
Respective Correction Rates of Lateral Lumbar Interbody Fusion and Percutaneous Pedicle Screw Fixation for Lumbar Degenerative Spondylolisthesis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Variables
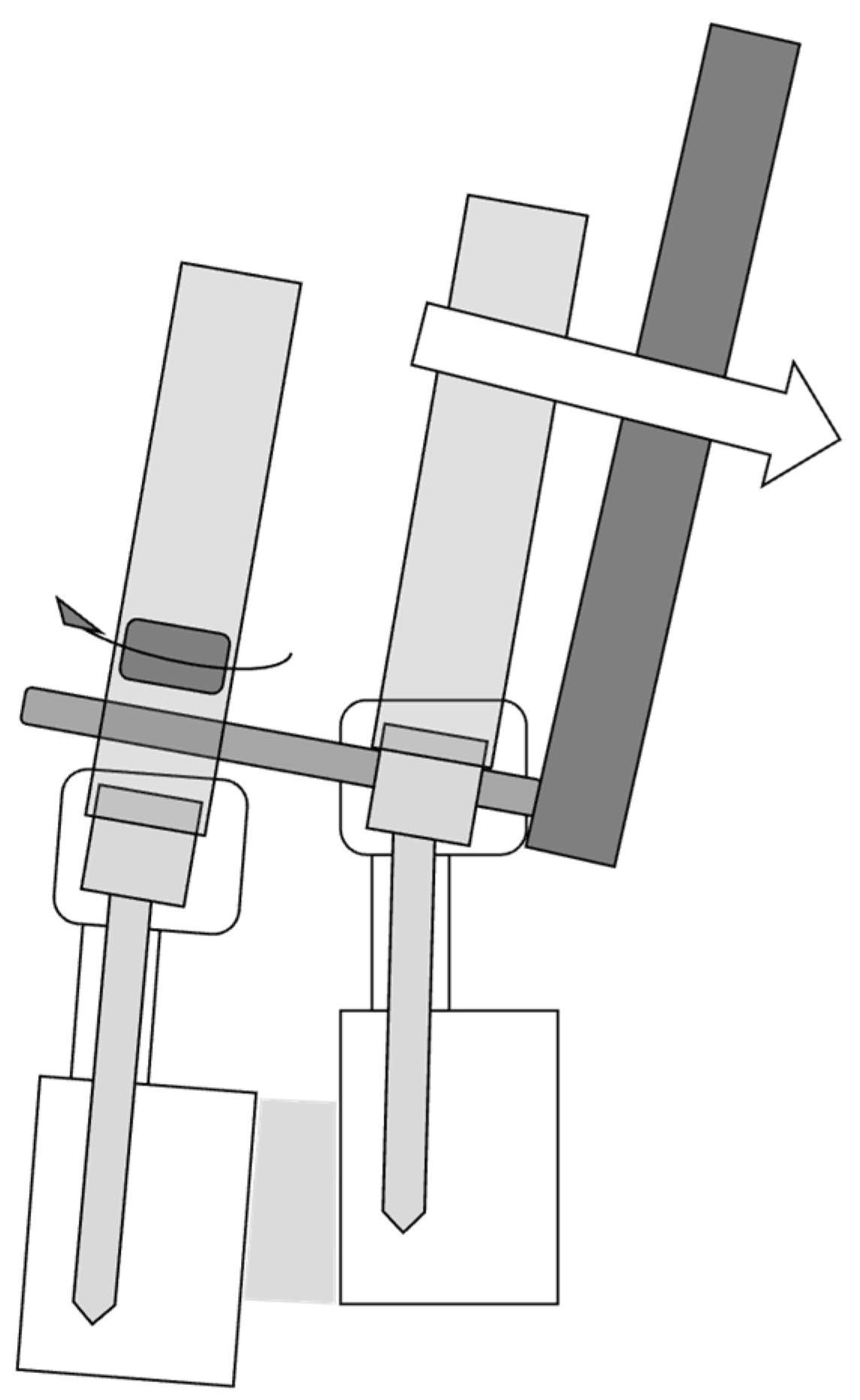
2.3. Surgical Technique
2.4. Statistical Analysis
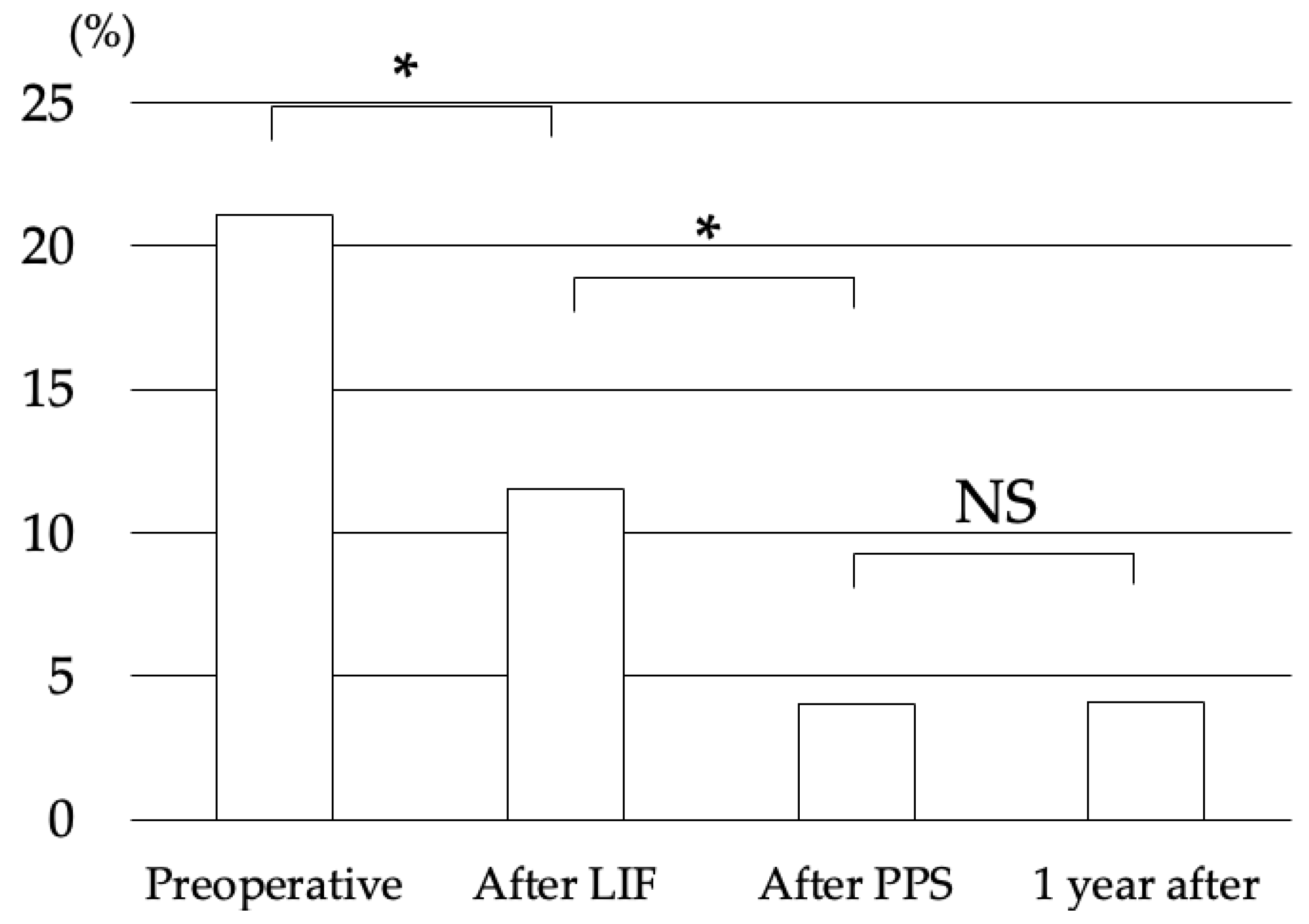
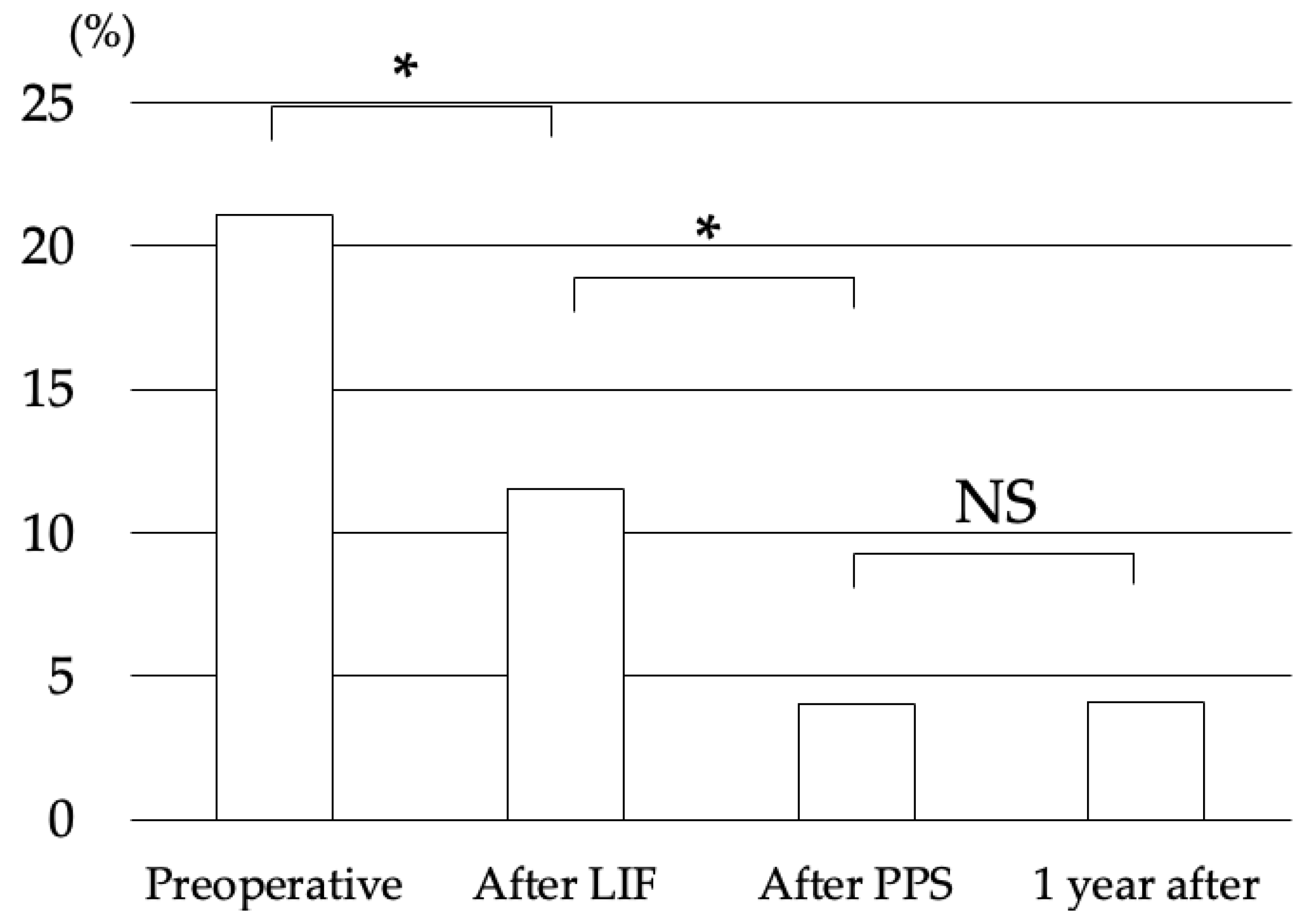
3. Results
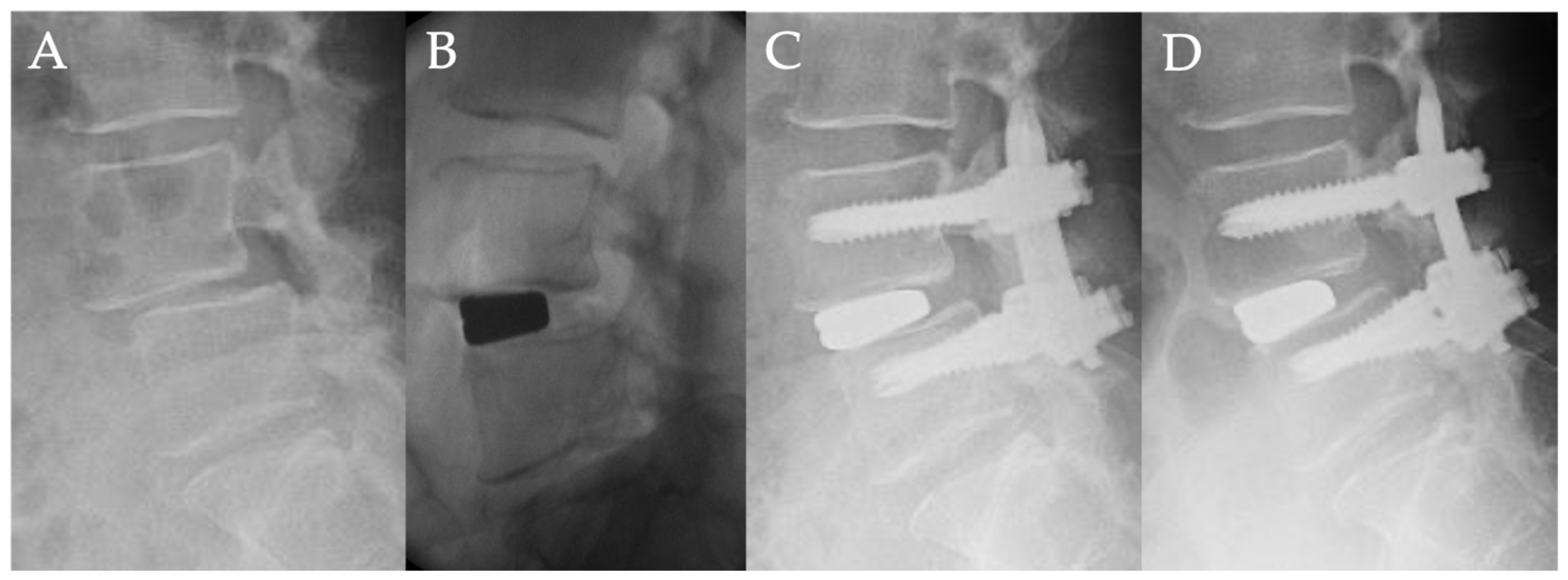
Case Presentation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sengupta, D.K.; Herkowitz, H.N. Degenerative spondylolisthesis: Review of current trends and controversies. Spine 2005, 30, S71–S81. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.X.J.; Kaplar, Z.; Deng, M.; Leung, J.C.S. Lumbar degenerative spondylolisthesis epidemiology: A systematic review with a focus on gender-specific and age-specific prevalence. J. Orthop. Translat. 2017, 11, 39–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, P.H. Spondylolisthesis, its cause and effect. Ann. R Coll. Surg. Engl. 1955, 16, 305–323. [Google Scholar] [PubMed]
- Malham, G.M.; Parker, R.M.; Goss, B.; Blecher, C.M.; Ballok, Z.E. Indirect foraminal decompression is independent of metabolically active facet arthropathy in extreme lateral interbody fusion. Spine 2014, 39, E1303–E1310. [Google Scholar] [CrossRef]
- Heo, D.H.; Jang, J.W.; Lee, J.K.; Park, C.K. Slippage reduction of lumbar spondylolisthesis using percutaneous pedicle screw with reduction fixation system after interbody fusion: A comparison with traditional open fusion and pedicle screw fixation. J. Clin. Neurosci. 2019, 67, 156–162. [Google Scholar] [CrossRef]
- Campbell, R.C.; Mobbs, R.J.; Lu, V.M.; Xu, J.; Rao, P.J.; Phan, K. Posterolateral Fusion Versus Interbody Fusion for Degenerative Spondylolisthesis: Systematic Review and Meta-Analysis. Glob. Spine J. 2017, 7, 482–490. [Google Scholar] [CrossRef] [Green Version]
- Isaacs, R.E.; Sembrano, J.N.; Tohmeh, A.G.; Group SDS. Two-Year Comparative Outcomes of MIS Lateral and MIS Transforaminal Interbody Fusion in the Treatment of Degenerative Spondylolisthesis: Part II: Radiographic Findings. Spine 2016, 41 (Suppl. S8), S133–S144. [Google Scholar] [CrossRef]
- Lu, V.M.; Kerezoudis, P.; Gilder, H.E.; McCutcheon, B.A.; Phan, K.; Bydon, M. Minimally Invasive Surgery Versus Open Surgery Spinal Fusion for Spondylolisthesis: A Systematic Review and Meta-analysis. Spine 2017, 42, E177–E185. [Google Scholar] [CrossRef]
- Musluman, A.M.; Yilmaz, A.; Cansever, T.; Cavusoglu, H.; Colak, I.; Genc, H.A.; Aydın, Y. Posterior lumbar interbody fusion versus posterolateral fusion with instrumentation in the treatment of low-grade isthmic spondylolisthesis: Midterm clinical outcomes. J. Neurosurg. Spine. 2011, 14, 488–496. [Google Scholar] [CrossRef] [Green Version]
- Galbusera, F.; Volkheimer, D.; Reitmaier, S.; Berger-Roscher, N.; Kienle, A.; Wilke, H.J. Pedicle screw loosening: A clinically relevant complication? Eur. Spine J. 2015, 24, 1005–1016. [Google Scholar] [CrossRef]
- Boos, N.; Webb, J.K. Pedicle screw fixation in spinal disorders: A European view. Eur. Spine J. 1997, 6, 2–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, B.R.; Grob, D.; Dvorak, J.; Muntener, M. Posterior surgical approach to the lumbar spine and its effect on the multifidus muscle. Spine 1997, 22, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, K.; Christensen, F.B.; Eiskjaer, S.P.; Hansen, E.S.; Fruensgaard, S.; Bunger, C.E. 1997 Volvo Award winner in clinical studies. The effect of pedicle screw instrumentation on functional outcome and fusion rates in posterolateral lumbar spinal fusion: A prospective, randomized clinical study. Spine 1997, 22, 2813–2822. [Google Scholar] [CrossRef] [PubMed]
- Mobbs, R.J.; Sivabalan, P.; Li, J. Minimally invasive surgery compared to open spinal fusion for the treatment of degenerative lumbar spine pathologies. J. Clin. Neurosci. 2012, 19, 829–835. [Google Scholar] [CrossRef]
- Foley, K.T.; Gupta, S.K.; Justis, J.R.; Sherman, M.C. Percutaneous pedicle screw fixation of the lumbar spine. Neurosurg. Focus. 2001, 10, E10. [Google Scholar] [CrossRef]
- Oliveira, L.; Marchi, L.; Coutinho, E.; Pimenta, L. A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements. Spine 2010, 35, S331–S337. [Google Scholar] [CrossRef] [Green Version]
- Khajavi, K.; Shen, A.; Lagina, M.; Hutchison, A. Comparison of clinical outcomes following minimally invasive lateral interbody fusion stratified by preoperative diagnosis. Eur. Spine J. 2015, 24 (Suppl. S3), 322–330. [Google Scholar] [CrossRef]
- Lian, X.F.; Hou, T.S.; Xu, J.G.; Zeng, B.F.; Zhao, J.; Liu, X.K.; Zhao, C.; Li, H. Posterior lumbar interbody fusion for aged patients with degenerative spondylolisthesis: Is intentional surgical reduction essential? Spine J. 2013, 13, 1183–1189. [Google Scholar] [CrossRef]
- Wegmann, K.; Gundermann, S.; Siewe, J.; Eysel, P.; Delank, K.S.; Sobottke, R. Correlation of reduction and clinical outcome in patients with degenerative spondylolisthesis. Arch. Orthop. Trauma. Surg. 2013, 133, 1639–1644. [Google Scholar] [CrossRef]
- Takahashi, Y.; Funao, H.; Yoshida, K.; Sasao, Y.; Nishiyama, M.; Isogai, N.; Ishii, K. Sequential MRI Changes After Lateral Lumbar Interbody Fusion in Spondylolisthesis with Mild and Severe Lumbar Spinal Stenosis. World Neurosurg. 2021, 152, e289–e296. [Google Scholar] [CrossRef]
- Goyal, A.; Kerezoudis, P.; Alvi, M.A.; Goncalves, S.; Bydon, M. Outcomes following minimally invasive lateral transpsoas interbody fusion for degenerative low grade lumbar spondylolisthesis: A systematic review. Clin. Neurol. Neurosurg. 2018, 167, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Ishii, K.; Isogai, N.; Shiono, Y.; Yoshida, K.; Takahashi, Y.; Takeshima, K.; Nakayama, M.; Funao, H. Contraindication of Minimally Invasive Lateral Interbody Fusion for Percutaneous Reduction of Degenerative Spondylolisthesis: A New Radiographic Indicator of Bony Lateral Recess Stenosis Using I Line. Asian Spine J. 2021, 15, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Rajpal, S.; Resnick, D.K. Rod cantilever techniques. Neurosurgery 2008, 63, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.S.; Park, J.Y.; Kim, K.H.; Kuh, S.U.; Chin, D.K.; Kim, K.S.; Cho, Y.E. Minimally invasive transforaminal lumbar interbody fusion with unilateral pedicle screw fixation: Comparison between primary and revision surgery. Biomed. Res. Int. 2014, 2014, 919248. [Google Scholar] [CrossRef] [PubMed]
- El Saman, A.; Meier, S.; Sander, A.; Kelm, A.; Marzi, I.; Laurer, H. Reduced loosening rate and loss of correction following posterior stabilization with or without PMMA augmentation of pedicle screws in vertebral fractures in the elderly. Eur. J. Trauma. Emerg. Surg. 2013, 39, 455–460. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Age (y/o) | 64.7 ± 6.4 (44–90) |
| Gender | Male 17/Female 33 |
| Height (m) | 1.58 ± 0.10 (1.43–1.84) |
| Weight (kg) BMI (kg/m2) | 56 ± 11 (36–85) 22.3 ± 3.1 (16.2–30.3) |
| Meyerding classification Mean preoperative % slip (%) Preoperative JOA score (Pts) Final JOA score (Pts) | Grade 1: 35/Grade 2: 15 21.1 ± 7.0 14.7 ± 4.2 27.7 ± 1.7 |
| Pre-Operation | Final | p-Value | |
|---|---|---|---|
| Pelvic Incidence (°) | 53.1 ± 8.7 | ||
| Lumbar Lordosis (°) | 40.0 ± 14.3 | 43.3 ± 12.4 | 0.41 |
| Pelvic Tilt (°) | 25.6 ± 10.9 | 22.2 ± 11.0 | 0.30 |
| Sagittal Vertical Axis (mm) | 38.2 ± 27.2 | 39.9 ± 25.3 | 0.84 |
| Local Lordosis (°) | 7.5 ± 4.9 | 10.0 ± 5.9 | 0.14 |
| Lateral Interbody Fusion | Percutaneous Pedicle Screw | |||
|---|---|---|---|---|
| Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | |
| Pelvic Incidence | 0.04 | 0.85 | −0.39 | 0.07 |
| Lumbar Lordosis | 0.15 | 0.49 | 0.03 | 0.90 |
| Pelvic Tilt | −0.06 | 0.77 | −0.26 | 0.24 |
| Sagittal Vertical Axis | −0.31 | 0.17 | 0.21 | 0.35 |
| Local Lordosis | 0.01 | 0.97 | 0.27 | 0.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isogai, N.; Yoshida, K.; Shiono, Y.; Sasao, Y.; Funao, H.; Ishii, K. Respective Correction Rates of Lateral Lumbar Interbody Fusion and Percutaneous Pedicle Screw Fixation for Lumbar Degenerative Spondylolisthesis. Medicina 2022, 58, 169. https://doi.org/10.3390/medicina58020169
Isogai N, Yoshida K, Shiono Y, Sasao Y, Funao H, Ishii K. Respective Correction Rates of Lateral Lumbar Interbody Fusion and Percutaneous Pedicle Screw Fixation for Lumbar Degenerative Spondylolisthesis. Medicina. 2022; 58(2):169. https://doi.org/10.3390/medicina58020169
Chicago/Turabian StyleIsogai, Norihiro, Kodai Yoshida, Yuta Shiono, Yutaka Sasao, Haruki Funao, and Ken Ishii. 2022. "Respective Correction Rates of Lateral Lumbar Interbody Fusion and Percutaneous Pedicle Screw Fixation for Lumbar Degenerative Spondylolisthesis" Medicina 58, no. 2: 169. https://doi.org/10.3390/medicina58020169
APA StyleIsogai, N., Yoshida, K., Shiono, Y., Sasao, Y., Funao, H., & Ishii, K. (2022). Respective Correction Rates of Lateral Lumbar Interbody Fusion and Percutaneous Pedicle Screw Fixation for Lumbar Degenerative Spondylolisthesis. Medicina, 58(2), 169. https://doi.org/10.3390/medicina58020169