | 0.37 (0.15–0.90) | 0.03 |
| Stenosis severity group | <70% | 19 (43.2%) | 6 (46.2%) | 1.00 | 17 (48.6%) | 8 (36.4%) | 1.00 | ||
| ≥70% | 25 (56.8%) | 7 (53.8%) | 0.93 (0.31–2.75) | 0.89 | 18 (51.4%) | 14 (63.6%) | 1.50 (0.62–3.59) | 0.37 | |
| Fractional flow reserve | 0.77 ± 0.12 | 0.77 ± 0.12 | 1.00 | 0.78 ± 0.12 | 0.76 ± 0.13 | 0.32 (0.01–10.00) | 0.51 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.W.; Dayah, T.J.; Javaid, A.; Monlezun, D.J.; Balanescu, D.V.; Donisan, T.; Karimzad, K.; Hakeem, A.; Boone, D.L.; Palaskas, N.; et al. Reclassification of Treatment Strategy with Fractional Flow Reserve in Cancer Patients with Coronary Artery Disease. Medicina 2022, 58, 884. https://doi.org/10.3390/medicina58070884
Kim JW, Dayah TJ, Javaid A, Monlezun DJ, Balanescu DV, Donisan T, Karimzad K, Hakeem A, Boone DL, Palaskas N, et al. Reclassification of Treatment Strategy with Fractional Flow Reserve in Cancer Patients with Coronary Artery Disease. Medicina. 2022; 58(7):884. https://doi.org/10.3390/medicina58070884
Chicago/Turabian StyleKim, Jin Wan, Tariq J. Dayah, Awad Javaid, Dominique J. Monlezun, Dinu V. Balanescu, Teodora Donisan, Kaveh Karimzad, Abdul Hakeem, David L. Boone, Nicolas Palaskas, and et al. 2022. "Reclassification of Treatment Strategy with Fractional Flow Reserve in Cancer Patients with Coronary Artery Disease" Medicina 58, no. 7: 884. https://doi.org/10.3390/medicina58070884
APA StyleKim, J. W., Dayah, T. J., Javaid, A., Monlezun, D. J., Balanescu, D. V., Donisan, T., Karimzad, K., Hakeem, A., Boone, D. L., Palaskas, N., Lopez-Mattei, J., Kim, P. Y., Durand, J.-B., Song, J., Balanescu, S. M., Yang, E. H., Herrmann, J., Marmagkiolis, K., Toutouzas, K., ... Iliescu, C. A. (2022). Reclassification of Treatment Strategy with Fractional Flow Reserve in Cancer Patients with Coronary Artery Disease. Medicina, 58(7), 884. https://doi.org/10.3390/medicina58070884