
Update on Interventional Management of Neuropathic Pain: A Delphi Consensus of the Spanish Pain Society Neuropathic Pain Task Force

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
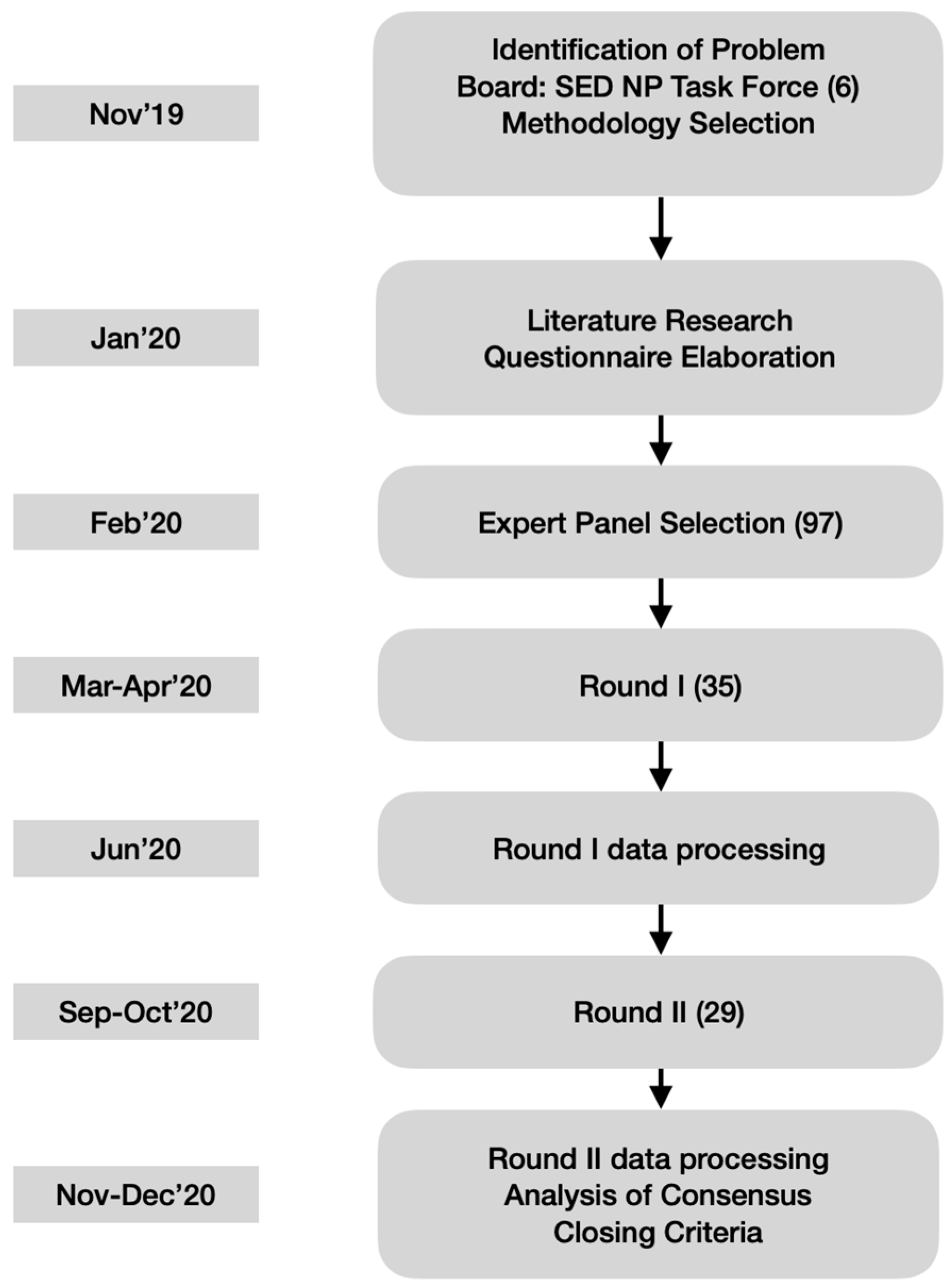
2.1. The Delphi Technique
- the use of a reproducible procedure to select participants and a pre-specified definition of consensus (see below),
- a fixed criterion to stop the process after the completion of the second round regardless of the level of consensus reached,
- and the inability to drop, add or combine items between both rounds by neither study coordinators nor panelists.
2.2. The Questionnaire
2.3. Participants
2.4. Ethical and Legal Aspects
3. Results
3.1. Botulinum Toxins
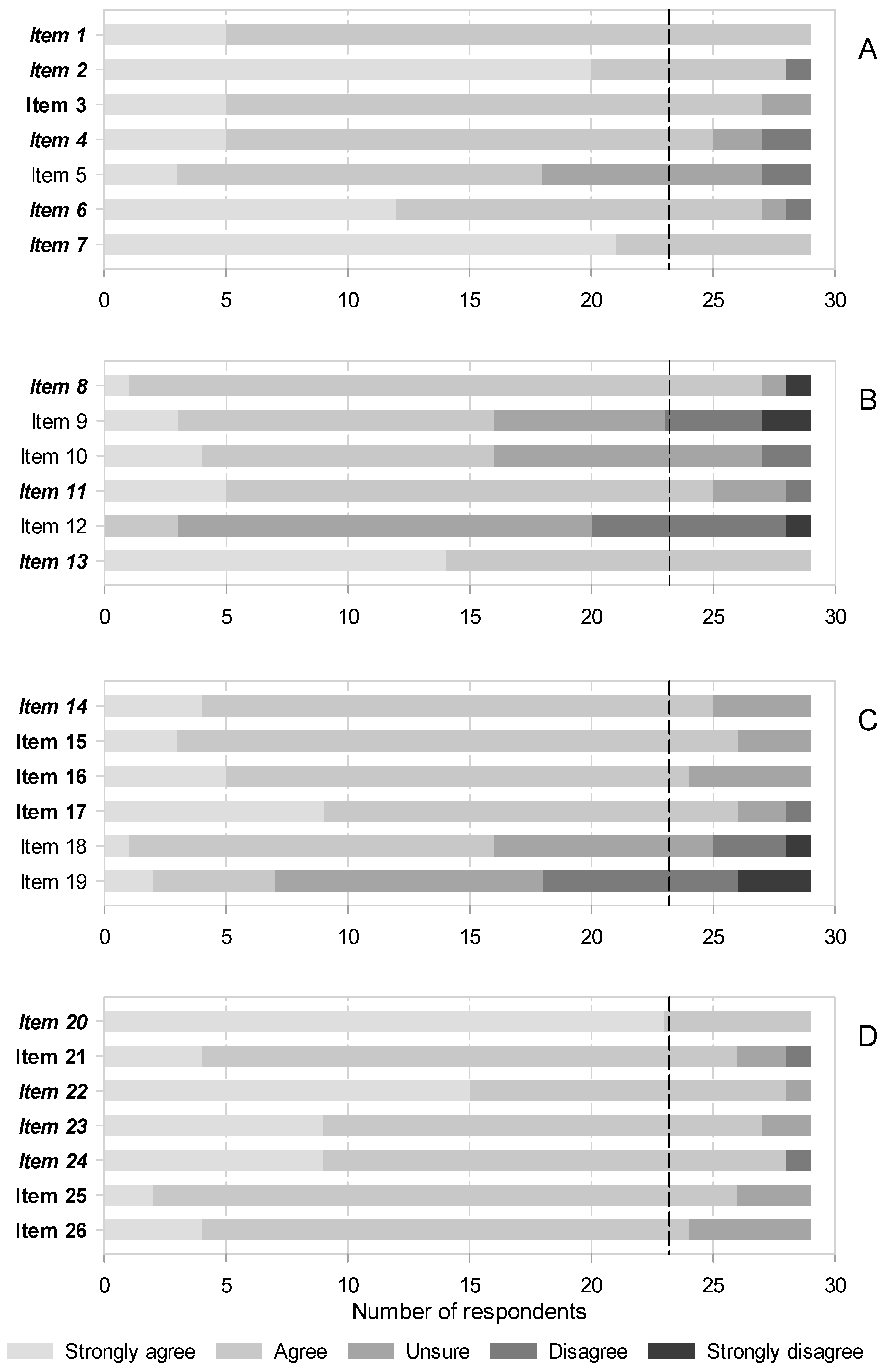
3.2. Infiltrations
- that infiltrative blocks for postherpetic neuralgia (PHN) should be recommended in clinical practices (Figure 2B, items 8),
- that perineural blocks with corticosteroids are effective for NP in general (Figure 2B, 11),
- and that first lumbar spinal (ilioinguinal and iliohypogastric) nerve blocks with local anesthetics and corticosteroids in combination are effective to treat chronic postsurgical pain (CPSP) after hernia repair (Figure 2B, 13).
3.3. Radiofrequency
3.4. Neuromodulation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van Hecke, O.; Austin, S.K.; Khan, R.A.; Smith, B.H.; Torrance, N. Neuropathic pain in the general population: A systematic review of epidemiological studies. Pain 2014, 155, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.B.; et al. Neuropathic pain. Nat. Rev. Drug Prers. 2017, 3, 17002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doth, A.H.; Hansson, P.T.; Jensen, M.P.; Taylor, R.S. The burden of neuropathic pain: A systematic review and meta-analysis of health utilities. Pain 2010, 149, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.H.; Torrance, N.; Bennett, M.I.; Lee, A.J. Health and quality of life associated with chronic pain of predominantly neuropathic origin in the community. Clin. J. Pain 2007, 23, 143–149. [Google Scholar] [CrossRef]
- Smith, B.H.; Hebert, H.L.; Veluchamy, A. Neuropathic pain in the community: Prevalence, impact, and risk factors. Pain 2020, 161 (Suppl. 1), S127–S137. [Google Scholar] [CrossRef]
- Breivik, H.; Eisenberg, E.; O’Brien, T.; OPENMinds. The individual and societal burden of chronic pain in Europe: The case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Health 2013, 13, 1229. [Google Scholar] [CrossRef] [Green Version]
- Baron, R.; Maier, C.; Attal, N.; Binder, A.; Bouhassira, D.; Cruccu, G.; Finnerup, N.B.; Haanpää, M.; Hansson, P.; Hüllemann, P.; et al. Peripheral neuropathic pain: A mechanism-related organizing principle based on sensory profiles. Pain 2017, 158, 261–272. [Google Scholar] [CrossRef] [Green Version]
- Scholz, J.; Finnerup, N.B.; Attal, N.; Aziz, Q.; Baron, R.; Bennet, M.I.; Benoliel, R.; Cohen, M.; Cruccu, G.; Davis, K.D.; et al. The IASP classification of chronic pain for ICD-11: Chronic neuropathic pain. Pain 2019, 160, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Dworkin, R.H.; O’Connor, A.B.; Kent, J.; Mackey, S.C.; Raja, S.N.; Stacey, B.R.; Levy, R.M.; Backonja, M.; Baron, R.; Harke, H.; et al. Interventional management of neuropathic pain: NeuPSIG recommendations. Pain 2013, 154, 2249–2261. [Google Scholar] [CrossRef] [Green Version]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Bouhassira, D.; Attal, N. Emerging therapies for neuropathic pain: New molecules or new indications for old treatments? Pain 2018, 159, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Finnerup, N.B.; Haroutounian, S.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Jensen, T.S.; Kamerman, P.R.; McNicol, E.; Moore, A.; et al. Neuropathic pain clinical trials: Factors associated with decreases in estimated drug efficacy. Pain 2018, 159, 2339–2346. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.; Schultheis, B.C.; Hanes, M.C.; Joly, S.M.; Chakravarthy, K.V.; Deer, T.R.; Levy, R.M.; Hunter, C.W. A Comprehensive Algorithm for Management of Neuropathic Pain. Pain Med. 2019, 20, S2–S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, Y.; Luo, L.; Hu, Y.; Liu, J. Clinical practice guidelines for the management of neuropathic pain: A systematic review. BMC Anesth. 2016, 16, 12. [Google Scholar] [CrossRef] [Green Version]
- Cruccu, G.; Truini, A. A review of Neuropathic Pain: From Guidelines to Clinical Practice. Pain 2017, 6, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Moisset, X.; Bouhassira, D.; Avez Couturier, J.; Alchaar, J.; Conradi, S.; Delmotte, M.H.; Lanteri-Minet, M.; Lefaucheur, J.P.; Mick, G.; Piano, V.; et al. Pharmacological and non-pharmacological treatments for neuropathic pain: Systematic review and French recommendations. Rev. Neurol. 2020, 176, 325–352. [Google Scholar] [CrossRef]
- Varshney, V.; Osborn, J.; Chaturvedi, R.; Shah, V.; Chakravarthy, K.V. Advances in the interventional management of neuropathic pain. Ann. Transl. Med. 2021, 9, 187. [Google Scholar] [CrossRef]
- Deer, T.R.; Mekhail, N.; Provenzano, D.; Pope, J.; Krames, E.; Leong, M.; Levy, R.M.; Abejon, D.; Buchser, E.; Burton, A.; et al. The appropriate use of neurostimulation of the spinal cord and peripheral nervous system for the treatment of chronic pain and ischemic diseases: The Neuromodulation Appropriateness Consensus Committee. Neuromodulation 2014, 17, 515–550, discussion 550. [Google Scholar] [CrossRef]
- McMillan, S.S.; King, M.; Tully, M.P. How to use the nominal group and Delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef]
- Oh, H.M.; Chung, M.E. Botulinum Toxin for Neuropathic Pain: A Review of the Literature. Toxins 2015, 7, 3127–3154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittal, S.O.; Safarpour, D.; Jabbari, B. Botulinum Toxin Treatment of Neuropathic Pain. Semin. Neurol. 2016, 36, 73–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, F.; Peng, K.; Yang, J.P.; Ji, F.H.; Xia, F.; Meng, X.W. Botulinum toxin-A for the treatment of neuralgia: A systematic review and meta-analysis. J. Pain Res. 2018, 11, 2343–2351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, J.; Zhu, X.; Yang, G.; Shen, J.; Xie, P.; Zuo, X.; Xia, L.; Han, Q.; Zhao, Y. The efficacy and safety of botulinum toxin type A in treatment of trigeminal neuralgia and peripheral neuropathic pain: A meta-analysis of randomized controlled trials. Brain Behav. 2019, 9, e01409. [Google Scholar] [CrossRef]
- Wang, C.; Zhang, Q.; Wang, R.; Xu, L. Botulinum Toxin Type A for Diabetic Peripheral Neuropathy Pain: A Systematic Review and Meta-Analysis. J. Pain Res. 2021, 14, 3855–3863. [Google Scholar] [CrossRef]
- Egeo, G.; Fofi, L.; Barbanti, P. Botulinum Neurotoxin for the Treatment of Neuropathic Pain. Front. Neurol. 2020, 11, 716. [Google Scholar] [CrossRef]
- Attal, N.; de Andrade, D.C.; Adam, F.; Ranoux, D.; Teixeira, M.J.; Galhardoni, R.; Raicher, I.; Üçeyler, N.; Sommer, C.; Bouhassira, D. Safety and efficacy of repeated injections of botulinum toxin A in peripheral neuropathic pain (BOTNEP): A randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2016, 15, 555–565. [Google Scholar] [CrossRef]
- Bendtsen, L.; Zakrzewska, J.M.; Abbott, J.; Braschinsky, M.; Di Stefano, G.; Donnet, A.; Eide, P.K.; Leal, P.R.L.; Maarbjerg, S.; May, A.; et al. European Academy of Neurology guideline on trigeminal neuralgia. Eur. J. Neurol. 2019, 26, 831–849. [Google Scholar] [CrossRef] [Green Version]
- Meyer-Friessem, C.H.; Eitner, L.B.; Kaisler, M.; Maier, C.; Vollert, J.; Westermann, A.; Zahn, P.K.; Ávila González, C.A. Perineural injection of botulinum toxin-A in painful peripheral nerve injury—A case series: Pain relief, safety, sensory profile and sample size recommendation. Curr. Med. Res. Opin. 2019, 35, 1793–1803. [Google Scholar] [CrossRef]
- Fabregat, G.; De Andres, J.; Villanueva-Perez, V.L.; Asensio-Samper, J.M. Subcutaneous and perineural botulinum toxin type a for neuropathic pain: A descriptive review. Clin. J. Pain 2013, 29, 1006–1012. [Google Scholar] [CrossRef]
- Rovenstine, E.A.; Wertheim, H.M. Therapeutic Nerve Block. JAMA 1941, 117, 1599–1603. [Google Scholar] [CrossRef]
- Varrassi, G.; Paladini, A.; Marinangeli, F.; Racz, G. Neural modulation by blocks and infusions. Pain Pr. 2006, 6, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Vlassakov, K.V.; Narang, S.; Kissin, I. Local anesthetic blockade of peripheral nerves for treatment of neuralgias: Systematic analysis. Anesth. Analg. 2011, 112, 1487–1493. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.S.; Lin, Y.C.; Lao, H.C.; Chen, C.C. Interventional Treatments for Postherpetic Neuralgia: A Systematic Review. Pain Physician 2019, 22, 209–228. [Google Scholar] [CrossRef]
- Kim, H.J.; Ahn, H.S.; Lee, J.Y.; Choi, S.S.; Cheong, Y.S.; Kwon, K.; Yoon, S.H.; Leem, J.G. Effects of applying nerve blocks to prevent postherpetic neuralgia in patients with acute herpes zoster: A systematic review and meta-analysis. Korean J. Pain 2017, 30, 3–17. [Google Scholar] [CrossRef]
- Makharita, M.Y.; Amr, Y.M. Effect of Repeated Paravertebral Injections with Local Anesthetics and Steroids on Prevention of Post-herpetic Neuralgia. Pain Physician 2020, 23, 565–572. [Google Scholar]
- Manchikanti, L.; Knezevic, N.N.; Navani, A.; Christo, P.J.; Limerick, G.; Calodney, A.K.; Grider, J.; Harned, M.E.; Cintron, L.; Gharibo, C.J.; et al. Epidural Interventions in the Management of Chronic Spinal Pain: American Society of Interventional Pain Physicians (ASIPP) Comprehensive Evidence-Based Guidelines. Pain Physician 2021, 24, S27–S208. [Google Scholar]
- Bhatia, A.; Flamer, D.; Shah, P.S. Perineural steroids for trauma and compression-related peripheral neuropathic pain: A systematic review and meta-analysis. Can. J. Anaesth. 2015, 62, 650–662. [Google Scholar] [CrossRef] [Green Version]
- Eker, H.E.; Cok, O.Y.; Aribogan, A.; Arslan, G. Management of neuropathic pain with methylprednisolone at the site of nerve injury. Pain Med. 2012, 13, 443–451. [Google Scholar] [CrossRef] [Green Version]
- Abram, S.E. Neural blockade for neuropathic pain. Clin. J. Pain 2000, 16, S56–S61. [Google Scholar] [CrossRef]
- Chesterton, L.S.; Blagojevic-Bucknall, M.; Burton, C.; Dziedzic, K.S.; Davenport, G.; Jowett, S.M.; Myers, H.L.; Oppong, R.; Rathood-Mistry, T.; van der Windt, D.A.; et al. The clinical and cost-effectiveness of corticosteroid injection versus night splints for carpal tunnel syndrome (INSTINCTS trial): An open-label, parallel group, randomised controlled trial. Lancet 2018, 392, 1423–1433. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Chen, M.; Zhang, Y.; Zhou, H.; Yu, X.; Chen, G. Ilioinguinal/iliohypogastric nerve block versus transversus abdominis plane block for pain management following inguinal hernia repair surgery: A systematic review and meta-analysis of randomized controlled trials. Medicine 2019, 98, e17545. [Google Scholar] [CrossRef] [PubMed]
- Massaron, S.; Bona, S.; Fumagalli, U.; Battafarano, F.; Elmore, U.; Rosati, R. Analysis of post-surgical pain after inguinal hernia repair: A prospective study of 1,440 operations. Hernia 2007, 11, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.S.; Rai, A.; Sundara Rajan, R.; Jackson, T.D.; Bhatia, A. A scoping review of perineural steroids for the treatment of chronic postoperative inguinal pain. Hernia 2016, 20, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Wie, C.; Gupta, R.; Maloney, J.; Pew, S.; Freeman, J.; Strand, N. Interventional Modalities to Treat Complex Regional Pain Syndrome. Curr. Pain Headache Rep. 2021, 25, 10. [Google Scholar] [CrossRef]
- Cosman, E.R., Jr.; Cosman, E.R., Sr. Electric and thermal field effects in tissue around radiofrequency electrodes. Pain Med. 2005, 6, 405–424. [Google Scholar] [CrossRef]
- Bogduk, N. Pulsed radiofrequency. Pain Med. 2006, 7, 396–407. [Google Scholar] [CrossRef]
- Sluijter, M.E.; van Kleef, M. Pulsed Radiofrequency. Pain Med. 2007, 8, 388–389. [Google Scholar] [CrossRef] [Green Version]
- Sweet, W.G. Proceedings: Analgesia dolorosa after differential retrogasserian thermal or mechanical rhizotomy: Tactics employed to decrease its influence. J. Neurol. Neurosurg. Psychiatry 1975, 38, 407. [Google Scholar] [CrossRef] [Green Version]
- Chang, M.C. Efficacy of Pulsed Radiofrequency Stimulation in Patients with Peripheral Neuropathic Pain: A Narrative Review. Pain Physician 2018, 21, E225–E234. [Google Scholar] [CrossRef]
- Wan, C.; Dong, D.S.; Song, T. High-Voltage, Long-Duration Pulsed Radiofrequency on Gasserian Ganglion Improves Acute/Subacute Zoster-Related Trigeminal Neuralgia: A Randomized, Double-Blinded, Controlled Trial. Pain Physician 2019, 22, 361–368. [Google Scholar] [PubMed]
- Ding, Y.; Li, H.; Hong, T.; Zhao, R.; Yao, P.; Zhao, G. Efficacy and Safety of Computed Tomography-Guided Pulsed Radiofrequency Modulation of Thoracic Dorsal Root Ganglion on Herpes Zoster Neuralgia. Neuromodulation 2019, 22, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.D.; Lee, Y.I.; Park, H.J. Comparison of efficacy of continuous epidural block and pulsed radiofrequency to the dorsal root ganglion for management of pain persisting beyond the acute phase of herpes zoster. PLoS ONE 2017, 12, e0183559. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Dong, X.; Zhao, X. Treatment of trigeminal neuralgia by radiofrequency of the Gasserian ganglion. Rev. Neurosci. 2016, 27, 739–743. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, Z.; Li, K.; Su, X.; Du, C.; Tian, J. Radiofrequency thermocoagulation for the treatment of trigeminal neuralgia. Exp. Med. 2022, 23, 17. [Google Scholar] [CrossRef] [PubMed]
- Kanpolat, Y.; Savas, A.; Bekar, A.; Berk, C. Percutaneous controlled radiofrequency trigeminal rhizotomy for the treatment of idiopathic trigeminal neuralgia: 25-year experience with 1,600 patients. Neurosurgery 2001, 48, 524–532, discussion 532–524. [Google Scholar] [CrossRef] [PubMed]
- Bharti, N.; Sujith, J.; Singla, N.; Panda, N.B.; Bala, I. Radiofrequency Thermoablation of the Gasserian Ganglion Versus the Peripheral Branches of the Trigeminal Nerve for Treatment of Trigeminal Neuralgia: A Randomized, Control Trial. Pain Physician 2019, 22, 147–154. [Google Scholar] [CrossRef]
- Huibin, Q.; Jianxing, L.; Guangyu, H.; Dianen, F. The treatment of first division idiopathic trigeminal neuralgia with radiofrequency thermocoagulation of the peripheral branches compared to conventional radiofrequency. J. Clin. Neurosci. 2009, 16, 1425–1429. [Google Scholar] [CrossRef]
- Ding, Y.; Hong, T.; Li, H.; Yao, P.; Zhao, G. Efficacy of CT Guided Pulsed Radiofrequency Treatment for Trigeminal Postherpetic Neuralgia. Front. Neurosci. 2019, 13, 708. [Google Scholar] [CrossRef]
- Shi, Y.; Wu, W. Treatment of Neuropathic Pain Using Pulsed Radiofrequency: A Meta-analysis. Pain Physician 2016, 19, 429–444. [Google Scholar]
- Racz, G.B.; Stanton-Hicks, M. Lumbar and thoracic sympathetic radiofrequency lesioning in complex regional pain syndrome. Pain Pr. 2002, 2, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Straube, S.; Derry, S.; Moore, R.A.; Cole, P. Cervico-thoracic or lumbar sympathectomy for neuropathic pain and complex regional pain syndrome. Cochrane Database Syst. Rev. 2013, CD002918. [Google Scholar] [CrossRef] [PubMed]
- Mailis, A.; Furlan, A. Sympathectomy for neuropathic pain. Cochrane Database Syst. Rev. 2003, CD002918. [Google Scholar]
- Zacharias, N.A.; Karri, J.; Garcia, C.; Lachman, L.K.; Abd-Elsayed, A. Interventional Radiofrequency Treatment for the Sympathetic Nervous System: A Review Article. Pain 2021, 10, 115–141. [Google Scholar] [CrossRef]
- International Neuromodulation Society. About Neuromodulation. Available online: https://www.neuromodulation.com/about-neuromodulation (accessed on 31 December 2021).
- Malinowski, M.N.; Chopra, P.R.; Tieppo Francio, V.; Budwany, R.; Deer, T.R. A narrative review and future considerations of spinal cord stimulation, dorsal root ganglion stimulation and peripheral nerve stimulation. Curr. Opin. Anaesthesiol. 2021, 34, 774–780. [Google Scholar] [CrossRef]
- Vallejo, R.; Bradley, K.; Kapural, L. Spinal Cord Stimulation in Chronic Pain: Mode of Action. Spine 2017, 42 (Suppl. 14), S53–S60. [Google Scholar] [CrossRef] [PubMed]
- Rock, A.K.; Truong, H.; Park, Y.L.; Pilitsis, J.G. Spinal Cord Stimulation. Neurosurg. Clin. N Am. 2019, 30, 169–194. [Google Scholar] [CrossRef]
- Joosten, E.A.; Franken, G. Spinal cord stimulation in chronic neuropathic pain: Mechanisms of action, new locations, new paradigms. Pain 2020, 161 (Suppl. 1), S104–S113. [Google Scholar] [CrossRef]
- Deer, T.R.; Pope, J.E.; Lamer, T.J.; Grider, J.S.; Provenzano, D.; Lubenow, T.R.; FitzGerald, J.J.; Hunter, C.; Falowski, S.; Sayed, D.; et al. The Neuromodulation Appropriateness Consensus Committee on Best Practices for Dorsal Root Ganglion Stimulation. Neuromodulation 2019, 22, 1–35. [Google Scholar] [CrossRef]
- Stelter, B.; Karri, J.; Marathe, A.; Abd-Elsayed, A. Dorsal Root Ganglion Stimulation for the Treatment of Non-Complex Regional Pain Syndrome Related Chronic Pain Syndromes: A Systematic Review. Neuromodulation 2021, 24, 622–633. [Google Scholar] [CrossRef]
- Horan, M.; Jacobsen, A.H.; Scherer, C.; Rosenlund, C.; Gulisano, H.A.; Søe, M.; Sørensen, J.C.H.; Meier, K.; Blichfeldt-Eckhardt, M.R. Complications and Effects of Dorsal Root Ganglion Stimulation in the Treatment of Chronic Neuropathic Pain: A Nationwide Cohort Study in Denmark. Neuromodulation 2021, 24, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Sun, Z.; Wu, J.; Rana, M.; Garza, J.; Zhu, A.C.; Chakravarthy, K.V.; Abd-Elsayed, A.; Rosenquist, E.; Basi, H.; et al. Peripheral Nerve Stimulation in Pain Management: A Systematic Review. Pain Physician 2021, 24, E131–E152. [Google Scholar] [PubMed]
- Jandhyala, R. Delphi, non-RAND modified Delphi, RAND/UCLA appropriateness method and a novel group awareness and consensus methodology for consensus measurement: A systematic literature review. Curr. Med. Res. Opin. 2020, 36, 1873–1887. [Google Scholar] [CrossRef]
- Suarez-Alvarez, J.; Pedrosa, I.; Lozano, L.M.; García-Cueto, E.; Cuesta, M.; Muñiz, J. Using reversed items in Likert scales: A questionable practice. Psicothema 2018, 30, 149–158. [Google Scholar] [PubMed]
- Jünger, S.; Payne, S.A.; Brine, J.; Radbruch, L.; Brearly, S.G. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: Recommendations based on a methodological systematic review. Palliat Med. 2017, 31, 684–706. [Google Scholar] [CrossRef] [Green Version]
- Roth, R.S.; Geisser, M.E.; Williams, D.A. Interventional pain medicine: Retreat from the biopsychosocial model of pain. Transl. Behav. Med. 2012, 2, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Hatzakis, M.; Schatman, M.E. The Impact of Interventional Approaches when used Within the Context of Multidisciplinary Chronic Pain Management. In Chronic Pain Management Guidelines for Multidisciplinary Program Development; Schatman, M.E., Campbell, A., Eds.; Informa Healthcare: New York, NY, USA, 2007; pp. 101–116. [Google Scholar]


{kind=link}
{kind=link}
| (A) Botulinum toxins |
|
| (B) Neural blocks and infiltrations |
|
| (C) Radiofrequency |
|
| (D) Neuromodulation |
|
| Participants | First Round | Second Round |
|---|---|---|
| Gender (M/F) | 14/21 | 10/19 |
| Years of experience in NP–mean (s.d.) | 16.37 (8.81) | 15.79 (9.16) |
| Dept Head/Director | 9 | 7 |
| Specialty | ||
| Anesthesiology | 23 | 20 |
| Ph. Med. and Rehabilitation | 9 | 6 |
| Rheumatology | 3 | 3 |
| GP | 1 | 1 |
| Statement | Mean Consensus Degree | Variability Change |
|---|---|---|
| Its use in combination with standard therapy is recommended in refractory patients. * | 3.42/3.62 | 0.19 |
| The evidence on the use of BT in perineural areas is very weak (case series), although we cannot rule out its usefulness based on current publications. Therefore, embarking in rigorous studies to demonstrate the safety and efficacy of this promising new therapeutic modality is warranted. | 3.51/3.72 | 0.12 |
| Ilioinguinal and ilio-hypogastric blocks with local anesthetics and corticosteroids in combination can be effective for the treatment of chronic post herniorrhaphy groin pain | 3.46/3.48 | 0.15 |
| Repeated, long duration therapies should be considered for PHN. $ | 2.74/3.00 | 0.15 |
| Conventional radiofrequency is more effective than PRF for idiopathic trigeminal neuralgia. | 3.09/3.17 | 0.22 |
| Dorsal column stimulation therapy (SCS) is indicated for FBSS and CRPS | 3.60/3.79 | 0.11 |
| High frequency (HF10) is as efficacious as low frequency stimulation for FBSS | 2.71/3.00 | 0.2 |
| DRG stimulation should be considered for radicular pain | 3.37/3.48 | 0.16 |
| DRG stimulation would be indicated for localized NP | 2.86/3.24 | 0.18 |
| Percutaneous electrical nerve stimulation is useful for chronic NP | 2.86/2.97 | 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serrano-Afonso, A.; Gálvez, R.; Paramés, E.; Navarro, A.; Ochoa, D.; Pérez-Hernández, C. Update on Interventional Management of Neuropathic Pain: A Delphi Consensus of the Spanish Pain Society Neuropathic Pain Task Force. Medicina 2022, 58, 627. https://doi.org/10.3390/medicina58050627
Serrano-Afonso A, Gálvez R, Paramés E, Navarro A, Ochoa D, Pérez-Hernández C. Update on Interventional Management of Neuropathic Pain: A Delphi Consensus of the Spanish Pain Society Neuropathic Pain Task Force. Medicina. 2022; 58(5):627. https://doi.org/10.3390/medicina58050627
Chicago/Turabian StyleSerrano-Afonso, Ancor, Rafael Gálvez, Elena Paramés, Ana Navarro, Dolores Ochoa, and Concepción Pérez-Hernández. 2022. "Update on Interventional Management of Neuropathic Pain: A Delphi Consensus of the Spanish Pain Society Neuropathic Pain Task Force" Medicina 58, no. 5: 627. https://doi.org/10.3390/medicina58050627
APA StyleSerrano-Afonso, A., Gálvez, R., Paramés, E., Navarro, A., Ochoa, D., & Pérez-Hernández, C. (2022). Update on Interventional Management of Neuropathic Pain: A Delphi Consensus of the Spanish Pain Society Neuropathic Pain Task Force. Medicina, 58(5), 627. https://doi.org/10.3390/medicina58050627