
Efficiency of Hyaluronic Acid in Infrabony Defects: A Systematic Review of Human Clinical Trials



Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- —
- Participants (P), patients with infrabony defects;
- —
- Intervention (I), open-flap debridement + addition of hyaluronic acid;
- —
- Comparison (C), open-flap debridement alone;
- —
- Outcome (O), regenerative potential of hyaluronic acid in terms of periodontal indices (probing depth, clinical attachment level) with follow-up (12 months);
- —
- Study type (S): split or parallel randomized clinical trials (RCTs), published in the English language.
2.2. Literature Search
2.3. Data Extraction
2.4. Risk of Bias
2.5. Statistical Analysis
3. Results
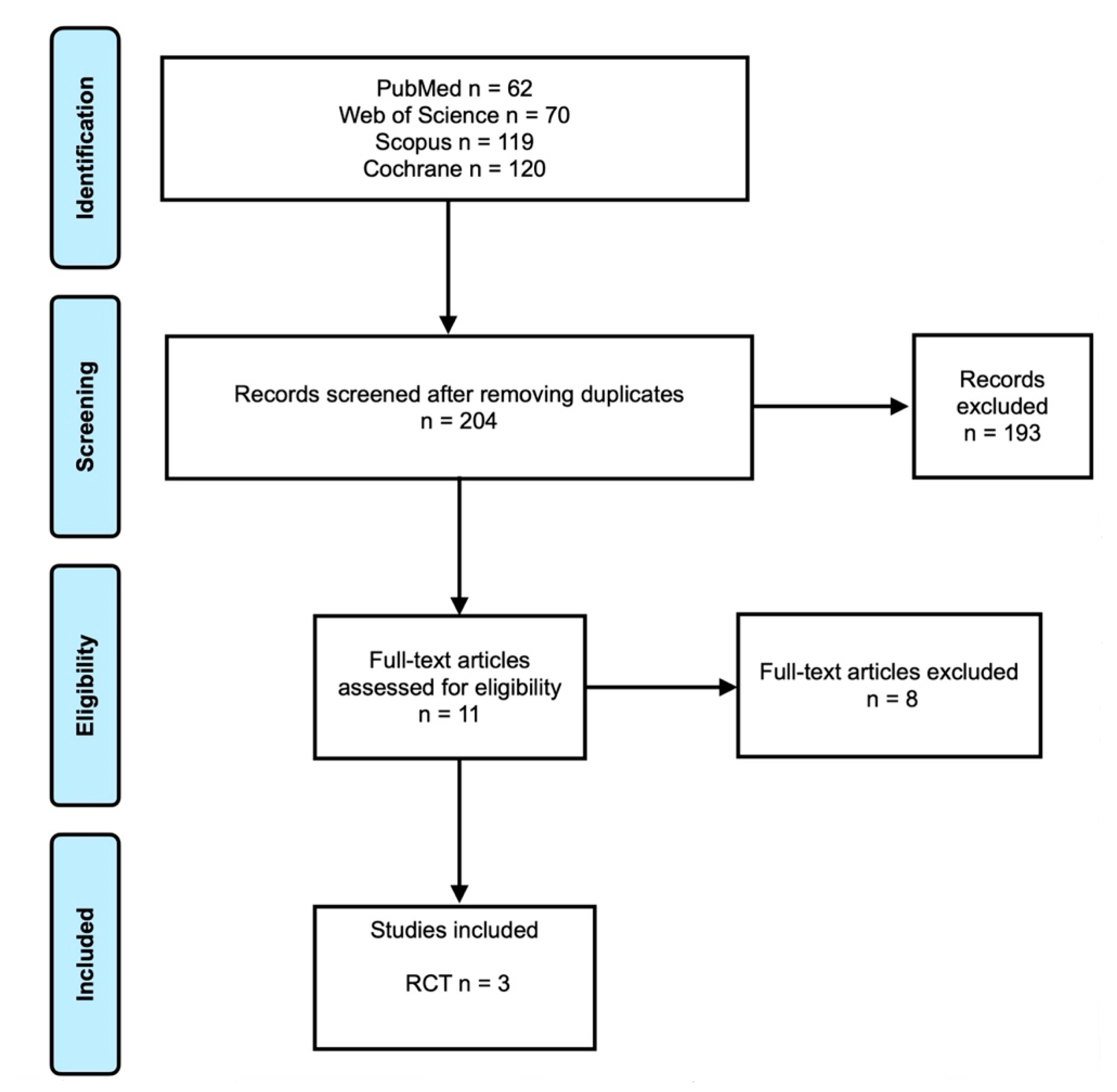
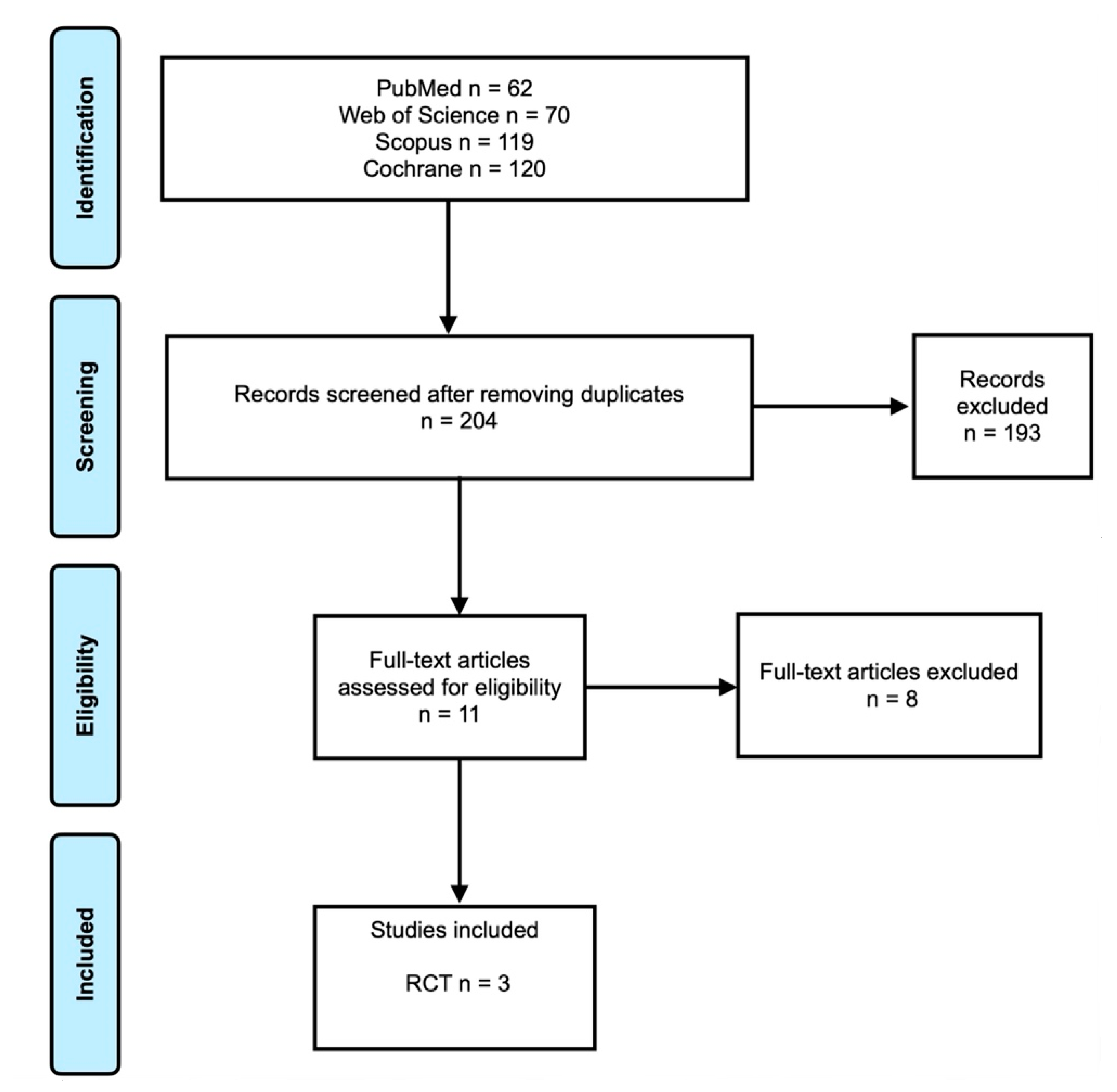
3.1. Search Results
3.2. General Characteristics
3.3. Treatment of Infrabony Defects for Test and Control Groups
3.4. Periodontal Parameter Assessment
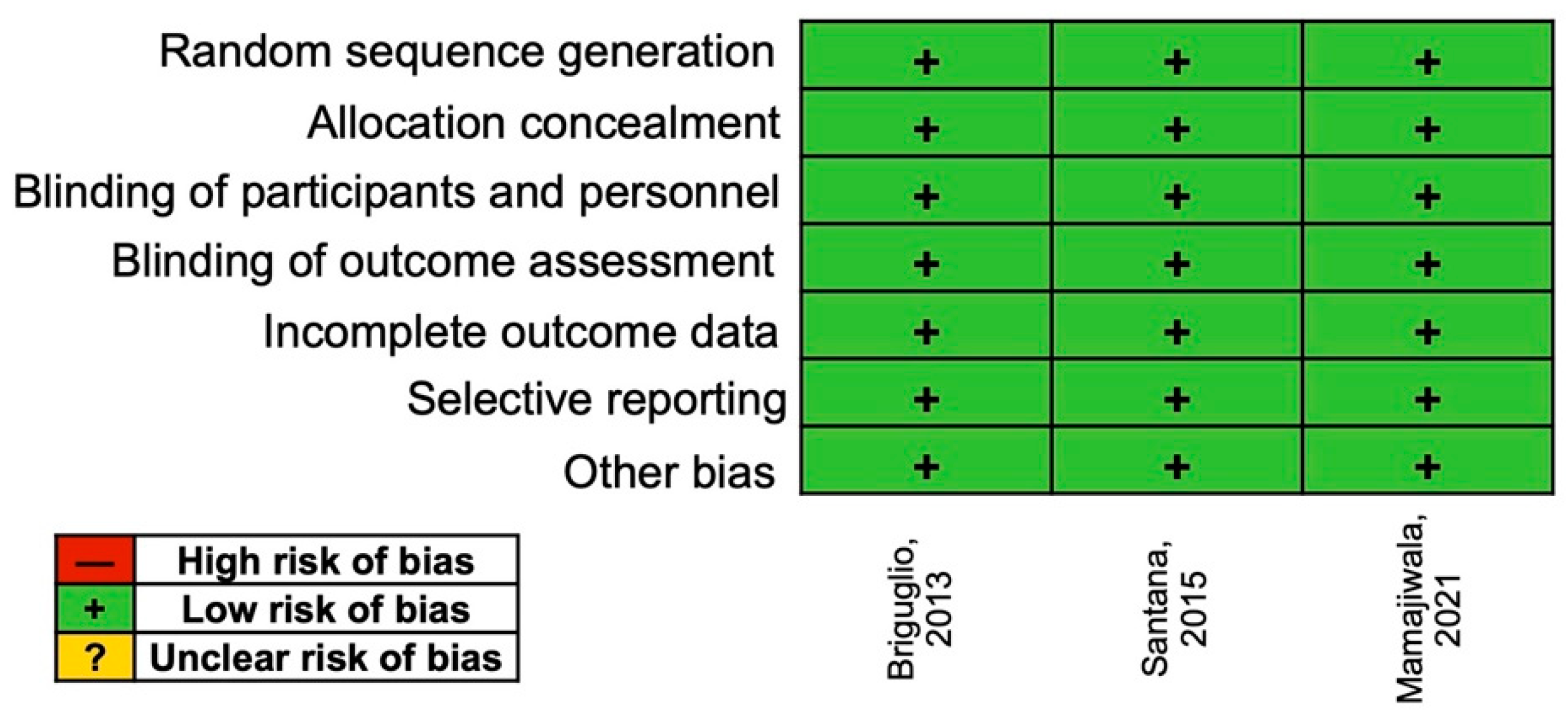
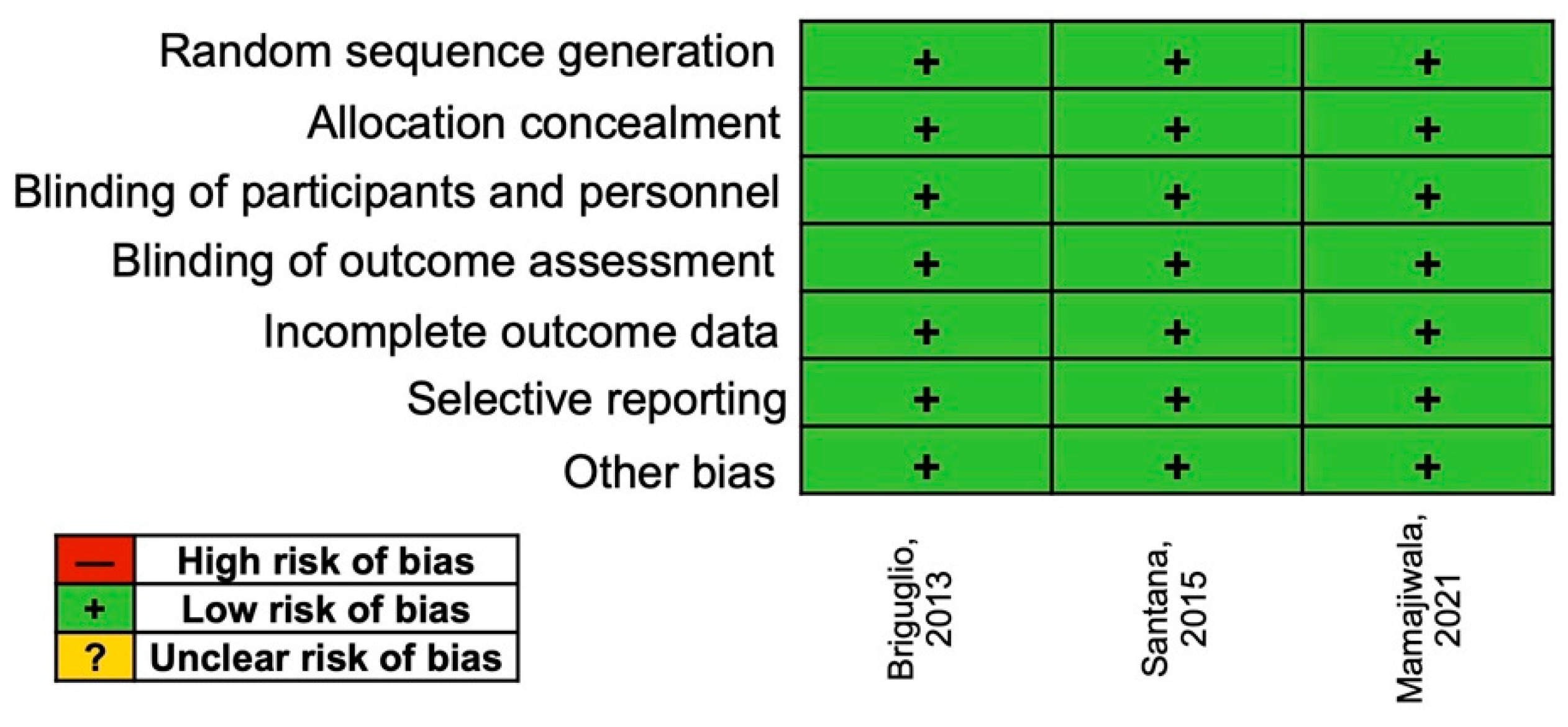
3.5. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Casale, M.; Moffa, A.; Vella, P.; Sabatino, L.; Capuano, F.; Salvinelli, B.; Lopez, M.A.; Carinci, F.; Salvinelli, F. Hyaluronic acid: Perspectives in dentistry. A systematic review. Int. J. Immunopathol. Pharmacol. 2016, 29, 572–582. [Google Scholar] [CrossRef] [PubMed]
- Kopchak, O.V.; Marchenko, N.S.; Kaniura, O.A.; Savosko, S.I.; Yanishevsky, K.A.; Makarenko, O.M.; Doroshenko, O.M.; Asharenkova, O.V. The Effect of Hyaluronic Acid on the Periodontium in Spontaneous Periodontitis in Rats. Int. J. Morphol. 2021, 39, 1028–1035. [Google Scholar] [CrossRef]
- Nibali, L.; Sultan, D.; Arena, C.; Pelekos, G.; Lin, G.H.; Tonetti, M. Periodontal infrabony defects: Systematic review of healing by defect morphology following regenerative surgery. J. Clin. Periodontol. 2021, 48, 101–114. [Google Scholar] [CrossRef] [PubMed]
- Petsos, H.; Ratka-Krüger, P.; Neukranz, E.; Raetzke, P.; Eickholz, P.; Nickles, K. Infrabony defects 20 years after open flap debridement and guided tissue regeneration. J. Clin. Periodontol. 2019, 46, 552–563. [Google Scholar] [CrossRef]
- Chitsazi, M.T.; Shirmohammadi, A.; Faramarzie, M.; Pourabbas, R.; Rostamzadeh, A.N. A clinical comparison of nano-crystalline hydroxyapatite (Ostim) and autogenous bone graft in the treatment of periodontal intrabony defects. Med. Oral. Patol. Oral. Cir. Bucal. 2011, 16, e448–e453. [Google Scholar] [CrossRef]
- Dahiya, P.; Kamal, R. Hyaluronic acid: A boon in periodontal therapy. N. Am. J. Med. Sci. 2013, 5, 309–315. [Google Scholar] [CrossRef]
- Eliezer, M.; Imber, J.C.; Sculean, A.; Pandis, N.; Teich, S. Hyaluronic acid as adjunctive to non-surgical and surgical periodontal therapy: A systematic review and meta-analysis. Clin. Oral. Investig. 2019, 23, 3423–3435. [Google Scholar] [CrossRef]
- Sukumar, S.; Drizhal, I. Hyaluronic acid and periodontitis. Acta. Medica (Hradec Kralove) 2007, 50, 225–228. [Google Scholar] [CrossRef] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Pilloni, A.; Rojas, M.A.; Marini, L.; Russo, P.; Shirakata, Y.; Sculean, A.; Iacono, R. Healing of intrabony defects following regenerative surgery by means of single-flap approach in conjunction with either hyaluronic acid or an enamel matrix derivative: A 24-month randomized controlled clinical trial. Clin. Oral. Investig. 2021, 25, 5095–5107. [Google Scholar] [CrossRef] [PubMed]
- Ballini, A.; Cantore, S.; Capodiferro, S.; Grassi, F.R. Esterified hyaluronic acid and autologous bone in the surgical correction of the infra-bone defects. Int. J. Med. Sci. 2009, 6, 65–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanden Bogaerde, L. Treatment of infrabony periodontal defects with esterified hyaluronic acid: Clinical report of 19 consecutive lesions. Int. J. Periodontics. Restorative Dent. 2009, 29, 315–323. [Google Scholar] [PubMed]
- Božić, D.; Ćatović, I.; Badovinac, A.; Musić, L.; Par, M.; Sculean, A. Treatment of Intrabony Defects with a Combination of Hyaluronic Acid and Deproteinized Porcine Bone Mineral. Materials 2021, 14, 6795. [Google Scholar] [CrossRef]
- Bhowmik, E.; Rao, D.P.C. Clinicoradiographic evaluation of hyaluronan-nano hydroxyapatite composite graft in the management of periodontal infrabony defects. J. Indian Soc. Periodontol. 2021, 25, 220–227. [Google Scholar] [CrossRef]
- Engström, P.E.; Shi, X.Q.; Tronje, G.; Larsson, A.; Welander, U.; Frithiof, L.; Engstrom, G.N. The effect of hyaluronan on bone and soft tissue and immune response in wound healing. J. Periodontol. 2001, 72, 1192–1200. [Google Scholar] [CrossRef]
- Sehdev, B.; Bhongade, M.L.; Ganji, K.K. Evaluation of effectiveness of hyaluronic acid in combination with bioresorbable membrane (poly lactic acid-poly glycolic acid) for the treatment of infrabony defects in humans: A clinical and radiographic study. J. Indian Soc. Periodontol. 2016, 20, 50–56. [Google Scholar] [CrossRef]
- Fawzy El-Sayed, K.M.; Dahaba, M.A.; Aboul-Ela, S.; Darhous, M.S. Local application of hyaluronan gel in conjunction with periodontal surgery: A randomized controlled trial. Clin. Oral. Investig. 2012, 16, 1229–1236. [Google Scholar] [CrossRef]
- Briguglio, F.; Briguglio, E.; Briguglio, R.; Cafiero, C.; Isola, G. Treatment of infrabony periodontal defects using a resorbable biopolymer of hyaluronic acid: A randomized clinical trial. Quintessence Int. 2013, 44, 231–240. [Google Scholar]
- De Santana, R.B.; de Santana, C.M. Human intrabony defect regeneration with rhFGF-2 and hyaluronic acid—A randomized controlled clinical trial. J. Clin. Periodontol. 2015, 42, 658–665. [Google Scholar] [CrossRef]
- Mamajiwala, A.S.; Sethi, K.S.; Raut, C.P.; Karde, P.A.; Mamajiwala, B.S. Clinical and radiographic evaluation of 0.8% hyaluronic acid as an adjunct to open flap debridement in the treatment of periodontal intrabony defects: Randomized controlled clinical trial. Clin. Oral. Investig. 2021, 25, 5257–5271. [Google Scholar] [CrossRef] [PubMed]
- Bansal, J.; Kedige, S.D.; Anand, S. Hyaluronic acid: A promising mediator for periodontal regeneration. Indian J. Dent. Res. 2010, 21, 575–578. [Google Scholar]
- King, S.R.; Hickerson, W.L.; Proctor, K.G. Beneficial actions of exogenous hyaluronic acid on wound healing. Surgery 1991, 109, 76–84. [Google Scholar]
- Monheit, G.D.; Coleman, K.M. Hyaluronic acid fillers. Dermatol. Ther. 2006, 19, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Fujioka-Kobayashi, M.; Müller, H.D.; Mueller, A.; Lussi, A.; Sculean, A.; Schmidlin, P.R.; Miron, R.J. In Vitro effects of hyaluronic acid on human periodontal ligament cells. BMC Oral Health 2017, 17, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, D.G.; Malmonge, S.M.; Campos, D.M.; Attik, N.G.; Grosgogeat, B.; Gritsch, K. A chitosan-hyaluronic acid hydrogel scaffold for periodontal tissue engineering. J. Biomed. Mater. Res. B Appl. Biomater. 2016, 104, 1691–1702. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Grusovin, M.G.; Papanikolaou, N.; Coulthard, P.; Worthington, H.V. Enamel matrix derivative (Emdogain®) for periodontal tissue regeneration in intrabony defects. Cochrane Database Syst. Rev. 2009, 2009, CD003875. [Google Scholar] [CrossRef] [Green Version]
- Ramenzoni, L.L.; Annasohn, L.; Miron, R.J.; Attin, T.; Schmidlin, P.R. Combination of enamel matrix derivative and hyaluronic acid inhibits lipopolysaccharide-induced inflammatory response on human epithelial and bone cells. Clin. Oral. Investig. 2022, 26, 1773–1783. [Google Scholar] [CrossRef]
- Shue, L.; Yufeng, Z.; Mony, U. Biomaterials for periodontal regeneration: A review of ceramics and polymers. Biomatter 2012, 2, 271–277. [Google Scholar] [CrossRef] [Green Version]
- Onisor, F.; Bran, S.; Mitre, I.; Mester, A.; Voina-Tonea, A.; Armencea, G.; Baciut, M. Polymer-Based Bone Substitutes in Periodontal Infrabony Defects: A Systematic Evaluation of Clinical Studies. Polymers 2021, 13, 4445. [Google Scholar] [CrossRef]
- Onicas, M.I.; Narita, L.E.; Mester, A.; Onisor, F.; Mancini, L. Platelet-Rich Fibrin: A Viable Therapy for Endodontic-Periodontal Lesions? A Preliminary Assessment. Appl. Sci. 2021, 11, 7081. [Google Scholar] [CrossRef]
- Chang, Y.C.; Zhao, J.H. Effects of platelet-rich fibrin on human periodontal ligament fibroblasts and application for periodontal infrabony defects. Aust. Dent. J. 2011, 56, 365–371. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article | Reason for Exclusion |
|---|---|
| Pilloni [11] | RCT—comparison between EMD and HA with no control group |
| Ballini [12] | Prospective study with no control group |
| Bogaerde [13] | Prospective study with no control group |
| Bozic [14] | Prospective study—use of HA and deproteinized porcine bone with no control group |
| Bhowmik [15] | Prospective study with no control group |
| Engstrom [16] | Prospective study using guided tissue regeneration procedure |
| Sehdev [17] | Prospective study using guided tissue regeneration procedure |
| Fawzy El-Sayed [18] | RCT with follow-up of less than 12 months. |
| Author, Year, Country | Study | Patients | Surgical Intervention | Results | Conclusions | |
|---|---|---|---|---|---|---|
| Briguglio, 2013, Italy [19] | Parallel RCT | 40 patients Male: 18 Female: 22 Mean age: 45 ± 8.2 years | Open-flap debridement | Baseline | Follow-up (12 months/24 months) | HA with OFD offered additional benefits in terms of PD reduction and CAL gain. |
| PD: Control 8.0 ± 0.7 mm | PD: Control 7.1 ± 1.3 mm 7.2 ± 0.5 mm | |||||
| Test 8.6 ± 1.1 mm | Test 7.4 ± 0.6 mm 7.0 ± 1.2 mm | |||||
| CAL: Control 8.3 ± 1.2 mm | CAL: Control 6.9 ± 1.8 mm 7.2 ± 0.7 mm | |||||
| Test: 7.2 ± 1.5 mm | Test: 6.5 ± 0.9 mm 5.3 ± 1.8 mm | |||||
| Santana, 2015, Brazil [20] | Split-mouth RCT | 30 patients Male: 11 Female: 19 Mean age: 49.2 years Control group (n = 30 sites) Test group (n = 30 sites) | Open debridement with the papilla preservation flap | Baseline | Follow-up (1 year) | rhFGF-2/HA was able to improve periodontal parameters. |
| PD: Control 9.5 ± 1.5 mm | PD: Control 6.6 ± 1.3 mm | |||||
| Test 9.7 ± 1.9 mm | Test 4.2 ± 0.8 mm | |||||
| CAL: Control 10.3 ± 1.3 mm | CAL: Control 8.0 ± 1.9 mm | |||||
| Test: 10.4 ± 1.6 mm | Test: 5.7 ± 1.4 mm | |||||
| Mamajiwala, 2021, India [21] | Split-mouth RCT | 20 patients Male: 11 Female: 9 Mean age: 39.9 ± 4.18 years Control group (n = 20 sites) Test group (n = 20 sites) | Open-flap debridement | Baseline | Follow-up (6 months/12 months) | HA in addition to OFD improved clinical and radiographic outcomes. |
| PD: Control 8.45 ± 0.51 mm | PD: Control 5.2 ± 0.61 mm 4.3 ± 0.47 mm | |||||
| Test 8.5 ± 0.94 mm | Test 4.5 ± 0.51 mm 3.1 ± 0.58 mm | |||||
| CAL: Control 9.3 ± 0.73 mm | CAL: Control 6.8 ± 0.76 mm 5.4 ± 0.82 mm | |||||
| Test: 9.15 ± 0.48 mm | Test: 5.6 ± 0.74 mm 4.0 ± 0.56 mm | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onisor, F.; Bran, S.; Mester, A.; Voina-Tonea, A. Efficiency of Hyaluronic Acid in Infrabony Defects: A Systematic Review of Human Clinical Trials. Medicina 2022, 58, 580. https://doi.org/10.3390/medicina58050580
Onisor F, Bran S, Mester A, Voina-Tonea A. Efficiency of Hyaluronic Acid in Infrabony Defects: A Systematic Review of Human Clinical Trials. Medicina. 2022; 58(5):580. https://doi.org/10.3390/medicina58050580
Chicago/Turabian StyleOnisor, Florin, Simion Bran, Alexandru Mester, and Andrada Voina-Tonea. 2022. "Efficiency of Hyaluronic Acid in Infrabony Defects: A Systematic Review of Human Clinical Trials" Medicina 58, no. 5: 580. https://doi.org/10.3390/medicina58050580
APA StyleOnisor, F., Bran, S., Mester, A., & Voina-Tonea, A. (2022). Efficiency of Hyaluronic Acid in Infrabony Defects: A Systematic Review of Human Clinical Trials. Medicina, 58(5), 580. https://doi.org/10.3390/medicina58050580