
Comparison of Navigated Expandable Vertebral Cage with Conventional Expandable Vertebral Cage for Minimally Invasive Lumbar/Thoracolumbar Corpectomy

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Operation Procedure
2.2. Clinical Evaluation
2.3. Radiographic Evaluation
3. Results
3.1. Clinical Evaluation
3.2. Radiographic Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benson, D.R.B.; Bukus, J.K.; Montesano, P.X. Unstable thoracolumbar and lumbar burst fractures treated with the AO fixateur interne. J. Spinal Disord. 1992, 5, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Meves, R.; Avanzi, O. Correlation among canal compromise, neurologic deficit, and injury severity in thoracolumbar burst fractures. Spine 2006, 31, 2137–2141. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, T.; Jaiswal, A.; Tanaka, M.; Fujiwara, Y.; Oda, Y.; Arataki, S.; Misawa, H. Minimally Invasive L5 Corpectomy with Navigated Expandable Vertebral Cage: A Technical Note. Brain Sci. 2021, 11, 1241. [Google Scholar] [CrossRef] [PubMed]
- Wood, K.; Buttermann, G.; Mehbod, A.; Garvey, T.; Jhanjee, R.; Sechriest, V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J. Bone Jt. Surg. Am. 2003, 85, 773–781. [Google Scholar] [CrossRef]
- Tropiano, P.; Huang, R.C.; Louis, C.A.; Poitout, D.G.; Louis, R.P. Functional and radiographic outcome of thoracolumbar and lumbar burst fractures managed by closed orthopaedic reduction and casting. Spine 2003, 28, 2459–2465. [Google Scholar] [CrossRef]
- Patel, A.A.; Dailey, A.; Brodke, D.S.; Daubs, M.; Harrop, J.; Whang, P.G.; Vaccaro, A.R.; Spine Trauma Study Group. Thoracolumbar spine trauma classification: The Thoracolumbar Injury Classification and Severity Score system and case examples. J. Neurosurg. Spine 2009, 10, 201–206. [Google Scholar] [CrossRef]
- Kramer, D.L.; Rodgers, W.B.; Mansfield, F.L. Transpedicular instrumentation and short-segment fusion of thoracolumbar fractures: A prospective study using a single instrumentation system. J. Orthop. Trauma 1995, 9, 499–506. [Google Scholar] [CrossRef]
- Podet, A.G.; Morrow, K.D.; Robichaux, J.M.; Shields, J.A.; DiGiorgio, A.M.; Tender, G.C. Minimally invasive lateral corpectomy for thoracolumbar traumatic burst fractures. Neurosurg. Focus 2020, 49, E12. [Google Scholar] [CrossRef]
- Pannu, C.D.; Farooque, K.; Sharma, V.; Singal, D. Minimally invasive spine surgeries for treatment of thoracolumbar fractures of spine: A systematic review. J. Clin. Orthop. Trauma 2019, 10 (Suppl. S1), S147–S155. [Google Scholar] [CrossRef]
- Tanaka, M.; Fujiwara, Y.; Uotani, K.; Ayhan, S.; Yamauchi, T.; Sonawane, S.; Nakanishi, K. Minimally invasive thoracolumbar corpectomy with navigated expandable vertebral cage: A technical note. Interdiscip. Neurosurg. 2021, 24, 101123. [Google Scholar] [CrossRef]
- Holdsworth, F. Fractures, dislocations, and fracture-dislocations of the spine. J. Bone Jt. Surg. Am. 1970, 52, 1534–1551. [Google Scholar] [CrossRef]
- Denis, F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine 1983, 8, 817–831. [Google Scholar] [CrossRef] [PubMed]
- Rajasekaran, S. Thoracolumbar burst fractures without neurological deficit: The role for conservative treatment. Eur. Spine J. 2010, 19 (Suppl. S1), S40–S47. [Google Scholar] [CrossRef] [Green Version]
- Krompinger, W.J.; Fredrickson, B.E.; Mino, D.E.; Yuan, H.A. Conservative treatment of fractures of the thoracic and lumbar spine. Orthop. Clin. N. Am. 1986, 17, 161–170. [Google Scholar] [CrossRef]
- Cantor, J.; Lebwohl, N.; Garvey, T.; Eismont, F.J. Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine 1993, 18, 971–976. [Google Scholar] [CrossRef]
- Shen, W.J.; Shen, Y.S. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine 1999, 24, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Agus, H.; Kayali, C.; Arslantas, M. Nonoperative treatment of bursttype thoracolumbar vertebra fractures: Clinical and radiological results of 29 patients. Eur. Spine J. 2005, 14, 536–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajasekaran, S.; Kanna, R.M.; Shetty, A.P. Management of thoracolumbar spine trauma: An overview. Indian J. Orthop. 2015, 49, 72–82. [Google Scholar] [CrossRef]
- Yu, J.Y.H.; Fridley, J.; Gokaslan, Z.; Telfeian, A.; Oyelese, A.A. Minimally Invasive Thoracolumbar Corpectomy and Stabilization for Unstable Burst Fractures Using Intraoperative Computed Tomography and Computer-Assisted Spinal Navigation. World Neurosurg. 2019, 122, e1266–e1274. [Google Scholar] [CrossRef]
- Tanaka, M.; Singh, M.; Fujiwara, Y.; Uotani, K.; Arataki, S.; Yamauchi, T.; Nakanishi, K. Minimally invasive thoracolumbar corpectomy and percutaneous pedicle screw fixation with computer-assisted rod-bending system in single lateral position: Technical note. World Neurosurg. 2021, 151, 138–144. [Google Scholar] [CrossRef]
- Prod’homme, M.; Sans-Merce, M.; Pitteloud, N.; Damet, J.; Lascombes, P. Intraoperative 2D C-arm and 3D O-arm in children: A comparative phantom study. J. Child. Orthop. 2018, 12, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Theologis, A.A.; Tabaraee, E.; Toogood, P.; Kennedy, A.; Birk, H.; McClellan, R.T.; Pekmezci, M. Anterior corpectomy via the mini-open, extreme lateral, transpsoas approach combined with short-segment posterior fixation for single-level traumatic lumbar burst fractures: Analysis of health-related quality of life outcomes and patient satisfaction. J. Neurosurg. Spine 2016, 24, 60–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, H.; Barber, J.; Phan, E.; Hurley, R.K., Jr.; Javidan, Y. Minimally Invasive Lateral Corpectomy of the Thoracolumbar Spine: A Case Series of 20 Patients. Glob. Spine J. 2022, 12, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Smith, W.D.; Dakwar, E.; Le, T.V. Christian G, Serrano S, Uribe JS. Minimally invasive surgery for traumatic spinal pathologies: Mini-open, lateral approach in the thoracic and lumbar spine. Spine 2010, 35 (Suppl. S26), S338–S346. [Google Scholar] [CrossRef] [PubMed]
- Cappelletto, B.; Giorgiutti, F.; Balsano, M. Evaluation of the effectiveness of expandable cages for reconstruction of the anterior column of the spine. J. Orthop. Surg. 2020, 28, 2309499019900472. [Google Scholar] [CrossRef]
- Lau, D.; Song, Y.; Guan, Z.; La Marca, F.; Park, P. Radiological outcomes of static vs. expandable titanium cages after corpectomy: A retrospective cohort analysis of subsidence. Neurosurgery 2013, 72, 529–539; discussion 528–529. [Google Scholar] [CrossRef]
- Pekmezci, M.; McDonald, E.; Kennedy, A.; Dedini, R.; McClellan, T.; Ames, C.; Deviren, V. Can a novel rectangular footplate provide higher resistance to subsidence than circular footplates? An ex vivo biomechanical study. Spine 2012, 37, E1177–E1181. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Cage | Age (Year) | Patients | Follow Up (Month) |
|---|---|---|---|---|
| Group N | Navigated | 77.0 ± 5.5 | Man 1 Woman 10 | 31.9 ± 7.0 |
| Group C | Conventional | 76.2 ± 10.2 | Man 3 Woman 7 | 34.7 ± 9.5 |
| Group N (11 Cases) | Group C (10 Cases) | p Value | |
|---|---|---|---|
| Surgical time (min) | 234 ± 62 | 267 ± 90 | 0.438 |
| Blodd loss (mL) | 656 ± 325 | 786 ± 283 | 0.359 |
| Postoperative ODI (%) | 24.2 ± 6.5 | 27.2 ± 5.1 | 0.256 |
| Postoperative VAS (mm) | 22.9 ± 6.1 | 26.7 ± 7.8 | 0.243 |
| Complication | |||
| PJK | 1 | 1 | |
| Screw back out | 1 | ||
| Severe low back pain | 1 | ||
| Donar site infection | 1 | ||
| Another OVF | 1 | 1 |
| Group N (11 Cases) | Group C (10 Cases) | p Value | |
|---|---|---|---|
| AP cage mal-position (mm) | 2.7 ± 2.5 | 3.8 ± 4.4 | 0.525 |
| AP cage mal-angle (degree) | 1.3 ± 2.3 | 4.4 ± 4.9 | 0.079 |
| Cage sinking (mm) | 2.6 ± 4.0 | 4.2 ± 1.9 | 0.033 * |
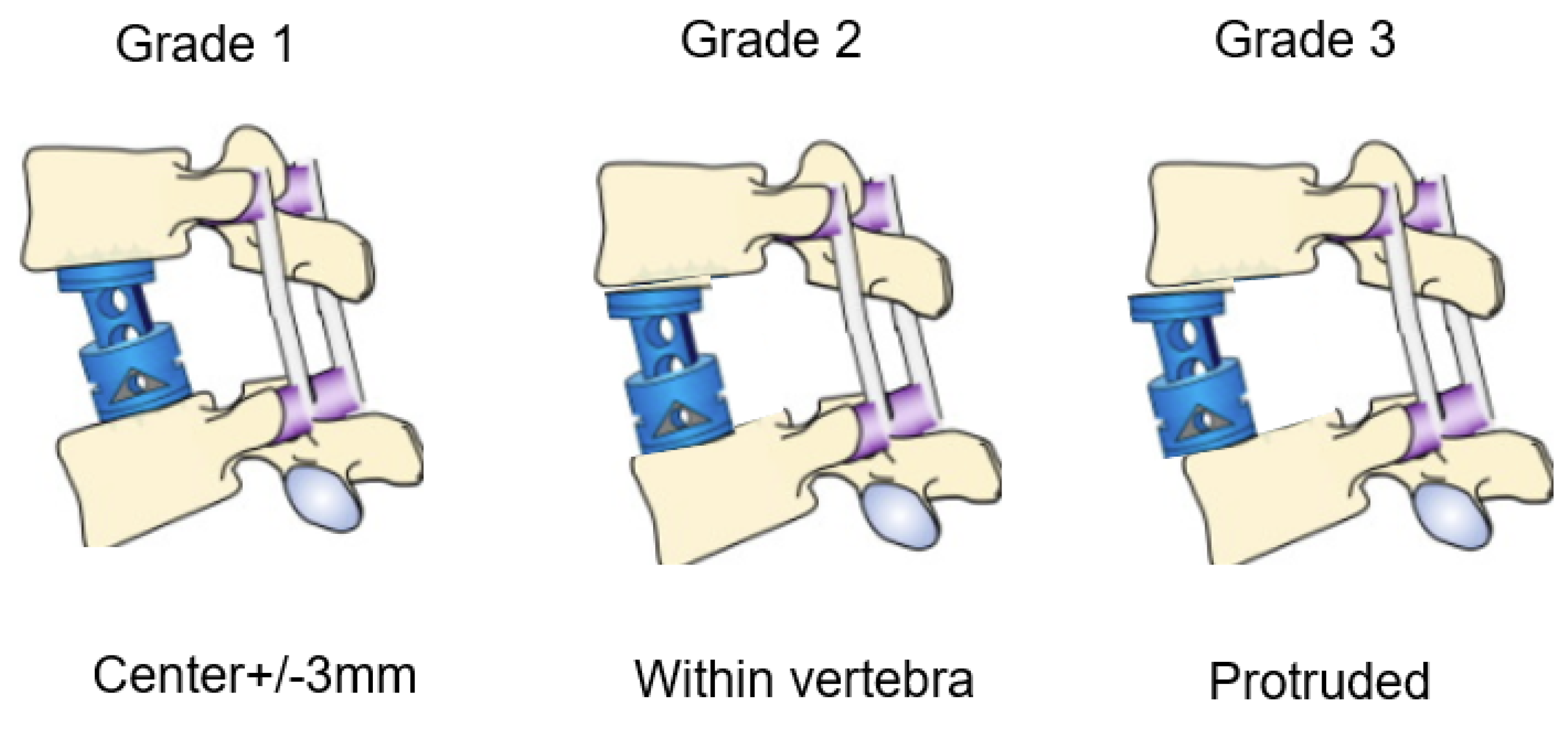
| Group N (11 Cases) | Group C (10 Cases) | Odds Ratio | |
|---|---|---|---|
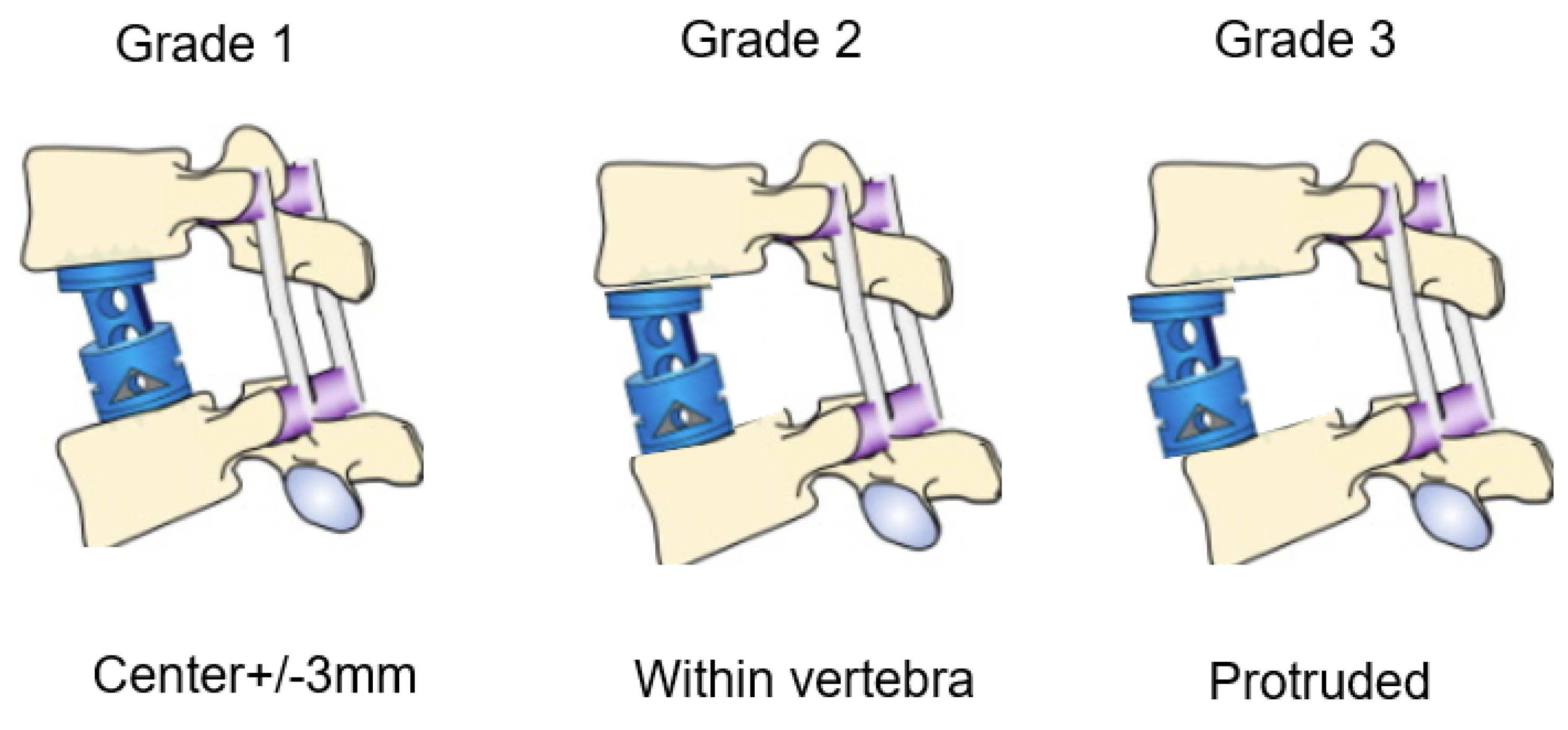
| Grade 1 | 9 | 5 | |
| Gdade 2 | 2 | 4 | |
| Grade 3 | 0 | 1 | |
| % Grade 1 | 82% | 50% | 4.5 |
| Authors | Number of Cases | Technique iCT/Fluoro | Cage C/N | Surgical Time (monute) | Blood Loss (mL) |
|---|---|---|---|---|---|
| Yu [19] | 11 | iCT | C | 396 | 541 |
| Tanaka [20] | 1 | iCT | C | 232 | 480 |
| Tanaka [10] | 1 | iCT | N | 150 | 120 |
| Yamauchi [3] | 1 | iCT | N | 215 | 750 |
| Theologis [21] | 12 | Fluoro | C | 289 (205–498) | 988 (50–3000) |
| Hai [22] | 20 | Fluoro | C | 276 | 558 |
| Smith [23] | 52 | Fluoro | C | 127 | 300 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, M.; Singh, M.; Fujiwara, Y.; Uotani, K.; Oda, Y.; Arataki, S.; Yamauchi, T.; Takigawa, T.; Ito, Y. Comparison of Navigated Expandable Vertebral Cage with Conventional Expandable Vertebral Cage for Minimally Invasive Lumbar/Thoracolumbar Corpectomy. Medicina 2022, 58, 364. https://doi.org/10.3390/medicina58030364
Tanaka M, Singh M, Fujiwara Y, Uotani K, Oda Y, Arataki S, Yamauchi T, Takigawa T, Ito Y. Comparison of Navigated Expandable Vertebral Cage with Conventional Expandable Vertebral Cage for Minimally Invasive Lumbar/Thoracolumbar Corpectomy. Medicina. 2022; 58(3):364. https://doi.org/10.3390/medicina58030364
Chicago/Turabian StyleTanaka, Masato, Mahendra Singh, Yoshihiro Fujiwara, Koji Uotani, Yoshiaki Oda, Shinya Arataki, Taro Yamauchi, Tomoyuki Takigawa, and Yasuo Ito. 2022. "Comparison of Navigated Expandable Vertebral Cage with Conventional Expandable Vertebral Cage for Minimally Invasive Lumbar/Thoracolumbar Corpectomy" Medicina 58, no. 3: 364. https://doi.org/10.3390/medicina58030364
APA StyleTanaka, M., Singh, M., Fujiwara, Y., Uotani, K., Oda, Y., Arataki, S., Yamauchi, T., Takigawa, T., & Ito, Y. (2022). Comparison of Navigated Expandable Vertebral Cage with Conventional Expandable Vertebral Cage for Minimally Invasive Lumbar/Thoracolumbar Corpectomy. Medicina, 58(3), 364. https://doi.org/10.3390/medicina58030364