
Hidden in the Eyes—Recurrence of Systemic Hemopathies Reportedly “In Remission”: Six Cases and Review of Literature

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Presentation of Our Cases
3.1.1. Case 1. First Relapse of an ALL
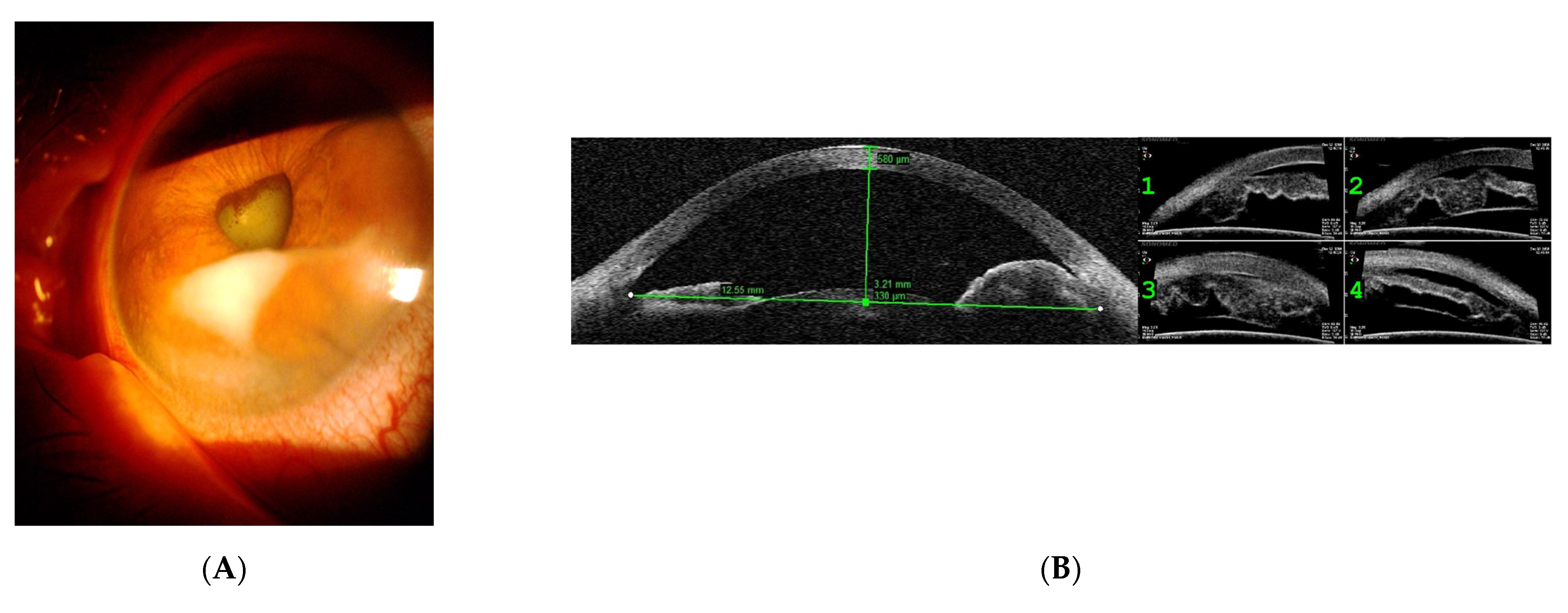
3.1.2. Case 2. Relapse in the Form of Iris Plasmacytoma
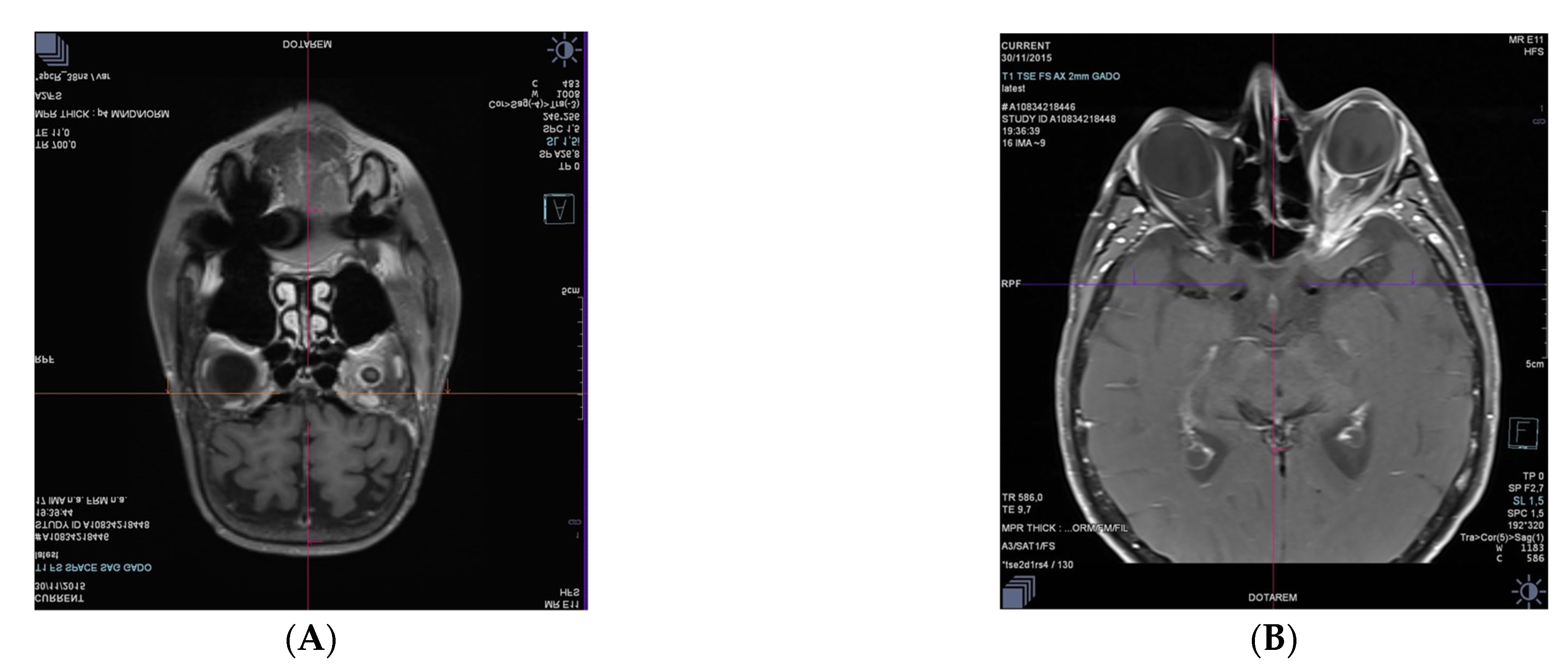
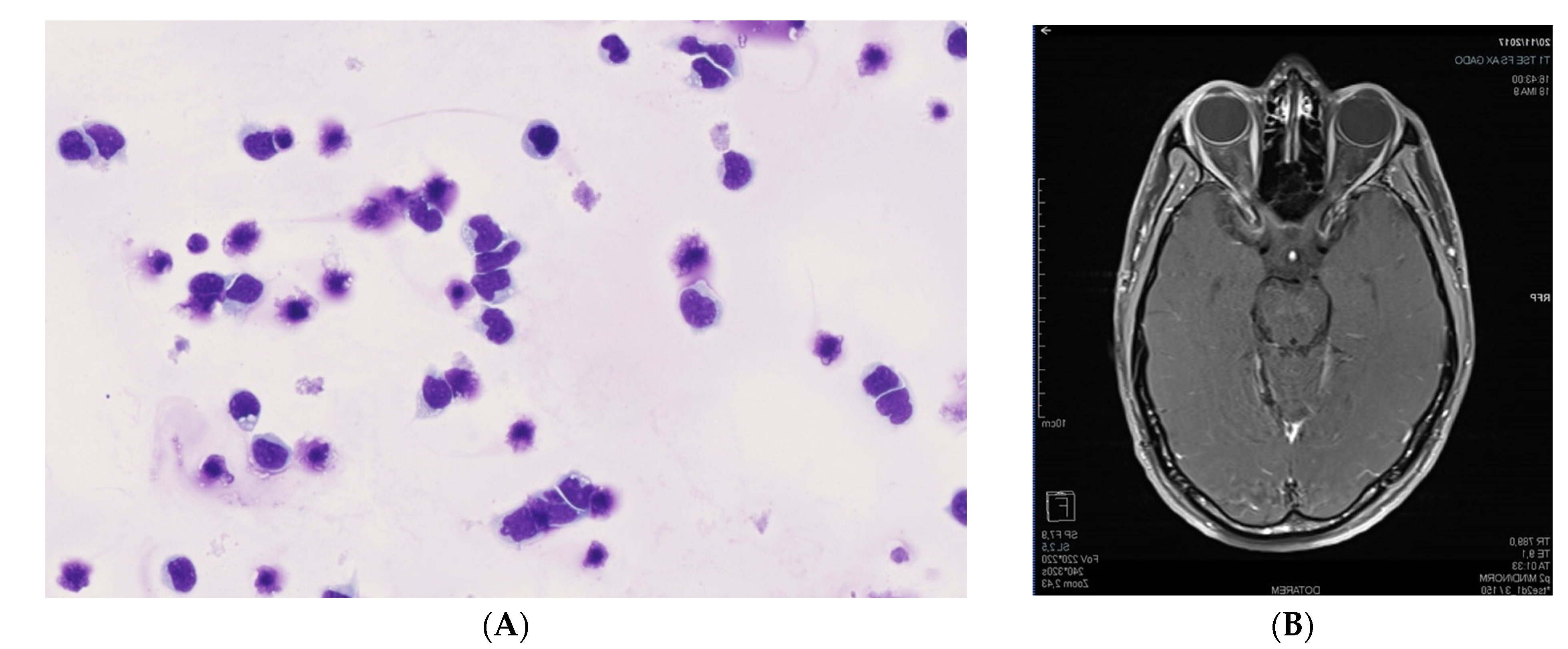
3.1.3. Case 3. Orbital Relapses in the Case of Systemic DLBCL, despite Auto and Allograft Transplant of Hematopoietic Stem Cells
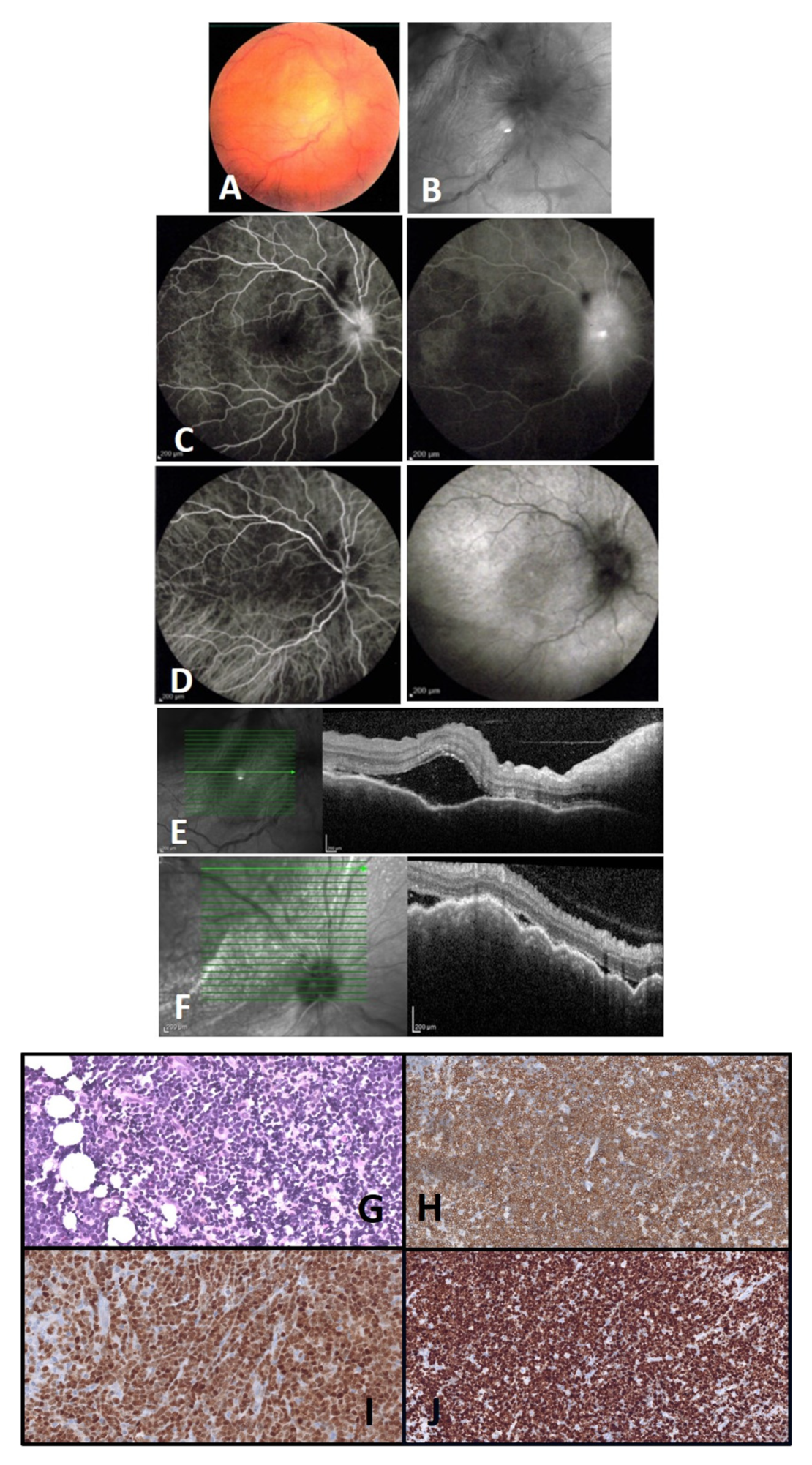
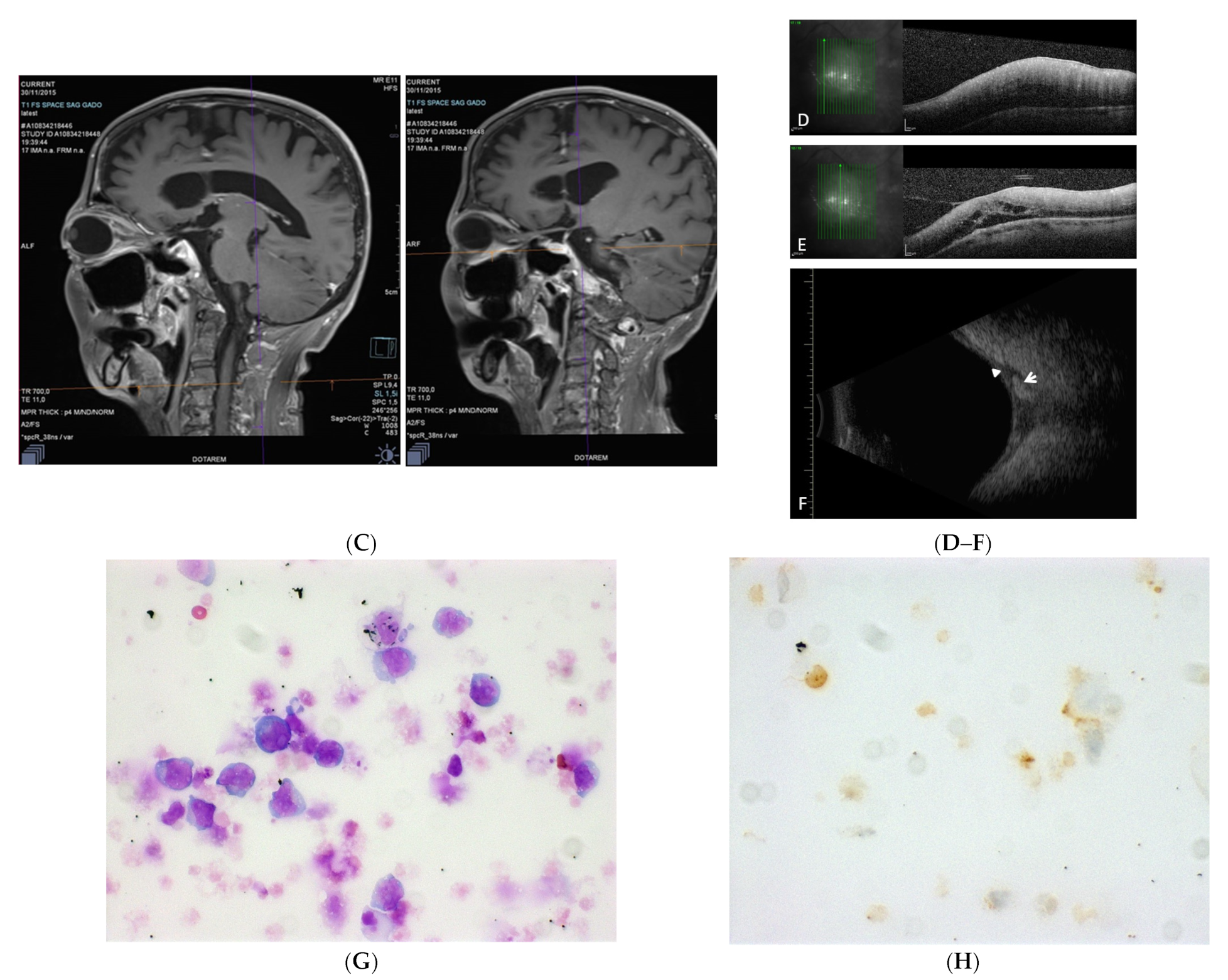
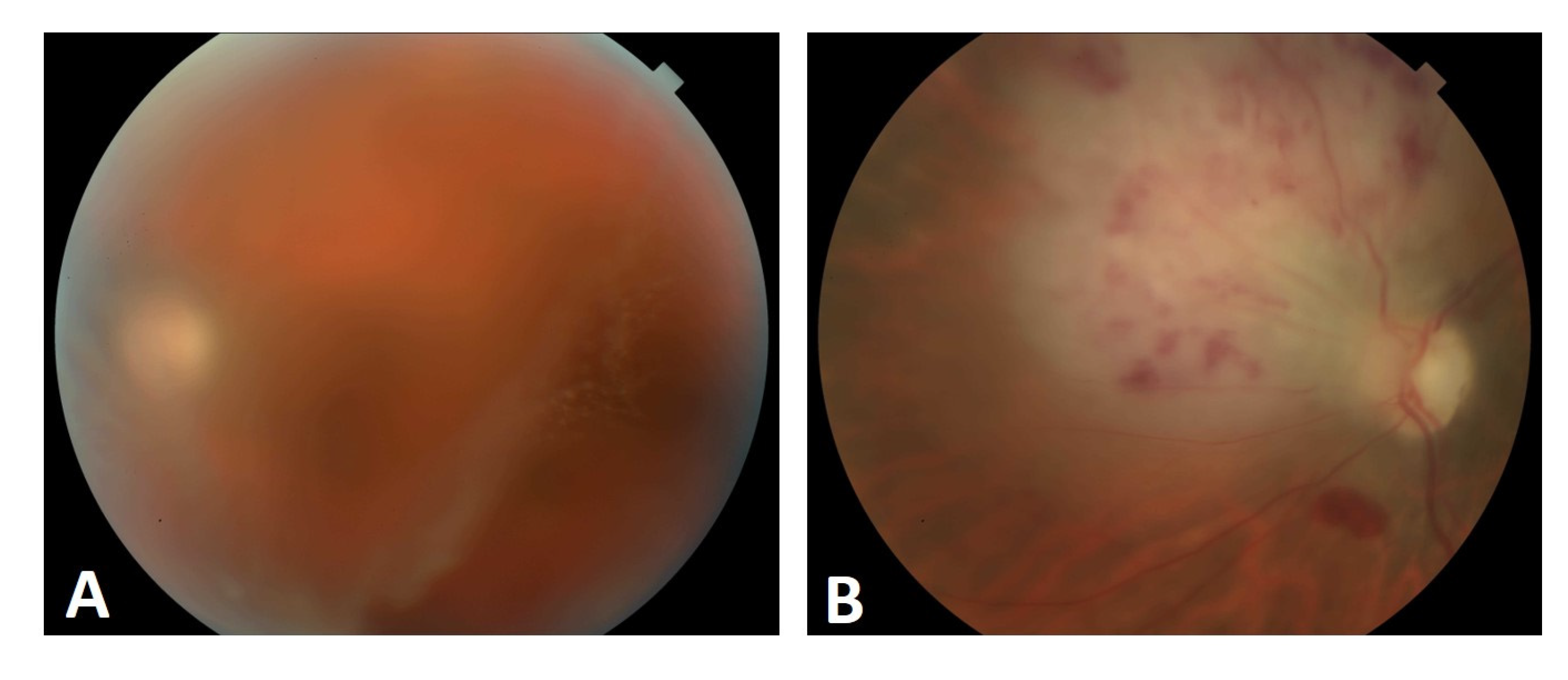
3.1.4. Case 4. First Vitreous Relapse in the Case of Systemic DLBCL, despite CAR T-cell Therapy with Axicabtagene Ciloleucel. Second Retinal Relapse in the Form of a Retinitis after Pembrolizumab Infusions, Intravitreal Methotrexate, and Intrathecal Methotrexate
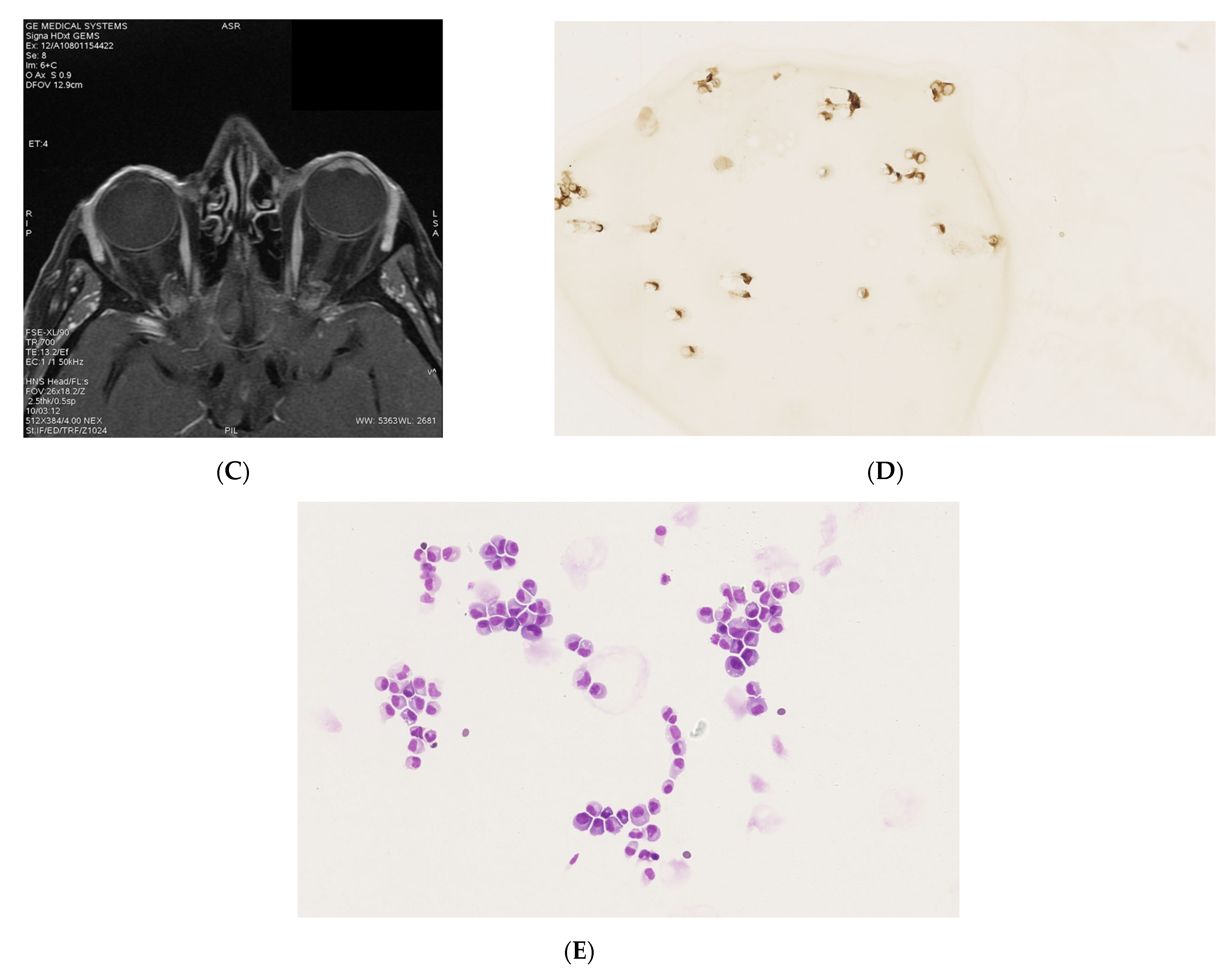
3.1.5. Case 5. Location in the Ciliary Process Associated with an Anterior Pseudo-Uveitis, Six Months after Completing a Treatment for ALL
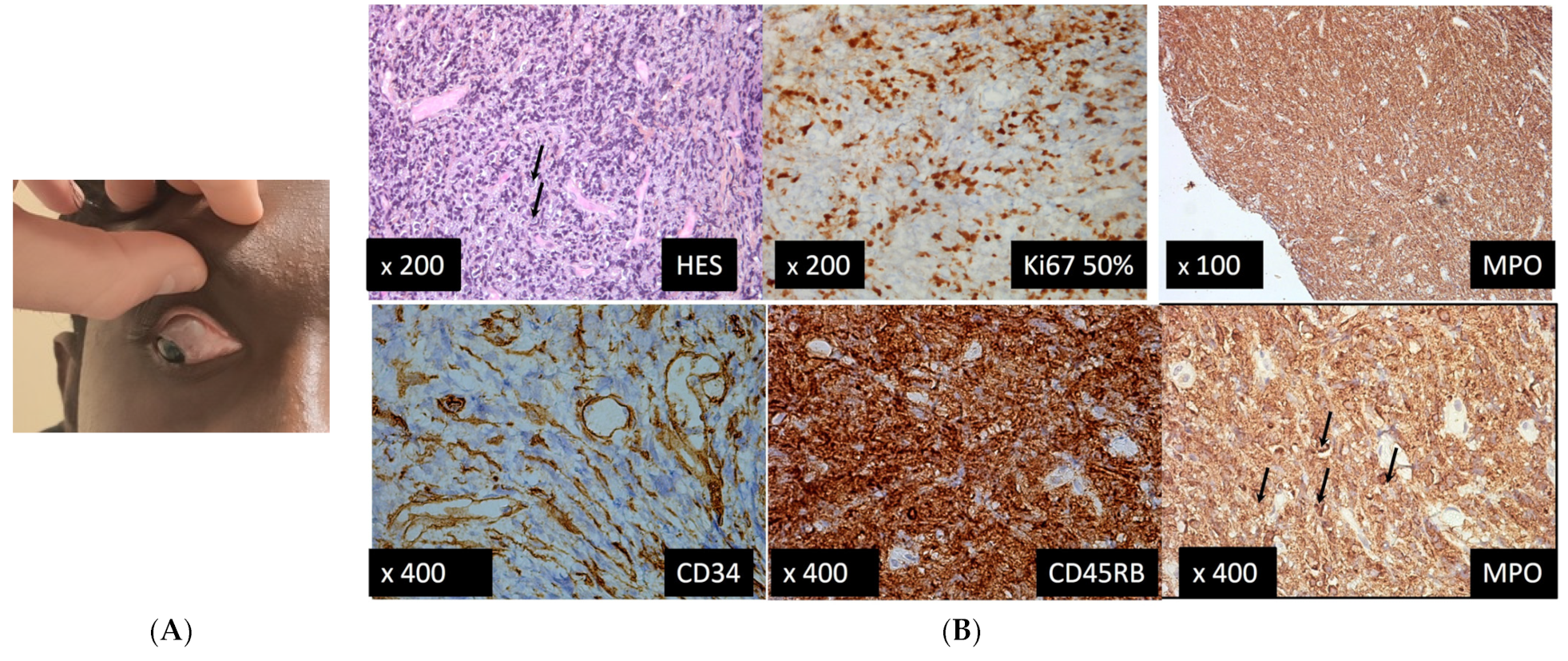
3.1.6. Case 6. Location in the Conjunctiva Associated with a Myeloid Sarcoma, Six Months after Completing a Treatment for ALL
4. Discussion
4.1. Cases 1, 5, and 6
4.2. Case 2
4.3. Cases 3 and 4
4.4. General Discussion
5. Conclusions
Clinical Practice Points
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- World Health Organization. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2017. [Google Scholar]
- LLS CalSo Blood Cancer Awareness Month. Leukemia and Lymphoma Society. Available online: https://www.lls.org/article/lls-calso-blood-cancer-awareness-month (accessed on 22 November 2021).
- Monnereau, A.; Remontet, L.; Maynadié, M.; Binder-Foucard, F.; Belot, A.; Troussard, X.; Bossard, N.; Monnereau, A. Estimation Nationale de l’Incidence des Cancers en France entre 1980 et 2012 n.d. Available online: http://invs.santepubliquefrance.fr/Publications-et-outils/Rapports-et-syntheses/Maladies-chroniques-et-traumatismes/2013/Estimation-nationale-de-l-incidence-et-de-la-mortalite-par-cancer-en-France-entre-1980-et-2012 (accessed on 31 March 2017).
- Schachat, A.P. Ophthalmic manifestations of leukemia. Arch. Ophthalmol. 1989, 107, 697. [Google Scholar] [CrossRef] [PubMed]
- Albert, D.M.; Jakobiec, F.A.; Miller, J.W. Chapter 170—Retinopathy associated with blood anomalies. In Albert & Jakobiec’s Principles and Practice of Ophthalmology; Saunders/Elsevier: Philadelphia, PA, USA, 2008. [Google Scholar]
- Russo, V.; Scott, I.; Querques, G.; Stella, A.; Barone, A.; Noci, N.D. Orbital and ocular manifestations of acute childhood leukemia: Clinical and statistical analysis of 180 patients. Eur. J. Ophthalmol. 2008, 18, 619–623. [Google Scholar] [CrossRef] [PubMed]
- MacLean, H.; Clarke, M.P.; Strong, N.P.; Kernahan, J.; Ashraf, S. Primary ocular relapse in acute lymphoblastic leukaemia. Eye 1996, 10, 719–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burkat, C.N.; Van Buren, J.J.; Lucarelli, M.J. Characteristics of orbital multiple myeloma: A case report and literature review. Surv. Ophthalmol. 2009, 54, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Ashton, N. Ocular changes in multiple myelomatosis. Arch. Ophthalmol. 1965, 73, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Kyle, R.A.; Rajkumar, S.V. Multiple myeloma. N. Engl. J. Med. 2004, 351, 1860–1873. [Google Scholar] [CrossRef]
- Aronson, S.B.; Shaw, R. Corneal crystals in multiple myeloma. JAMA Arch. Ophthalmol. 1959, 61, 541–546. [Google Scholar] [CrossRef]
- Yeung, S.N.; Paton, K.E.; Dorovini-Zis, K.; Chew, J.B.; White, V.A. Histopathologic features of multiple myeloma involving the optic nerves. J. Neuro-Ophthalmol. 2008, 28, 12–16. [Google Scholar] [CrossRef]
- Shakin, E.P.; Augsburger, J.J.; Eagle, R.C.; Ehya, H.; Shields, J.A.; Fischer, D.; Koepsell, D.G. Multiple myeloma involving the iris. Arch. Ophthalmol. 1988, 106, 524–526. [Google Scholar] [CrossRef]
- Rubenzik, R.; Tenzel, R. Multiple myeloma involving the lacrimal gland. Ann. Ophthalmol. 1975, 7, 1077–1078. [Google Scholar]
- Shen, Y.-C.; Wang, C.-Y.; Huang, T.-Y.; Lo, Y.-S.; Fong, S.-C.; Lee, Y.-F. Multiple myeloma manifesting as a salmon patch conjunctival mass. Am. J. Ophthalmol. 2006, 141, 948–949. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, A.S.; Stein, R.M.; Gaines, B.I.; Deutsch, T.A. Ocular deposition of copper associated with multiple myeloma. Am. J. Ophthalmol. 2001, 131, 257–259. [Google Scholar] [CrossRef]
- Fung, S.; Selva, D.; Leibovitch, I.; Hsuan, J.; Crompton, J. Ophthalmic manifestations of multiple myeloma. Ophthalmologica 2005, 219, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Thoumazet, F.; Donnio, A.; Ayeboua, L.; Brebion, A.; Diedhou, A.; Merle, H. Orbital and muscle involvement in multiple myeloma. Can. J. Ophthalmol. 2006, 41, 733–736. [Google Scholar] [CrossRef]
- Adkins, J.W.; Shields, J.A.; Shields, C.L.; Eagle, R.C.; Flanagan, J.C.; Campanella, P.C. Plasmacytoma of the eye and orbit. Int. Ophthalmol. 1996, 20, 339–343. [Google Scholar] [CrossRef]
- Tung, G.; Finger, P.T.; Klein, I.; Chess, Q. Plasmacytoma of the orbit. Arch. Ophthalmol. 1988, 106, 1622. [Google Scholar] [CrossRef]
- Shields, C.L.; Chong, W.H.; Ehya, H.; Shields, J.A. Sequential bilateral solitary extramedullary plasmacytoma of the ciliary body. Cornea 2007, 26, 759–761. [Google Scholar] [CrossRef]
- Omoti, A.E.; Omoti, C.E. Ophthalmic manifestations of multiple myeloma. West Afr. J. Med. 2007, 26, 265–268. [Google Scholar] [CrossRef] [Green Version]
- Buggage, R.R.; Chan, C.-C.; Nussenblatt, R.B. Ocular manifestations of central nervous system lymphoma. Curr. Opin. Oncol. 2001, 13, 137–142. [Google Scholar] [CrossRef]
- Tang, L.J.; Gu, C.L.; Zhang, P. Intraocular lymphoma. Int. J. Ophthalmol. 2017, 10, 1301–1307. [Google Scholar]
- Araujo, I.; Coupland, S. Primary vitreoretinal lymphoma—A review. Asia-Pac. J. Ophthalmol. 2017, 6, 283–289. [Google Scholar]
- Davis, J.L. Intraocular lymphoma: A clinical perspective. Eye 2013, 27, 153–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coupland, S.E.; Damato, B. Lymphomas involving the eye and the ocular adnexa. Curr. Opin. Ophthalmol. 2006, 17, 523–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coupland, S.E.; Krause, L.; Delecluse, H.J.; Anagnostopoulos, I.; Foss, H.D.; Hummel, M.; Bornfeld, N.; Lee, W.R.; Stein, H. Lymphoproliferative lesions of the ocular adnexa. Ophthalmology 1998, 105, 1430–1441. [Google Scholar] [CrossRef]
- McKelvie, P.A. Ocular adnexal lymphomas: A review. Adv. Anat. Pathol. 2010, 17, 251–261. [Google Scholar] [CrossRef]
- Yamamoto, J.F.; Goodman, M.T. Patterns of leukemia incidence in the United States by subtype and demographic characteristics, 1997–2002. Cancer Causes Control 2008, 19, 379–390. [Google Scholar] [CrossRef]
- Döhner, H.; Estey, E.H.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Burnett, A.K.; Dombret, H.; Fenaux, P.; Grimwade, D.; Larson, R.A.; et al. Diagnosis and management of acute myeloid leukemia in adults: Recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood 2010, 115, 453–474. [Google Scholar] [CrossRef]
- De Kouchkovsky, I.; Abdul-Hay, M. Acute myeloid leukemia: A comprehensive review and 2016 update. Blood Cancer J. 2016, 6, e441. [Google Scholar] [CrossRef]
- Karesh, J.W.; Goldman, E.J.; Reck, K.; Kelman, S.E.; Lee, E.J.; Schiffer, C.A. A prospective ophthalmic evaluation of patients with acute myeloid leukemia: Correlation of ocular and hematologic findings. J. Clin. Oncol. 1989, 7, 1528–1532. [Google Scholar] [CrossRef]
- Jackson, N.; Reddy, S.; Hishamuddin, M.; Low, H. Retinal findings in adult leukaemia: Correlation with leukocytosis. Clin. Int. J. Lab. Hematol. 1996, 18, 105–109. [Google Scholar] [CrossRef]
- Reddy, S.C.; Jackson, N.; Menon, B.S. Ocular involvement in leukemia—A study of 288 cases. Ophthalmologica 2003, 217, 441–445. [Google Scholar] [CrossRef]
- Novakovic, P.; Kellie, S.J.; Taylor, D. Childhood leukaemia: Relapse in the anterior segment of the eye. Br. J. Ophthalmol. 1989, 73, 354–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Decker, E.B.; Burnstine, R.A. Leukemic relapse presenting as acute unilateral hypopyon in acute lymphocytic leukemia. Ann. Ophthalmol. 1993, 25, 346–349. [Google Scholar] [PubMed]
- Yi, D.H.; Rashid, S.; Cibas, E.S.; Arrigg, P.G.; Dana, M.R. Acute unilateral leukemic hypopyon in an adult with relapsing acute lymphoblastic leukemia. Am. J. Ophthalmol. 2005, 139, 719–721. [Google Scholar] [CrossRef] [PubMed]
- Ninane, J.; Taylor, D.; Day, S. The eye as a sanctuary in acute lymphoblastic leukaemia. Lancet 1980, 1, 452–453. [Google Scholar] [CrossRef]
- Sanders, T.E.; Podos, S.M.; Rosenbaum, L.J. Intraocular manifestations of multiple myeloma. Arch. Ophthalmol. 1967, 77, 789–794. [Google Scholar] [CrossRef]
- Rodman, H.I. Orbital involvement in multiple myeloma: Review of the literature and report of three cases. Arch. Ophthalmol. 1972, 87, 30. [Google Scholar] [CrossRef]
- De Smet, M.D.; Rootman, J. Orbital manifestations of piasmacytic lymphoproliferations. Ophthalmology 1987, 94, 995–1003. [Google Scholar] [CrossRef]
- Chin, K.J.; Kempin, S.; Milman, T.; Finger, P.T. Ocular manifestations of multiple myeloma: Three cases and a review of the literature. Optometry 2011, 82, 224–230. [Google Scholar] [CrossRef]
- Greipp, P.R.; Miguel, J.S.; Durie, B.G.; Crowley, J.J.; Barlogie, B.; Bladé, J.; Boccadoro, M.; Child, J.A.; Avet-Loiseau, H.; Kyle, R.A.; et al. International staging system for multiple myeloma. J. Clin. Oncol. 2005, 23, 3412–3420. [Google Scholar] [CrossRef]
- Kyle, R.A.; Rajkumar, S.V. Treatment of multiple myeloma: A comprehensive review. Clin. Lymphoma Myeloma 2009, 9, 278–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: A report of the International Myeloma Working Group. Br. J. Haematol. 2003, 121, 749–757. [Google Scholar] [CrossRef] [Green Version]
- Bairey, O.; Kremer, I.; Rakowsky, E.; Hadar, H.; Shaklai, M. Orbital and adnexal involvement in systemic non-Hodgkin’s lymphoma. Cancer 1994, 73, 2395–2399. [Google Scholar] [CrossRef]
- Lazzarino, M.; Morra, E.; Rosso, R.; Brusamolino, E.; Pagnucco, G.; Castello, A.; Ghisolfi, A.; Tafi, A.; Zennaro, G.; Bernasconi, C. Clinicopathologic and immunologic characteristics of non-Hodgkin’s lymphomas presenting in the orbit. A report of eight cases. Cancer 1985, 55, 1907–1912. [Google Scholar] [CrossRef]
- Sullivan, T.J.; Whitehead, K.; Williamson, R.; Grimes, D.; Schlect, D.; Brown, I.; Dickie, G. Lymphoproliferative disease of the ocular adnexa: A clinical and pathologic study with statistical analysis of 69 patients. Ophthalmic Plast. Reconstr. Surg. 2005, 21, 177–188. [Google Scholar] [CrossRef]
- McKelvie, P.A.; McNab, A.; Francis, I.C.; Fox, R.; O’Day, J. Ocular adnexal lymphoproliferative disease: A series of 73 cases. Clin. Exp. Ophthalmol. 2001, 29, 387–393. [Google Scholar] [CrossRef]
- Fung, C.Y.; Tarbell, N.J.; Lucarelli, M.J.; Goldberg, S.I.; Linggood, R.M.; Harris, N.L.; Ferry, J.A. Ocular adnexal lymphoma: Clinical behavior of distinct World Health Organization classification subtypes. Int. J. Radiat. Oncol. Biol. Phys. 2003, 57, 1382–1391. [Google Scholar] [CrossRef]
- White, W.L.; Ferry, J.A.; Harris, N.L.; Grove, A.S. Ocular adnexal lymphoma. A clinicopathologic study with identification of lymphomas of mucosa-associated lymphoid tissue type. Ophthalmology 1995, 102, 1994–2006. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis | Immune Phenotype | Treatments before Ocular Malignant Location | |
|---|---|---|---|
| Case 1 | Pre-T cell leukemia/T commune (EGIL scoring of TII/TIII). At presentation before ocular involvement CD33,65,61,64,14,MPO Negative B lymphoid markers: CD19,22,79aic Negative CD56. Periocular biopsy: lymphoblasts positive for TdT, CD10, and express CD3 T lineage specific marker. | Chemotherapy GRAALL-2005 protocol (46). Induction: prophase comprising 1 mg/kg/d oral PDN and one IT-MTX, then VCR, DNR, CPM, PDN, L-Aspa; Triple IT (from day 1–day 14), then (from day 15) VCR, DNR, CPM, and L-Aspa, G-CSF (from D18). Consolidation with MRX, aracytine, and cranial irradiation. | |
| Chemotherapy GRAALL-2005 protocol (46). Induction: prophase comprising 1 mg/kg/d oral PDN and one IT-MTX, then VCR, DNR, CPM, PDN, L-Aspa; Triple IT (from day 1–day 14), then (from day 15) VCR, DNR, CPM, and L-Aspa, G-CSF (from D18). Consolidation with MRX, aracytine, and cranial irradiation. | |||
| Chemotherapy GRAALL-2005 protocol (46). Induction: prophase comprising 1 mg/kg/d oral PDN and one IT-MTX, then VCR, DNR, CPM, PDN, L-Aspa; Triple IT (from day 1–day 14), then (from day 15) VCR, DNR, CPM, and L-Aspa, G-CSF (from D18). Consolidation with MRX, aracytine and cranial irradiation. | |||
| Case 2 | IgG lambda multiple myeloma | monoclonal gammapathy: CD38+ CD56+ CD19± CD20± CD17− | Initial chemotherapy (VAD followed by DCEP) then autograft procedure.
|
| Case 3 | HGBL with rearrangements of MYC and BCL6 | Tumor cells were CD20(+), BCL6(+), BCL2(+), c-MYC+ CD10(–), MUM1(–), CD5(–), EBV(–) with Ki67 index at 85%. Rearrangements of BCL6 and MYC by FISH. | 4 cycles of immune-chemotherapy with R-CHOP (rituximab/CPM/doxorubicin/VCR/PDN) and MTX followed by high dose chemotherapy with BEAM (BCNU/etoposide/cytarabine/melphalan). R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) and methotrexate and then BEAM (BCNU, etoposide, cytarabine, melphalan). Second line therapy with R2-ICE (rituximab, ifosphamide, carboplatin, etoposide, and lenalidomide). |
| Case 4 | diffuse large B-cell NHL, R-IPI score 2 | At diagnosis: Bone marrow biopsy: hypercellular marrow (100%) with 90% involvement by CD20 positive large B-cell lymphoma. FISH for MYC, BCL2, and BCL-6 was negative. | data |
| Diagnostic imaging showed splenomegaly, lymphadenopathy on both sides of her diaphragm and pancytopenia. At diagnosis, she had an associated HLH as her presentation included fevers, splenomegaly, cytopenias, ferritin of 13,230, elevated triglycerides of 972, fibrinogen of 175, and an elevated soluble IL2 receptor level of 3903 | Vitrectomy biopsy: CD5 negative, CD10 negative, CD19 positive (variable/possibly partial), CD20 positive (variable/possibly partial), CD38 positive (moderate intensity), CD45 positive (slightly dim), kappa positive, and lambda negative. Also present are CD5 positive T cells. |
Salvage therapy with ESHAP ×2 Bridging chemotherapy with gemcitabine/oxaliplatin 3x cycles CAR T cell therapy. Lymphodepleting chemotherapy with fludarabine and cyclophosphamide
Polatuzumab and BR (3 cycles) | |
| Case 5 | ALL | pro-T-cell ALL CD2- surface CD3 intra CD3+ CD5- CD7+ CD19- CD33+ CD34+ CD123+ intra MPO+ | 1st line: chemotherapy according to FRALLE protocol 2nd line: nelarabine 3rd line: induction chemotherapy with idarubicine and cytarabine followed by an allogeneic peripheral blood stem cell transplantation with sequential conditioning regimen from a matched unrelated donor |
| Case 6 | ALL | poorly differentiated tumor infiltration of high-grade evoking a conjunctival localization of a myeloid sarcoma. Molecular biology: positive IDH1 mutation + duplication of the positive FLT3 gene |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denier, M.; Tick, S.; Dubois, R.; Dulery, R.; Eller, A.W.; Suarez, F.; Burroni, B.; Maurage, C.-A.; Bories, C.; Konopacki, J.; et al. Hidden in the Eyes—Recurrence of Systemic Hemopathies Reportedly “In Remission”: Six Cases and Review of Literature. Medicina 2022, 58, 456. https://doi.org/10.3390/medicina58030456
Denier M, Tick S, Dubois R, Dulery R, Eller AW, Suarez F, Burroni B, Maurage C-A, Bories C, Konopacki J, et al. Hidden in the Eyes—Recurrence of Systemic Hemopathies Reportedly “In Remission”: Six Cases and Review of Literature. Medicina. 2022; 58(3):456. https://doi.org/10.3390/medicina58030456
Chicago/Turabian StyleDenier, Margot, Sarah Tick, Romain Dubois, Remy Dulery, Andrew W. Eller, Felipe Suarez, Barbara Burroni, Claude-Alain Maurage, Claire Bories, Johanna Konopacki, and et al. 2022. "Hidden in the Eyes—Recurrence of Systemic Hemopathies Reportedly “In Remission”: Six Cases and Review of Literature" Medicina 58, no. 3: 456. https://doi.org/10.3390/medicina58030456
APA StyleDenier, M., Tick, S., Dubois, R., Dulery, R., Eller, A. W., Suarez, F., Burroni, B., Maurage, C.-A., Bories, C., Konopacki, J., Puech, M., Bouscary, D., Cantalloube, A., Héron, E., Marçais, A., Habas, C., Theillac, V., Keilani, C., Bonhomme, G. R., ... Errera, M.-H. (2022). Hidden in the Eyes—Recurrence of Systemic Hemopathies Reportedly “In Remission”: Six Cases and Review of Literature. Medicina, 58(3), 456. https://doi.org/10.3390/medicina58030456