
A Review of Neovascular Glaucoma: Etiology, Pathogenesis, Diagnosis, and Treatment



Abstract
1. Introduction
2. Prevalence and Etiology
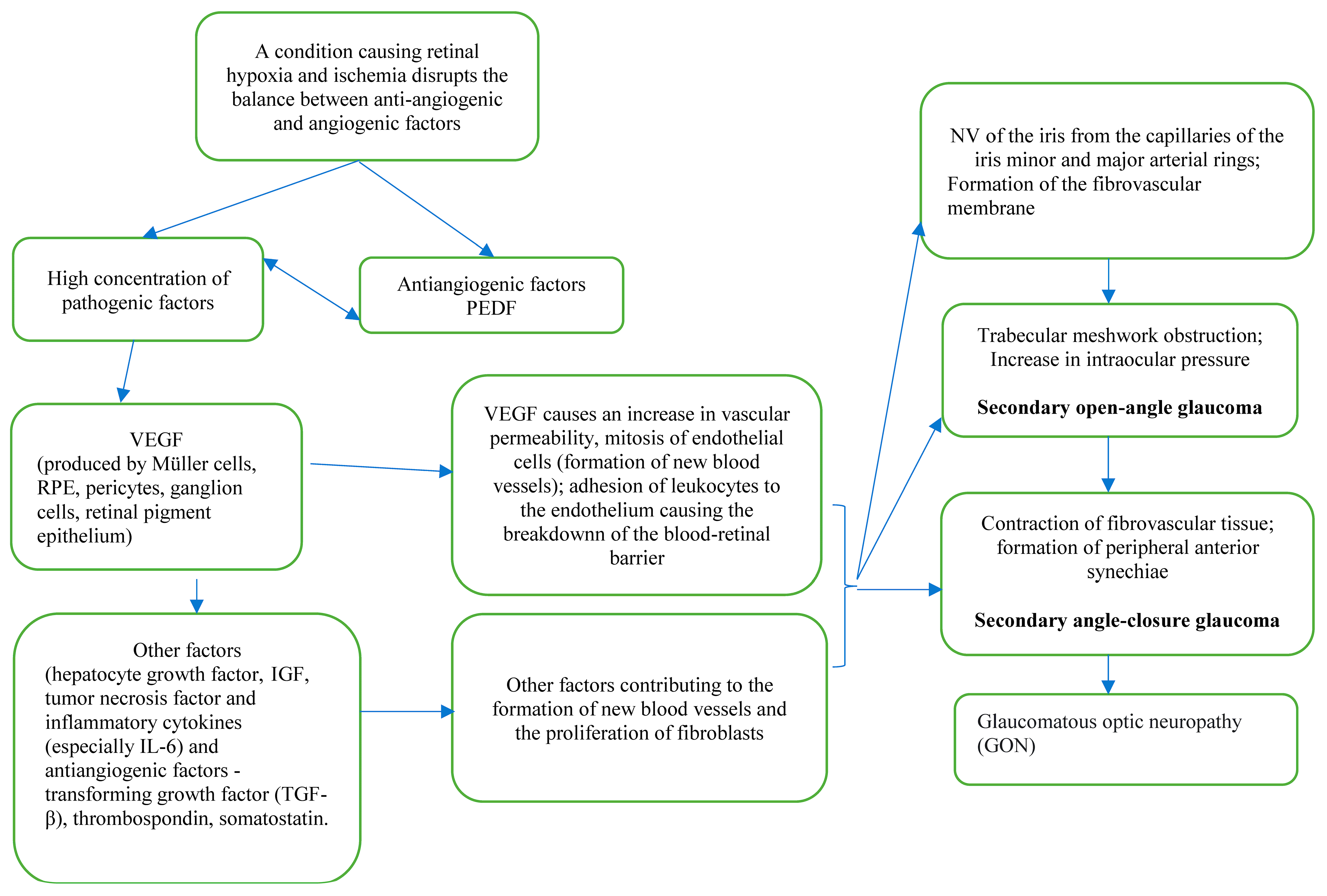
3. Pathogenesis
4. Clinical Profile
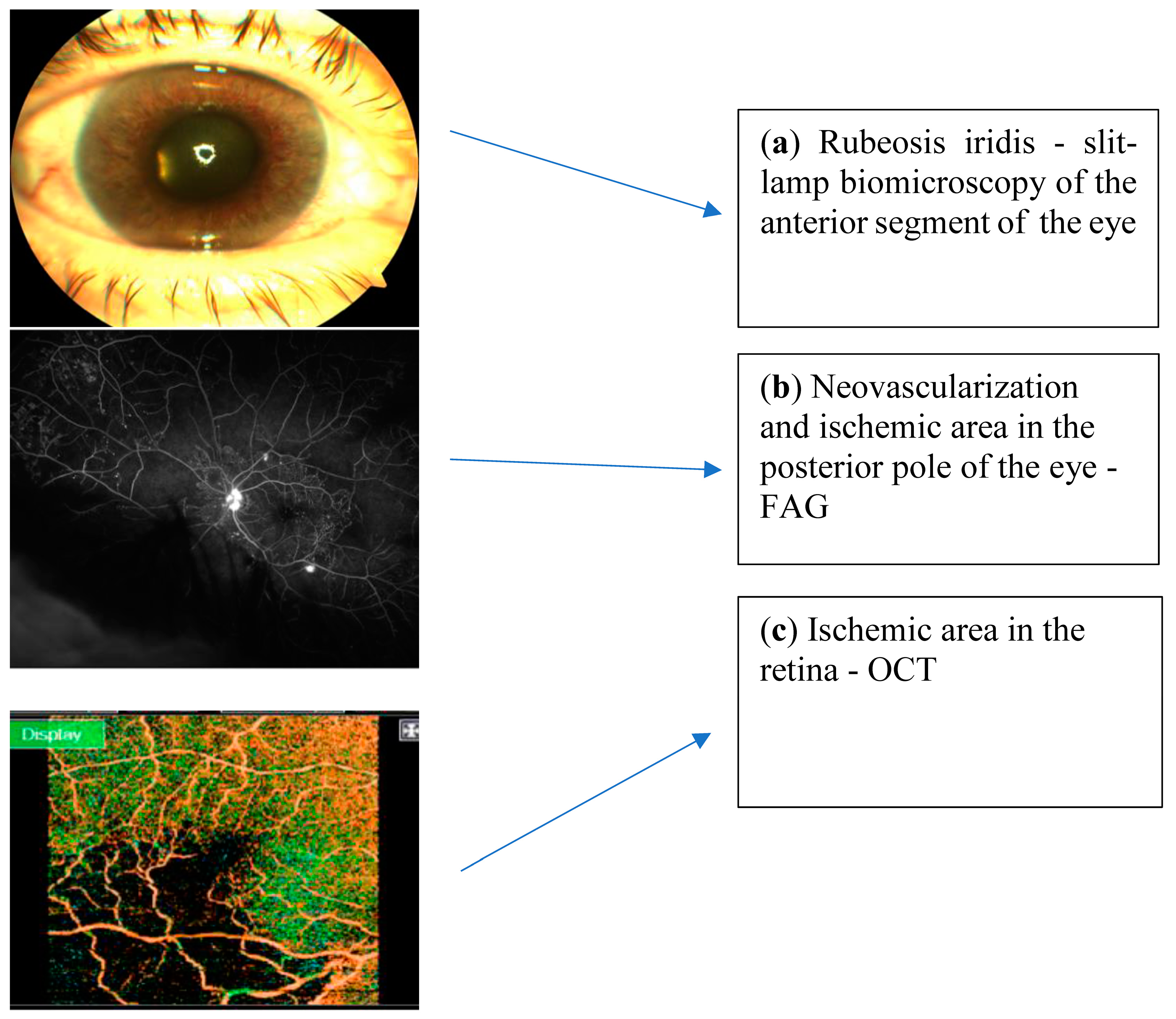
5. Ophthalmic Diagnostics
6. Treatment
6.1. Treating the Underlying Pathology
6.2. The Management of Intraocular Pressure
6.2.1. Pharmacological Treatment
- (1)
- Prostaglandins—increases fluid leakage through trabecular and uveoscleral pathways, so their effectiveness is questionable; contraindicated when the inflammation is observed.
- (2)
- Anti-cholinergics are contraindicated because of an increase in inflammation and also cause miosis due to further forward movement of the iris lens diaphragm, increasing the anterior chamber angle-closure and reducing uveoscleral leakage [20].
6.2.2. Surgical Treatment
- valuable visual acuity (VA) >0.05;
- insufficient maximum pharmacological control of IOP: >50% of NVG patients
- closed anterior chamber angle due to synechiae.
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schuster, A.K.; Erb, C.; Hoffmann, E.M.; Dietlein, T.; Pfeiffer, N. The Diagnosis and Treatment of Glaucoma. Dtsch. Arztebl. Int. 2020, 117, 225. [Google Scholar] [CrossRef]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Senthil, S.; Dada, T.; Das, T.; Kaushik, S.; Puthuran, G.; Philip, R.; Rani, P.K.; Rao, H.; Singla, S.; Vijaya, L. Neovascular glaucoma—A review. Indian J. Ophthalmol. 2021, 69, 525–535. [Google Scholar] [CrossRef]
- Havens, S.J.; Gulati, V. Neovascular Glaucoma. Dev. Ophthalmol. 2016, 55, 196–204. [Google Scholar]
- Weiss, D.I.; Shaffer, R.N.; Nehrenberg, T.R. Neovascular Glaucoma Complicating Carotid-Cavernous Fistula. Arch. Ophthalmol. 1963, 69, 304–307. [Google Scholar] [CrossRef]
- Kumar, S.; Kumari, S.; Sinha, A.K.; Kumar, S.; Kumari, S.; Sinha, A.K. Neovascular Glaucoma: An Update on Etiopathogenesis, Diagnostics and Management. Open J. Ophthalmol. 2022, 12, 242–258. [Google Scholar] [CrossRef]
- Esponda-Lammoglia, C.; Castaneda-Díez, R.; García-Aguirre, G.; Albis-Donado, O.; Jiménez-Román, J. Neovascular Glaucoma. In Glaucoma—Basic and Clinical Aspects; S. Rumelt: London, UK, 2013; p. 522. [Google Scholar]
- Haefiiger, I.O.; Zschauer, A.; Anderson, D.R. Relaxation of retinal pericyte contractile tone through the nitric oxide-cyclic guanosine monophosphate pathway. Investig. Ophthalmol. Vis. Sci. 1994, 35, 991–997. [Google Scholar]
- Cabral, T.; Mello, L.G.M.; Lima, L.H.; Polido, J.; Regatieri, C.V.; Belfort, R.; Mahajan, V.B. Retinal and choroidal angiogenesis: A review of new targets. Int. J. Retin. Vitr. 2017, 3, 31. [Google Scholar] [CrossRef]
- Olmos, L.C.; Lee, R.K. Medical and Surgical Treatment of Neovascular Glaucoma. Int. Ophthalmol. Clin. 2011, 51, 27. [Google Scholar] [CrossRef]
- Iwasaki, K.; Kojima, S.; Wajima, R.; Okazaki, T.; Yokoyama, Y.; Inoue, T.; Higashide, T.; Miki, A.; Nakazawa, T.; Inatani, M. Comparing Surgical Outcomes in Neovascular Glaucoma between Tube and Trabeculectomy: A Multicenter Study. Ophthalmol. Glaucoma 2022, 5, 672–680. [Google Scholar] [CrossRef]
- Yu, T.C.; Tseng, G.L.; Chen, C.C.; Liou, S.W. Surgical treatment of neovascular glaucoma with Ex-PRESS glaucoma shunt. Medicine 2017, 96, e7845. [Google Scholar] [CrossRef] [PubMed]
- Pandya, K.H.; Tewari, A.; Shingleton, B.; Ahmed, K.I.; Khan, U.B.; Hasanee, K.; Freudenthal, J. Neovascular Glaucoma Clinical Presentation: History, Physical, Causes. Medscape Drugs&Diseases>Ophthalmology. 19 May 2020, p. ePub. Available online: https://emedicine.medscape.com/article/1205736-overview (accessed on 14 September 2022).
- Fernández-Vigo, J.; Castro, J.; Macarro, A. Diabetic iris neovascularization. Natural history and treatment. Acta Ophthalmol. Scand. 1997, 75, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Bourne, R.R.A.; Steinmetz, J.D.; Saylan, M.; Mersha, A.M.; Weldemariam, A.H.; Wondmeneh, T.G.; Sreeramareddy, C.T.; Pinheiro, M.; Yaseri, M.; Yu, C.; et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet. Glob. Heal. 2021, 9, e144–e160. [Google Scholar]
- Chen, H.F.; Chen, M.C.; Lai, C.C.; Yeung, L.; Wang, N.K.; Chen, H.S.L.; Ku, W.C.; Wu, S.C.; Chang, S.H.L.; Chuang, L.H. Neovascular glaucoma after central retinal vein occlusion in pre-existing glaucoma. BMC Ophthalmol. 2014, 14, 119. [Google Scholar] [CrossRef]
- De Vasconcellos, J.P.C.; Costa, V.P.; Kara-José, N. Neovascular glaucoma: Epidemiology and prognostic factors. Proposal of a flow chart to guide the treatment. Arq. Bras. Oftalmol. 1998, 61, 519–524. [Google Scholar]
- Dumbrăveanu, L.; Cușnir, V.; Bobescu, D. A review of neovascular glaucoma. Etiopathogenesis and treatment. Rom. J. Ophthalmol. 2021, 65, 315–329. [Google Scholar]
- Ajayi, I.A.; Omotoye, O.; Ajite, K.; Abah, E. Presentation, etiology and treatment outcome of neovascular glaucoma in Ekiti state, South Western Nigeria. Afr. Health Sci. 2021, 21, 1266. [Google Scholar] [CrossRef]
- Rodrigues, G.B.; Abe, R.Y.; Zangalli, C.; Sodre, S.L.; Donini, F.A.; Costa, D.C.; Leite, A.; Felix, J.P.; Torigoe, M.; Diniz-Filho, A.; et al. Neovascular glaucoma: A review. Int. J. Retin. Vitr. 2016, 2, 26. [Google Scholar] [CrossRef]
- Călugăru, D.; Călugăru, M. Etiology, pathogenesis, and diagnosis of neovascular glaucoma. Int. J. Ophthalmol. 2022, 15, 1005. [Google Scholar] [CrossRef]
- Barac, I.R.; Pop, M.D.; Gheorghe, A.I.; Taban, C. Neovascular secondary glaucoma, etiology and pathogenesis. Rom. J. Ophthalmol. 2015, 59, 24. [Google Scholar]
- Wang, J.W.; Zhou, M.W.; Zhang, X.; Huang, W.B.; Gao, X.B.; Wang, W.; Chen, S.; Zhang, X.Y.; Ding, X.Y.; Jonas, J.B. Short-term effect of intravitreal ranibizumab on intraocular concentrations of vascular endothelial growth factor-A and pigment epithelium-derived factor in neovascular glaucoma. Clin. Experiment. Ophthalmol. 2015, 43, 415–421. [Google Scholar] [CrossRef]
- Aiello, L.P.; Avery, R.L.; Arrigg, P.G.; Keyt, B.A.; Jampel, H.D.; Shah, S.T.; Pasquale, L.R.; Thieme, H.; Iwamoto, M.A.; Park, J.E.; et al. Vascular Endothelial Growth Factor in Ocular Fluid of Patients with Diabetic Retinopathy and Other Retinal Disorders. N. Engl. J. Med. 1994, 331, 1480–1487. [Google Scholar] [CrossRef]
- Chalam, K.V.; Brar, V.S.; Murthy, R.K. Human Ciliary Epithelium as a Source of Synthesis and Secretion of Vascular Endothelial Growth Factor in Neovascular Glaucoma. JAMA Ophthalmol. 2014, 132, 1350–1354. [Google Scholar] [CrossRef]
- Tolentino, M.J.; Miller, J.W.; Gragoudas, E.S.; Chatzistefanou, K.; Ferrara, N.; Adamis, A.P. Vascular Endothelial Growth Factor Is Sufficient to Produce Iris Neovascularization and Neovascular Glaucoma in a Nonhuman Primate. Arch. Ophthalmol. 1996, 114, 964–970. [Google Scholar] [CrossRef]
- Yu, X.B.; Sun, X.H.; Dahan, E.; Guo, W.Y.; Qian, S.H.; Meng, F.R.; Song, Y.L.; Simon, G.J.B. Increased levels of transforming growth factor-betal and -beta2 in the aqueous humor of patients with neovascular glaucoma. Ophthalmic Surg. Lasers Imaging 2007, 38, 6–14. [Google Scholar] [CrossRef]
- Tripathi, R.C.; Borisuth, N.S.C.; Tripathi, B.J. Detection, quantification, and significance of basic fibroblast growth factor in the aqueous humor of man, cat, dog and pig. Exp. Eye Res. 1992, 54, 447–454. [Google Scholar] [CrossRef]
- Shazly, T.A.; Latina, M.A. Neovascular glaucoma: Etiology, diagnosis and prognosis. Semin. Ophthalmol. 2009, 24, 113–121. [Google Scholar] [CrossRef]
- Mosaed, S.; Minckler, D. Neovascular Glaucoma. In Clinical Glaucoma Care; Springer: New York, NY, USA, 2022; pp. 361–373. [Google Scholar]
- Yazdani, S.; Hendi, K.; Pakravan, M. Intravitreal bevacizumab (Avastin) injection for neovascular glaucoma. J. Glaucoma 2007, 16, 437–439. [Google Scholar] [CrossRef]
- Saikumar, S.J.; Manju, A.; Abhilash, N. Neovascular glaucoma. Kerala J. Ophthalmol. 2018, 30, 172–177. [Google Scholar] [CrossRef]
- Kim, Y.H.; Sung, M.S.; Park, S.W. Clinical Features of Ocular Ischemic Syndrome and Risk Factors for Neovascular Glaucoma. Korean J. Ophthalmol. 2017, 31, 343. [Google Scholar] [CrossRef]
- Li, Z.Q.; Zhou, X.X.; Lin, S.; Li, J.L.; Wu, J.G. Angiography reveals early hiding iris neovascularization after ischemic CRVO. Int. J. Ophthalmol. 2013, 6, 253–254. [Google Scholar]
- Brancato, R.; Bandello, F.; Lattanzio, R. Iris fluorescein angiography in clinical practice. Surv. Ophthalmol. 1997, 42, 41–70. [Google Scholar] [CrossRef]
- Roberts, P.K.; Goldstein, D.A.; Fawzi, A. Anterior Segment Optical Coherence Tomography Angiography for Identification of Iris Vasculature and Staging of Iris Neovascularization: A Pilot Study. Curr Eye Ress 2017, 42, 1136–1142. [Google Scholar] [CrossRef]
- Hayren, S.S. Neovascular Glaucoma. Prog Retin Eye Res 2007, 26, 470–485. [Google Scholar] [CrossRef]
- Vinod, K.; Gedde, S.J.; Feuer, W.J.; Panarelli, J.F.; Chang, T.C.; Chen, P.P.; Parrish, R.K., 2nd. Practice Preferences for Glaucoma Surgery: A Survey of the American Glaucoma Society. J. Glaucoma 2017, 26, 687–693. [Google Scholar] [CrossRef]
- Terelak-Borys, B.; Skonieczna, K.; Grabska-Liberek, I. Akių išeminis sindromas—Sisteminė apžvalga. Med. Sci. Monit. 2012, 18, 138–144. [Google Scholar]
- Spaeth, G.L. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. BMJ J. Ophthalmol. 2021, 105, 1–169. [Google Scholar]
- Simha, A.; Aziz, K.; Braganza, A.; Abraham, L.; Samuel, P.; Lindsley, K.B. Anti-vascular endothelial growth factor for neovascular glaucoma. Cochrane Database Syst. Rev. 2020, 2, 1465–1858. [Google Scholar] [CrossRef]
- Laatikainen, L. Preliminary report on effect of retinal panphotocoagulation on rubeosis iridis and neovascular glaucoma. Br. J. Ophthalmol. 1977, 61, 278. [Google Scholar] [CrossRef]
- Salim, S. Diagnosis and Treatment of Neovascular Glaucoma. American Academy of Ophthalmology, EyeNet Magazine. 2006, p. Epub. Available online: https://www.aao.org/eyenet/article/diagnosis-treatment-of-neovascular-glaucoma (accessed on 14 September 2022).
- Yilmaz, T.; Cordero-Coma, M.; Gallagher, M.J.; Teasley, L.A. Systematic review of intravitreal bevacizumab injection for treatment of primary diabetic macular oedema. Acta Ophthalmol. 2011, 89, 709–717. [Google Scholar] [CrossRef]
- Ghanem, A.A.; Kannishy, A.M.E.-; Wehidy, A.S.E.; El-Agamy, A.F. Intravitreal Bevacizumab (Avastin) as an Adjuvant Treatment in Cases of Neovascular Glaucoma. Middle East Afr. J. Ophthalmol. 2009, 16, 75. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.Y.; Lee, T.H.; Sung, M.S.; Park, S.W. Efficacy and Safety of Intracameral Bevacizumab for Treatment of Neovascular Glaucoma. Korean J. Ophthalmol. 2017, 31, 538–547. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ferrara, N.; Damico, L.; Shams, N.; Lowman, H.; Kim, R. Development of ranibizumab, an anti-vascular endothelial growth factor antigen binding fragment, as therapy for neovascular age-related macular degeneration. Retina 2006, 26, 859–870. [Google Scholar] [CrossRef] [PubMed]
- Li, D.K.; Zhang, F.; Yu, J.Q.; Liu, Z.K.; Wang, Y.; Mu, Y.T. Clinical observation of ranibizumab combined with surgery in the treatment of neovascular glaucoma with vitreous hemorrhage. Int. Ophthalmol. 2022, 42, 2757–2763. [Google Scholar] [CrossRef]
- Lüke, J.; Nassar, K.; Lüke, M.; Grisanti, S. Ranibizumab as adjuvant in the treatment of rubeosis iridis and neovascular glaucoma—Results from a prospective interventional case series. Graefe’s Arch. Clin. Exp. Ophthalmol. 2013, 251, 2403–2413. [Google Scholar] [CrossRef]
- Mira, F.; Paulo, M.; Henriques, F.; Figueira, J. Switch to Aflibercept in Diabetic Macular Edema Patients Unresponsive to Previous Anti-VEGF Therapy. J. Ophthalmol. 2017, 2017, 5632634. [Google Scholar] [CrossRef]
- Inatani, M.; Higashide, T.; Matsushita, K.; Miki, A.; Ueki, M.; Iwamoto, Y.; Kobayashi, M.; Leal, S.; VEGA Investigators. Intravitreal Aflibercept in Japanese Patients with Neovascular Glaucoma: The VEGA Randomized Clinical Trial. Adv. Ther. 2020, 38, 1116–1129. [Google Scholar] [CrossRef]
- Tadayoni, R.; Sararols, L.; Weissgerber, G.; Verma, R.; Clemens, A.; Holz, F.G. Brolucizumab: A Newly Developed Anti-VEGF Molecule for the Treatment of Neovascular Age-Related Macular Degeneration. Ophthalmologica 2021, 244, 93–101. [Google Scholar] [CrossRef]
- Mason, J.O.; Albert, M.A.; Mays, A.; Vail, R. Regression of neovascular iris vessels by intravitreal injection of bevacizumab. Retina 2006, 26, 839–841. [Google Scholar] [CrossRef]
- Wakabayashi, T.; Oshima, Y.; Sakaguchi, H.; Ikuno, Y.; Miki, A.; Gomi, F.; Otori, Y.; Kamei, M.; Kusaka, S.; Tano, Y. Intravitreal Bevacizumab to Treat Iris Neovascularization and Neovascular Glaucoma Secondary to Ischemic Retinal Diseases in 41 Consecutive Cases. Ophthalmology 2008, 115, 1571–1580.e3. [Google Scholar] [CrossRef]
- Zhao, X.; Wang, Z.; Yang, X. Management of neovascular glaucoma with intravitreal ranibizumab, panretinal photocoagulation, and subsequent 5-fluorouracil augmented trabeculectomy. Medicine 2017, 96, e7221. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.Y.; Nam, K.Y.; Lee, S.J.; Lee, S.U. The effect of intravitreal bevacizumab injection before Ahmed valve implantation in patients with neovascular glaucoma. Int. Ophthalmol. 2013, 34, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Rani, P.K.; Sen, P.; Sahoo, N.K.; Senthil, S.; Chakurkar, R.; Anup, M.; Behera, U.C.; Sivaprasad, S.; Das, T.; India Retinal Disease Study Group. Outcomes of neovascular glaucoma in eyes presenting with moderate to good visual potential. Int. Ophthalmol. 2021, 41, 2359–2368. [Google Scholar] [CrossRef] [PubMed]
- Shchomak, Z.; Sousa, D.C.; Leal, I.; Pinto, L.A. Surgical treatment of neovascular glaucoma: A systematic review and meta-analysis. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 1079–1089. [Google Scholar] [CrossRef]
- Tokumo, K.; Komatsu, K.; Yuasa, Y.; Murakami, Y.; Okumichi, H.; Hirooka, K.; Nakakura, S.; Tabuchi, H.; Kiuchi, Y. Treatment outcomes n the neovascular glaucoma tube versus trabeculectomy study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 3067–3076. [Google Scholar] [CrossRef]
- Kiuchi, Y.; Sugimoto, R.; Nakae, K.; Saito, Y.; Ito, S. Trabeculectomy with Mitomycin C for Treatment of Neovascular Glaucoma in Diabetic Patients. Ophthalmologica 2006, 220, 383–388. [Google Scholar] [CrossRef]
- Hoang, T.K.H.; Kim, Y.K.; Jeoung, J.W.; Park, K.H. Relationship between age and surgical success after trabeculectomy with adjunctive mitomycin C. Eye 2018, 32, 1321. [Google Scholar] [CrossRef]
- Nilforushan, N.; Es’Haghi, A.; Miraftabi, A.; Abolfathzadeh, N.; Banifatemi, M. Trabeculectomy in patients with diabetes: Subconjunctival Mitomycin C with or without intravitreal bevacizumab. Br. J. Ophthalmol. 2022, 106, 648–654. [Google Scholar] [CrossRef]
- Higashide, T.; Ohkubo, S.; Sugiyama, K.; Shukla, D. Long-Term Outcomes and Prognostic Factors of Trabeculectomy following Intraocular Bevacizumab Injection for Neovascular Glaucoma. PLoS ONE 2015, 10, 135766. [Google Scholar] [CrossRef]
- Takihara, Y.; Inatani, M.; Fukushima, M.; Iwao, K.; Iwao, M.; Tanihara, H. Trabeculectomy with Mitomycin C for Neovascular Glaucoma: Prognostic Factors for Surgical Failure. Am. J. Ophthalmol. 2009, 147, 912–918.e1. [Google Scholar] [CrossRef]
- Saito, Y.; Higashide, T.; Takeda, H.; Ohkubo, S.; Sugiyama, K. Beneficial effects of preoperative intravitreal bevacizumab on trabeculectomy outcomes in neovascular glaucoma. Acta Ophthalmol. 2010, 88, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Dally, L.G.; Ederer, F.; Gaasterland, D.; Blackwell, B.; Van Veldhuisen, P.; Allen, R.C.; Beck, A.; Weber, P.A.; Ashburn, F. The Advanced Glaucoma Intervention Study (AGIS): Risk factors for failure of trabeculectomy and argon laser trabeculoplasty. Am. J. Ophthalmol. 2002, 134, 481–498. [Google Scholar] [CrossRef]
- Bar-David, L.; Blumenthal, E.Z. Evolution of Glaucoma Surgery in the Last 25 Years. Rambam Maimonides Med. J. 2018, 9, e0024. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, P.; Bhardwaj, P. Glaucoma drainage implants. Int. J. Ophthalmol. 2020, 13, 1318. [Google Scholar] [CrossRef] [PubMed]
- Xie, Z.; Liu, H.; Du, M.; Zhu, M.; Tighe, S.; Chen, X.; Yuan, Z.; Sun, H. Efficacy of Ahmed Glaucoma Valve Implantation on Neovascular Glaucoma. Int. J. Med. Sci. 2019, 16, 1371–1376. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Tian, Y.; Song, W.; Su, T.; Jiang, H.; Xia, X. Clinical efficacy analysis of Ahmed glaucoma valve implantation in neovascular glaucoma and influencing factors. Medicine 2017, 96, e8350. [Google Scholar] [CrossRef]
- Shen, C.C.; Salim, S.; Du, H.; Netland, P.A. Trabeculectomy versus Ahmed Glaucoma Valve implantation in neovascular glaucoma. Clin Ophthalmol 2011, 5, 281–286. [Google Scholar]
- Hwang, H.B.; Lee, N.Y. Effect of anti-vascular endothelial growth factor on the surgical outcome of neovascular glaucoma: An overview and meta-analysis. Medicine 2021, 100, e27326. [Google Scholar] [CrossRef]
- Kwon, J.; Sung, R.K. Effect of Preoperative Intravitreal Bevacizumab on the Surgical Outcome of Neovascular Glaucoma at Different Stages. J. Ophthalmol. 2017, 2017, 7672485. [Google Scholar] [CrossRef]
- Christakis, P.G.; Kalenak, J.W.; Tsai, J.C.; Zurakowski, D.; Kammer, J.A.; Harasymowycz, P.J.; Mura, J.J.; Cantor, L.B.; Ahmed, I.I.K. The Ahmed Versus Baerveldt Study: Five-Year Treatment Outcomes. Ophthalmology 2016, 123, 2093–2102. [Google Scholar] [CrossRef]
- Bhartiya, S.; Dhingra, D.; Shaarawy, T. Revisiting Results of Conventional Surgery: Trabeculectomy, Glaucoma Drainage Devices, and Deep Sclerectomy in the Era of MIGS. J Curr Glaucoma Pr. 2019, 13, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Jindal, A.P.; Aref, A.A.; Giaconi, J.A.; Eliassi-Rad, B. Cyclodestructive Procedures in Treatment of Glaucoma. American Academy of Ophthalmology, EyeWiki. 2019, p. ePub. Available online: https://eyewiki.aao.org/Cyclodestructive_Procedures_in_Treatment_of_Glaucoma (accessed on 14 September 2022).
- Anand, N.; Klug, E.; Nirappel, A.; Solá-Del Valle, D. A Review of Cyclodestructive Procedures for the Treatment of Glaucoma. Semin. Ophthalmol. 2020, 35, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.L.; Moster, M.R.; Rahmatnejad, K.; Resende, A.F.; Horan, T.; Reynolds, M.; Yung, E.; Abramowitz, B.; Kuchar, S.; Waisbourd, M. Clinical efficacy and safety profile of micropulse transscleral cyclophotocoagulation in refractory glaucoma. J. Glaucoma 2018, 27, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Penniecook, J.A.; Cruz, D.S.G.; Caminos, M.S.P. Managing the painful blind eye. Community Eye Health J. 2021, 34, 55–56. [Google Scholar]
- Şalkacı, O.; Ayyıldız, T.; Kandemir, B.; Çallı, Ü.; Rodop Özgür, Ö.; Özertürk, Y.; Lütfi Kırdar Eğitim ve Araştırma Hastanesi, K. Pain Management by Retrobulbar Alcohol Injection in Blind Painful Eyes Due to Late-Stage Neovascular Glaucoma. South. Clin. Ist. Euras 2017, 28, 17–21. [Google Scholar] [CrossRef]
- Kawabata, K.; Shobayashi, K.; Iwao, K.; Takahashi, E.; Tanihara, H.; Inoue, T. Efficacy and safety of Ex-PRESS® mini shunt surgery versus trabeculectomy for neovascular glaucoma: A retrospective comparative study. BMC Ophthalmol. 2019, 19, 75. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Retinal ischemic diseases | Proliferative diabetic retinopathy (PDR) Central retinal vein occlusion (CRVO) Branch retinal vein occlusion (BRVO) Ocular ischemic syndrome Central retinal artery occlusion Chronic retinal detachment Eale, Coats diseases Leber’s congenital amaurosis Retinopathy of prematurity Sickle cell retinopathy Retinoschisis Angiomatosis retinae (Von Hippel’s disease) Hemorrhagic retina disease Family exudation vitreoretinopathy Proliferative vitreoretinopathy | [4,19,20,21,22] |
| Extraocular vascular/Systemic diseases | Carotid-cavernous disease Giant cell arteritis Takayasu‘s disease Internal carotid artery occlusion Youthful myelomonocytic leukemia Systemic lupus erythematosus Youthful xantogranuloma Type 1 cryoglobulinemia Type 1 neurofibromatosis | [20,21,22] |
| Ocular inflammation | Endophthalmitis Chronic uveitis Purtscher’s retinopathy Sympathetic ophthalmia Retinal vasculitis Injuries | [4,20,21,22] |
| Ocular tumors | Uveal melanoma Retinoblastoma Ciliary body medulloepithelioma Large cell lymphoma Squamous cell carcinoma Ocular metastasis Vasoproliferative retinal tumors | [20,21,22] |
| Surgical involvement | Cataract extraction Pars plana vitrectomy YAG capsulotomy Carotid endarterectomy Radiation therapy | [21,22] |
| Stages | Symptoms | Clinical Findings | Gonioscopy Findings | Tonometry | NVI | Prognosis | References |
|---|---|---|---|---|---|---|---|
| Pre-rubeosis | No visible symptoms | New vessels on the iris or in the angle of anterior chamber are not visible. Clinical findings of underlying disease causing retinal ischemia (PDR, CRVO, IOS). | Normal | Normal IOP | Absent | Good | [6,21] |
| Rubeosis iridis (Pre glaucoma) | Eye redness, pain, photophobia | New abnormal blood vessels (NVI) randomly oriented over the iris surface and primarily observed in the pupillary edge of the iris. Impaired pupil response | Open angles; NVA may be detected | Normal IOP | Present | Good | [18,21] |
| Secondary open-angle glaucoma | Eye redness, pain, photophobia, mild headache | Occurs due to the formation of fibrovascular membrane on anterior surface of the iris and angle of anterior chamber. In time, this membrane causes the obstruction which disrupts fluid leakage through TM. Poorly reactive pupil | Open angles; NVA may be visible | Raised IOP | Significant | Good if treatment is timely | [21] |
| Secondary angle-closure glaucoma | Urgent ophthalmic condition: acute, severe eye pain; severe headache; nause/vomiting; conjuctival injection; swollen cornea; retinal bruising; hyphema | Development of goniosynechiae resulting from contracture of the neovascular membrane. Distorted, mid-dilated pupil. | Closed angles; NVA not visible | High IOP (Often 40-60 mmHg) | Significant with ectropion uveae | Bad | [6,20,21] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urbonavičiūtė, D.; Buteikienė, D.; Janulevičienė, I. A Review of Neovascular Glaucoma: Etiology, Pathogenesis, Diagnosis, and Treatment. Medicina 2022, 58, 1870. https://doi.org/10.3390/medicina58121870
Urbonavičiūtė D, Buteikienė D, Janulevičienė I. A Review of Neovascular Glaucoma: Etiology, Pathogenesis, Diagnosis, and Treatment. Medicina. 2022; 58(12):1870. https://doi.org/10.3390/medicina58121870
Chicago/Turabian StyleUrbonavičiūtė, Danielė, Dovilė Buteikienė, and Ingrida Janulevičienė. 2022. "A Review of Neovascular Glaucoma: Etiology, Pathogenesis, Diagnosis, and Treatment" Medicina 58, no. 12: 1870. https://doi.org/10.3390/medicina58121870
APA StyleUrbonavičiūtė, D., Buteikienė, D., & Janulevičienė, I. (2022). A Review of Neovascular Glaucoma: Etiology, Pathogenesis, Diagnosis, and Treatment. Medicina, 58(12), 1870. https://doi.org/10.3390/medicina58121870