
Evolution of Acute Respiratory Distress Syndrome in Emergency and Critical Care: Therapeutic Management before and during the Pandemic Situation

 , , , and
, , , and
Abstract
:1. Introduction
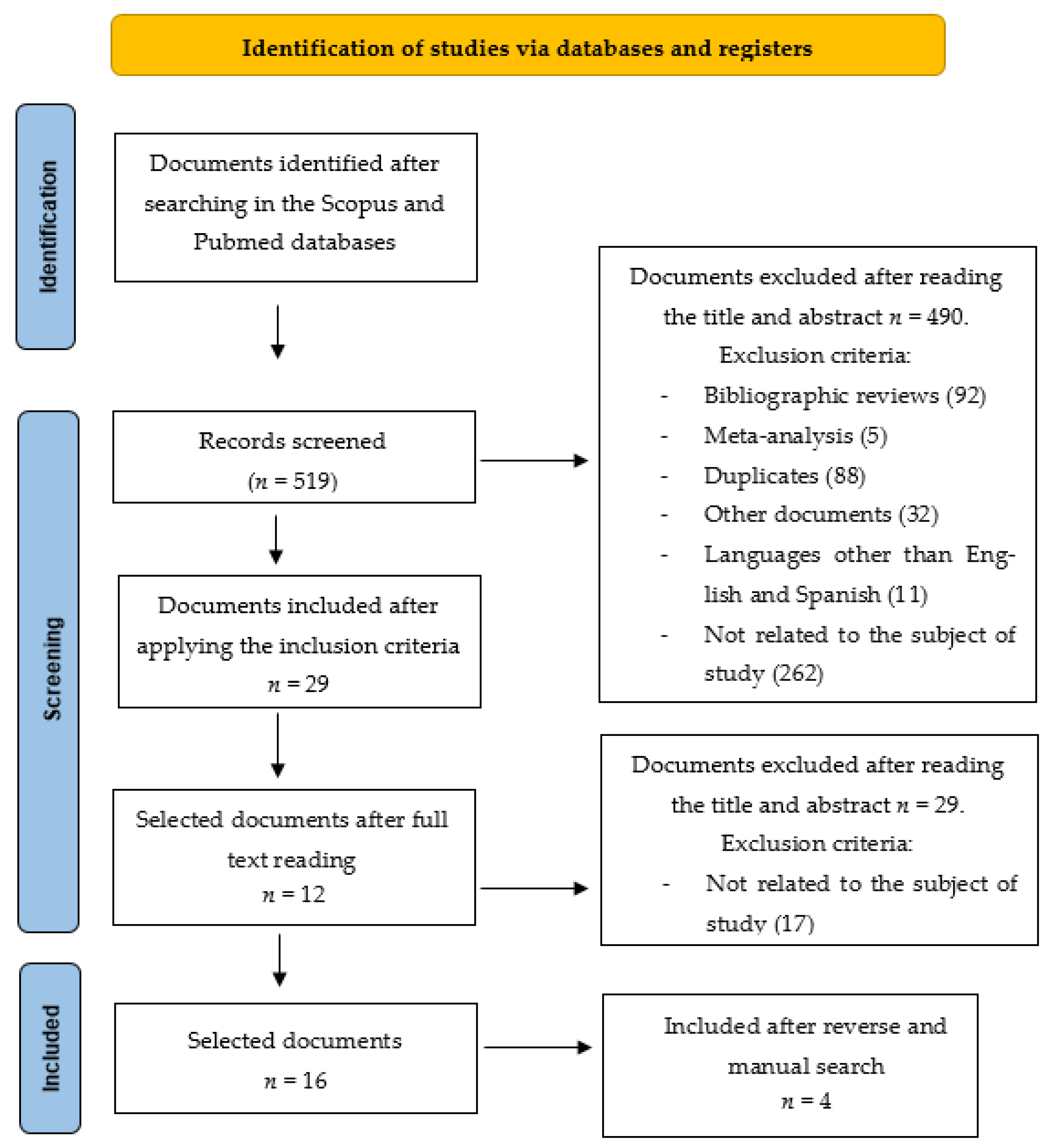
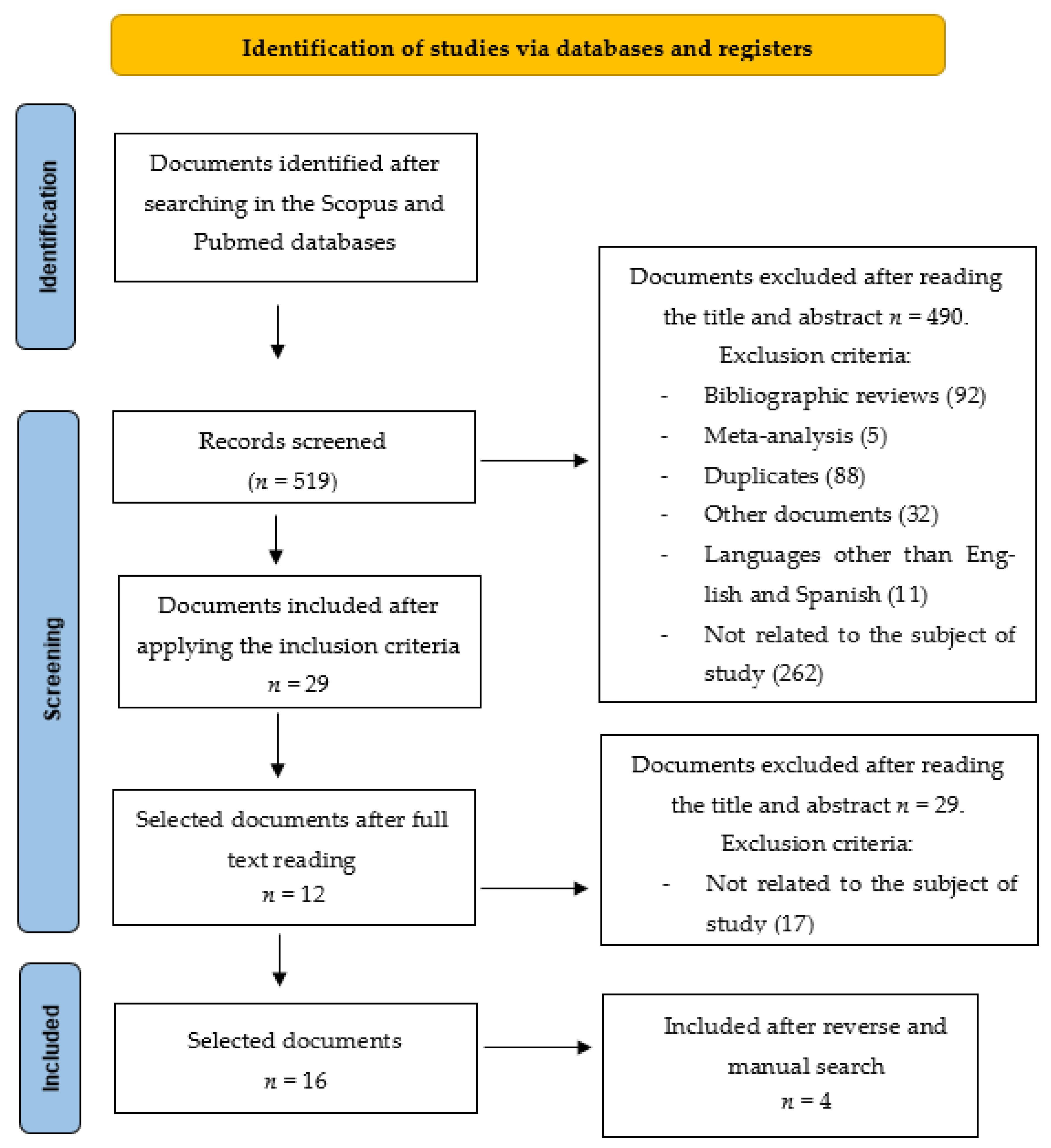
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Level of Evidence
2.4. Variables and Data Collection
3. Results
3.1. Characteristics of the Selected Studies
3.2. Clinical Characteristics of ARDS
3.3. Ventilatory Support in ARDS
3.4. Adjuvant Therapies in ARDS
3.5. Optimization of Resources in Patients with ARDS in Emergency Situations
3.6. Complications of Acute Respiratory Distress Syndrome in Children
4. Discussion
4.1. Future Practical Implications
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Papazian, L.; Aubron, C.; Brochard, L.; Chiche, J.-D.; Combes, A.; Dreyfuss, D.; Forel, J.M.; Guérin, C.; Jaber, S.; Mekontso-Dessap, A.; et al. Formal guidelines: Management of acute respiratory distress syndrome. Ann. Intensive Care 2019, 9, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Oxford University Press. Oxford Learner´s Dictionaries. Available online: https://www.oxfordlearnersdictionaries.com/definition/american_english/emergency (accessed on 24 May 2021).
- Quiroz Carrillo, C.G.; Pareja Cruz, A.; Valencia Ayala, E.; Enriquez Valencia, Y.; Pastora De Leon Delgado, J.; Ramirez, P.A. Un nuevo coronavirus, una nueva enfermedad: COVID-19. Horiz. Med. 2020, 20, e1208. Available online: http://www.scielo.org.pe/scielo.php?script=sci_arttext&pid=S1727-558X2020000200011&lng=es (accessed on 29 June 2021). [CrossRef]
- Soto, G.J.; Kor, D.J.; Park, P.K.; Hou, P.C.; Kaufman, D.A.; Kim, M.; Yadav, H.; Teman, N.; Hsu, M.; Shvikina, T.; et al. Lung Injury Prediction Score in Hospitalized Patiens at Risk of Aute Respiratory Distress Syndrome. Crit. Care Med. 2016, 44, 2182–2191. [Google Scholar] [CrossRef]
- Estenssorio, E.; Dubin, A. Acute respiratory Distress Syndrome. Med. Buenos Aires 2016, 76, 235–241. [Google Scholar]
- Centro nacional de Epidemiologia. Situación de COVID-19 en España a 02 de Junio de 2021. Equipo COVID-19. RENAVE. CNE. CNM (ISCIII). Available online: https://cnecovid.isciii.es/ (accessed on 22 May 2021).
- Torres-González, J.I.; Arias-Rivera, S.; Velasco-Sanz, T.; Mateos, D.A.; Planas, P.B.; Zaragoza-García, I.; Raurell-Torredà, M. ¿Qué ha sucedido con los cuidados durante la pandemia COVID 19? Enferm. Intensiva 2020, 31, 101–104. [Google Scholar] [CrossRef]
- Kurihara, C.; Manerikar, A.; Querrey, M.; Felicelli, C.; Yeldandi, A.; Garza-Castillon, R., Jr.; Lung, K.; Kim, S.; Ho, B.; Tomic, R.; et al. Clinical characteristics and outcomes of patients with COVID-19 associated Acute Respiratory Distress Syndrome who underwent lung transplant. JAMA 2022, 327, 652. [Google Scholar] [CrossRef]
- Lebreton, G.; Schmidt, M.; Ponnaiah, M.; Folliguet, T.; Para, M.; Guihaire, J.; Lansac, E.; Sage, E.; Cholley, B.; Mégarbane, B.; et al. Extracorporeal membrane oxygenation network organisation and clinical outcomes during the COVID-19 pandemic in Greater Paris, France: A multicentre cohort study. Lancet Respir. Med. 2021, 9, 851–862. [Google Scholar] [CrossRef]
- Núñez Herrera, A.; Fernández Urquiza, M.; González Puerto, Y.; Gaimetea Castillo, C.; Rojas Rodríguez, Y.; López Otero, T. Resultados de la capacitación sobre la COVID-Universidad de Ciencias Médicas de Cienfuegos, 2020. Medisur 2020, 18, 7. Available online: http://medisur.sld.cu/index.php/medisur/article/view/4694 (accessed on 15 June 2020).
- Hortal-Carmona, J.; Padilla-Bernáldez, J.; Melguizo-Jiménez, M.; Ausín, T.; Cruz-Piqueras, M.; Puyol, À.; López de la Vieja, M.T.; Rodríguez-Arias, D.; Tamayo-Velázquez, M.I.; Triviño, R. Efficiency is not enough. Ethical Analysis and recommendations for the allocation of scarce resources in a Pandemic Situation. Gac. Sanit. 2021, 2, 1–9. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalg, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H. The Oxford Levels of Evidence. 2011. Available online: https://www.cebm.net/2016/05/ocebmlevels-of-evidence (accessed on 24 May 2021).
- Bohman, J.K.; Hyder, J.A.; Iyer, V.; Pannu, S.R.; Franco, P.M.; Seelhammer, T.G.; Schenck, L.A.; Schears, G.J. Early prediction of extracorporeal membrana oxygenation eligibility for severe acute respiratory distress syndrome in adults. J. Crit. Care 2016, 33, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Chiu, L.-C.; Chuang, L.-P.; Lin, S.-W.; Chiou, Y.-C.; Li, H.-H.; Chen, Y.-C.; Lin, Y.-J.; Chang, C.-J.; Tsai, F.-C.; Chang, K.-W.; et al. Cumulative Fluid Balance during Extracorporeal Membrane Oxygenation and Mortality in Patients with Acute Respiratory Distress Syndrome. Membranes 2021, 11, 567. [Google Scholar] [CrossRef] [PubMed]
- Ehrmann, S.; Li, J.; Ibarra-Estrada, M.; Perez, Y.; Pavlov, I.; McNicholas, B.; Roca, O.; Mirza, S.; Vines, D.; Garcia-Salcido, R.; et al. Awake prone positioning for COVID-19 acute hypoxaemic respiratory failure: A randomised, controlled, multinational, open-label meta-trial. Lancet Respir. Med. 2021, 9, 1387–1395. [Google Scholar] [CrossRef]
- Fernández-Tobar, R.; Chamorro-Jambrina, C.; Pérez-Torres, M.; Castiñeiras-Amor, B.; Alcántara-Carmona, S.; Romera-Ortega, M. Metadona como fármaco de rescate para el control de la sedoanalgesia difícil en pacientes con SDRA asociado a infección por SARS-CoV-2. Med. Intensiv. 2021, 46, 279–281. [Google Scholar] [CrossRef]
- Fujishima, S.; Gando, S.; Saitoh, D.; Kushimoto, K.; Ogura, H.; Abe, T.; Shiraishi, A.; Mayumi, T.; Sasaki, J.; Kotani, J.; et al. Outcomes of Acute Respiratory Distress Syndrome: The Focused Outcomes Research in Emergency Care in Acute Respiratory Distress Syndrome, Sepsis, and Trauma (FORECAST) Study. Shock 2020, 53, 544–549. [Google Scholar] [CrossRef]
- Fuller, B.M.; Ferguson, I.T.; Mohr, N.M.; Drewry, A.M.; Palmer, C.; Wessman, B.T.; Ablordeppey, E.; Keeperman, J.; Stephens, R.J.; Briscoe, C.C.; et al. A quasi-experimental, before-after trial examining the impact of an emergency department mechanical ventilator protocolo clinical outcomes and lung-protective ventilation in acute respiratory distress síndrome. Crit. Care Med. 2017, 45, 645–652. [Google Scholar] [CrossRef]
- Guervilly, C.; Prudhomme, E.; Pauly, V.; Bourenne, J.; Hrainech, S.; Daviet, F.; Adda, M.; Coiffard, B.; Forel, J.M.; Roch, A.; et al. Prone positioning and extracorporeal membrane oxygenation for severe acute respiratory distress syndrome: Time for a randomized trial? Intensive Care Med. 2019, 45, 1040–1042. [Google Scholar] [CrossRef]
- Killien, E.Y.; Mills, B.; Watson, R.S.; Vavilala, M.S.; Rivara, F.P. Morbidity and mortality among critically injured children with acute respiratory distress syndrome. Crit. Care Med. 2019, 47, 112–119. [Google Scholar] [CrossRef]
- Le Borgne, P.; Oberlin, M.; Bassand, A.; Abensur Vuillaume, L.; Gottwalles, Y.; Noizet, M.; Gennai, S.; Baicry, F.; Jaeger, D.; Girerd, N.; et al. Pre-Hospital management of critically ill patients with SARS-CoV-2 Infection: A retrospective multicenter study. J. Clin. Med. 2020, 9, 3744. [Google Scholar] [CrossRef]
- Li, X.; Hu, M.; Zheng, R.; Wang, Y.; Kang, H.; Jiang, L.; Zhong, M.; Sang, L.; Zheng, X.; Pan, C.; et al. Delayed initiation of Ecmo is associated with poor outcomes in patients with severe COVID-19: A multicenter retrospective cohort study. Front. Med. 2021, 8, 716086. [Google Scholar] [CrossRef] [PubMed]
- Loureiro-Amigo, J.; Suárez-Carantona, C.; Oriol, I.; Sánchez-Díaz, C.; Coloma-Conde, A.; Manzano-Espinosa, L.; Rubio-Rivas, M.; Otero-Perpiná, B.; Jenaro, M.M.F.-M.; Coduras-Erdozain, A.; et al. Prone position in COVID-19 patients with severe Acute Respiratory Distress syndrome receiving conventional oxigen therapy: A restrospective study. Arch. Bronconeumonia 2021, 57, 277–280. [Google Scholar]
- Nielsen VM, L.; Madsen, J.; Aasen, A.; Toft-Petersen, A.P.; Lübcke, K.; Rasmussen, B.S.; Christensen, E.F. Prehospital treatment with continuous positive airway pressure in patients with acute respiratory failure: A regional observational study. Scand. J. Trauma Resuscitacion Emerg. Med. 2016, 24, 121. [Google Scholar] [CrossRef] [Green Version]
- Osei-Ampofo, M.; Aidoo, A.; Antwi-Kusi, A.; Ofungwu, O.J.; Kotey, S.N.-K.; Siaw-Frimpong, M.; Chiedozie, O.; Tafoya, M.J.; Becker, T.K. Respiratory Failure requiring mechanical ventilación in critically ill adults in Ghana: A prospective observational study. Afr. J. Emerg. Med. 2018, 8, 155–157. [Google Scholar] [CrossRef]
- Piva, S.; Filippini, M.; Turla, F.; Cattaneo, S.; Margola, A.; de Fulviis, S.; Nardiello, I.; Beretta, A.; Ferrari, L.; Trotta, R.; et al. Clinical presentation and initial management critically ill patients with severe acute respiratory syndrome coronavirus 2(SARS-CoV-2) infection in Brescia Italy. J. Crit. Care 2020, 58, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Scaramuzzo, G.; Gamberini, L.; Tonetti, T.; Zani, G.; Ottaviani, I.; Mazzoli, C.A.; Capozzi, C.; Giampalma, E.; Reggiani, M.L.B.; Bertellini, E.; et al. Sustained oxygenation improvement after first prone positioning is associated with liberation from mechanical ventilation and mortality in critically ill COVID-19 patients: A cohort study. Ann. Intensiv. Care 2021, 11, 63. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Hajage, D.; Lebreton, G.; Monsel, A.; Voiriot, G.; Levy, D.; Baron, E.; Beurton, A.; Chommeloux, J.; Meng, P.; et al. Extracorporeal Membrane Oxigenation for several Acute Respiratory Distress Syndrome associate with COVID-19: A restrospective cohort study. Lancet Respir. Med. 2020, 8, 1121–1131. [Google Scholar] [CrossRef]
- Sánchez Zuñiga, M.; Carrillo Esper, R.; Garnica Escamilla, M.; Medveczky Ordoñes, N.; Carrillo Cordoba, D. Stratification of the severity of the Acute Respiratory Distress Syndrome at 24 hours after diagnosis. Med. Interna México 2019, 35, 5–15. [Google Scholar]
- Hodroge, S.S.; Glenn, M.; Breyre, A.; Lee, B.; Aldridge, N.R.; Sporer, K.A.; Koenig, K.L.; Gausche-Hill, M.; Salvucci, A.A.; Rudnick, E.M.; et al. Adult Patients with Respiratory Distress: Current Evidence-based Recommendations for Prehospital Care. West. J. Emerg. Med. 2020, 21, 849–857. [Google Scholar] [CrossRef]
- Mohammadi, M.; Pour Khamseh, A.K.; Varpaei, H.A. Invasive Airway "Intubation" in COVID-19 Patients; Statistics, Causes, and Recommendations: A Review Article. Anesthesiol. Pain Med. 2021, 11, e115868. [Google Scholar] [CrossRef]
- Fayed, M.; Patel, N.; Yeldo, N.; Nowak, K.; Penning, D.H.; Torres, F.V.; Natour, A.K.; Chhina, A. Effect of Intubation Timing on the Outcome of Patients With Severe Respiratory Distress Secondary to COVID-19 Pneumonia. Cureus 2021, 13, e19620. [Google Scholar] [CrossRef] [PubMed]
- Papoutsi, E.; Giannakoulis, V.G.; Xourgia, E.; Routsi, C.; Kotanidou, A.; Siempos, I.I. Effect of timing of intubation on clinical outcomes of critically ill patients with COVID-19: A systematic review and meta-analysis of non-randomized cohort studies. Crit. Care 2021, 25, 121. [Google Scholar] [CrossRef] [PubMed]
- Laghlam, D.; Charpentier, J.; Hamou, Z.A.; Nguyen, L.S.; Pene, F.; Cariou, A.; Mira, J.-P.; Jozwiak, M. Effects of Prone Positioning on Respiratory Mechanics and Oxygenation in Critically Ill Patients With COVID-19 Requiring Venovenous Extracorporeal Membrane Oxygenation. Front. Med. 2022, 8, 810393. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Hentschker, C.; Westhoff, M.; Weber-Carstens, S.; Janssens, U.; Kluge, S.; Pfeifer, M.; Spies, C.; Welte, T.; Rossaint, R.; et al. Observational study of changes in utilization and outcomes in mechanical ventilation in COVID-19. PLoS ONE. 2022, 17, e0262315. [Google Scholar] [CrossRef]
- Guerin, C.; Richard, K.; Beitler, J.; Gattinoni, L.; Jaber, S.; Marini, J.; Munshi, L.; Papazian, L.; Pesenti, A.; Vieillard-Baron, A.; et al. Posición Prone Position in ARDS Patients: Why, When, How and for Whom. Intensive. Care. Med. 2020, 46, 2385–2396. [Google Scholar] [CrossRef]
- Jiang, L.G.; LeBaron, J.; Bodnar, D.; Caputo, N.D.; Chang, B.P.; Chiricolo, G.; Flores, S.; Kenny, J.; Melville, L.; Sayan, O.R.; et al. Conscious Proning: An Introduction of a Proning Protocol for Nonintubated, Awake, Hypoxic Emergency Department COVID-19 Patients. Acad. Emerg. Med. 2020, 27, 566–569. [Google Scholar] [CrossRef]
- Liu, C.; Chen, Y.; Chen, Y.; Chen, B.; Xie, G.; Chen, Y. Effects of prone positioning during extracorporeal membrane oxygenation for refractory respiratory failure: A systematic review. SN Compr. Clin. Med. 2021, 15, 1–7. [Google Scholar] [CrossRef]
- David, B.; Tobias, W.; George, K. Transport of a prone position Acute Respiratory Distress Syndrome patient. Air Med. J. 2018, 37, 206–210. [Google Scholar]
- Shaefi, S.; Brenner, S.K.; Gupta, S.; O’Gara, B.P.; Krajewski, M.L.; Charytan, D.M.; Chaudhry, S.; Mirza, S.H.; Peev, V.; Anderson, M.; et al. Extracorporeal membrane oxygenation in patients with severe respiratory failure from COVID-19. Intensive Care Med. 2021, 47, 208–221. [Google Scholar] [CrossRef]
- Baltaji, S.; Ledgerwood, C.; Finoli, L.; Lyons, C.; Cheema, T. Supportive Management and Interventions for Respiratory Failure Due to SARS-CoV-2. Crit. Care Nurse 2022, 43, 369–380. [Google Scholar] [CrossRef]
- Ronco, C.; Navalesi, P.; Vincent, J. Coronavirus Epidemic Preparing for extracorporeal Organ Support in intensive Care. Lancet Respir. Med. 2020, 8, 240–241. [Google Scholar] [CrossRef]
- Kuljit, S.; Parhar, L.; Blackwood Zuege, D.; Singh, G. Optimizing provision of estracorporeal life support during the COVID-19 pandemic: Praticas considerations for Canadian Jurisdictions. CMAJ 2020, 192, 372–374. [Google Scholar]
- Winck, J.C.; Ambrosino, N. COVID-19 pandemic and non invasive respiratory management: Every Goliath needs a David. An evidence based evaluation of problems. Pulmonology 2020, 26, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, M.; Brábek, J. COVID-19, corticosteroids and public health: A reappraisal. Public Health 2021, 197, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Chen, L.; Ni, H. The effectiveness of Corticosteroids on mortality in patients with acute respiratory distress syndrome or acute lung injury: A secondary analysis. Sci. Rep. 2015, 5, 17654. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.U.; Nair, S.C.; Din, M.U.; Dar, M.R.; Masood, M.; Al Menhali, A.R.S.; Al Nuaimi, M.M.; Sreedharan, J.; Gasmelseed, H.I.; Khan, A.A. Methylprednisolone Treatment Versus Standard Supportive Care for Adult COVID-19 Mechanically Ventilated, Acute Respiratory Distress Syndrome Patients. SN Compr. Clin. Med. 2022, 4, 11. [Google Scholar] [CrossRef]
- Naveda, O.; Romero, A. Risk factors for the development of acute respiratory distress syndrome: A case-control study. Pediatría 2016, 43, 225–231. [Google Scholar] [CrossRef] [Green Version]
- RECOVERY. Oxford: University of Oxford. Low-cost dexamethasone reduces death by up to one third in hospitalised patients with severe respiratory complications of COVID-19. 2020. Available online: https://www.recoverytrial.net/files/recovery_dexamethasone_statement_160620_v2final.pdf (accessed on 8 February 2022).
- Carmona, L.E.O.; Nielfa, M.D.C.C.; Alvarado, A.L.D. The Covid-19 pandemic seen from the frontline. Int. Braz. J. Urol. 2020, 46 (Suppl S1), 181–194. [Google Scholar] [CrossRef]

{kind=link}
| Author/Year (Country) | Design | Sample | Aims | Support and Technique | Results | Level of Evidence/Grade of Recommendation |
|---|---|---|---|---|---|---|
| Bohman et al. [15], 2016. (EEUU) | Observational prospective | 767 patients | Identify and classify patients with newly diagnosed acute respiratory distress syndrome (ARDS) who may progress to severe ARDS. | ECMO | Data-Driven Early Prediction ECMO Eligibility for Severe ARDS Score commonly uses variables from ARDS patients within 12 h of intubation and could be used to identify patients who may merit early transfer to a center ECMO-trained physician. | 2c/B |
| Chiu et al. [16], 2021. (China) | Observational prospective | 152 patients | To investigate the effect of cumulative fluid balance during the early phase of ECMO on clinical outcomes and hospital mortality in patients with severe ARDS | There was a stepwise increase in hospital mortality corresponding to an increase in CFB quartile, with significant between-group differences in terms of 28-, 60-, and 90-day hospital mortality (all p < 0.05). Patients in lower CFB quartiles presented more ECMO-free days by day 28; however, the effect was not significant. We observed significantly higher 28- and 60-day ventilator-free days in lower CFB quartiles (p = 0.002 and 0.001, respectively). We also observed significantly lower overall 90-day survival rates in quartile 4 (overall comparison, p = 0.001, log-rank test), as follows: quartile 1 (63.2%), quartile 2 (55.3%), quartile 3 (50%), and quartile 4 (31.6%). | 2c/B | |
| Ehrmann et al. [17], 2021. (Canada, EEUU, France, Ireland, Mexico, Spain) | Randomized Controlled Trial | 1126 patients | To evaluate the efficacy of awake prone positioning to prevent intubation or death in patients with severe COVID-19 in a large-scale randomised trial. | Prone positioning | Treatment failure occurred in 223 (40%) of 564 patients assigned to awake prone positioning and in 257 (46%) of 557 patients assigned to standard care (relative risk 0·86 [95% CI 0·75–0·98]). The hazard ratio for intubation was 0·75 (0·62–0·91), and the HR for mortality was 0·87 (0·68–1·11) with awake prone positioning compared with standard care within 28 days of enrolment. The incidence of prespecified adverse events was low and similar in both groups. | 1b/A |
| Fernández Tobar et al. [18], 2016. (Spain) | Observational retrospective | 13 patients | To describe the experience with the use of methadone for the control of difficult sedation (SAD), in patients ventilated for secondary ARDS COVID-19 in whom it has been failed with the use of the usual drugs. | Use of methadone | 85% of the patients improved the quality of sedation-analgesia, achieving values -2 and 0 on the RASS scale (Richmond Agitation-Sedation Scale), pain control, with a visual numerical scale <4 and the dose could be reduced of drugs used for adaptation to MV. Methadone is a drug to be considered in the management of SAD pictures secondary to the administration of high and prolonged doses of sedative drugs and opiates during MV in patients with ARDS. | 2c/B |
| Fujishima et al. [19], 2020. (Japan) | Observational prospective | 166 patients | To examine therapeutic strategies for ARDS. | Mechanic ventilation | The proportion of patients with PaO2/FIO2 ≤ 100, patients under positive pressure invasive ventilation, and in-hospital mortality was 39.2%, 92.2%, and 38.0% for American—European Consensus Conference acute lung injury criteria. As well, 38.9%, 96.8%, and 37.6% for patients with Berlin definition ARDS, respectively. | 2c/B |
| Fuller et al. [20], 2018. (EEUU) | Quasi-experimental | 229 patients | To assess the impact of mechanical ventilation in an emergency department (ED). Protocol on clinical outcomes and adherence to lung protective ventilation in patients with ARDS. | Mechanical Ventilation Protocol (1) protective tidal volume of the lungs; (2) appropriate setting of positive pressure at the end of expiration (PEEP); (3) weaning from oxygen; and (4) elevation of the head of the bed) | The mechanical ventilation protocol was associated with a reduction in mortality from 54.8% to 39.5% (OR 0.38, 95% CI 0.17–0.83, p = 0.02) and a 3.9-day increase in ventilator-free days, p = 0.01. | 2c/B |
| Guervilly et al. [21], 2019. (EEUU) | Observational retrospective | 168 patients | To compare the results of patients with severe ARDS under ECMO according to the use of Prone Position or lack of it during their execution of ECMO. | Prone and ulnar position and ECMO | Patients in the prone ECMO group were more likely to be weaned from ECMO. Consequently, the 30-day, 60-day, and 90-day survival rates were significantly higher. | 2c/B |
| Killien et al [22], 2019. (Canada and EEUU) | Observational prospective | 146,058 patients | To assess morbidity and mortality in children with ARDS. | Hospital mortality and the need for post-discharge care | Mortality was 20.0% among patients with ARDS versus 4.3% among patients without ARDS. Post-discharge care was required in an additional 44.8% of patients with ARDS versus 16.0% of patients without ARDS (aRR 3.59, 2.87–4.49). | 2c/B |
| Le Borgne et al. [23], 2020. (France) | Observational retrospective | 103 patients | To describe the characteristics and therapeutic management of the mobile emergency service of patients with vital distress due to COVID-19, their hospital care pathway and their in-hospital evolution. | Mechanic ventilation | Serious SARS-CoV-2 infections have revealed two different clinical presentations. The first phenotype (“happy” hypoxemia) should be managed similarly to the second phenotype (hypoxemia with clinical acute respiratory failure) which includes early admission to the ICU or close supervision in a high dependency unit for appropriate life support. The clinical phenotypes appear to be highly differentiable in the pre-hospital setting, but no differences were found in terms of mortality; therefore, identical management is recommended in the initial phase. | 2c/B |
| Li et al. [24], 2021. (Thailand) | Observational retrospective | 31 patients | To investigate the timing of ECMO initiation in critically ill patients with COVID-19. | ECMO | The 60-day mortality rate after ECMO was 71% and the weaning rate from ECMO was 26%. The early initiation of ECMO was associated with a decrease in mortality at 60 days after ECMO (50 vs. 88%, p = 0.044) and an increase in the weaning rate of ECMO (50 vs. 6%, p = 0.011). | 2c/B |
| Loureiro-Amigo et al. [25], 2021. (Spain) | Observational retrospective | 163 patients | To assess the impact on hospital mortality of the prone position in spontaneously breathing patients with COVID-19 and severe ARDS. | Prone positioning | Patients treated with the prone position had lower mortality (62.1% vs. 43.3%, p = 0.0229), with an estimated OR of 0.47 (95% CI: 0.24 to 0.89). The use of the prone position showed a protective effect on mortality (OR 0.42, 95% CI 0.18 to 0.98). | 2c/B |
| Nielsen et al. [26], 2016. (Denmark) | Observational prospective | 171 patients | To assess adherence to treatment and the efficacy of CPAP as an addition to standard care. | Continuous positive airway pressure CPAP | Patients with CPAP had a greater increase in SpO2 than patients without CPAP (87 to 96% versus 92 to 96%, p < 0.01) and a greater decrease in respiratory rate (32 to 25 versus 28 to 24 breaths/min, p < 0.01. | 2c/B |
| Osei-Ampofo [27] et al, 2018. (Ghana) | Observational prospective | 82 patients | To assess the incidence of respiratory failure requiring mechanical ventilation and the presence and Outcomes of ARDS. | Mechanic ventilation | In this study, intubation and mechanical ventilation were performed in 9% of critically ill patients. While only 2.4% of the intubated patients met the criteria for ARDS. | 2c/B |
| Piva et al. [28], 2020. (Italy) | Observational prospective | 44 patients | To analyse the experience in caring for COVID-19 patients. | Use of invasive, non-invasive ventilation, and adjuvant therapies for the treatment of COVID-19 | Non-invasive ventilation was performed in 39% of the patients during part or all of their stay in the ICU without infection of the patient. 97% of the patients required FiO2 ≥50% upon admission to the ICU, with a mean of 80%, although the patients were able to oxygenate with adequate SaO2 values. Severe ARDS, with PaO2/FiO2 <150 mmHg, was present in 64% of the patients. 39% of the patients were managed with non-invasive positive pressure ventilation for part or all of their stay in the ICU. Patients who received invasive mechanical ventilation were ventilated with low tidal volume ventilation. | 2c/B |
| Scaramuzzo et al. [29], 2021. (Italy) | Observational prospective | 470 patients | To analyze whether the variation in oxygenation after the first prone positioning session, compared to the pre- prone positioning state, could be associated with ventilation-free days (VFD) in the ICU, mortality in the ICU and the probability of release of mechanical ventilation evaluated at 28 days after admission to the ICU. | Prone positioning | The median PaO2/FiO2 variation after the first PP cycle was 49 [19–100%] and no differences were found in demographics, comorbidities, ventilatory treatment and PaO2/FiO2 before prone positioning between responders (96/191) and non-responders (95/191). Moreover, oxygenation response after the first positioning was independently associated to liberation from mechanical ventilation at 28 days and was increasingly higher being higher the oxygenation response to PP | 2c/B |
| Schimdt et al. [30], 2018. (France) | Prospective observational cohort | 83 patients | To describe the ventilatory management, characteristics and outcome of patients treated with ECMO with ARDS. | ECMO | ECMO must be considered for patients who develop refractory respiratory failure. | 2c/B |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Granados-Bolivar, M.E.; Quesada-Caballero, M.; Suleiman-Martos, N.; Romero-Béjar, J.L.; Albendín-García, L.; Cañadas-De la Fuente, G.A.; Caballero-Vázquez, A. Evolution of Acute Respiratory Distress Syndrome in Emergency and Critical Care: Therapeutic Management before and during the Pandemic Situation. Medicina 2022, 58, 726. https://doi.org/10.3390/medicina58060726
Granados-Bolivar ME, Quesada-Caballero M, Suleiman-Martos N, Romero-Béjar JL, Albendín-García L, Cañadas-De la Fuente GA, Caballero-Vázquez A. Evolution of Acute Respiratory Distress Syndrome in Emergency and Critical Care: Therapeutic Management before and during the Pandemic Situation. Medicina. 2022; 58(6):726. https://doi.org/10.3390/medicina58060726
Chicago/Turabian StyleGranados-Bolivar, Monserrat E., Miguel Quesada-Caballero, Nora Suleiman-Martos, José L. Romero-Béjar, Luis Albendín-García, Guillermo A. Cañadas-De la Fuente, and Alberto Caballero-Vázquez. 2022. "Evolution of Acute Respiratory Distress Syndrome in Emergency and Critical Care: Therapeutic Management before and during the Pandemic Situation" Medicina 58, no. 6: 726. https://doi.org/10.3390/medicina58060726