
Doppler Echocardiography-Guided Heart Rate Modulation Therapy Using Ivabradine in a Patient with Systolic Heart Failure



{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
2.1. Before Referral
2.2. After the Discharge
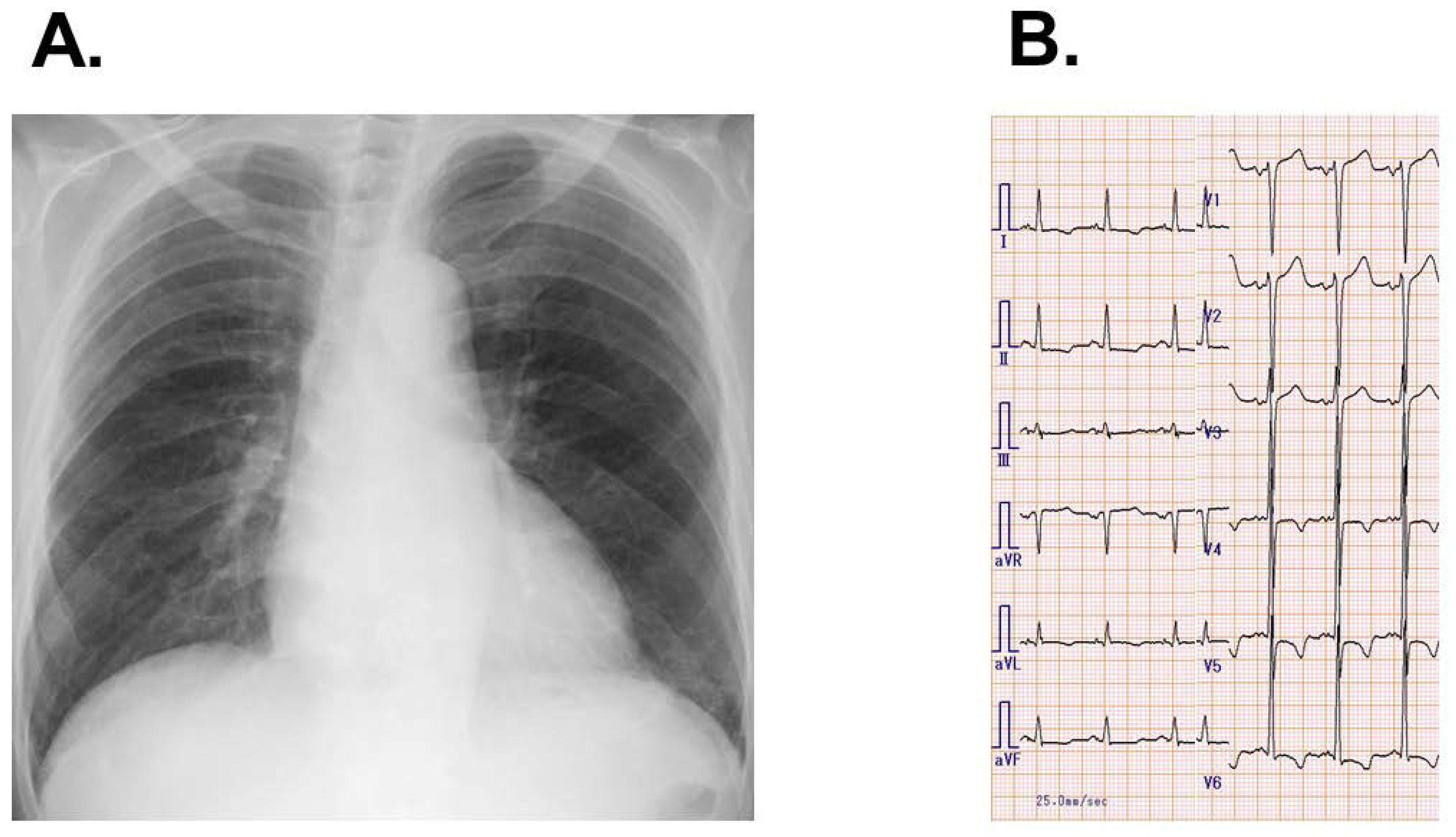
2.3. On Referral
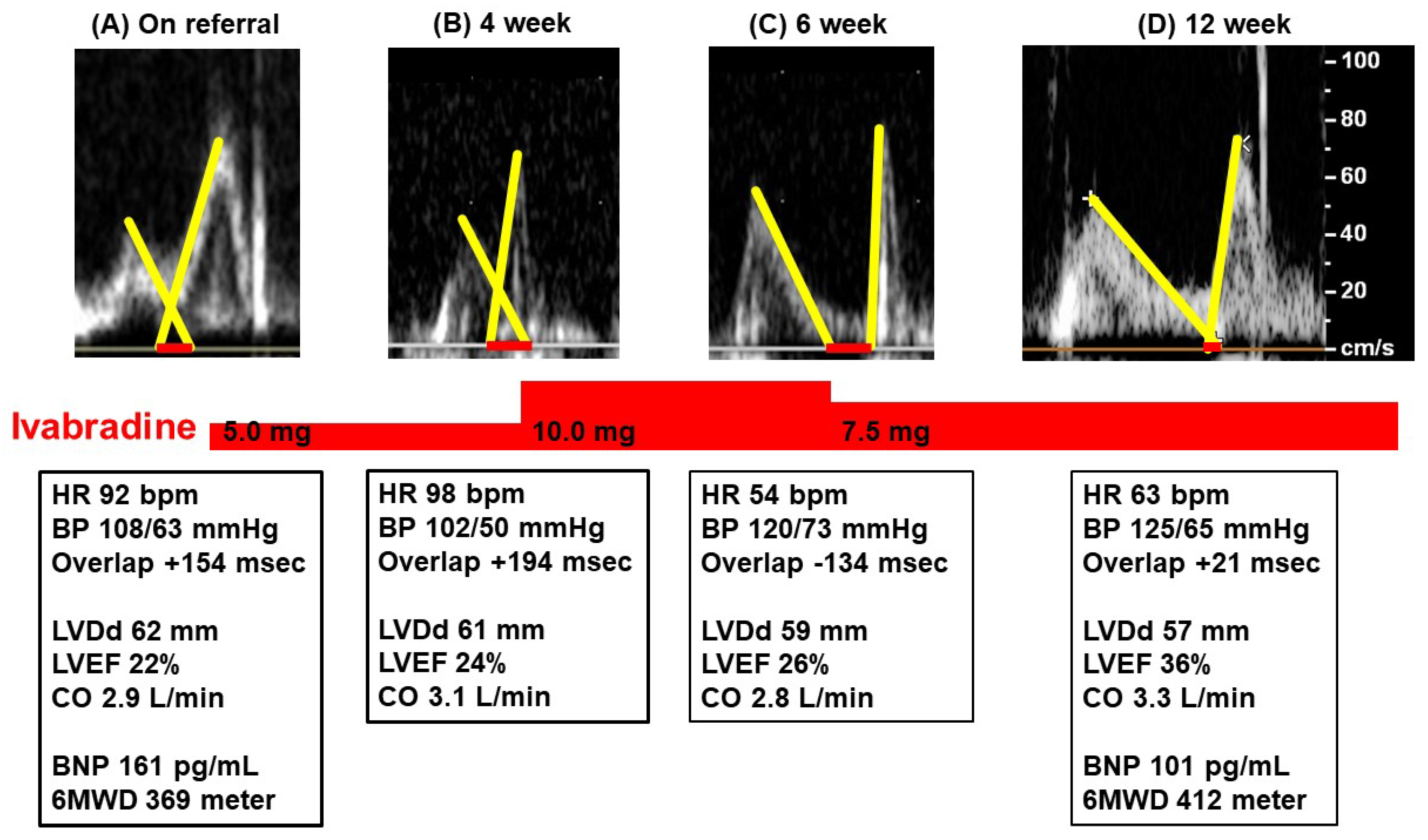
2.4. Follow-Up
3. Discussion
3.1. Ideal Heart Rate
3.2. Aggressive Heart Rate Modulation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Koruth, J.S.; Lala, A.; Pinney, S.; Reddy, V.Y.; Dukkipati, S.R. The Clinical Use of Ivabradine. J. Am. Coll. Cardiol. 2017, 70, 1777–1784. [Google Scholar] [CrossRef] [PubMed]
- Swedberg, K.; Komajda, M.; Bohm, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L. Ivabradine and outcomes in chronic heart failure (SHIFT): A randomised placebo-controlled study. Lancet 2010, 376, 875–885. [Google Scholar] [CrossRef]
- Izumida, T.; Imamura, T.; Nakamura, M.; Fukuda, N.; Kinugawa, K. How to consider target heart rate in patients with systolic heart failure. ESC Heart Fail. 2020, 7, 3231–3234. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, A.; Iwama, K.; Makise, N.; Domoto, Y.; Ishida, J.; Morita, H.; Komuro, I. Use of a Non-invasive Cardiac Output Measurement in a Patient with Low-output Dilated Cardiomyopathy. Intern. Med. 2020, 59, 1525–1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izumida, T.; Imamura, T.; Ueno, Y.; Tanaka, S.; Kataoka, N.; Nakamura, M.; Kinugawa, K. Impact of optimal heart rate on left ventricular reverse remodeling and functional improvement in patients with systolic heart failure. Heart Vessel. 2021, 36, 1688–1693. [Google Scholar] [CrossRef] [PubMed]
- Hori, M.; Imamura, T.; Narang, N.; Kinugawa, K. Implications of Doppler Echocardiography-guided Heart Rate Modulation Using Ivabradine. Intern. Med. 2021, 60, 3873–3877. [Google Scholar] [CrossRef] [PubMed]
- Imamura, T.; Hori, M.; Narang, N.; Besser, S.; Kinugawa, K. Prognostic implications of mitral valve inflow pattern overlap during ivabradine therapy. Int. Heart J. 2021; in press. [Google Scholar]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, T.; Kinugawa, K. Doppler Echocardiography-Guided Heart Rate Modulation Therapy Using Ivabradine in a Patient with Systolic Heart Failure. Medicina 2022, 58, 164. https://doi.org/10.3390/medicina58020164
Imamura T, Kinugawa K. Doppler Echocardiography-Guided Heart Rate Modulation Therapy Using Ivabradine in a Patient with Systolic Heart Failure. Medicina. 2022; 58(2):164. https://doi.org/10.3390/medicina58020164
Chicago/Turabian StyleImamura, Teruhiko, and Koichiro Kinugawa. 2022. "Doppler Echocardiography-Guided Heart Rate Modulation Therapy Using Ivabradine in a Patient with Systolic Heart Failure" Medicina 58, no. 2: 164. https://doi.org/10.3390/medicina58020164
APA StyleImamura, T., & Kinugawa, K. (2022). Doppler Echocardiography-Guided Heart Rate Modulation Therapy Using Ivabradine in a Patient with Systolic Heart Failure. Medicina, 58(2), 164. https://doi.org/10.3390/medicina58020164