
Peri-Neural Invasion Is an Important Prognostic Factor of T2N0 Oral Cancer


 ,
, 
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects Inclusion Criteria
2.2. Adjuvant Therapy after Surgery
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefèbvre, J.-L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.S.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Campbell, B.H.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Postoperative Concurrent Radiotherapy and Chemotherapy for High-Risk Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2004, 350, 1937–1944. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.S.; Zhang, Q.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Long-term follow-up of the RTOG 9501/intergroup phase III trial: Postoperative concurrent radiation therapy and chemotherapy in high-risk squamous cell carcinoma of the head & neck. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 1198–1205. [Google Scholar] [PubMed]
- Li, Y.; Bai, S.; Carroll, W.; Dayan, D.; Dort, J.C.; Heller, K.; Jour, G.; Lau, H.; Penner, C.; Prystowsky, M.; et al. Validation of the Risk Model: High-Risk Classification and Tumor Pattern of Invasion Predict Outcome for Patients with Low-Stage Oral Cavity Squamous Cell Carcinoma. Head Neck Pathol. 2013, 7, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Sessions, D.G.; Spector, G.J.; Lenox, J.; Haughey, B.; Chao, C.; Marks, J. Analysis of Treatment Results for Oral Tongue Cancer. Laryngoscope 2002, 112, 616–625. [Google Scholar] [CrossRef]
- Ho, C.M.; Lam, K.H.; Wei, W.; Lau, S.K.; Lam, L.K. Occult lymph node metastasis in small oral tongue cancers. Head Neck 1992, 14, 359–363. [Google Scholar] [CrossRef]
- Capote, A.; Escorial, V.; Munoz-Guerra, M.F.; Rodríguez-Campo, F.J.; Gamallo, C.; Naval, L. Elective neck dissection in early-stage oral squamous cell carcinoma-does it influence recurrence and survival? Head Neck 2007, 29, 3–11. [Google Scholar] [CrossRef]
- Chatzistefanou, I.; Lubek, J.; Markou, K.; Ord, R.A. The role of perineural invasion in treatment decisions for oral cancer patients: A review of the literature. J. Cranio-Maxillofac. Surg. 2017, 45, 821–825. [Google Scholar] [CrossRef]
- Jones, H.; Sykes, A.; Bayman, N.; Sloan, P.; Swindell, R.; Patel, M.; Musgrove, B. The impact of lymphovascular invasion on survival in oral carcinoma. Oral. Oncol. 2009, 45, 10–15. [Google Scholar] [CrossRef]
- Seethala, R.R.; Weinreb, I.; Bullock, M.J.; Carlson, D.L.; Ferris, R.L.; Harrison, L.B.; McHugh, J.B.; Pettus, J.; Richardson, M.S.; Shah, J.; et al. Cancer Protocols and Checklists: Lip and Oral Cavity; Version 4.0.0.1.; College of American Pathologists: Northfield, IL, USA, 2017. [Google Scholar]
- Woolgar, J.A. Histopathological prognosticators in oral and oropharyngeal squamous cell carcinoma. Oral. Oncol. 2006, 42, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Goodman, M.; Liu, L.; Ward, K. Invasion characteristics of oral tongue cancer: Frequency of reporting and effect on survival in a population-based study. Cancer 2009, 115, 4010–4020. [Google Scholar] [CrossRef]
- Haddad, R.I.; Shin, D.M. Recent Advances in Head and Neck Cancer. N. Engl. J. Med. 2008, 359, 1143–1154. [Google Scholar] [CrossRef]
- Brandwein-Gensler, M.; Smith, R.V.; Wang, B.; Penner, C.; Theilken, A.; Broughel, D.; Schiff, B.; Owen, R.P.; Smith, J.; Sarta, C.; et al. Validation of the histologic risk model in a new cohort of patients with head and neck squamous cell carcinoma. Am. J. Surg. Pathol. 2010, 34, 676–688. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, K.A.; Hoffman, H.T.; Zimmerman, M.B.; Robinson, R.A. Perineural and vascular invasion in oral cavity squamous carcinoma: Increased incidence on re-review of slides and by using immunohistochemical enhancement. Arch. Pathol. Lab. Med. 2005, 129, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Tai, S.-K.; Li, W.-Y.; Yang, M.-H.; Chang, S.-Y.; Chu, P.-Y.; Tsai, T.-L.; Wang, Y.-F.; Chang, P.M.-H. Treatment for T1-2 Oral squamous cell carcinoma with or without perineural invasion: Neck dissection and postoperative adjuvant therapy. Ann. Surg. Oncol. 2012, 19, 1995–2002. [Google Scholar] [CrossRef]
- Sparano, A.; Weinstein, G.; Chalian, A.; Yodul, M.; Weber, R. Multivariate predictors of occult neck metastasis in early oral tongue cancer. Otolaryngol. Head Neck Surg. 2004, 131, 472–476. [Google Scholar] [CrossRef]
- Aires, F.T.; Lin, C.S.; Matos, L.L.; Kulcsar, M.A.V.; Cernea, C.R. Metastasis in patients with oral cavity squamous cell carcinoma undergoing surgical treatment. J. Otorhinolaryngol. Relat. Spec. 2017, 79, 347–355. [Google Scholar] [CrossRef]
- Luryi, A.L.; Chen, M.M.; Mehra, S.; Roman, S.A.; Sosa, J.A.; Judson, B.L. Treatment factors associated with survival in early-stage oral cavity cancer. JAMA Otolaryngol. Neck Surg. 2015, 141, 593. [Google Scholar] [CrossRef]
- Rubin, S.J.; Gurary, E.B.; Qureshi, M.M.; Salama, A.R.; Ezzat, W.H.; Jalisi, S.; Truong, M.T. stage II oral tongue cancer: Survival impact of adjuvant radiation based on depth of invasion. Otolaryngol. Neck Surg. 2019, 160, 77–84. [Google Scholar] [CrossRef]
- Nair, D.; Mair, M.; Singhvi, H.; Singhvi, H.; Mishra, A.; Nair, S.; Agrawal, J.; Chaturvedi, P. Perineural invasion: In dependent prognostic factor in oral cancer that warrants adjuvant treatment. Head Neck 2018, 40, 1780–1787. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, S.; Li, Z.; Han, X.; Que, L. Prognostic value of perineural invasion in oral tongue squamous cell carcinoma: A systemic review and meta-analysis. Front. Oncol. 2021, 11, 683825. [Google Scholar] [CrossRef] [PubMed]
- Rahima, B.; Shingaki, S.; Nagata, M.; Saito, C. Prognostic significance of perineural invasion in oral and oropharyngeal carcinoma. Oral Surg. Oral Med. Oral Pathol. Ora. Radiol. Endod. 2004, 97, 423–431. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Numbers (%) | 3-Year DSS | p Value | 3-Year DFS | p Value |
|---|---|---|---|---|---|
| Age | 33–92 | ||||
| Median:56 | |||||
| ≤56 | 83 (50) | 85.7% | 86.4% | ||
| >56 | 83 (50) | 84.6% | p = 0.22 | 74.0% | p = 0.25 |
| Gender | |||||
| Male | 148 (89.2) | 85.7% | 80.1% | ||
| Female | 18 (10.8) | 88.8% | p = 0.56 | 80.4% | p = 0.85 |
| Grade | |||||
| Well differentiated | 14 (8.4) | 100% | 84.4% | ||
| Moderate differentiated | 132 (79.6) | 85.8% | 81.2% | ||
| Poor differentiated | 20 (12.0) | 70.1% | p = 0.56 | 70.0% | p = 0.53 |
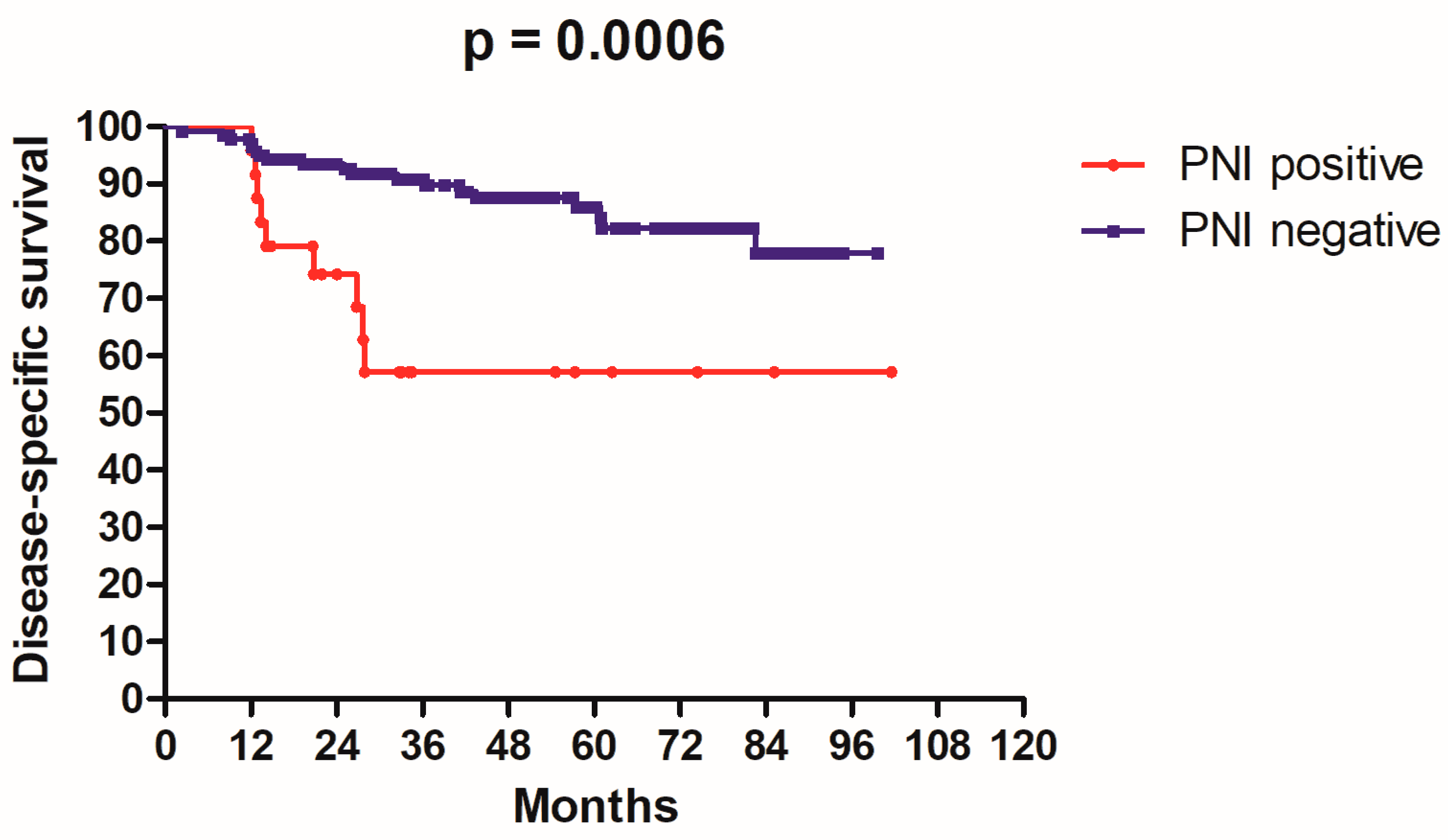
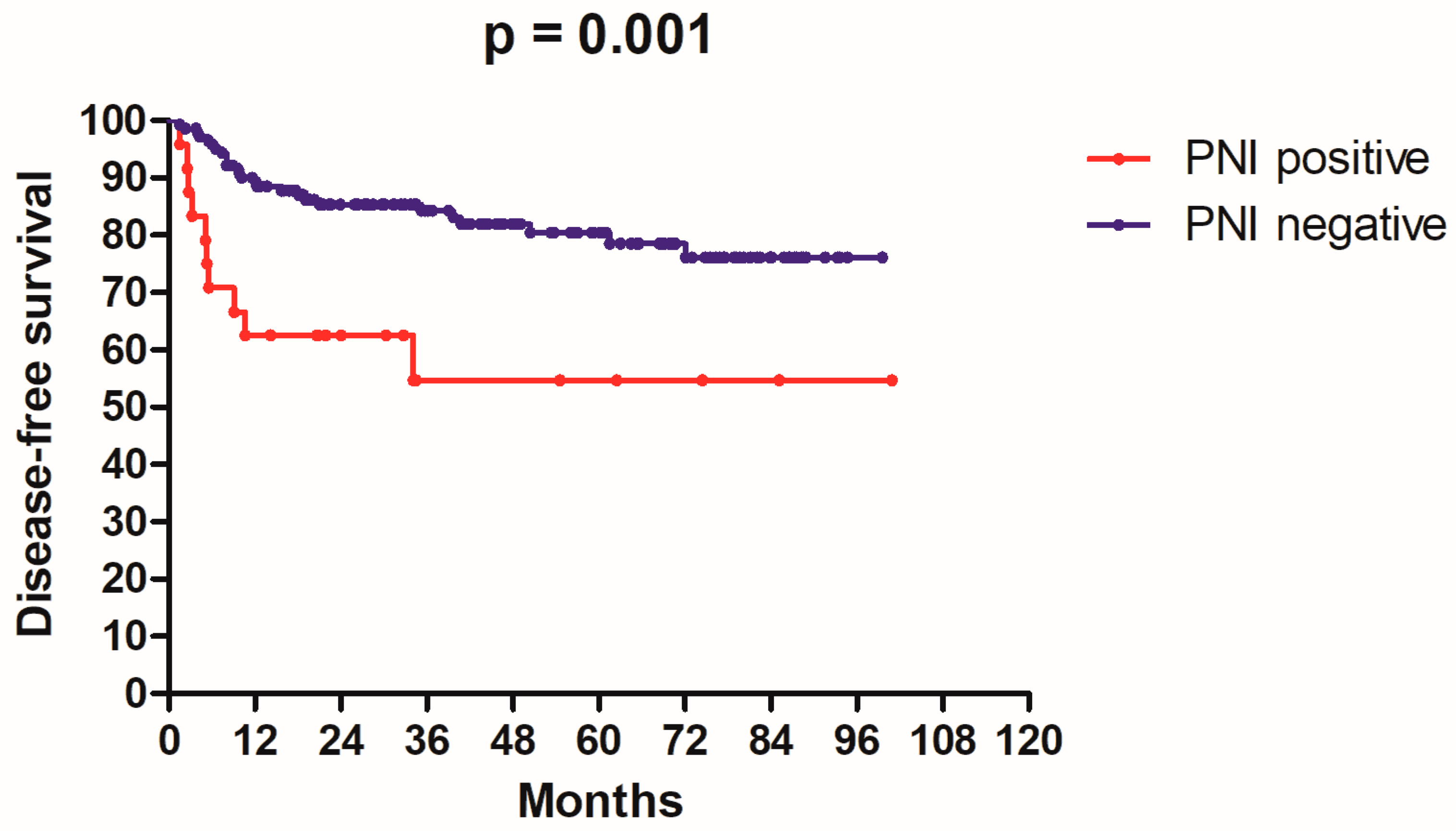
| PNI | |||||
| Positive | 24 (14.4) | 57.0% | 54.6% | ||
| Negative | 142 (85.6) | 90.8% | p = 0.0006 | 84.2% | p = 0.001 |
| ALI | |||||
| Positive | 6 (3.6) | 50.0% | 50.0% | ||
| Negative | 160 (96.4) | 87.5% | p = 0.01 | 82.2% | p = 0.0009 |
| Margin | |||||
| Positive | 20 (12.0) | 72.3% | 68.8% | ||
| Negative | 146 (88.0) | 86.9% | p = 0.25 | 81.6% | p = 0.33 |
| Adjuvant radiotherapy | |||||
| Yes | 28 (16.8) | 88.2% | 92.8% | ||
| No | 138 (83.2) | 83.1% | p = 0.24 | 77.5% | p = 0.11 |
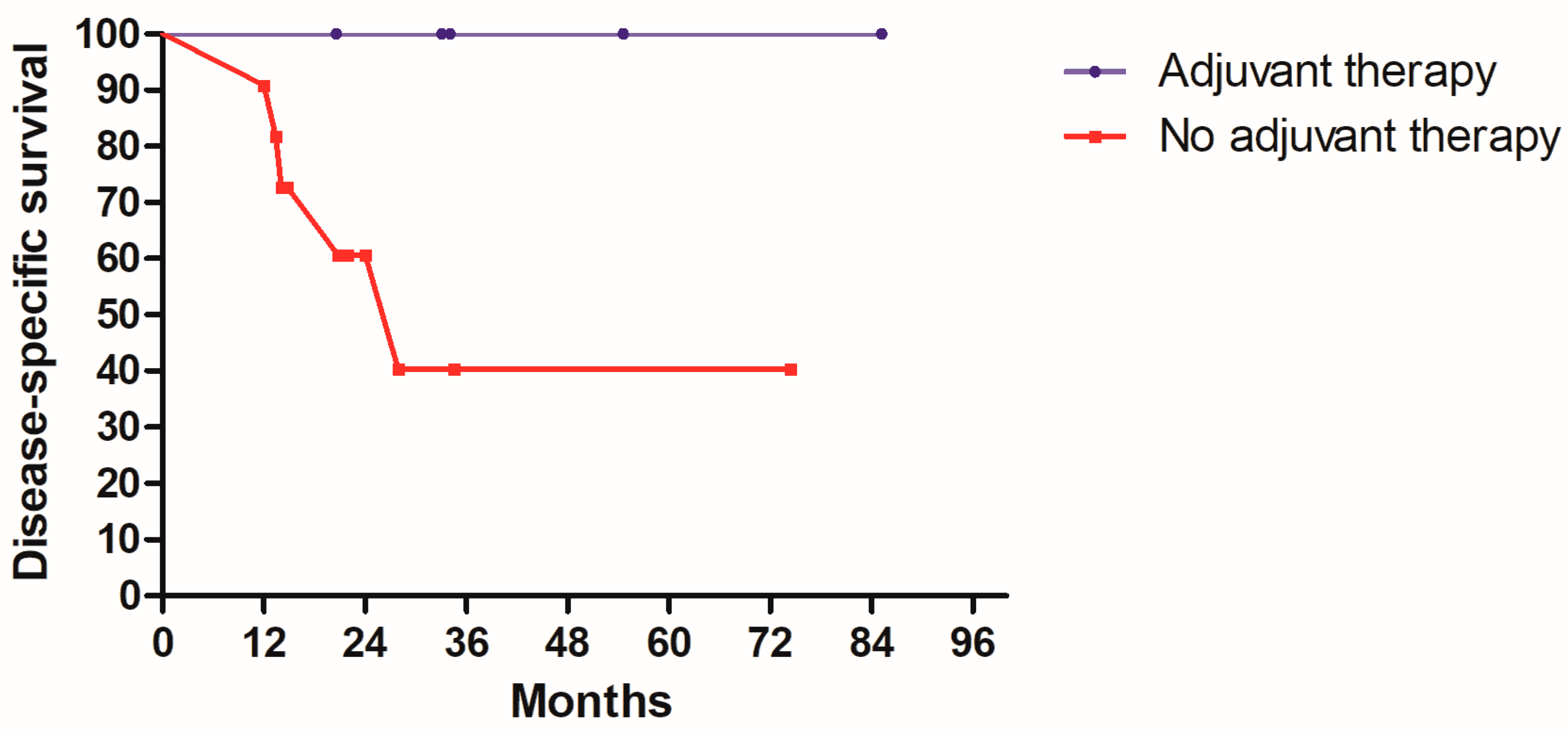
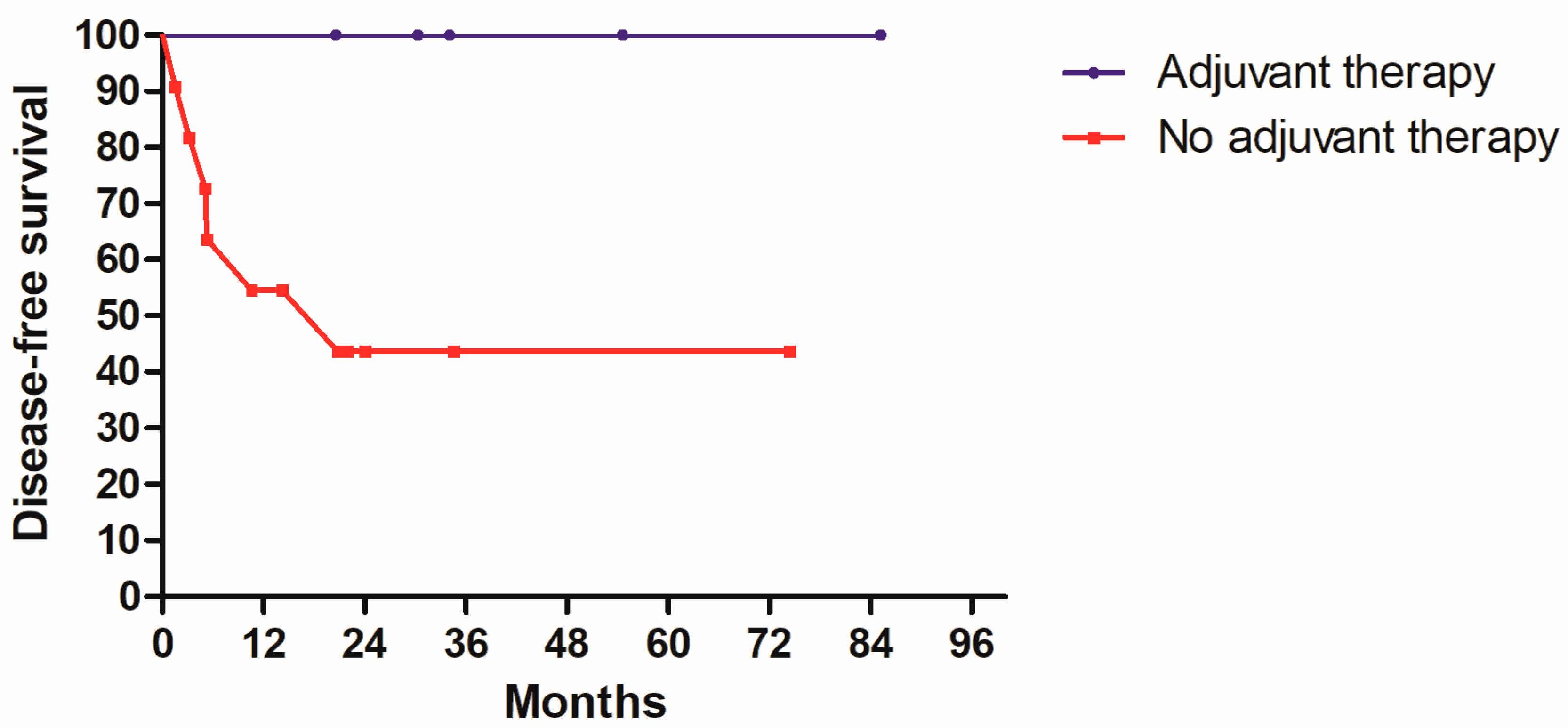
| Adjuvant chemotherapy | |||||
| Yes | 24 (14.4) | 100% | 100% | ||
| No | 142 (85.6) | 82.4% | p = 0.01 | 76.7% | p = 0.02 |
| Variables | HR (95%CI) | p Value |
|---|---|---|
| DSS | ||
| PNI | 5.02 (1.99–12.6) | p = 0.001 |
| ALI | 1.79 (0.45–7.16) | p = 0.405 |
| Adjuvant chemotherapy | 0.01 (0.00–5.57) | p = 0.957 |
| DFS | ||
| PNI | 3.92 (1.65–9.32) | p = 0.002 |
| ALI | 3.23 (0.95–10.9) | p = 0.059 |
| Adjuvant chemotherapy | 0.06 (0.01–0.52) | p = 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, C.-S.; Chen, C.-C.; Liu, Y.-C.; Wang, C.-C.; Chou, Y.-S. Peri-Neural Invasion Is an Important Prognostic Factor of T2N0 Oral Cancer. Medicina 2022, 58, 1809. https://doi.org/10.3390/medicina58121809
Cheng C-S, Chen C-C, Liu Y-C, Wang C-C, Chou Y-S. Peri-Neural Invasion Is an Important Prognostic Factor of T2N0 Oral Cancer. Medicina. 2022; 58(12):1809. https://doi.org/10.3390/medicina58121809
Chicago/Turabian StyleCheng, Chi-Sheng, Chien-Chih Chen, Yi-Chun Liu, Chen-Chi Wang, and Yu-Shu Chou. 2022. "Peri-Neural Invasion Is an Important Prognostic Factor of T2N0 Oral Cancer" Medicina 58, no. 12: 1809. https://doi.org/10.3390/medicina58121809
APA StyleCheng, C.-S., Chen, C.-C., Liu, Y.-C., Wang, C.-C., & Chou, Y.-S. (2022). Peri-Neural Invasion Is an Important Prognostic Factor of T2N0 Oral Cancer. Medicina, 58(12), 1809. https://doi.org/10.3390/medicina58121809