
Current and Future Approaches in Management of Chronic Spontaneous Urticaria Using Anti-IgE Antibodies



 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
3. Results
- Anti-IgE therapy;
- Management of chronic spontaneous urticaria with omalizumab and ligelizumab in clinical practice;
- Potential biomarkers for the effectiveness of chronic urticaria treatment.
3.1. Anti-IgE Therapy
3.2. Management of Chronic Spontaneous Urticaria with Omalizumab and Ligelizumab in Clinical Practice
3.3. Potential Biomarkers for the Effectiveness of Chronic Urticaria Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
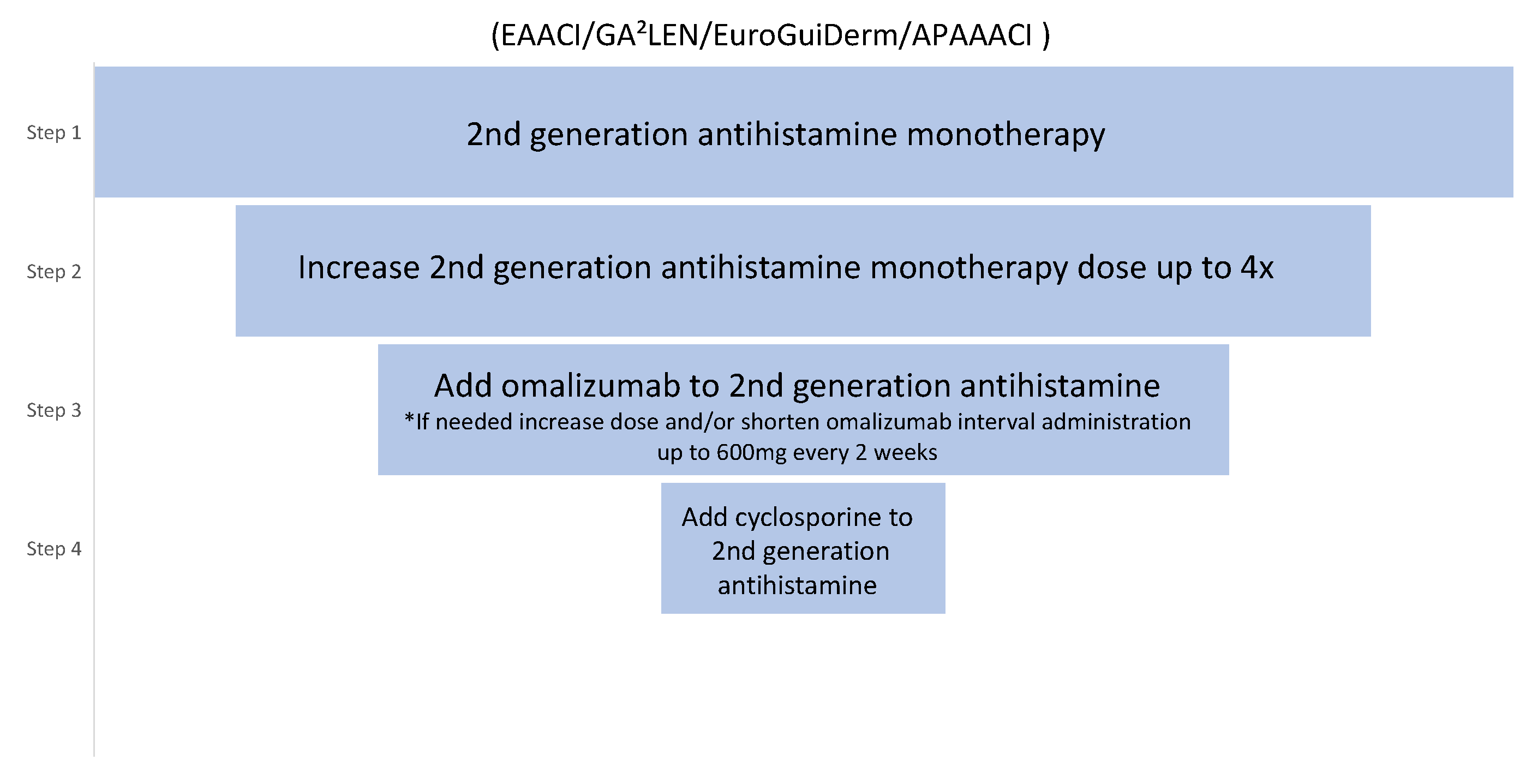
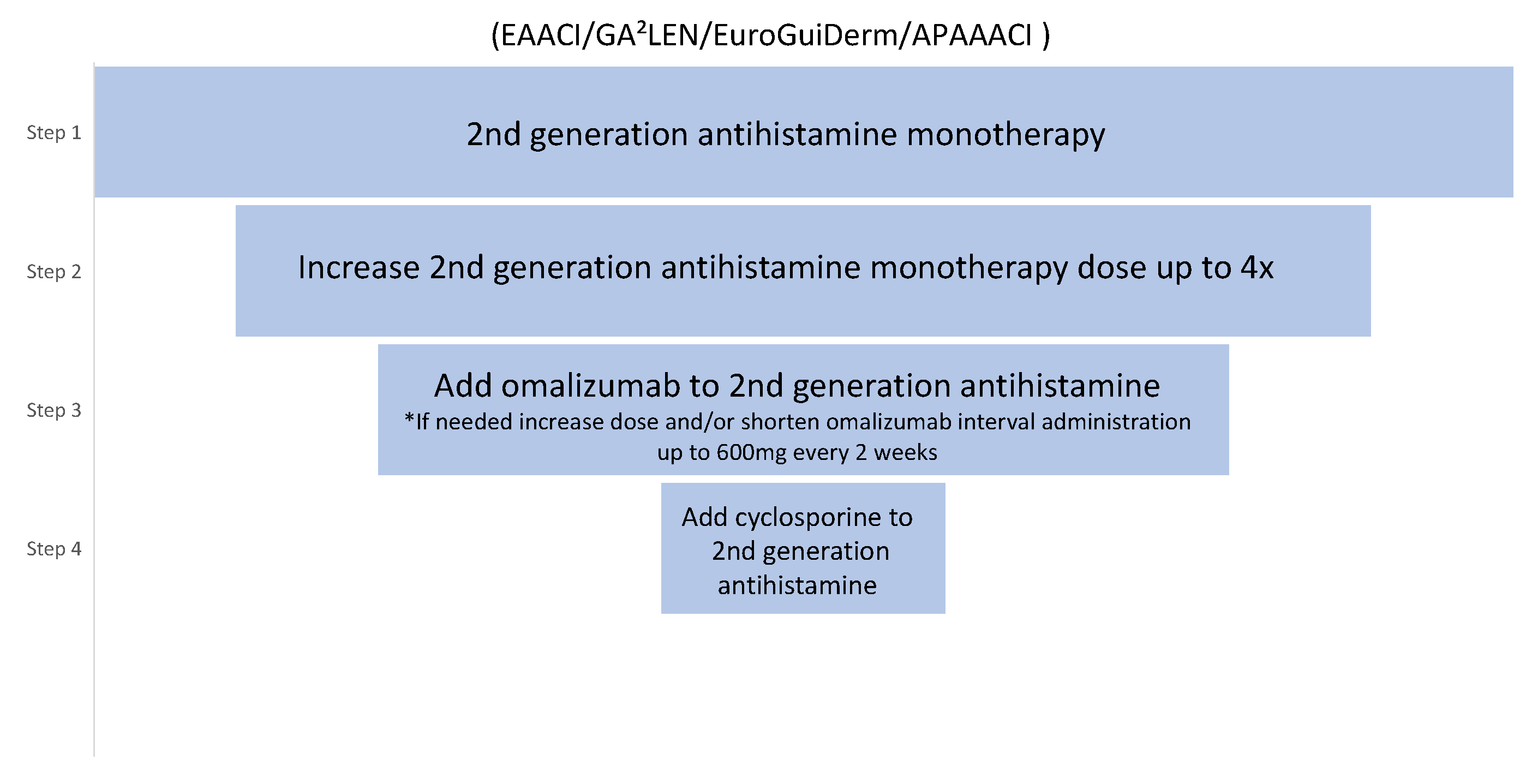
- Zuberbier, T.; Abdul Latiff, A.H.; Abuzakouk, M.; Aquilina, S.; Asero, R.; Baker, D.; Ballmer-Weber, B.; Bangert, C.; Ben-Shoshan, M.; Bernstein, J.A.; et al. The international EAACI/GA2LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy 2022, 77, 734–766. [Google Scholar] [CrossRef] [PubMed]
- Wedi, B. Urticaria and angioedema. In Braun-Falco’s Dermatology; Plewig, G., French, L., Ruzicka, T., Kaufmann, R., Hertl, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2020; Volume 4, pp. 1–26. [Google Scholar]
- Moon, T.C.; Befus, A.D.; Kulka, M. Mast Cell Mediators: Their Differential Release and the Secretory Pathways Involved. Front. Immunol. 2014, 5, 569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pałgan, K.; Bartuzi, Z. Platelet activating factor in allergies. Int. J. Immunopathol. Pharmacol. 2015, 28, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, G.; Schwartz, L.B. Mast cell heterogeneity: Structure and mediators. In Asthma and Rhinitis; Busse, W.W., Holgate, S.T., Eds.; Blackwell Science: Boston, MS, USA, 1995; p. 195. [Google Scholar]
- Grieco, T.; Porzia, A.; Paolino, G.; Chello, C.; Sernicola, A.; Faina, V.; Mainiero, F. IFN-c/IL-6 and related cytokines in chronic spontaneous urticaria: Evaluation of their pathogenetic role and changes during omalizumab therapy. J. Int. Dermatol. 2020, 59, 590–594. [Google Scholar] [CrossRef]
- Babaie, D.; Nabavi, M.; Arshi, S.; Gorjipour, H.; Darougar, S. The Relationship Between Serum Interleukin-6 Level and Chronic Urticaria. Immunoregulation 2019, 2, 41–46. [Google Scholar] [CrossRef]
- Gould, H.J.; Sutton, B.J. IgE in allergy and asthma today. Nat. Rev. Immunol. 2008, 8, 205–217. [Google Scholar] [CrossRef]
- Bracken Sonali, J.; Soman, A.; MacLeod, A.S. Autoimmune Theories of Chronic Spontaneous Urticaria. Front. Immunol. 2019, 10, 627. [Google Scholar] [CrossRef]
- Confino-Cohen, R.; Chodick, G.; Shalev, V.; Leshno, M.; Kimhi, O.; Goldberg, A. Chronic urticaria and autoimmunity: Associations found in a large population study. J. Allergy Clin. Immunol. 2012, 129, 1307–1313. [Google Scholar] [CrossRef]
- Giménez-Arnau, A.M.; Toubi, E.; Marsland, A.M.; Maurer, M. Clinical management of urticaria using omalizumab: The first licensed biological therapy available for chronic spontaneous urticaria. J. Eur. Acad. Derm. Venereol. 2016, 30, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Gomez, G. Current Strategies to Inhibit High Affinity FcεRI-Mediated Signaling for the Treatment of Allergic Disease. Front. Immunol. 2019, 10, 175. [Google Scholar] [CrossRef] [Green Version]
- Savic, S.; Marsland, A.; McKay, D.; Ardern-Jones, M.R.; Leslie, T.; Somenzi, O.; Grattan, C. Retrospective case note review of chronic spontaneous urticaria outcomes and adverse effects in patients treated with omalizumab or ciclosporin in UK secondary care. All Asth. Clin. Immun. 2015, 11, 21. [Google Scholar] [CrossRef] [Green Version]
- Maurer, M.; Rosén, K.; Hsieh, H.-J.; Saini, S.; Grattan, C.; Gimenéz-Arnau, A.; Agarwal, S.; Doyle, R.; Canvin, J.; Kaplan, A.; et al. Omalizumab for the Treatment of Chronic Idiopathic or Spontaneous Urticaria. N. Engl. J. Med. 2013, 368, 924–935. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, A.; Ledford, D.; Ashby, M.; Canvin, J.; Zazzali, J.L.; Conner, E.; Zazzali, J.L.; Conner, E.; Veith, J.; Kamath, N.; et al. Omalizumab in patients with symptomatic chronic idiopathic/spontaneous urticaria despite standard combination therapy. J. Allergy Clin. Immunol. 2013, 132, 101–109. [Google Scholar] [CrossRef]
- Zhao, Z.-T.; Ji, C.-M.; Yu, W.-J.; Meng, L.; Hawro, T.; Wei, J.F.; Maurer, M. Omalizumab for the treatment of chronic spontaneous urticaria: A meta-analysis of randomized clinical trials. J. Allergy Clin. Immunol. 2016, 137, 1742–1750.e1744. [Google Scholar] [CrossRef] [Green Version]
- Staubach, P.; Metz, M.; Chapman-Rothe, N.; Sieder, C.; Bräutigam, M.; Canvin, J.; Maurer, M. Effect of omalizumab on angioedema in H1-antihistamine-resistant chronic spontaneous urticaria patients: Results from X-ACT.; A randomized controlled trial. Allergy 2016, 71, 1135–1144. [Google Scholar] [CrossRef]
- Tharp, M.D.; Bernstein, J.A.; Kavati, A.; Ortiz, B.; MacDonald, K.; Denhaerynck, K.; Lee, C.S. Benefits and Harms of Omalizumab Treatment in Adolescent and Adult Patients with Chronic Idiopathic (Spontaneous) Urticaria: A Meta-analysis of “Real-world” Evidence. JAMA Derm. 2019, 155, 29–38. [Google Scholar] [CrossRef]
- Urgert, M.C.; van den Elzen, M.T.; Knulst, A.C.; Fedorowicz, Z.; van Zuuren, E.J. Omalizumab in patients with chronic spontaneous urticaria: A systematic review and GRADE assessment. Br. J. Derm. 2015, 173, 404–415. [Google Scholar] [CrossRef]
- Dressler, C.; Werner, R.N.; Eisert, L.; Zuberbier, T. Nast A and Maurer M: Chronic inducible urticaria: A systematic review of treatment options. J. Allergy Clin. Immunol. 2018, 141, 1726–1734. [Google Scholar] [CrossRef] [Green Version]
- Maurer, M.; Metz, M.; Brehler, R.; Hillen, U.; Jakob, T.; Mahler, V.; Pföhler, C.; Staubach, P.; Treudler, R.; Wedi, B.; et al. Omalizumab treatment in patients with chronic inducible urticaria: A systematic review of published evidence. J. Allergy Clin. Immunol. 2018, 141, 638–649. [Google Scholar] [CrossRef] [Green Version]
- Maurer, M.; Weller, K.; Bindslev-Jensen, C.; Giménez-Arnau, A.; Bousquet, P.J.; Bousquet, J.; Zuberbier, T. Unmet clinical needs in chronic spontaneous urticaria. A GA2LEN task force report1. Allergy 2011, 66, 317–330. [Google Scholar] [CrossRef]
- Ferrer, M.; Giménez-Arnau, A.; Saldana, D.; Janssens, N.; Balp, M.M.; Khalil, S.; Risson, V. Predicting Chronic Spontaneous Urticaria Symptom Return After Omalizumab Treatment Discontinuation: Exploratory Analysis. J. Allergy Clin. Immunol. Pract. 2018, 6, 1191–1197.e1195. [Google Scholar] [CrossRef]
- Türk, M.; Maurer, M.; Yılmaz, İ. How to discontinue omalizumab in chronic spontaneous urticaria? Allergy 2019, 74, 821–824. [Google Scholar] [CrossRef]
- Schoepke, N.; Asero, R.; Ellrich, A.; Ferrer, M.; Gimenez-Arnau, A.; Grattan, C.E.H.; Maurer, M. Biomarkers and clinical characteristics of autoimmune chronic spontaneous urticaria: Results of the PURIST Study. Allergy 2019, 74, 2427–2436. [Google Scholar] [CrossRef]
- Maurer, M.; Altrichter, S.; Schmetzer, O.; Scheffel, J.; Church, M.K.; Metz, M. Immunoglobulin E-Mediated Autoimmunity. Front. Immunol. 2018, 9, 689. [Google Scholar] [CrossRef] [Green Version]
- Gauvreau, G.M.; Arm, J.P.; Boulet, L.-P.; Leigh, R.; Cockcroft, D.W.; Davis, B.E.; O’Byrne, P.M. Efficacy and safety of multiple doses of QGE031 (ligelizumab) versus omalizumab and placebo in inhibiting allergen-induced early asthmatic responses. J. Allergy Clin. Immunol. 2016, 138, 1051–1059. [Google Scholar] [CrossRef] [Green Version]
- Metz, M.; Maurer, M. Use of biologics in chronic spontaneous urticaria-beyond omalizumab therapy? Allergol. Sel. 2021, 5, 89–95. [Google Scholar] [CrossRef]
- Maurer, M.; Giménez-Arnau, A.M.; Sussman, G.; Metz, M.; Baker, D.R.; Bauer, A.; Janocha, R. Ligelizumab for Chronic Spontaneous Urticaria. N. Engl. J. Med. 2019, 381, 1321–1332. [Google Scholar] [CrossRef] [Green Version]
- NCT03907878; A Safety and Efficacy Study of Ligelizumab in the Treatment of CSU in Japanese Patients Inadequately Controlled with H1-Antihistamines. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2019. Available online: https://ClinicalTrials.gov/show/NCT03907878 (accessed on 20 April 2022).
- NCT04210843; Study of Efficacy and Safety of Ligelizumab in Chronic Spontaneous Urticaria Patients Who Completed a Previous Study with Ligelizumab. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2019. Available online: https://ClinicalTrials.gov/show/NCT04210843 (accessed on 20 April 2022).
- NCT04513548; Study of Mechanism of Action of Ligelizumab (QGE031) in Patients with Chronic Urticaria. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2020. Available online: https://ClinicalTrials.gov/show/NCT04513548 (accessed on 20 April 2022).
- NCT03437278; Study to Investigate the Efficacy and Safety of QGE031 in Adolescent Patients with Chronic Spontaneous Urticaria (CSU). ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2018. Available online: https://ClinicalTrials.gov/show/NCT03437278 (accessed on 20 April 2022).
- NCT03580369; A Phase III Study of Efficacy and Safety of Ligelizumab in the Treatment of CSU in Adolescents and Adults Inadequately Controlled with H1-antihistamines. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2018. Available online: https://ClinicalTrials.gov/show/NCT03580356 (accessed on 20 April 2022).
- NCT03632291; Evaluate the Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of UB-221 as an Add-on Therapy in CSU Patients. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2018. Available online: https://ClinicalTrials.gov/show/NCT0363229 (accessed on 20 April 2022).
- NCT04175704; Evaluating the Safety and Tolerability and Determining the PK and PD of Single Dose UB-221 in Chronic Spontaneous Urticaria. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2019. Available online: https://ClinicalTrials.gov/show/NCT04175704 (accessed on 20 April 2022).
- Metz, M.; Ohanyan, T.; Church, M.; Maurer, M. Omalizumab is an effective and rapidly acting therapy in difficult-to-treat chronic urticaria: A retrospective clinical analysis. J. Derm. Sci. 2014, 73, 57–62. [Google Scholar] [CrossRef]
- Metz, M.; Ohanyan, T.; Church, M.K.; Maurer, M. Retreatment with Omalizumab Results in Rapid Remission in Chronic Spontaneous and Inducible Urticaria. JAMA Derm. 2014, 150, 288–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labrador-Horrillo, M.; Valero, A.; Velasco, M.; Jáuregui, I.; Sastre, J.; Bartra, J.; Silvestre, K.F.; Ortiz de Frutos, J.; Gimenez-Arnau, A.; Ferrer, M. Efficacy of omalizumab in chronic spontaneous urticaria refractory to conventional therapy: Analysis of 110 patients in real-life practice. Expert Opin. Biol. 2013, 13, 1225–1228. [Google Scholar] [CrossRef] [PubMed]
- Snast, I.; Kremer, N.; Lapidoth, M.; Enk, C.D.; Tal, Y.; Rosman, Y.; Levi, A. Omalizumab for the Treatment of Solar Urticaria: Case Series and Systematic Review of the Literature. J. Allergy Clin. Immunol. Pract. 2018, 6, 1198–1204.e1193. [Google Scholar] [CrossRef]
- Bullerkotte, U.; Wieczorek, D.; Kapp, A.; Wedi, B. Effective treatment of refractory severe heat urticaria with omalizumab. Allergy 2010, 65, 931–932. [Google Scholar] [CrossRef] [PubMed]
- Metz, M.; Schütz, A.; Weller, K.; Gorczyza, M.; Zimmer, S.; Staubach, P.; Maurer, M. Omalizumab is effective in cold urticaria—results of a randomized placebo-controlled trial. J. Allergy Clin. Immunol. 2017, 140, 864–867.e865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gastaminza, G.; Azofra, J.; Nunez-Cordoba, J.M.; Baeza, M.L.; Echechipía, S.; Gaig, P.; García, B.E.; Labrador-Horrillo, M.; Sala-Cunil, A.; Ferrer, M.; et al. Efficacy and Safety of Omalizumab (Xolair) for Cholinergic Urticaria in Patients Unresponsive to a Double Dose of Antihistamines: A Randomized Mixed Double-Blind and Open-Label Placebo-Controlled Clinical Trial. J. Allergy Clin. Immunol. Pract. 2019, 7, 1599–1609.e1591. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.; Schütz, A.; Weller, K.; Schoepke, N.; Peveling-Oberhag, A.; Staubach, P.; Metz, M. Omalizumab is effective in symptomatic dermographism-results of a randomized placebo-controlled trial. J. Allergy Clin. Immunol. 2017, 140, 870–873.e875. [Google Scholar] [CrossRef] [Green Version]
- Yu, C.; Wang, K.; Cui, X.; Lu, L.; Dong, J.; Wang, M.; Gao, X. Clinical Efficacy and Safety of Omalizumab in the Treatment of Allergic Rhinitis: A Systematic Review and Meta-analysis of Randomized Clinical Trials. Am. J. Rhinol. Allergy 2019, 34, 196–208. [Google Scholar] [CrossRef]
- Dantzer, J.A.; Wood, R.A. The use of omalizumab in allergen immunotherapy. Clin. Exp. Allergy 2018, 48, 232–240. [Google Scholar] [CrossRef]
- Wedi, B. Ligelizumab for the treatment of chronic spontaneous urticaria. Expert Opin. Biol. 2020, 20, 853–861. [Google Scholar] [CrossRef]
- Jendoubi, F.; Gaudenzio, N.; Gallini, A.; Negretto, M.; Paul, C.; Bulai Livideanu, C. Omalizumab in the treatment of adult patients with mastocytosis: A systematic review. Clin. Exp. Allergy 2020, 50, 654–661. [Google Scholar] [CrossRef]
- Kremer, N.; Snast, I.; Cohen, E.S.; Hodak, E.; Mimouni, D.; Lapidoth, M.; Levi, A. Rituximab and Omalizumab for the Treatment of Bullous Pemphigoid: A Systematic Review of the Literature. Am. J. Clin. Derm. 2019, 20, 209–216. [Google Scholar] [CrossRef]
- Hasni, S.; Gupta, S.; Davis, M.; Poncio, E.; Temesgen-Oyelakin, Y.; Joyal, E.; Fike, A.; Manna, Z.; Rivera, J.; Auh, S.; et al. Safety and Tolerability of Omalizumab: A Randomized Clinical Trial of Humanized Anti-IgE Monoclonal Antibody in Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019, 71, 1135–1140. [Google Scholar] [CrossRef]
- Iqbal, K.; Bhargava, K.; Skov, P.S.; Falkencrone, S.; Grattan, C.E. A positive serum basophil histamine release assay is a marker for ciclosporin-responsiveness in patients with chronic spontaneous urticaria. Clin. Transl. Allergy 2012, 2, 19. [Google Scholar] [CrossRef] [Green Version]
- Soong, W.; Metz, M.; Bernstein, J.A.; Lanier, B.; Sitz, K.; Maurer, M.; Janocha, R. Long-term treatment with ligelizumab achieves prolonged symptom control in patients with chronic spontaneous urticaria during the post-treatment follow-up. J. Allergy Clin. Immunol. 2020, 145, AB341. [Google Scholar] [CrossRef]
- Maurer, M.; Giménez-Arnau, A.M.; Soong, W.; Bernstein, J.A.; Sussman, G.; Metz, M.; Janocha, R.; Lanier, B.; Hide, M.; Sitz, K.; et al. Treatment with ligelizumab achieves over forty percent higher complete response rate in chronic spontaneous urticaria patients originally treated with omalizumab. Allergy 2020, 75, 86. [Google Scholar]
- Wedi, B.; Traidl, S. Anti-IgE for the Treatment of Chronic Urticaria. Immunotargets Ther. 2021, 10, 27–45. [Google Scholar] [CrossRef]
- Jensen, R.K.; Jabs, F.; Miehe, M.; Mølgaard, B.; Pfützner, W.; Möbs, C.; Andersen, G.R. Structure of intact IgE and the mechanism of ligelizumab revealed by electron microscopy. Allergy 2020, 75, 1956–1965. [Google Scholar] [CrossRef]
- Palacios, T.; Stillman, L.; Borish, L.; Lawrence, M. Lack of basophil CD203c-upregulating activity as an immunological marker to predict response to treatment with omalizumab in patients with symptomatic chronic urticaria. J. Allergy Clin. Immunol. Pract. 2016, 4, 529–530. [Google Scholar] [CrossRef] [Green Version]
- Zipkin, M. Opportunities to target mast cells in inflammatory diseases expand. Biopharmdeal 2021, 15, 25. [Google Scholar] [CrossRef]
- NCT05129423; A Phase II.; Multicenter, Randomized, Double-Blind, Placebo-Controlled Pilot and Dose-Ranging Study of MTPS9579A in Participants with Refractory Chronic Spontaneous Urticaria. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT05129423 (accessed on 20 April 2022).
- Johal, K.J.; Saini, S.S. Current and emerging treatments for chronic spontaneous urticaria. Ann. Allergy Asthma Immunol. 2020, 125, 380–387. [Google Scholar] [CrossRef]
- NCT03137069; A Phase II, Multicenter, Randomized, Double-Blind, Placebo-Controlled Pilot and Dose-Ranging Study of GDC-0853 in Patients with Refractory Chronic Spontaneous Urticaria (CSU). ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT03137069 (accessed on 20 April 2022).
- NCT05048342; A Multicenter, Open-label Phase 3 Study of Remibrutinib (LOU064) to Investigate the Safety, Tolerability and Efficacy for 52 Weeks in Adult Japanese Chronic Spontaneous Urticaria Patients Inadequately Controlled by H1-antihistamines. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT05048342 (accessed on 20 April 2022).
- Alvarado, D.; Maurer, M.; Gedrich, R.; Seibel, S.B.; Murphy, M.B.; Crew, L.; Goldstein, J.; Crocker, A.; Heath-Chiozzi, M.; Vitale, L.A.; et al. Anti-KIT monoclonal antibody CDX-0159 induces profound and durable mast cell suppression in a healthy volunteer study. Eur. J. Allergy Clin. Immunol. 2022, 1–11. [Google Scholar] [CrossRef]
- NCT04538794; A Randomized, Double-Blind, Placebo-Controlled, Phase 1 Multiple Ascending Dose Study to Assess the Safety, Pharmacokinetics, and Pharmacodynamics of CDX-0159 as Add-on Therapy in Patients with Chronic Spontaneous Urticaria. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT04538794 (accessed on 20 April 2022).
- NCT03494881; Mepolizumab for the Treatment of Chronic Spontaneous Urticaria: An Open-Label, Single-Arm, Exploratory Study. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT03494881 (accessed on 20 April 2022).
- NCT03437278; A Multicenter, Randomized, Double-Blind, Placebo-Controlled Phase 2b Dose-Finding Study to Investigate the Efficacy and Safety of Ligelizumab (QGE031) in Adolescent Patients with Chronic Spontaneous Urticaria (CSU). ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT03437278 (accessed on 20 April 2022).
- NCT03749135; A Multicenter, Randomized, Double-Blind, Placebo-Controlled, Proof-of-Concept Phase 2, 16-Week Treatment Study with a 16 Week Follow-up Period to Assess the Efficacy and Safety of Dupilumab (Anti-IL4Ra) in Adult Patients with Chronic Spontaneous Urticaria Despite H1-antihistamine Treatment. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT03749135 (accessed on 20 April 2022).
- NCT04833855; A Randomized, Double-Blind, Placebo-Controlled, Multicenter, Dose-Ranging, Phase 2b Study to Evaluate Efficacy and Safety of Tezepelumab for the Treatment of Chronic Spontaneous Urticaria. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT04833855 (accessed on 20 April 2022).
- NCT05032157; A Multicenter, Randomized, Double-Blind, Placebo-Controlled Phase 3 Study of Remibrutinib (LOU064) to Investigate the Efficacy, Safety and Tolerability for 52 Weeks in Adult Chronic Spontaneous Urticaria (CSU) Patients Inadequately Controlled by H1-antihistamines. ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT05032157 (accessed on 20 April 2022).
- NCT03183024; Treatment of Chronic Urticarial Unresponsive to H1-antihistamines With an Anti-IL5Ralpha Monoclonal Antibody, ClinicalTrials.gov-National Library of Medicine (US). ClinicalTrials.gov-National Library of Medicine (US): Bethesda, MA, USA, 2017. Available online: https://clinicaltrials.gov/ct2/show/NCT03183024 (accessed on 20 April 2022).

{kind=link}
{kind=link}
| Molecule | Mechanism | Type | Stage | Indication |
|---|---|---|---|---|
| CDX-0159 | Anti-tyrosine kinase KIT | mAb | 1 | CSU and chronic inducible urticaria [63] |
| Mepolizumab | Anti-IL-5 | mAb | 1 | CSU [64] |
| Ligelizumab | Anti-IgE | mAb | 2 | CSU in children from 12 to <18 years of age [65] |
| Dupilumab | Anti-IL-4/-13 | mAb | 2 | CSU [66] |
| MTPS9579A | Tetrameric β-tryptase | mAb | 2 | CSU [59] |
| Tezepelumab | Thymic stromal lymphopoietin | mAb | 2 | CSU [67] |
| Remibrutinib | Anti-BTK | Small molecule | 3 | CSU [68] |
| Benralizumab | Anti-IL-5 receptor | mAb | 4 | CSU [69] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orzan, O.A.; Popa, L.G.; Mihai, M.M.; Cojocaru, A.; Giurcăneanu, C.; Dorobanțu, A.M. Current and Future Approaches in Management of Chronic Spontaneous Urticaria Using Anti-IgE Antibodies. Medicina 2022, 58, 816. https://doi.org/10.3390/medicina58060816
Orzan OA, Popa LG, Mihai MM, Cojocaru A, Giurcăneanu C, Dorobanțu AM. Current and Future Approaches in Management of Chronic Spontaneous Urticaria Using Anti-IgE Antibodies. Medicina. 2022; 58(6):816. https://doi.org/10.3390/medicina58060816
Chicago/Turabian StyleOrzan, Olguța Anca, Liliana Gabriela Popa, Mara Mădălina Mihai, Anca Cojocaru, Călin Giurcăneanu, and Alexandra Maria Dorobanțu. 2022. "Current and Future Approaches in Management of Chronic Spontaneous Urticaria Using Anti-IgE Antibodies" Medicina 58, no. 6: 816. https://doi.org/10.3390/medicina58060816
APA StyleOrzan, O. A., Popa, L. G., Mihai, M. M., Cojocaru, A., Giurcăneanu, C., & Dorobanțu, A. M. (2022). Current and Future Approaches in Management of Chronic Spontaneous Urticaria Using Anti-IgE Antibodies. Medicina, 58(6), 816. https://doi.org/10.3390/medicina58060816