
Update of Robotic Surgery in Benign Gynecological Pathology: Systematic Review

 , ,
, ,
Abstract
:1. Introduction
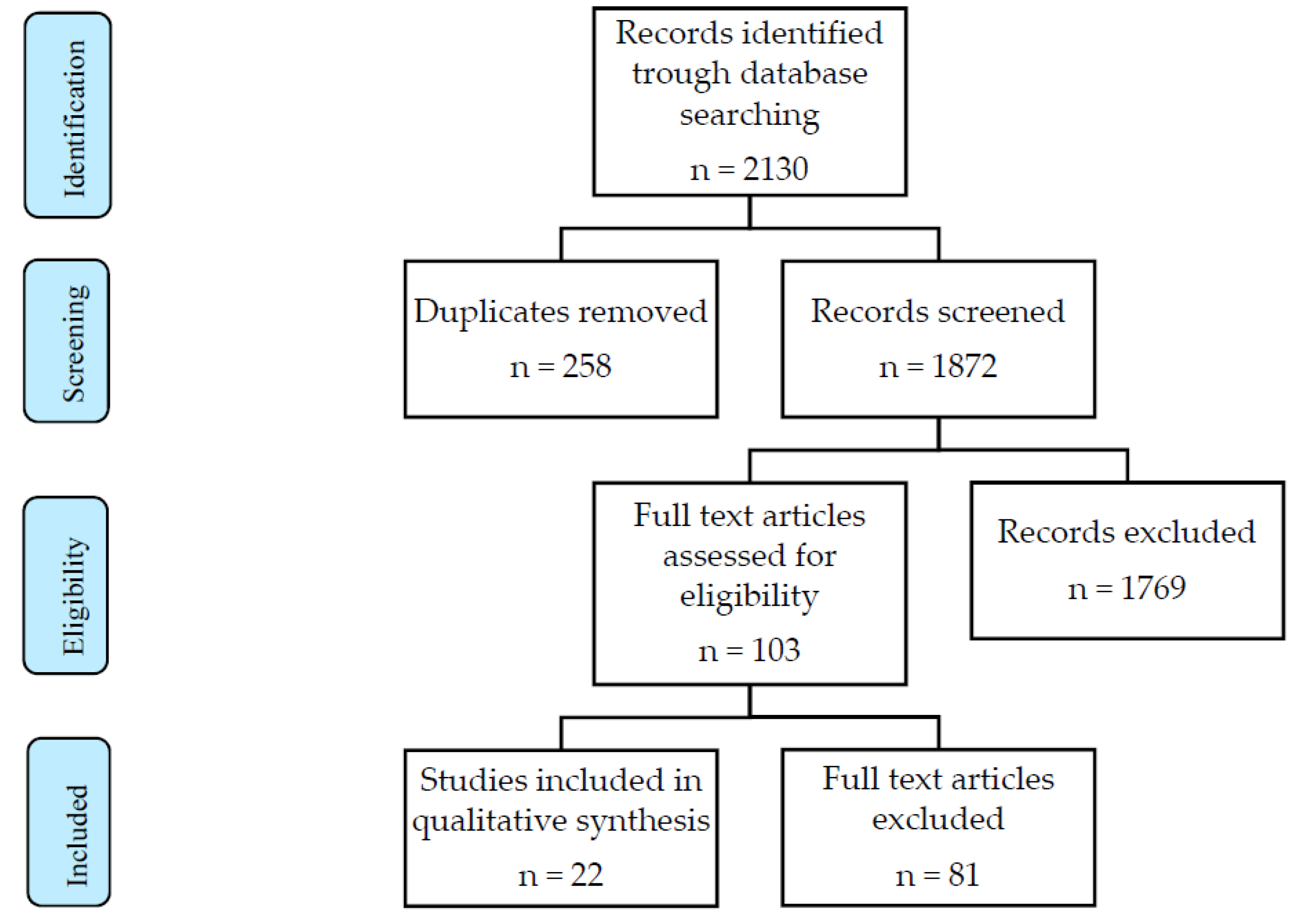
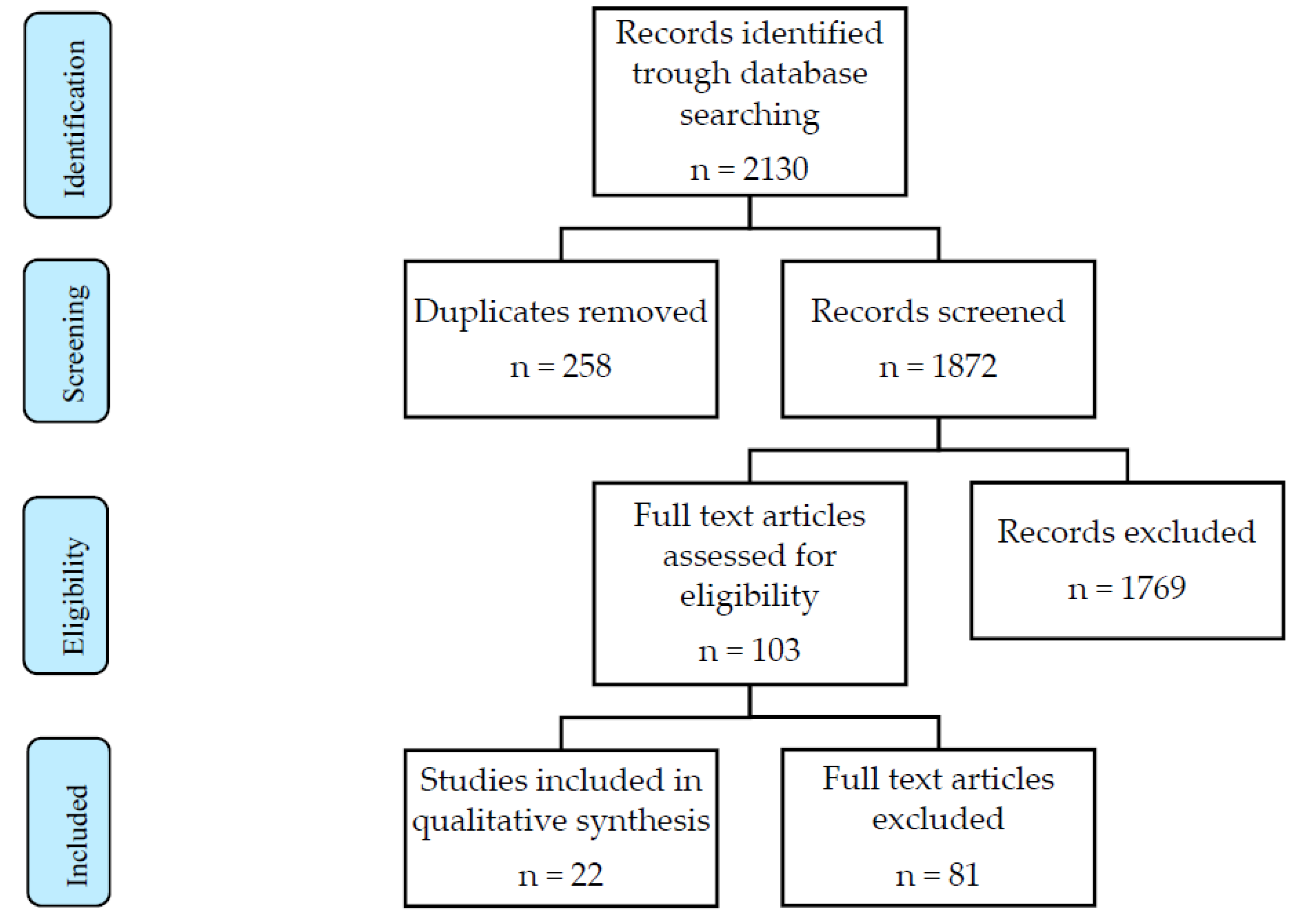
2. Materials and Methods
3. Results
3.1. Robotic Myomectomy
3.2. Robotic Hysterectomy
3.3. Robotic Endometriosis Treatment
3.4. Robotic Pelvic Organ Prolapse Treatment
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alletti, S.G.; Vizzielli, G.; Lafuenti, L.; Costantini, B.; Fagotti, A.; Fedele, C.; Cianci, S.; Perrone, E.; Gallotta, V.; Rossitto, C.; et al. Single-Institution Propensity-Matched Study to Evaluate the Psychological Effect of Minimally Invasive Interval Debulking Surgery Versus Standard Laparotomic Treatment: From Body to Mind and Back. J. Minim. Invasive Gynecol. 2018, 25, 816–822. [Google Scholar] [CrossRef] [PubMed]
- Bellia, A.; Vitale, S.G.; Laganà, A.S.; Cannone, F.; Houvenaeghel, G.; Rua, S.; Ladaique, A.; Jauffret, C.; Ettore, G.; Lambaudie, E. Feasibility and surgical outcomes of conventional and robot-assisted laparoscopy for early-stage ovarian cancer: A retrospective, multicenter analysis. Arch. Gynecol. Obstet. 2016, 294, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Cianci, S.; Rosati, A.; Rumolo, V.; Gueli Alletti, S.; Gallotta, V.; Turco, L.C.; Corrado, G.; Vizzielli, G.; Fagotti, A.; Fanfani, F.; et al. Robotic Single-Port Platform in General, Urologic, and Gynecologic Surgeries: A Systematic Review of the Literature and Meta-analysis. World J. Surg. 2019, 43, 2401–2419. [Google Scholar] [CrossRef] [PubMed]
- Gala, R.B.; Margulies, R.; Steinberg, A.; Murphy, M.; Lukban, J.; Jeppson, P.; Aschkenazi, S.; Olivera, C.; South, M.; Lowenstein; et al. Systematic review of robotic surgery in gynecology: Robotic techniques compared with laparoscopy and laparotomy. J. Minim. Invasive Gynecol. 2014, 21, 353–361. [Google Scholar] [CrossRef]
- Nelson, G.; Bakkum-Gamez, J.; Kalogera, E.; Glaser, G.; Altman, A.; Meyer, L.A.; Taylor, J.S.; Iniesta, M.; Lasala, J.; Mena, G.; et al. Guidelines for perioperative care in gynecologic/oncology: Enhanced Recovery After Surgery (ERAS) Society recommendations-2019 update. Int. J. Gynecol. Cancer 2019, 29, 651–668. [Google Scholar] [CrossRef]
- Alletti, S.G.; Perrone, E.; Fedele, C.; Cianci, S.; Pasciuto, T.; Chiantera, V.; Uccella, S.; Ercoli, A.; Vizzielli, G.; Fagotti, A.; et al. A Multicentric Randomized Trial to Evaluate the ROle of Uterine MANipulator on Laparoscopic/Robotic HYsterectomy for the Treatment of Early-Stage Endometrial Cancer: The Romanhy Trial. Front. Oncol. 2021, 11, 720894. [Google Scholar] [CrossRef]
- Cianci, S.; Arcieri, M.; Vizzielli, G.; Martinelli, C.; Granese, R.; La Verde, M.; Fagotti, A.; Fanfani, F.; Scambia, G.; Ercoli, A. Robotic Pelvic Exenteration for Gynecologic Malignancies, Anatomic Landmarks, and Surgical Steps: A Systematic Review. Front. Surg. 2021, 8, 790152. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Advincula, A.P.; Xu, X.; Goudeau, S., 4th; Ransom, S.B. Robot-assisted laparoscopic myomectomy versus abdominal myomectomy: A comparison of short-term surgical outcomes and immediate costs. J. Minim. Invasive Gynecol. 2007, 14, 698–705. [Google Scholar] [CrossRef]
- Bedient, C.E.; Magrina, J.F.; Noble, B.N.; Kho, R.M. Comparison of robotic and laparoscopic myomectomy. Am. J. Obstet Gynecol. 2009, 201, 566.e1–566.e5665. [Google Scholar] [CrossRef]
- Nezhat, C.; Lavie, O.; Hsu, S.; Watson, J.; Barnett, O.; Lemyre, M. Robotic-assisted laparoscopic myomectomy compared with standard laparoscopic myomectomy—A retrospective matched control study. Fertil. Steril. 2009, 91, 556–559. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, A.R.; Srouji, S.S.; Missmer, S.A.; Correia, K.F.; Vellinga, T.T.; Einarsson, J.I. Robot-assisted laparoscopic myomectomy compared with standard laparoscopic myomectomy. Obstet. Gynecol. 2012, 120 Pt 1, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Barakat, E.E.; Bedaiwy, M.A.; Zimberg, S.; Nutter, B.; Nosseir, M.; Falcone, T. Robotic-assisted, laparoscopic, and abdominal myomectomy: A comparison of surgical outcomes. Obstet. Gynecol. 2011, 117 Pt 1, 256–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gobern, J.M.; Rosemeyer, C.J.; Barter, J.F.; Steren, A.J. Comparison of robotic, laparoscopic, and abdominal myomectomy in a community hospital. JSLS J. Soc. Laparoendosc. Surg. 2013, 17, 116–120. [Google Scholar] [CrossRef] [Green Version]
- Flyckt, R.; Soto, E.; Nutter, B.; Falcone, T. Comparison of Long-Term Fertility and Bleeding Outcomes after Robotic-Assisted, Laparoscopic, and Abdominal Myomectomy. Obstet. Gynecol. Int. 2016, 2016, 2789201. [Google Scholar] [CrossRef] [Green Version]
- Özbaşlı, E.; Güngör, M. Comparison of perioperative outcomes among robot-assisted, conventional laparoscopic, and abdominal/open myomectomies. J. Turk. Ger. Gynecol. Assoc. 2021, 22, 312–318. [Google Scholar] [CrossRef]
- Wright, J.D.; Ananth, C.V.; Lewin, S.N.; Burke, W.M.; Lu, Y.S.; Neugut, A.I.; Herzog, T.J.; Hershman, D.L. Robotically assisted vs laparoscopic hysterectomy among women with benign gynecologic disease. JAMA 2013, 309, 689–698. [Google Scholar] [CrossRef]
- Paraiso, M.F.R.; Ridgeway, B.; Park, A.J.; Park, A.J.; Jelovsek, J.E.; Barber, M.D.; Falcone, T.; Einarsson, J.I. A randomized trial comparing conventional and robotically assisted total laparoscopic hysterectomy. Am. J. Obstet Gynecol. 2013, 208, 368.e1–368.e3687. [Google Scholar] [CrossRef]
- Sarlos, D.; Kots, L.; Stevanovic, N.; von Felten, S.; Schär, G. Robotic compared with conventional laparoscopic hysterectomy: A randomized controlled trial. Obstet. Gynecol. 2012, 120, 604–611. [Google Scholar] [CrossRef]
- Lönnerfors, C.; Reynisson, P.; Persson, J. A randomized trial comparing vaginal and laparoscopic hysterectomy vs robot-assisted hysterectomy. J. Minim. Invasive Gynecol. 2015, 22, 78–86. [Google Scholar] [CrossRef]
- Deimling, T.A.; Eldridge, J.L.; Riley, K.A.; Kunselman, A.R.; Harkins, G.J. Randomized controlled trial comparing operative times between standard and robot-assisted laparoscopic hysterectomy. Int. J. Gynaecol. Obstet. 2017, 136, 64–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soto, E.; Luu, T.H.; Liu, X.; Magrina, J.F.; Wasson, M.N.; Einarsson, J.I.; Cohen, S.L.; Falcone, T. Laparoscopy vs. Robotic Surgery for Endometriosis (LAROSE): A multicenter, randomized, controlled trial. Fertil. Steril. 2017, 107, 996–1002.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DuBeshter, B.; Angel, C.; Toy, E.; Thomas, S.; Glantz, J.C. Current Role of Robotic Hysterectomy. J. Gynecol. Surg. 2013, 29, 174–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magrina, J.F.; Espada, M.; Kho, R.M.; Cetta, R.; Chang, Y.H.; Magtibay, P.M. Surgical Excision of Advanced Endometriosis: Perioperative Outcomes and Impacting Factors. J. Minim. Invasive Gynecol. 2015, 22, 944–950. [Google Scholar] [CrossRef] [PubMed]
- Nezhat, F.R.; Sirota, I. Perioperative outcomes of robotic assisted laparoscopic surgery versus conventional laparoscopy surgery for advanced-stage endometriosis. JSLS J. Soc. Laparoendosc. Surg. 2014, 18, e2014.00094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nezhat, C.R.; Stevens, A.; Balassiano, E.; Soliemannjad, R. Robotic-assisted laparoscopy vs conventional laparoscopy for the treatment of advanced stage endometriosis. J. Minim. Invasive Gynecol. 2015, 22, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Paraiso, M.F.R.; Jelovsek, J.E.; Frick, A.; Chen, C.C.G.; Barber, M.D. Laparoscopic compared with robotic sacrocolpopexy for vaginal prolapse: A randomized controlled trial. Obstet. Gynecol. 2011, 118, 1005–1013. [Google Scholar] [CrossRef]
- Anger, J.T.; Mueller, E.R.; Tarnay, C.; Smith, B.; Stroupe, K.; Rosenman, A.; Brubaker, L.; Bresee, C.; Kenton, K. Robotic compared with laparoscopic sacrocolpopexy: A randomized controlled trial. Obstet. Gynecol. 2014, 123, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Illiano, E.; Ditonno, P.; Giannitsas, K.; De Rienzo, G.; Bini, V.; Costantini, E. Robot-assisted Vs. Laparoscopic Sacrocolpopexy for High-stage Pelvic Organ Prolapse: A Prospective, Randomized, Single-center Study. Urology 2019, 134, 116–123. [Google Scholar] [CrossRef]
- Nosti, P.A.; Umoh, A.U.; Kane, S.; White, D.E.; Harvie, H.S.; Lowenstein, L.; Gutman, R.E. Outcomes of abdominal and minimally invasive sacrocolpopexy: A retrospective cohort study. Female Pelvic. Med. Reconstr. Surg. 2014, 20, 33–37. [Google Scholar] [CrossRef]
- Kim, S.; Luu, T.H.; Llarena, N.; Falcone, T. Role of robotic surgery in treating fibroids and benign uterine mass. Best Pract. Res. Clin. Obstet. Gynaecol. 2017, 45, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Munro, M.G.; Critchley, H.O.; Broder, M.S.; Fraser, I.S.; FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int. J. Gynaecol. Obstet. 2011, 113, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Seracchioli, R.; Rossi, S.; Govoni, F.; Rossi, E.; Venturoli, S.; Bulletti, C.; Flamigni, C. Fertility and obstetric outcome after laparoscopic myomectomy of large myomata: A randomized comparison with abdominal myomectomy. Hum. Reprod. 2000, 15, 2663–2668. [Google Scholar] [CrossRef] [PubMed]
- Sizzi, O.; Rossetti, A.; Malzoni, M.; Minelli, L.; La Grotta, F.; Soranna, L.; Panunzi, S.; Spagnolo, R.; Imperato, F.; Landi, S.; et al. Italian multicenter study on complications of laparoscopic myomectomy. J. Minim. Invasive Gynecol. 2007, 14, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, H.R.; McCaffrey, C.; Amjad, H.; Kives, S. Fertility and Pregnancy Outcomes After Robotic-assisted Laparoscopic Myomectomy in a Canadian Cohort. J. Minim. Invasive Gynecol. 2022, 29, 72–76. [Google Scholar] [CrossRef]
- Albright, B.B.; Witte, T.; Tofte, A.N.; Chou, J.; Black, J.D.; Desai, V.; Erekson, E.A. Robotic Versus Laparoscopic Hysterectomy for Benign Disease: A Systematic Review and Meta-Analysis of Randomized Trials. J. Minim. Invasive Gynecol. 2016, 23, 18–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alletti, S.G.; Rossitto, C.; Cianci, S.; Perrone, E.; Pizzacalla, S.; Monterossi, G.; Vizzielli, G.; Gidaro, S.; Scambia, G. The Senhance™ surgical robotic system (“Senhance”) for total hysterectomy in obese patients: A pilot study. J. Robot. Surg. 2018, 12, 229–234. [Google Scholar] [CrossRef]
- Geppert, B.; Lönnerfors, C.; Persson, J. Robot-assisted laparoscopic hysterectomy in obese and morbidly obese women: Surgical technique and comparison with open surgery. Acta Obstet. Gynecol. Scand. 2011, 90, 1210–1217. [Google Scholar] [CrossRef]
- ACOG Committee. ACOG Committee Opinion No.444: Choosing the route of hysterectomy for benign disease. Obstet. Gynecol. 2009, 114, 1156–1158. [Google Scholar] [CrossRef]
- Uccella, S.; Capozzi, V.A.; Ricco’, M.; Perrone, E.; Zanello, M.; Ferrari, S.; Zorzato, P.C.; Seracchioli, R.; Cromi, A.; Serati, M.; et al. Sexual Function following Laparoscopic versus Transvaginal Closure of the Vaginal Vault after Laparoscopic Hysterectomy: Secondary Analysis of a Randomized Trial by the Italian Society of Gynecological Endoscopy Using a Validated Questionnaire. J. Minim. Invasive Gynecol. 2020, 27, 186–194. [Google Scholar] [CrossRef]
- Alletti, S.G.; Perrone, E.; Cretì, A.; Cianci, S.; Uccella, S.; Fedele, C.; Fanfani, F.; Palmieri, S.; Fagotti, A.; Scambia, G.; et al. Feasibility and perioperative outcomes of percutaneous-assisted laparoscopic hysterectomy: A multicentric Italian experience. Eur. J. Obstet. Gynecol. Reprod Biol. 2020, 245, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Cianci, S.; Perrone, E.; Rossitto, C.; Fanfani, F.; Tropea, A.; Biondi, A.; Scambia, G.; Gueli Alletti, S. Percutaneous-assisted vs mini-laparoscopic hysterectomy: Comparison of ultra-minimally invasive approaches. Updates Surg. 2021, 73, 2347–2354. [Google Scholar] [CrossRef] [PubMed]
- Alletti, S.G.; Perrone, E.; Cianci, S.; Rossitto, C.; Monterossi, G.; Bernardini, F.; Scambia, G. 3 mm Senhance robotic hysterectomy: A step towards future perspectives. J. Robot. Surg. 2018, 12, 575–577. [Google Scholar] [CrossRef] [PubMed]
- Aarts, J.W.; Nieboer, T.E.; Johnson, N.; Tavender, E.; Garry, R.; Mol, B.W.; Kluivers, K.B. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst. Rev. 2015, 2015, CD003677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laganà, A.S.; Garzon, S.; Raffaelli, R.; Gullo, G.; Franchi, M. Robotic Surgery in Female-To-Male Transition: A Possible Way for Further Improvement. J. Investig. Surg. 2021, 34, 651–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nawfal, A.K.; Orady, M.; Eisenstein, D.; Wegienka, G. Effect of body mass index on robotic-assisted total laparoscopic hysterectomy. J. Minim. Invasive Gynecol. 2011, 18, 328–332. [Google Scholar] [CrossRef]
- Cosentino, F.; Vizzielli, G.; Turco, L.C.; Fagotti, A.; Cianci, S.; Vargiu, V.; Zannoni, G.F.; Ferrandina, G.; Scambia, G. Near-Infrared Imaging with Indocyanine Green for Detection of Endometriosis Lesions (Gre-Endo Trial): A Pilot Study. J. Minim. Invasive Gynecol. 2018, 25, 1249–1254. [Google Scholar] [CrossRef]
- Daraï, E.; Dubernard, G.; Coutant, C.; Frey, C.; Rouzier, R.; Ballester, M. Randomized trial of laparoscopically assisted versus open colorectal resection for endometriosis: Morbidity, symptoms, quality of life, and fertility. Ann. Surg. 2010, 251, 1018–1023. [Google Scholar] [CrossRef]
- de Paula Andres, M.; Borrelli, G.M.; Kho, R.M.; Abrão, M.S. The current management of deep endometriosis: A systematic review. Minerva Ginecol. 2017, 69, 587–596. [Google Scholar] [CrossRef]
- ACOG Committee; Pelvic Organ Prolapse: ACOG Practice Bulletin, Number 214. Obstet. Gynecol. 2019, 134, e126–e142. [CrossRef]
- Maher, C.; Baessler, K.; Glazener, C.M.; Adams, E.J.; Hagen, S. Surgical management of pelvic organ prolapse in women. Cochrane Database Syst. Rev. 2004, 4, CD004014. [Google Scholar] [CrossRef] [Green Version]
- Freeman, R.M.; Pantazis, K.; Thomson, A.; Frappell, J.; Bombieri, L.; Moran, P.; Slack, M.; Scott, P.; Waterfield, M. A randomised controlled trial of abdominal versus laparoscopic sacrocolpopexy for the treatment of post-hysterectomy vaginal vault prolapse: LAS study. Int. Urogynecol. J. 2013, 24, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Akl, M.N.; Long, J.B.; Giles, D.L.; Cornella, J.L.; Pettit, P.D.; Chen, A.H.; Magtibay, P.M. Robotic-assisted sacrocolpopexy: Technique and learning curve. Surg. Endosc. 2009, 23, 2390–2394. [Google Scholar] [CrossRef] [PubMed]
- Kenton, K.; Mueller, E.R.; Tarney, C.; Bresee, C.; Anger, J.T. One-Year Outcomes After Minimally Invasive Sacrocolpopexy. Female Pelvic. Med. Reconstr. Surg. 2016, 22, 382–384. [Google Scholar] [CrossRef]

{kind=link}
| Author, Year | Design of the Study | Surgical Approach | Sample Size | Main Findings | Short Term Outcomes | Long Term Outcomes |
|---|---|---|---|---|---|---|
| Advincula, 2007 [9] | Retrospective case-matched study | AM RAM | 58 29 29 | A robotic approach is associated with higher costs compared to laparotomy. Decreased estimated blood loss, complication rates, and length of stay with the robotic approach may prove to have a significant benefit. | Operative times: RAM > AM Estimated blood loss: RAM < AM Hospitalization time: RAM < AM Complications rate: AM > RAM (n 12 vs. 3) | NA |
| Bedient, 2009 [10] | Retrospective study | LM RAM | 81 41 40 | Short-term surgical outcomes were similar after robotic and laparoscopic myomectomy; long-term outcomes were not assessed. | Operative times: no significant differences Estimated blood loss: no significant differences Hospitalization time: no significant differences Complications rate: no significant differences | NA |
| Nezhat, 2009 [11] | Retrospective case matched study | LM RAM | 50 35 15 | RAM has a shorter learning curve, and does not add any additional morbidity to the LM. However, RAM shows no clinical advantage compared to LM. It may be useful during the learning period for non-experienced endoscopic surgeons | Operative times: RAM > LM Estimated blood loss: no significant difference Hospitalization time: no significant difference Complications rate: no major complications in the two groups | Pregnancy rate: no significant difference |
| Gargiulo, 2012 [12] | Retrospective cohort study | LM RAM | 289 115 174 | RAM and LM have similar operative outcomes. Operative time and intraoperative estimated blood loss were significantly greater in the robot-assisted laparoscopic myomectomy group. Use of barbed suture in the laparoscopic myomectomy group may account for these differences. | Operative times: RAM > LM Estimated blood loss: RAM > LM Hospitalization time: RAM > L Complications rate: no significant difference | NA |
| Barakat, 2011 [13] | Retrospective study | AM LM RAM | 575 393 93 89 | RAM is associated with decreased blood loss and length of hospital stay compared with LM and AM. Robotic technology could improve the utilization of the laparoscopic approach for the surgical management of symptomatic myomas. | Operative times: RAM > LM and AM Estimated blood loss: RAM < LM and AM Hospitalization time: AM > RAM and LM Complications rate: no major complications in RAM group, 1 wound dehiscence in LM, and 1 bowel injury in the LM | NA |
| Gobern, 2013 [14] | Retrospective study | AM LM RAM | 308 169 73 66 | LM and RAM demonstrated shorter hospital stays, less blood loss, and fewer transfusions than abdominal myomectomies. Robotic myomectomy offers a minimally invasive alternative for management of symptomatic myoma in a community hospital setting. | Operative time: RAM > LM and AM Blood loss: RAM and LM < AM Hospitalization time: RAM and LM < AM Postoperative pain: NA Complications rate: no differences | NA |
| Flyckt, 2016 [15] | Retrospective cohort study | AM LM RAM | 133 80 28 25 | There is no significant difference in long-term bleeding or fertility outcomes in robotic-assisted, laparoscopic, or abdominal myomectomy. | NA | Pregnancy rate: 60% with no differences between groups Uterine rupture: no cases Quality of life: no significant differences |
| Özbaşlı, 2021 [16] | Retrospective study | AM LM RAM | 227 73 88 66 | LM or RM may be a good choice for women of reproductive age because of short hospitalization duration, less blood transfusion and less postoperative pain. RAM appeared to be advantageous for patients with large myomas, on the other hand RM is more expensive and has longer operative times. | Operative time: RAM > LM and AM Blood loss: RM > LM and AM Hospitalization time: no differences Postoperative pain: RAM < LM and AM Complications rate: no significant differences. | NA |
| Author, Year | Design of the Study | Surgical Approach | Sample Size | Main Findings | Short Term Outcomes | Long Term Outcomes |
|---|---|---|---|---|---|---|
| Wright, 2013 [17] | Retrospective cohort study | AH VH LH RH | 264758 123288 54912 75761 10797 | Between 2007 and 2010, the use of RH increased substantially. RH and LH had similar morbidity profiles, but the use of robotic technology resulted in more costs. | Hospitalization time: LH > RH Complications rate: 5.3% LH, 5.5% RH (no significant) | NA |
| Paraiso, 2013 [18] | RCT | LH RH | 53 27 26 | LH and RH are safe approaches to hysterectomy. RH requires a significantly longer operative time. | Operative time: RH > LH Blood loss: comparable Hospitalization time: comparable Postoperative pain: comparable Complications rate: no significant differences, no major complications. | Quality of life at six months: no significant difference |
| Sarlos, 2012 [19] | RCT | LH RH | 95 | RH and LH compare well in most surgical aspects, but the robotic procedure is associated with longer operating times. Postoperative quality of-life index was better; however, longterm, there was no difference. | Operative time: RH > LH Blood loss: no significant difference Hospitalization time: Postoperative pain: Complications rate: no significant difference. | Long term quality of life: no difference |
| Lonnerfors, 2015 [20] | RCT | MIS (LH and VH) RH | 122 61 61 | A similar hospital cost can be attained for laparoscopy and robotics when the robot is a preexisting investment. Robotic-assisted hysterectomy is not advantageous for treating benign conditions when a vaginal approach is feasible in a high proportion of patients. | Operative time: comparable Blood loss: RH < LH Hospitalization time: NA Postoperative pain: NA Complications rate: RH < LH and VH | NA |
| Deimling, 2017 [21] | RCT | LH RH | 144 72 72 | When performed by a surgeon experienced in both techniques, the operative time for RH was non-inferior to that achieved with LH. | Operative time: comparable Blood loss: comparable Hospitalization time: NA Postoperative pain: NA Complications rate: one ureter transection in RH group. No differences in postoperative complications | NA |
| Author, Year | Design of the Study | Surgical Approach | Sample Size | Main Findings | Short Term Outcomes | Long Term Outcomes |
|---|---|---|---|---|---|---|
| Soto, 2017 [22] | RCT | LPS RS | 73 38 35 | Laparoscopy and robotic surgery for the treatment of endometriosis have comparable perioperative outcomes, even after adjustment for stage of disease, and significant improvement in quality of life after intervention. | Operative time: comparable Blood loss: comparable Complications rate: comparable Quality of life at six weeks: comparable | Quality of life at six months |
| Dubeshter, 2013 [23] | Retrospective study | LPS RS | 423 292 131 | The results show a minor length of operative times for LPS, and comparable outcomes regarding complications and perioperative outcomes for both groups. | Operative time: comparable Blood loss: comparable Complications rate: comparable | NA |
| Magrina, 2015 [24] | Retrospective study | LPS RS | 493 162 331 | RS is associated with longer operating time. Operating time is an independent and significant factor for postoperative complications and hospital stay. | Operative time: RS > LS Blood loss: depending on operative time Hospitalization time: depending on operative time Complications rate: depending on operative time | NA |
| Nezhat, 2013 [25] | Retrospective study | LPS RS | 118 86 32 | Despite a higher operating room time, RS appears to be a safe minimally invasive approach for advanced stage endometriosis treatment, with all other perioperative outcomes, including intraoperative and postoperative complications, comparable with those in patients undergoing LPS. | Operative time: RS > LPS Blood loss: comparable Complications rate: comparable | NA |
| Nezhat, 2015 [26] | Retrospective study | LPS RS | 420 273 147 | LPS and RS are excellent methods for treatment of advanced stages of endometriosis. However, use of the robotic platform may increase operative time and might also be associated with a longer hospital stay. | Operative time: RS > LPS Blood loss: comparable Hospitalization time: RS > LPS Complications rate: comparable | NA |
| Author, Year | Design of the Study | Surgical Approach | Sample Size | Main Findings | Short Term Outcomes | Long Term Outcomes |
|---|---|---|---|---|---|---|
| Paraiso, 2011 [27] | RCT | LSC RSC | 78 38 40 | Robotic-assisted sacrocolpopexy results in longer operating time and increased pain and cost compared with the conventional laparoscopic approach. | Operative time: RSC > LSC Blood loss: comparable Postoperative pain: RSC > LSC Complications rate: comparable | one year functional outcomes and vaginal support: comparable |
| Anger, 2014 [28] | RCT | LSC RSC | 78 38 40 | Costs of robotic sacrocolpopexy are higher than laparoscopic, while short-term outcomes and complications are similar. Primary cost differences resulted from robot maintenance and purchase costs. | Operative time: RSC > LSC Postoperative pain: RS > LPS Complications rate: comparable | six months POP outcome: comparable |
| Illiano, 2019 [29] | RCT | LSC RSC | 100 51 49 | RSC provides outcomes as good as those of LSC with 100% anatomical correction of the apical compartment. RSC can be considered a good alternative in the treatment of symptomatic, stage III or IV, POP. | Operative time: RSC > LSC Blood loss: comparable Hospitalization time: comparable Complications rate: comparable | Urinary, anorectal symtpoms and sexual funtion improved in both groups without significant difference. |
| Nosti, 2014 [30] | Retrospective study | ASC LSC RSC | 1124 589 273 262 | ASC is associated with a higher rate of perioperative and postoperative complications compared to MISC. The MISC group had shorter length of hospitalization, less blood loss, and longer operative times. Within the MISC group, RSC was associated with fewer complications compared to LSC. There was no difference in anatomic failure with any sacrocolpopexy approach | Operative time: RSC > LSC Blood loss: ASC > RSC and LSC Hospitalization time: ASC > RSC and LSC Complications rate: RSC < LSC and ASC | No significant difference in the rate of anatomical failure between the ASC and MISC groups |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capozzi, V.A.; Scarpelli, E.; Armano, G.; Monfardini, L.; Celardo, A.; Munno, G.M.; Fortunato, N.; Vagnetti, P.; Schettino, M.T.; Grassini, G.; et al. Update of Robotic Surgery in Benign Gynecological Pathology: Systematic Review. Medicina 2022, 58, 552. https://doi.org/10.3390/medicina58040552
Capozzi VA, Scarpelli E, Armano G, Monfardini L, Celardo A, Munno GM, Fortunato N, Vagnetti P, Schettino MT, Grassini G, et al. Update of Robotic Surgery in Benign Gynecological Pathology: Systematic Review. Medicina. 2022; 58(4):552. https://doi.org/10.3390/medicina58040552
Chicago/Turabian StyleCapozzi, Vito Andrea, Elisa Scarpelli, Giulia Armano, Luciano Monfardini, Angela Celardo, Gaetano Maria Munno, Nicola Fortunato, Primo Vagnetti, Maria Teresa Schettino, Giulia Grassini, and et al. 2022. "Update of Robotic Surgery in Benign Gynecological Pathology: Systematic Review" Medicina 58, no. 4: 552. https://doi.org/10.3390/medicina58040552
APA StyleCapozzi, V. A., Scarpelli, E., Armano, G., Monfardini, L., Celardo, A., Munno, G. M., Fortunato, N., Vagnetti, P., Schettino, M. T., Grassini, G., Labriola, D., Loreto, C., Torella, M., & Cianci, S. (2022). Update of Robotic Surgery in Benign Gynecological Pathology: Systematic Review. Medicina, 58(4), 552. https://doi.org/10.3390/medicina58040552