
Filling the Upper Pole with the Pectoralis Major Muscle Flap in Profunda Femoris Artery Perforator Flap Breast Reconstruction


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Study Outcomes and Variables
2.3. Statistical Analysis
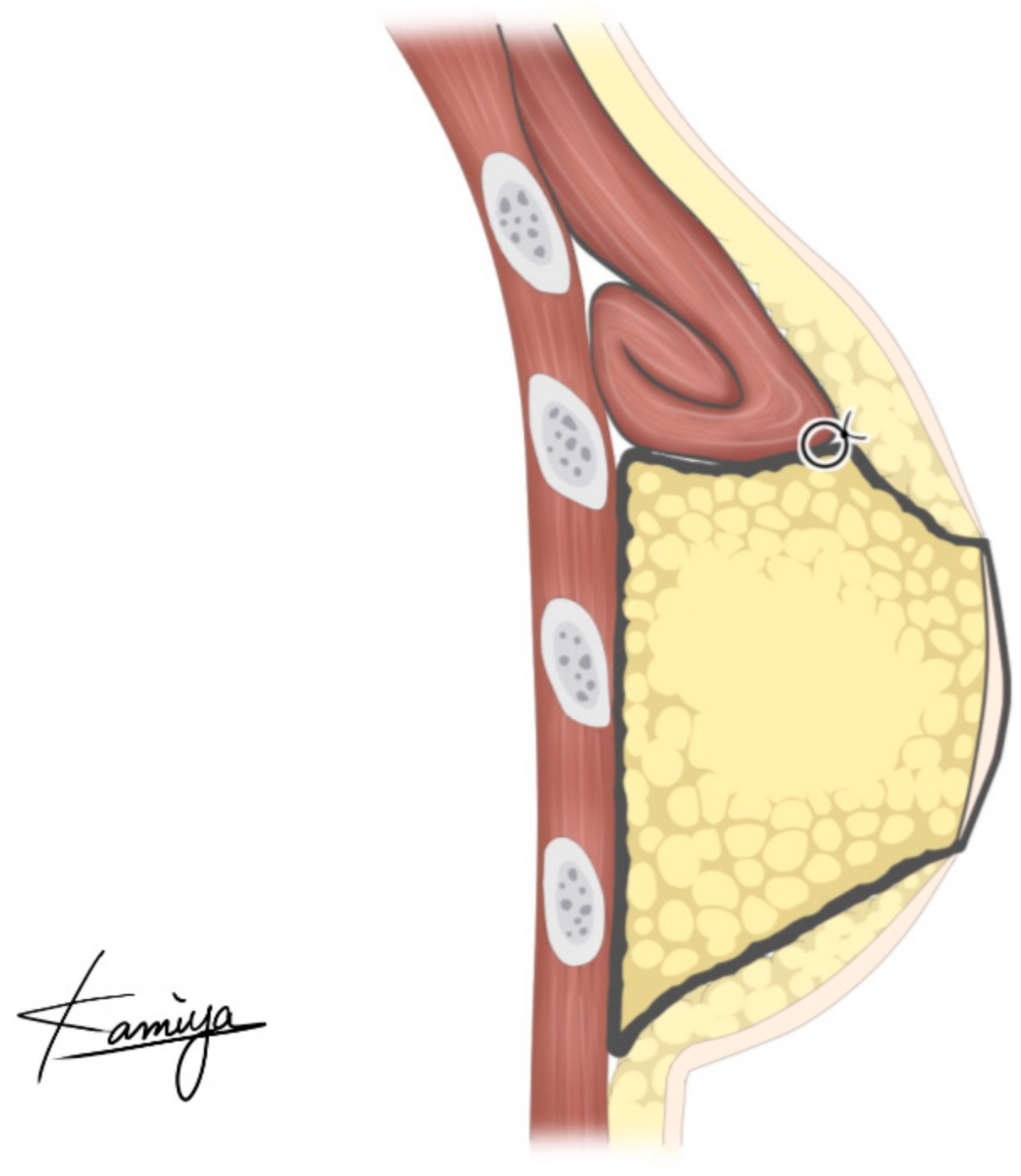
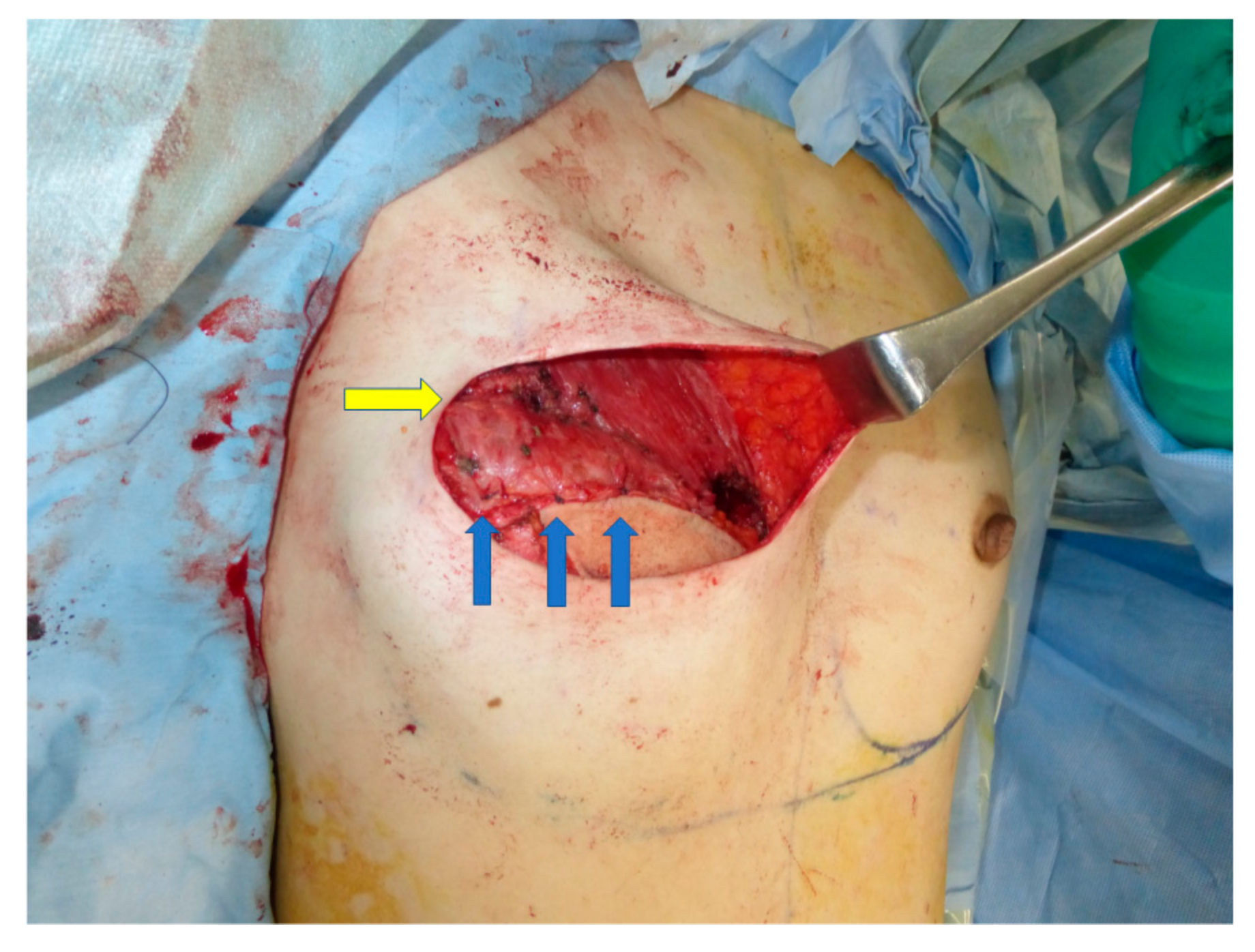
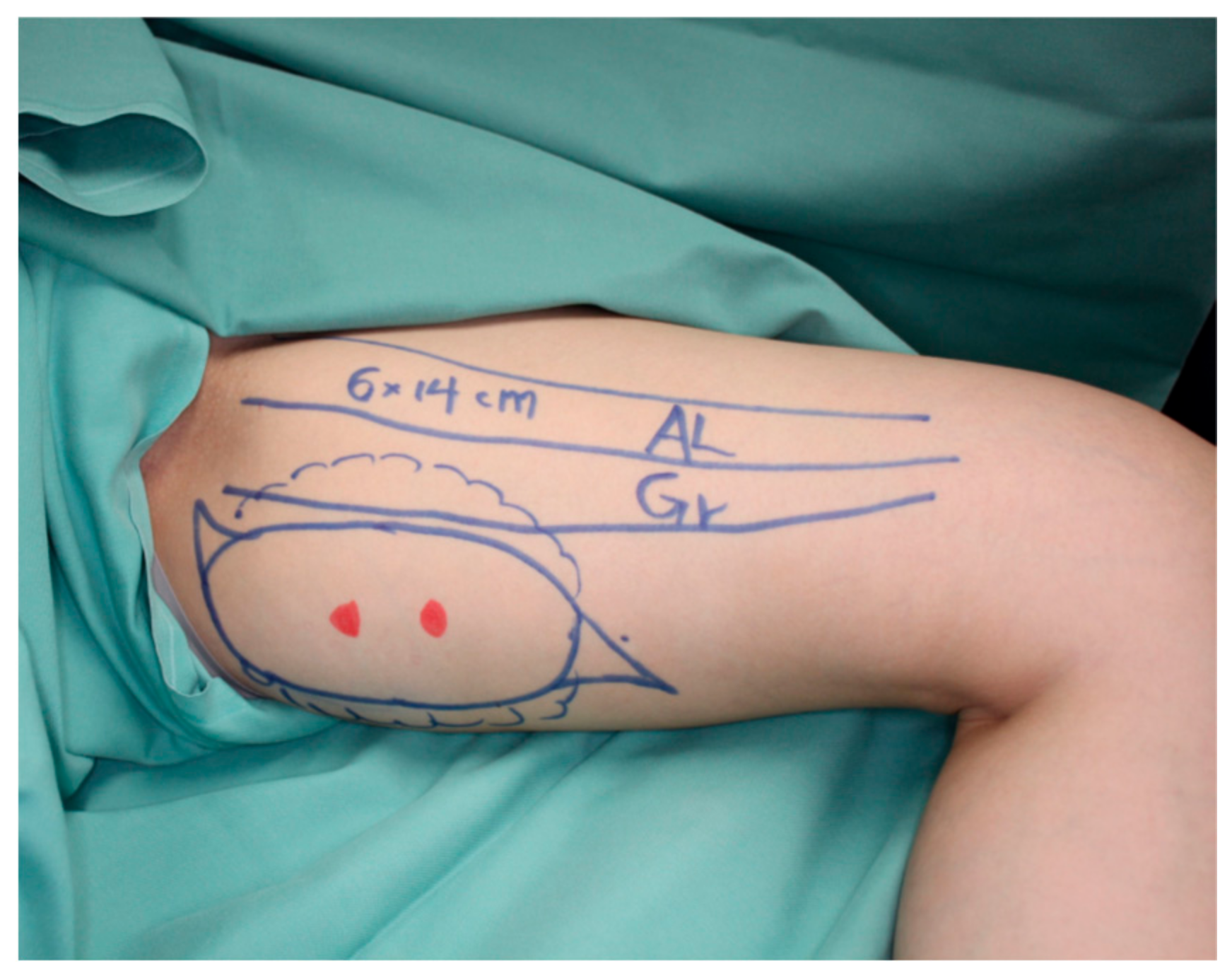
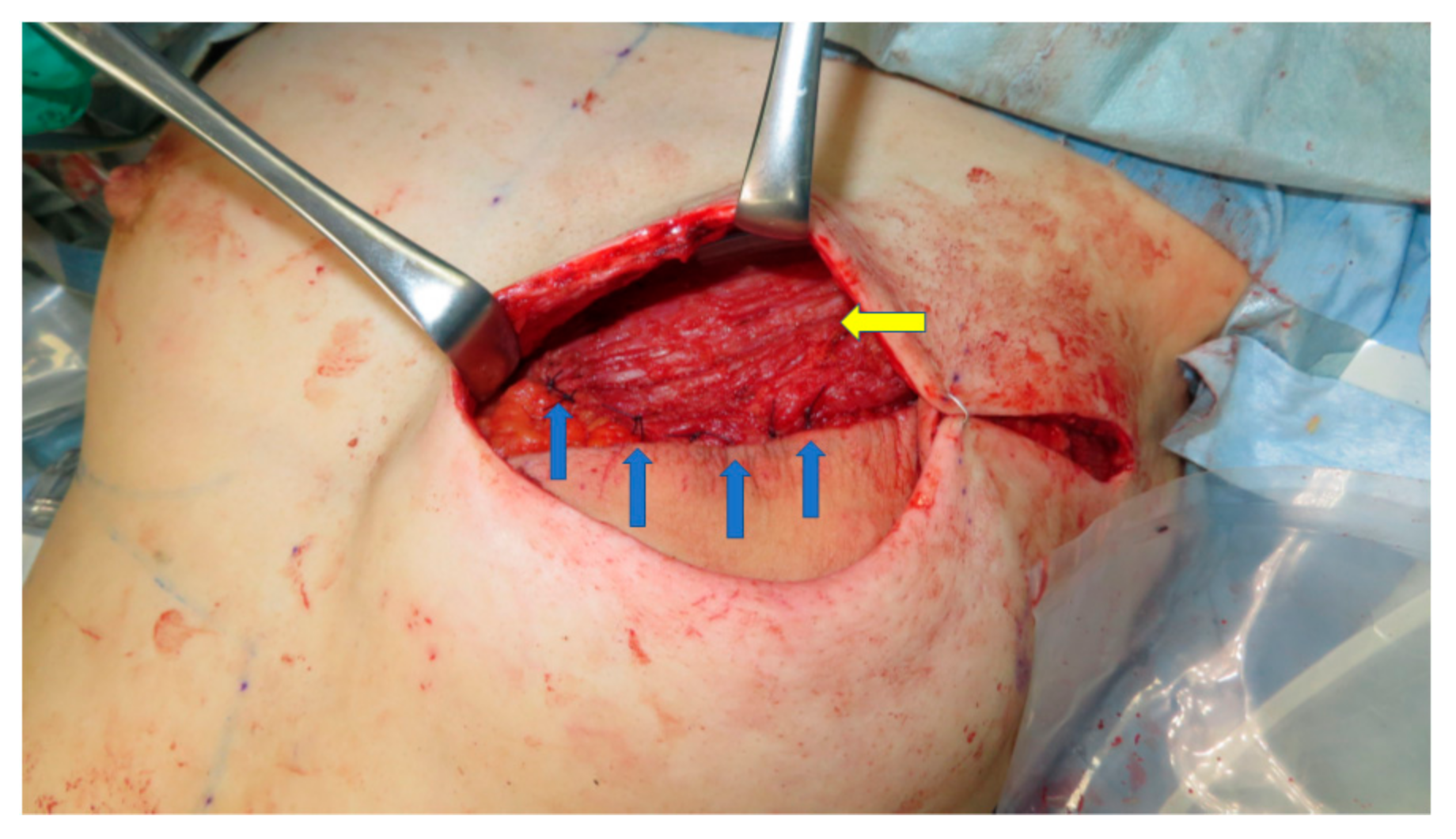
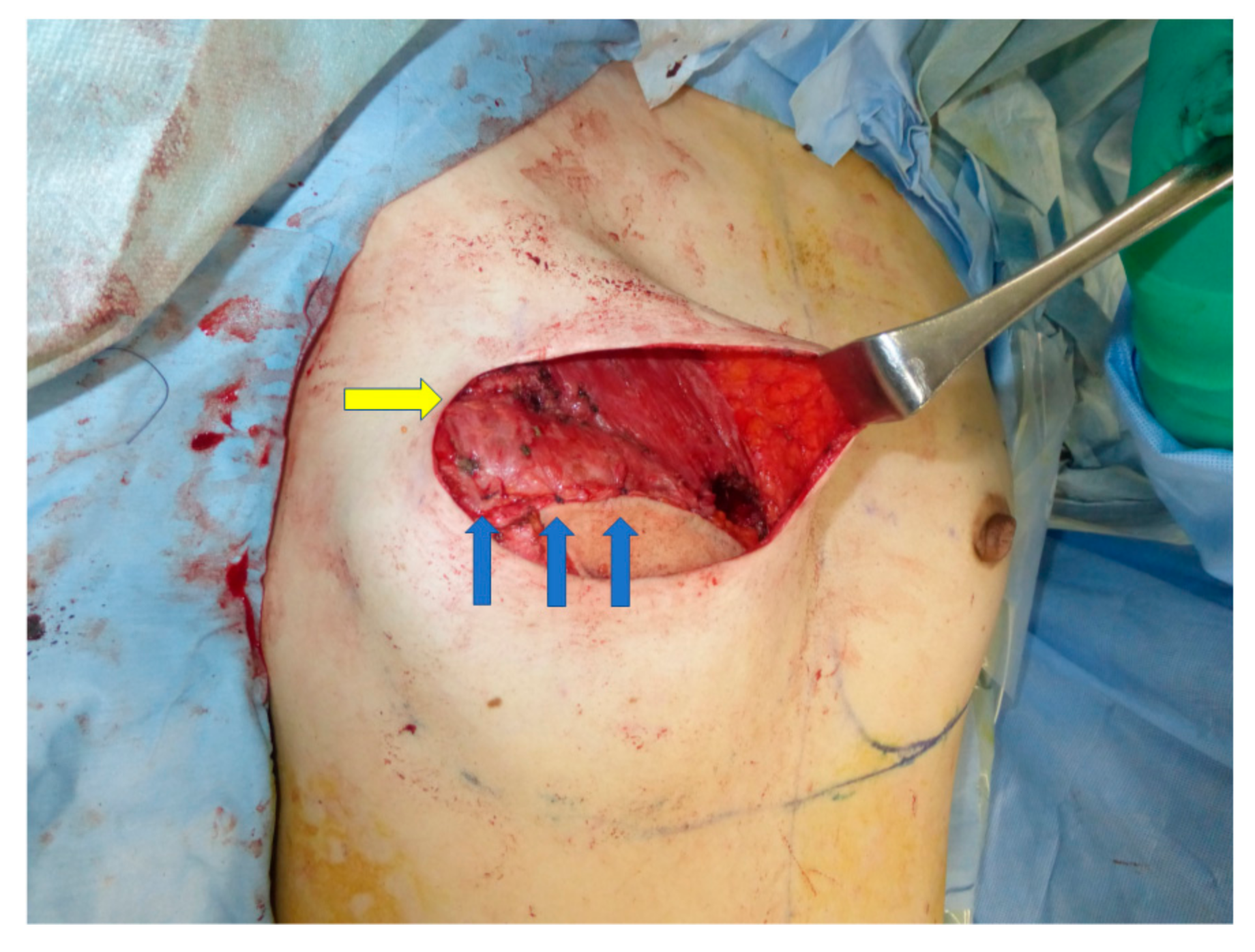
2.4. Surgical Technique of the Pectoralis Muscle Flap Augmentation
3. Results
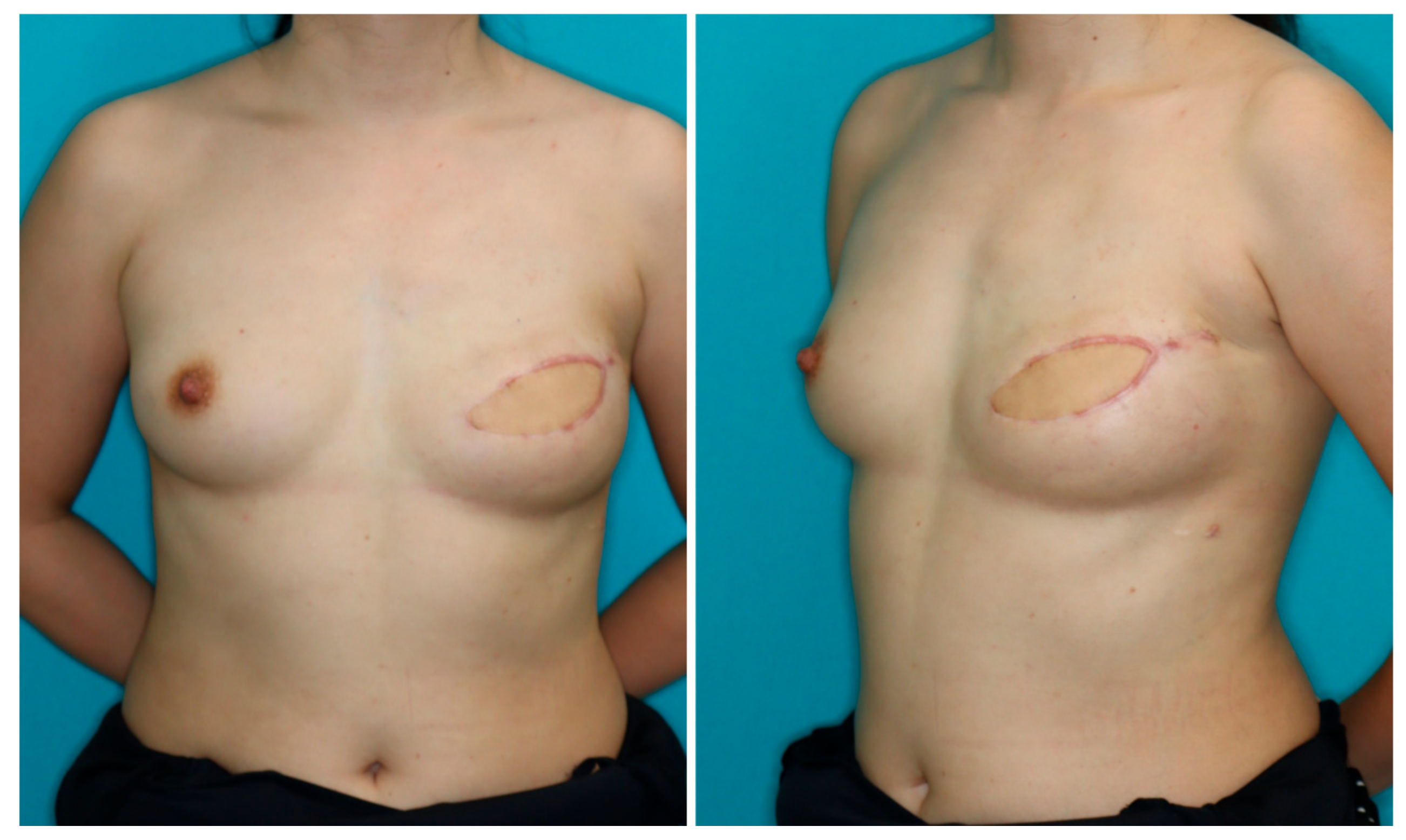
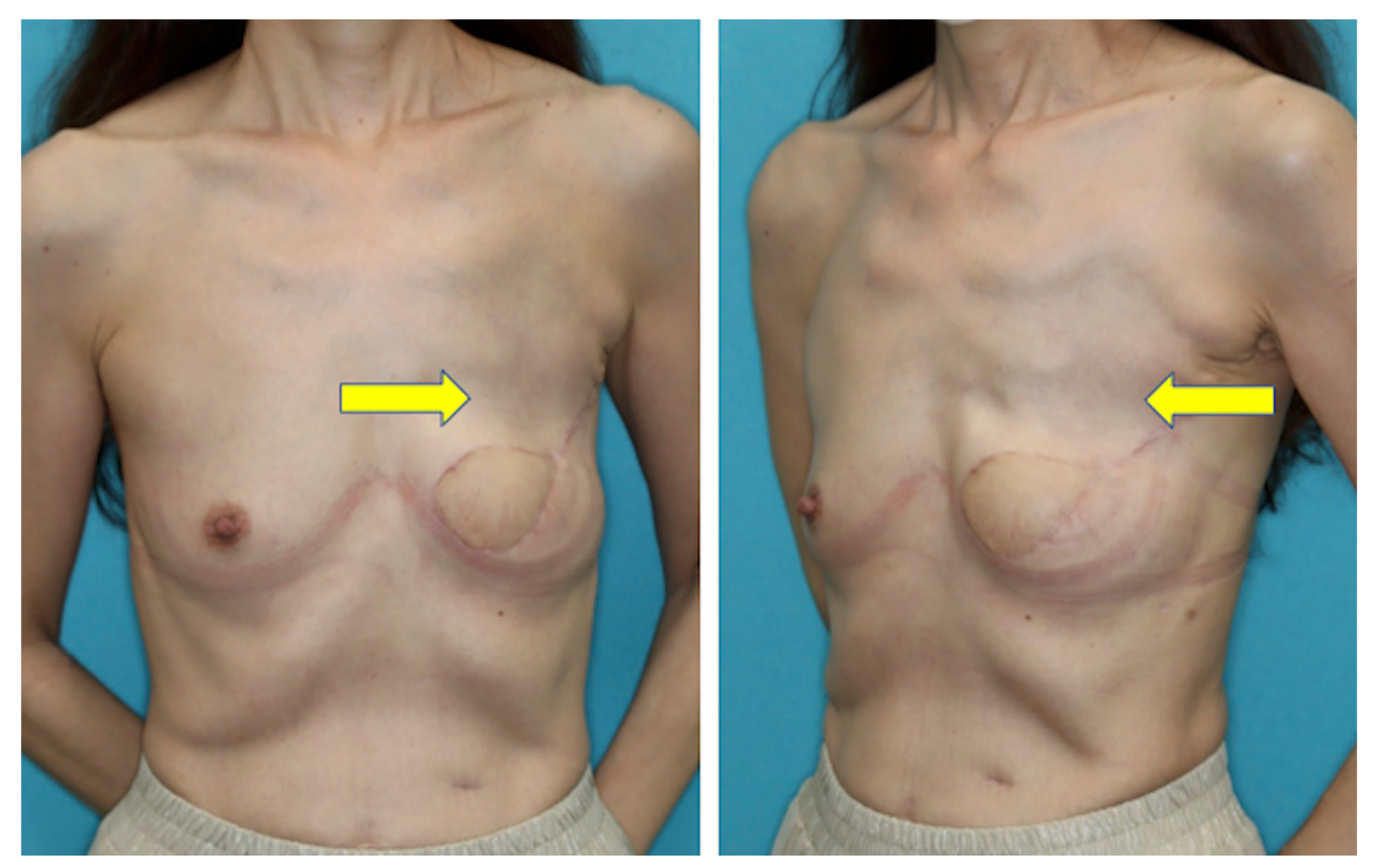
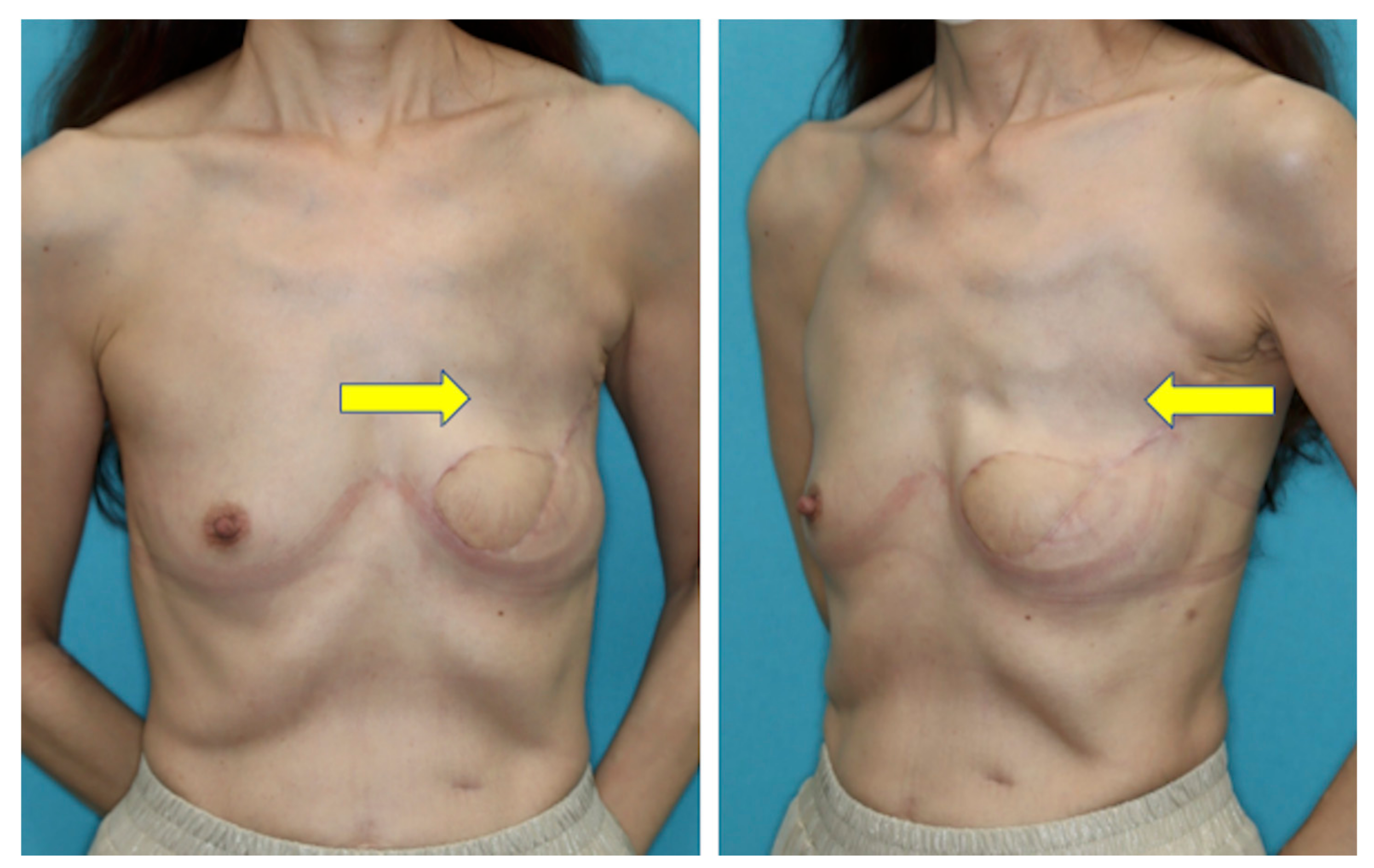
3.1. Case Reports
3.1.1. Case 1
3.1.2. Case 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Allen, R.J.; Haddock, N.T.; Ahn, C.Y.; Sadeghi, A. Breast reconstruction with the profunda artery perforator flap. Plast. Reconstr. Surg. 2012, 129, 16e–23e. [Google Scholar] [CrossRef]
- Allen, R.J.; Levine, J.L.; Granzow, J.W. The in-the-crease inferior gluteal artery perforator flap for breast reconstruction. Plast. Reconstr. Surg. 2006, 118, 333–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, R.J.; Tucker, C., Jr. Superior gluteal artery perforator free flap for breast reconstruction. Plast. Reconstr. Surg. 1995, 95, 1207–1212. [Google Scholar] [CrossRef] [PubMed]
- Fansa, H.; Schirmer, S.; Warnecke, I.C.; Cervelli, A.; Frerichs, O. The transverse myocutaneous gracilis muscle flap: A fast and reliable method for breast reconstruction. Plast. Reconstr. Surg. 2008, 122, 1326–1333. [Google Scholar] [CrossRef] [PubMed]
- Park, J.E.; Alkureishi, L.W.; Song, D.H. TUGs into VUGs and Friendly BUGs: Transforming the Gracilis Territory into the Best Secondary Breast Reconstructive Option. Plast. Reconstr. Surg. 2015, 136, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, M.F.; Chen, Y.C.; Lindenblatt, N.; Giovanoli, P. The vertical posteromedial thigh (vPMT) flap for autologous breast reconstruction: A novel flap design. Microsurgery 2017, 37, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Saad, A.; Sadeghi, A.; Allen, R.J. The anatomic basis of the profunda femoris artery perforator flap: A new option for autologous breast reconstruction-a cadaveric and computer tomography angiogram study. J. Reconstr. Microsurg. 2012, 28, 381–386. [Google Scholar] [CrossRef]
- DeLong, M.R.; Hughes, D.B.; Bond, J.E.; Thomas, S.M.; Boll, D.T.; Zenn, M.R. A detailed evaluation of the anatomical variations of the profunda artery perforator flap using computed tomographic angiograms. Plast. Reconstr. Surg. 2014, 134, 186e–192e. [Google Scholar] [CrossRef] [PubMed]
- Haddock, N.T.; Greaney, P.; Otterburn, D.; Levine, S.; Allen, R.J. Predicting perforator location on preoperative imaging for the profunda artery perforator flap. Microsurgery 2012, 32, 507–511. [Google Scholar] [CrossRef]
- Karakawa, R.; Yoshimatsu, H.; Tanakura, K.; Miyashita, H.; Shibata, T.; Kuramoto, Y.; Yano, T. An anatomical study of the lymph-collecting vessels of the medial thigh and clinical applications of lymphatic vessels preserving profunda femoris artery perforator (LpPAP) flap using pre- and intraoperative indocyanine green (ICG) lymphography. J. Plast. Reconstr. Aesthet. Surg. 2020, 73, 1768–1774. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.J.; Teotia, S.S.; Haddock, N.T. Classification and Management of Donor-Site Wound Complications in the Profunda Artery Perforator Flap for Breast Reconstruction. J. Reconstr. Microsurg. 2020, 36, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Blechman, K.M.; Broer, P.N.; Tanna, N.; Ireton, J.E.; Ahn, C.Y.; Allen, R.J. Stacked profunda artery perforator flaps for unilateral breast reconstruction: A case report. J. Reconstr. Microsurg. 2013, 29, 631–634. [Google Scholar]
- Haddock, N.T.; Cho, M.J.; Gassman, A.; Teotia, S.S. Stacked Profunda Artery Perforator Flap for Breast Reconstruction in Failed or Unavailable Deep Inferior Epigastric Perforator Flap. Plast. Reconstr. Surg. 2019, 143, 488e–494e. [Google Scholar] [CrossRef]
- Reissis, D.; Butler, D.P.; Henry, F.P.; Wood, S.H. Preserving a patent DIEP pedicle to facilitate salvage breast reconstruction with a second free flap: A case report. Microsurgery 2018, 38, 563–566. [Google Scholar] [CrossRef]
- Coleman, S.R. Long-term survival of fat transplants: Controlled demonstrations. Aesth. Plast. Surg. 1995, 19, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Ho Quoc, C.; Taupin, T.; Guérin, N. Delay E volumetric evaluation of fat resorption after breast lipofilling. Ann. Chir. Plast. Esthet. 2015, 60, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Tebbetts, J.B. Dual plane breast augmentation: Optimizing implant-soft-tissue relationships in a wide range of breast types. Plast Reconstr Surg. 2001, 107, 1255–1272. [Google Scholar] [CrossRef] [Green Version]
- Qi-Gen, F.; Shuang, S.; Xu, Z.; Zhen-Ning, L.; Fa-Yu, L.; Chang-Fu, S. Assessment of the quality of life of patients with oral cancer after pectoralis major myocutaneous flap reconstruction with a focus on speech. J. Oral Maxillofac. Surg. 2013, 71, 2004.e1–2004.e5. [Google Scholar]
- Hsing, C.Y.; Wong, Y.K.; Wang, C.P.; Wang, C.C.; Jiang, R.S.; Chen, F.J.; Liu, S.A. Comparison between free flap and pectoralis major pedicled flap for reconstruction of oral cavity cancer patients-A quality of life analysis. Oral Oncol. 2011, 47, 522. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Li, M.J.; Fang, Q.C.; Sun, C.F. A comparison between the pectoralis major myocutaneous flap and the free anterolateral thigh perforator flap for reconstruction in head and neck cancer patients: Assessment of the quality of life. J. Craniofac. Surg. 2014, 25, 868. [Google Scholar] [CrossRef] [PubMed]
- Moukarbel, R.V.; Fung, K.; Franklin, J.H.; Leung, A.; Rastogi, R.; Anderson, C.M.; Yoo, J.H. Neck and shoulder disability following reconstruction with the pectoralis major pedicled flap. Laryngoscope 2010, 120, 1129. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.M.; Shim, J.S. Volume Change of Pedicled Latissimus Dorsi Muscle Flap after Partial Breast Reconstruction. J. Reconstr. Microsurg. 2018, 34, 651–657. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PAP Flap without Use of the Pectoralis Major Muscle Flap Cohort (Group 1) N = 36 | PAP Flap Augmented with Pectoralis Major Muscle Flap Cohort (Group 2) N = 23 | p-Value | |
|---|---|---|---|
| Age (years), mean (range) | 46.6 (27–67) | 47.0 (34–64) | 0.91 |
| Delayed reconstruction | 19 (53%) | 22 (96%) | <0.001 |
| Body mass index, mean (range) | 20.6 (17.1–29.6) | 21.3 (17.0–30.0) | 0.32 |
| Flap weight (g), mean (range) | 218 (105–435) | 216 (140–370) | 0.92 |
| PAP Flap without Use of the Pectoralis Major Muscle Flap Cohort (Group 1) N = 36 | PAP Flap Augmented with Pectoralis Major Muscle Flap Cohort (Group 2) N = 23 | p-Value | |
|---|---|---|---|
| Satisfied after 12 months | 23 (64%) | 22 (96%) | 0.005 |
| Postoperative complications | 2 (5.6%) | 0 (0%) | 0.52 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshimatsu, H.; Miyashita, H.; Karakawa, R.; Fuse, Y.; Yano, T. Filling the Upper Pole with the Pectoralis Major Muscle Flap in Profunda Femoris Artery Perforator Flap Breast Reconstruction. Medicina 2022, 58, 458. https://doi.org/10.3390/medicina58040458
Yoshimatsu H, Miyashita H, Karakawa R, Fuse Y, Yano T. Filling the Upper Pole with the Pectoralis Major Muscle Flap in Profunda Femoris Artery Perforator Flap Breast Reconstruction. Medicina. 2022; 58(4):458. https://doi.org/10.3390/medicina58040458
Chicago/Turabian StyleYoshimatsu, Hidehiko, Hiroki Miyashita, Ryo Karakawa, Yuma Fuse, and Tomoyuki Yano. 2022. "Filling the Upper Pole with the Pectoralis Major Muscle Flap in Profunda Femoris Artery Perforator Flap Breast Reconstruction" Medicina 58, no. 4: 458. https://doi.org/10.3390/medicina58040458
APA StyleYoshimatsu, H., Miyashita, H., Karakawa, R., Fuse, Y., & Yano, T. (2022). Filling the Upper Pole with the Pectoralis Major Muscle Flap in Profunda Femoris Artery Perforator Flap Breast Reconstruction. Medicina, 58(4), 458. https://doi.org/10.3390/medicina58040458