

Comparison of Long-Term Skin Quality and Scar Formation in Partial-Thickness Burn Wounds Treated with Suprathel® and epicitehydro® Wound Dressings
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
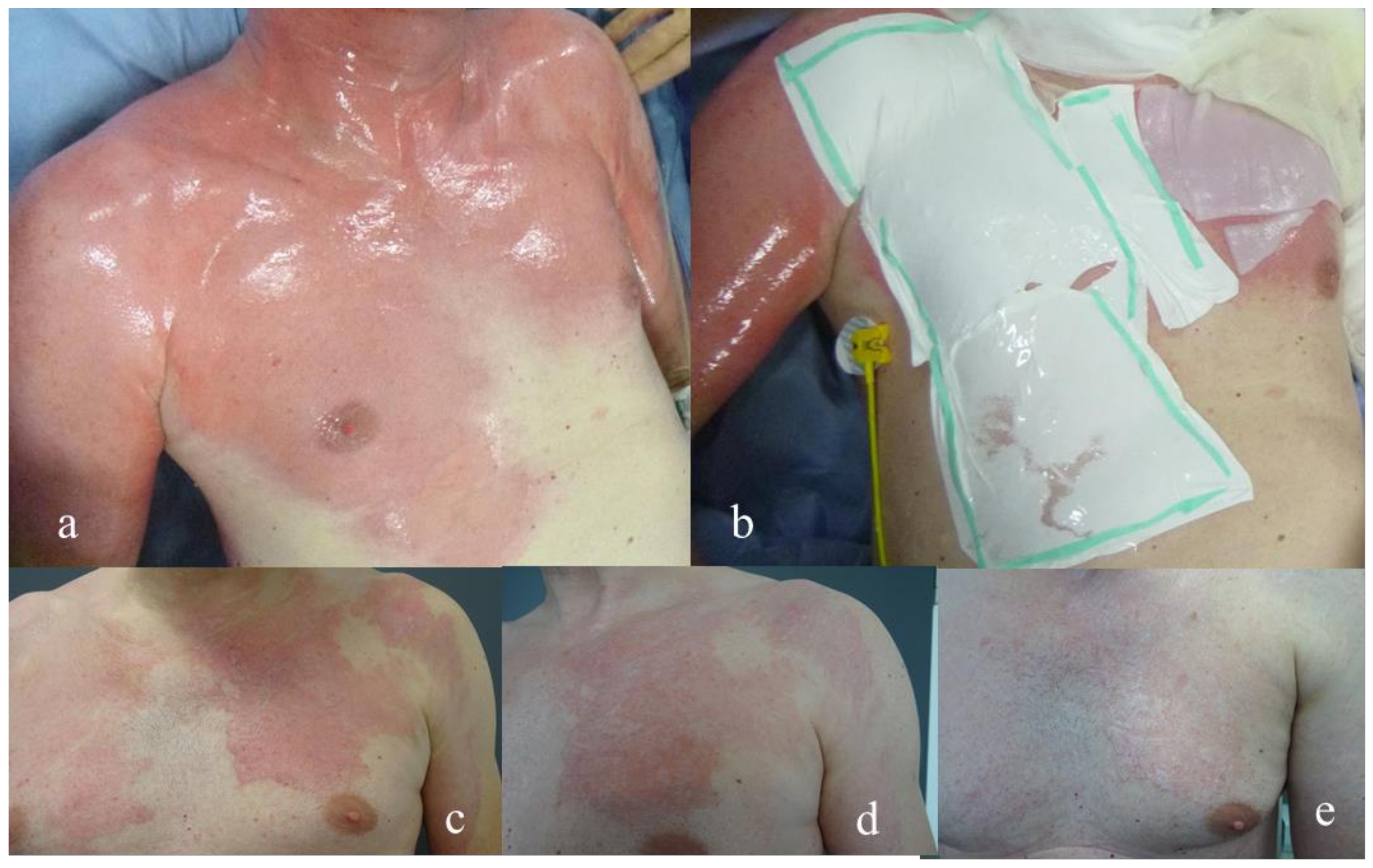
2.2. Wound Regime
2.3. Assessment of Scar Quality
2.4. Statistical Methods
3. Results
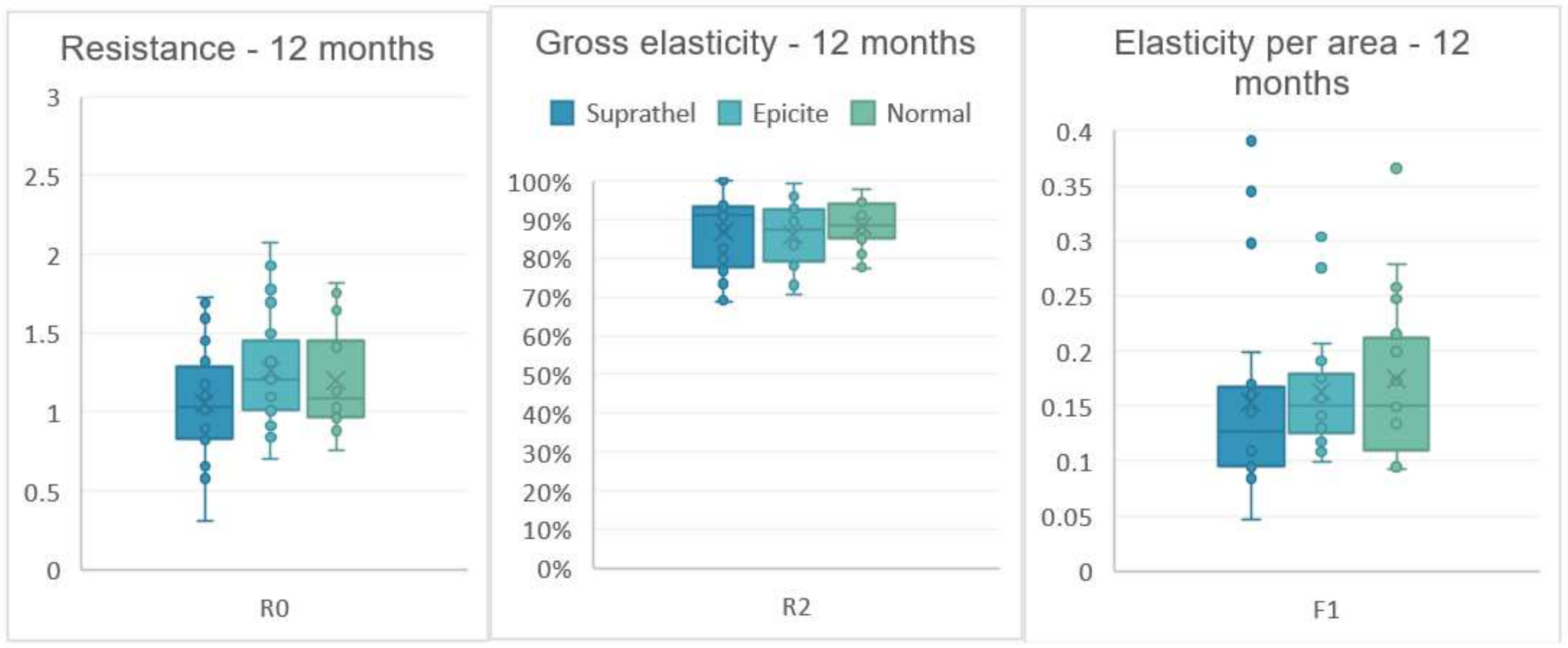
3.1. Skin Elasticity
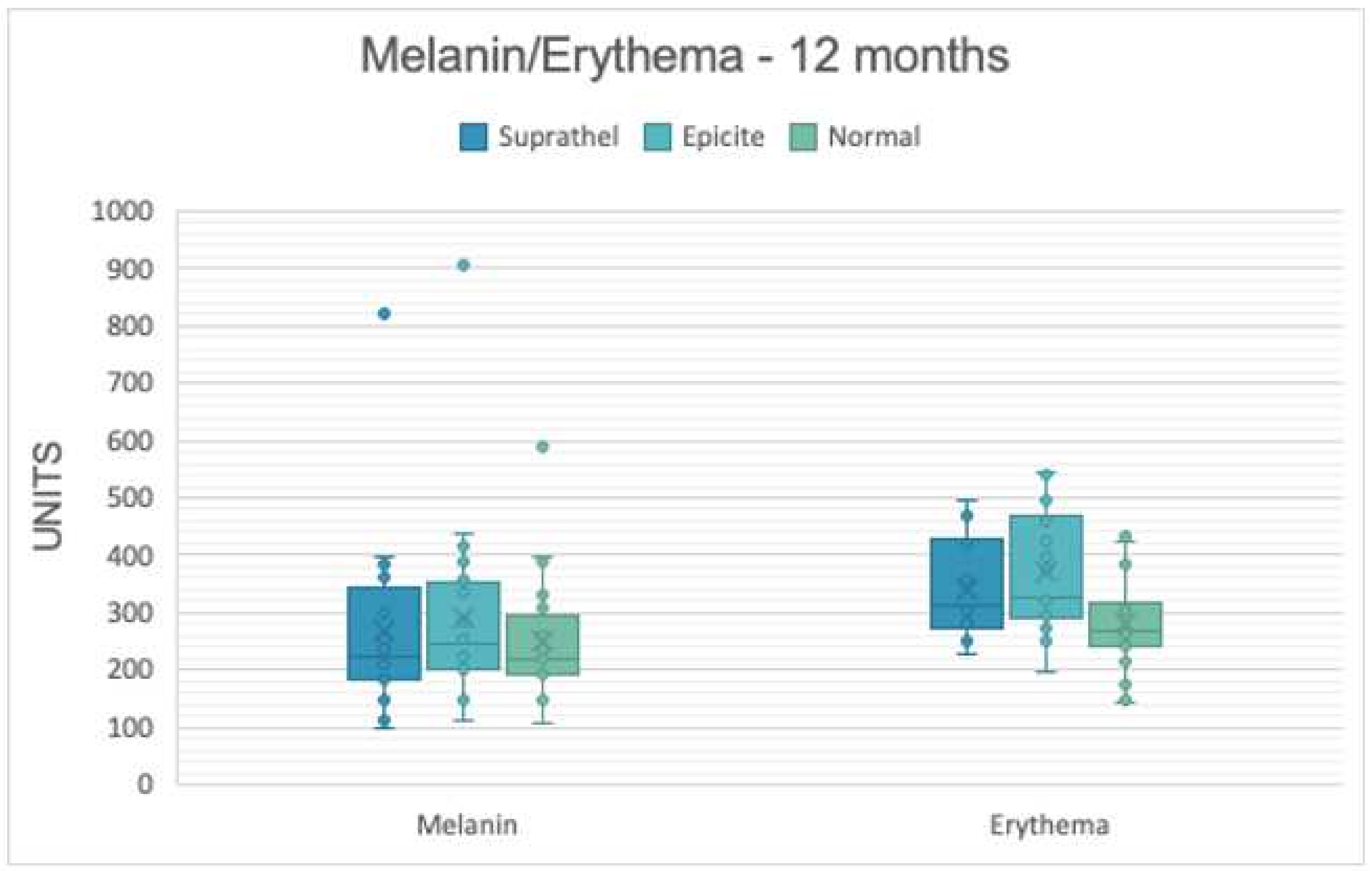
3.2. Skin Pigmentation
3.3. Trans-Epidermal Water Loss (in g/h/m2)
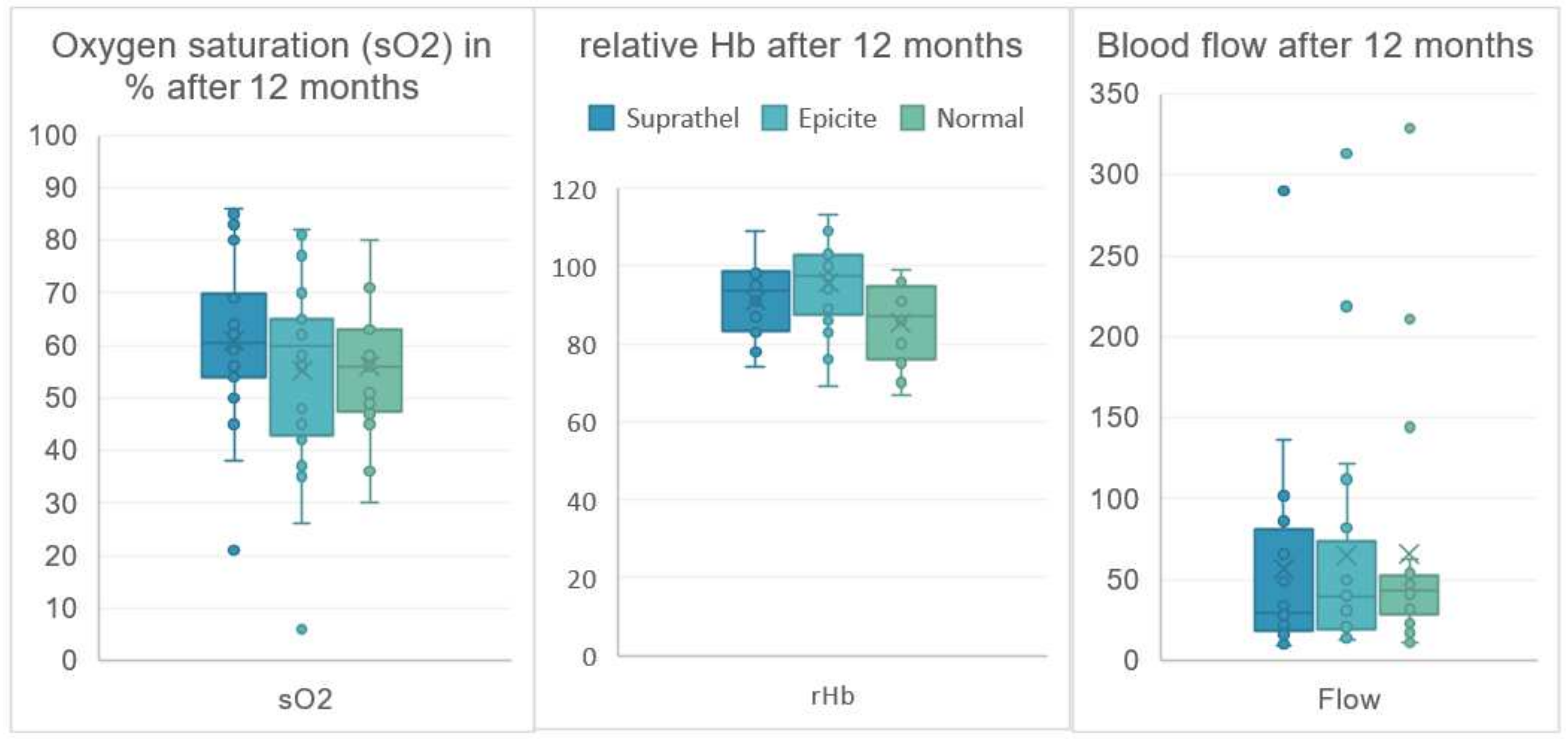
3.4. Skin Evaluation with Lightguide Spectrophotometry
3.5. Vancouver Scar Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peck, M.D. Epidemiology of burns throughout the world. Part I: Distribution and risk factors. Burns 2011, 37, 1087–1100. [Google Scholar] [CrossRef] [PubMed]
- Smolle, C.; Cambiaso-Daniel, J.; Forbes, A.A.; Wurzer, P.; Hundeshagen, G.; Branski, L.K.; Huss, F.; Kamolz, L.-P. Recent trends in burn epidemiology worldwide: A systematic review. Burns 2017, 43, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Schiefer, J.L.; Perbix, W.; Grigutsch, D.; Zinser, M.; Demir, E.; Fuchs, P.C.; Schulz, A. Etiology, incidence and gender-specific patterns of severe burns in a German Burn Center—Insights of 25 years. Burns 2016, 42, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Guideline: Treatments of thermal injuries oft he adult; Deutsche Gesellschaft für Verbrennungsmedizin; S2k Leitlinie Behandlung thermischer Verletzungen des Erwachsenen AWMF-Register-Nr.: 044-001. 2021. Available online: https://www.awmf.org/uploads/tx_szleitlinien/044-001l_S2k_Behandlung-thermischer-Verletzungen-des-Erwachsenen_2021-07.pdf (accessed on 7 September 2022).
- Karlsson, M.; Steinvall, I.; Sjöberg, F.; Olofsson, P.; Elmasry, M. Burn scar outcome at six and 12 months after injury in children with partial thickness scalds: Effects of dressing treatment. Burns 2020, 46, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Van der Wal, M.B.A.; Vloemans, J.F.P.M.; Tuinebreijer, W.E.; van de Ven, P.; van Unen, E.; van Zuijlen, P.P.M.; Middelkoop, E. Outcome after burns: An observational study on burn scar maturation and predictors for severe scarring. Wound Repair Regen. 2012, 20, 676–687. [Google Scholar] [CrossRef]
- Beele, H. Artificial skin: Past, present and future. Int. J. Artif. Organs 2002, 25, 163–173. [Google Scholar] [CrossRef]
- Przybilski, M.; Deb, R.; Erdmann, D.; Germann, G. New developments in skin replacement materials. Chirurg 2004, 75, 579–587. [Google Scholar] [CrossRef]
- Schiefer, J.L.; Daniels, M.; Grigutsch, D.; Fuchs, P.C.; Schulz, A. Feasibility of Pure Silk for the Treatment of Large Superficial Burn Wounds Covering Over 10% of the Total Body Surface. J. Burn Care Res. 2020, 41, 131–140. [Google Scholar] [CrossRef]
- Haller, H.L.; Blome-Eberwein, S.E.; Branski, L.K.; Carson, J.S.; Crombie, R.E.; Hickerson, W.L.; Kamolz, L.P.; King, B.T.; Nischwitz, S.P.; Popp, D.; et al. Porcine Xenograft and Epidermal Fully Synthetic Skin Substitutes in the Treatment of Partial-Thickness Burns: A Literature Review. Medicina 2021, 57, 432. [Google Scholar] [CrossRef]
- Schiefer, J.L.; Andreae, J.; Fuchs, P.C.; Lefering, R.; Heidekrueger, P.I.; Schulz, A.; Bagheri, M. Evaluation of Scar Quality after Treatment of Superficial Burns with Dressilk® and Suprathel®-In an Intraindividual Clinical Setting. J. Clin. Med. 2022, 11, 2857. [Google Scholar] [CrossRef]
- Schiefer, J.L.; Arens, E.; Grigutsch, D.; Rath, R.; Hoffmann, A.; Fuchs, P.C.; Schulz, A. A prospective intra-individual evaluation of silk compared to Biobrane for the treatment of superficial burns of the hand and face. Burns 2017, 43, 539–548. [Google Scholar] [CrossRef]
- Kim, L.K.; Martin, H.C.; Holland, A.J. Medical management of paediatric burn injuries: Best practice. J. Paediatr. Child Health 2012, 48, 290–295. [Google Scholar] [CrossRef]
- Maurer, K.; Renkert, M.; Duis, M.; Weiss, C.; Wessel, L.M.; Lange, B. Application of bacterial nanocellulose-based wound dressings in the management of thermal injuries: Experience in 92 children. Burns 2021, 48, 608–614. [Google Scholar] [CrossRef]
- Rashaan, Z.M.; Krijnen, P.; Allema, J.H.; Vloemans, A.F.; Schipper, I.B.; Breederveld, R.S. Usability and effectiveness of Suprathel® in partial thickness burns in children. Eur. J. Trauma Emerg. Surg. 2017, 43, 549–556. [Google Scholar] [CrossRef]
- Vloemans, A.F.P.M.; Hermans, M.H.E.; van der Wal, M.B.A.; Liebregts, J.; Middelkoop, E. Optimal treatment of partial thickness burns in children: A systematic review. Burns 2014, 40, 177–190. [Google Scholar] [CrossRef]
- Hundeshagen, G.; Collins, V.N.; Wurzer, P.; Sherman, W.; Voigt, C.D.; Cambiaso-Daniel, J.; Lopez, O.N.; Sheaffer, J.; Herndon, D.N.; Finnerty, C.C.; et al. A Prospective, Randomized, Controlled Trial Comparing the Outpatient Treatment of Pediatric and Adult Partial-Thickness Burns with Suprathel or Mepilex Ag. J. Burn Care Res. 2018, 39, 261–267. [Google Scholar] [CrossRef]
- Highton, L.; Wallace, C.; Shah, M. Use of Suprathel® for partial thickness burns in children. Burns 2013, 39, 136–141. [Google Scholar] [CrossRef]
- Keck, M.; Selig, H.F.; Lumenta, D.B.; Kamolz, L.P.; Mittlböck, M.; Frey, M. The use of Suprathel® in deep dermal burns: First results of a prospective study. Burns 2012, 38, 388–395. [Google Scholar] [CrossRef]
- Schwarze, H.; Küntscher, M.; Uhlig, C.; Hierlemann, H.; Prantl, L.; Ottomann, C.; Hartmann, B. Suprathel, a new skin substitute, in the management of partial-thickness burn wounds: Results of a clinical study. Ann. Plast. Surg. 2008, 60, 181–185. [Google Scholar] [CrossRef]
- Uhlig, C.; Rapp, M.; Hartmann, B.; Hierlemann, H.; Planck, H.; Dittel, K.-K. Suprathel-an innovative, resorbable skin substitute for the treatment of burn victims. Burns 2007, 33, 221–229. [Google Scholar] [CrossRef]
- Cattelaens, J.; Turco, L.; Berclaz, L.M.; Huelsse, B.; Hitzl, W.; Vollkommer, T.; Bodenschatz, K.J. The Impact of a Nanocellulose-Based Wound Dressing in the Management of Thermal Injuries in Children: Results of a Retrospective Evaluation. Life 2020, 10, 212. [Google Scholar] [CrossRef] [PubMed]
- Holzer, J.C.J.; Tiffner, K.; Kainz, S.; Reisenegger, P.; Bernardelli de Mattos, I.; Funk, M.; Lemarchand, T.; Laaff, H.; Bal, A.; Birngruber, T.; et al. A novel human ex-vivo burn model and the local cooling effect of a bacterial nanocellulose-based wound dressing. Burns 2020, 46, 1924–1932. [Google Scholar] [CrossRef] [PubMed]
- Nischwitz, S.P.; Bernardelli de Mattos, I.; Hofmann, E.; Groeber-Becker, F.; Funk, M.; Mohr, G.J.; Branski, L.K.; Mautner, S.I.; Kamolz, L.P. Continuous pH monitoring in wounds using a composite indicator dressing—A feasibility study. Burns 2019, 45, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- De Mattos, I.B.; Holzer, J.C.J.; Tuca, A.-C.; Groeber-Becker, F.; Funk, M.; Popp, D.; Mautner, S.; Birngruber, T.; Kamolz, L.-P. Uptake of PHMB in a bacterial nanocellulose-based wound dressing: A feasible clinical procedure. Burns 2019, 45, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Moritz, S.; Wiegand, C.; Wesarg, F.; Hessler, N.; Müller, F.A.; Kralisch, D.; Hipler, U.-C.; Fischer, D. Active wound dressings based on bacterial nanocellulose as drug delivery system for octenidine. Int. J. Pharm. 2014, 471, 45–55. [Google Scholar] [CrossRef]
- Schiefer, J.L.; Aretz, G.F.; Fuchs, P.C.; Bagheri, M.; Funk, M.; Schulz, A.; Daniels, M. Comparison of wound healing and patient comfort in partial-thickness burn wounds treated with SUPRATHEL and epicte(hydro) wound dressings. Int. Wound J. 2021, 19, 782–790. [Google Scholar] [CrossRef]
- Busche, M.N.; Thraen, A.-C.J.; Gohritz, A.; Rennekampff, H.-O.; Vogt, P.M. Burn Scar Evaluation Using the Cutometer® MPA 580 in Comparison to “Patient and Observer Scar Assessment Scale” and “Vancouver Scar Scale”. J. Burn Care Res. 2018, 39, 516–526. [Google Scholar] [CrossRef]
- Draaijers, L.J.; Botman, Y.A.; Tempelman, F.R.; Kreis, R.W.; Middelkoop, E.; van Zuijlen, P.P. Skin elasticity meter or subjective evaluation in scars: A reliability assessment. Burns 2004, 30, 109–114. [Google Scholar] [CrossRef]
- Lee, K.C.; Dretzke, J.; Grover, L.; Logan, A.; Moiemen, N. A systematic review of objective burn scar measurements. Burns Trauma 2016, 4, 14. [Google Scholar] [CrossRef]
- Baumann, M.E.; DeBruler, D.M.; Blackstone, B.N.; Coffey, R.A.; Boyce, S.T.; Supp, D.M.; Bailey, J.K.; Powell, H.M. Direct comparison of reproducibility and reliability in quantitative assessments of burn scar properties. Burns 2021, 47, 466–478. [Google Scholar] [CrossRef]
- Nedelec, B.; Correa, J.A.; Rachelska, G.; Armour, A.; LaSalle, L. Quantitative measurement of hypertrophic scar: Intrarater reliability, sensitivity, and specificity. J. Burn Care Res. 2008, 29, 489–500. [Google Scholar] [CrossRef]
- Busche, M.N.; Roettger, A.; Herold, C.; Vogt, P.M.; Rennekampff, H.-O. Evaporative Water Loss in Superficial to Full Thickness Burns. Ann. Plast. Surg. 2016, 77, 401–405. [Google Scholar] [CrossRef]
- Gardien, K.L.; Baas, D.C.; de Vet, H.C.; Middelkoop, E. Transepidermal water loss measured with the Tewameter TM300 in burn scars. Burns 2016, 42, 1455–1462. [Google Scholar] [CrossRef]
- Merz, K.M.; Pfau, M.; Blumenstock, G.; Tenenhaus, M.; Schaller, H.E.; Rennekampff, H.O. Cutaneous microcirculatory assessment of the burn wound is associated with depth of injury and predicts healing time. Burns 2010, 36, 477–482. [Google Scholar] [CrossRef]
- Sommer, A.; Lucassen, G.W.; Houben, A.J.; Neumann, M.H. Vasoconstrictive effect of topical applied corticosteroids measured by laser doppler imaging and reflectance spectroscopy. Microvasc. Res. 2003, 65, 152–159. [Google Scholar] [CrossRef]
- Thieme, D.; Spilker, G.; Lefering, R.; Weinand, C. O2C Laser Doppler and Digital Photo Analysis for Treatment Evaluation of Beta-Glucan versus Provitamin Pantothenic Acid of Facial Burns. Facial Plast. Surg. 2016, 32, 225–231. [Google Scholar] [CrossRef]
- Baryza, M.J.; Baryza, G.A. The Vancouver Scar Scale: An administration tool and its interrater reliability. J. Burn Care Rehabil. 1995, 16, 535–538. [Google Scholar] [CrossRef]
- Finlay, V.; Burrows, S.; Kendell, R.; Berghuber, A.; Chong, V.; Tan, J.; Edgar, D.W.; Wood, F. Modified Vancouver Scar Scale score is linked with quality of life after burn. Burns 2017, 43, 741–746. [Google Scholar] [CrossRef]
- Finnerty, C.C.; Jeschke, M.G.; Branski, L.K.; Barret, J.P.; Dziewulski, P.; Herndon, D.N. Hypertrophic scarring: The greatest unmet challenge after burn injury. Lancet 2016, 388, 1427–1436. [Google Scholar] [CrossRef]
- Schiefer, J.L.; Rath, R.; Ahrens, E.; Grigutsch, D.; Gräff, I.; Stromps, J.-P.; Fuchs, P.C.; Schulz, A. Evaluation of scar quality after treatment of superficial burns of the hands and face with Dressilk or Biobrane-An intra-individual comparison. Burns 2018, 44, 305–317. [Google Scholar] [CrossRef]
- Kaartinen, I.S.; Kuokkanen, H.O. Suprathel(®) causes less bleeding and scarring than Mepilex(®) Transfer in the treatment of donor sites of split-thickness skin grafts. J. Plast. Surg. Hand Surg. 2011, 45, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Hakkarainen, T.; Koivuniemi, R.; Kosonen, M.; Escobedo-Lucea, C.; Sanz-Garcia, A.; Vuola, J.; Valtonen, J.; Tammela, P.; Mäkitie, A.; Luukko, K.; et al. Nanofibrillar cellulose wound dressing in skin graft donor site treatment. J. Control. Release 2016, 244, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Cubison, T.C.; Pape, S.A.; Parkhouse, N. Evidence for the link between healing time and the development of hypertrophic scars (HTS) in paediatric burns due to scald injury. Burns 2006, 32, 992–999. [Google Scholar] [CrossRef] [PubMed]
- Deitch, E.A.; Wheelahan, T.M.; Rose, M.P.; Clothier, J.; Cotter, J. Hypertrophic burn scars: Analysis of variables. J. Trauma. 1983, 23, 895–898. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dressing | Suprathel® | epicitehydro® | Normal | ||||
|---|---|---|---|---|---|---|---|
| Cutometer | Mean | SD | Mean | SD | Mean | SD | |
| R0 Resistence | 3 months | 0.94 | 0.22 | 0.99 | 0.24 | 1.08 | 0.25 |
| 6 months | 1.06 | 0.32 | 1.16 | 0.36 | 1.10 | 0.24 | |
| 12 months | 1.05 | 0.37 | 1.25 | 0.35 | 1.20 | 0.31 | |
| R2 Gross Elasticity | 3 months | 0.83 | 0.1 | 0.83 | 0.11 | 0.84 | 0.1 |
| 6 months | 0.85 | 0.11 | 0.86 | 0.11 | 0.87 | 0.08 | |
| 12 months | 0.87 | 0.1 | 0.85 | 0.07 | 0.87 | 0.05 | |
| F1 Elasticity | 3 months | 0.13 | 0.06 | 0.14 | 0.05 | 0.14 | 0.06 |
| 6 months | 0.14 | 0.05 | 0.17 | 0.09 | 0.15 | 0.05 | |
| 12 months | 0.14 | 0.09 | 0.15 | 0.04 | 0.16 | 0.06 | |
| Dressing | Suprathel® | epicitehydro® | Normal | ||||
|---|---|---|---|---|---|---|---|
| Mexameter | Mean | SD | Mean | SD | Mean | SD | |
| Melanin | 3 months | 237.1 | 125.8 | 244.6 | 105.3 | 251.2 | 90.7 |
| 6 months | 247.7 | 131.1 | 268.3 | 151.4 | 249.1 | 102.2 | |
| 12 months | 265.6 | 156.5 | 288.7 | 170.5 | 249.3 | 111.0 | |
| Erythema | 3 months | 378.6 | 77.1 | 390.7 | 89.8 | 299.0 | 91.2 |
| 6 months | 359.1 | 85.3 | 376.3 | 72.1 | 270.2 | 93.6 | |
| 12 months | 341.3 | 85.5 | 368.6 | 104.6 | 282.6 | 86.7 | |
| Dressing | Suprathel® | epicitehydro® | Normal | ||||
|---|---|---|---|---|---|---|---|
| Tewameter | Mean | SD | Mean | SD | Mean | SD | |
| TEWL | 3 months | 18.8 | 15.5 | 18.3 | 16.2 | 17.8 | 19.8 |
| 6 months | 16.5 | 11.3 | 16.2 | 11.7 | 13.0 | 11.6 | |
| 12 months | 17.1 | 19.1 | 15.0 | 12.4 | 18.0 | 22.7 | |
| SSWL | 3 months | 2.0 | 1.2 | 2.1 | 2.2 | 1.9 | 2.0 |
| 6 months | 2.0 | 1.6 | 2.3 | 2.3 | 1.6 | 1.8 | |
| 12 months | 2.5 | 3.3 | 3.1 | 3.1 | 3.2 | 5.4 | |
| Dressing | Suprathel® | epicitehydro® | Normal | ||||
|---|---|---|---|---|---|---|---|
| Oxygen2See | Mean | SD | Mean | SD | Mean | SD | |
| sO2 | 3 months | 74.2 | 11.5 | 68.1 | 14.1 | 58.2 | 14.1 |
| 6 months | 73.3 | 17.3 | 61.3 | 16.0 | 63.0 | 12.8 | |
| 12 months | 61.0 | 16.2 | 55.2 | 19.1 | 56.1 | 12.5 | |
| rHb | 3 months | 94.6 | 11.8 | 97.5 | 11.5 | 82.1 | 11.2 |
| 6 months | 95.2 | 11.0 | 97.5 | 8.5 | 85.2 | 10.1 | |
| 12 months | 91.3 | 9.1 | 95.8 | 11.6 | 85.3 | 10.0 | |
| Flow | 3 months | 72.1 | 57.1 | 74.3 | 64.0 | 57.6 | 58.0 |
| 6 months | 73.2 | 69.4 | 77.5 | 102.9 | 42.2 | 30.8 | |
| 12 months | 57.1 | 65.7 | 64.9 | 76.6 | 65.6 | 77.4 | |
| Dressing | Suprathel® | epicitehydro® | |||
|---|---|---|---|---|---|
| VSS Parameter | Mean | SD | Mean | SD | |
| Pigmen-tation | 3 months | 1.5 | 0.607 | 1.45 | 0.686 |
| 6 months | 1.05 | 0.887 | 1.25 | 0.851 | |
| 12 months | 0.90 | 0.912 | 0.95 | 0.887 | |
| Vasculartity | 3 months | 1.25 | 0.444 | 1.15 | 0.366 |
| 6 months | 0.70 | 0.657 | 0.60 | 0.503 | |
| 12 months | 0.35 | 0.587 | 0.30 | 0.571 | |
| Pliability | 3 months | 0.00 | 0.000 | 0.05 | 0.224 |
| 6 months | 0.15 | 0.671 | 0.10 | 0.447 | |
| 12 months | 0.30 | 0.733 | 0.25 | 0.639 | |
| Height | 3 months | 0.15 | 0.366 | 0.10 | 0.447 |
| 6 months | 0.10 | 0.308 | 0.10 | 0.308 | |
| 12 months | 0.25 | 0.550 | 0.10 | 0.308 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schiefer, J.L.; Aretz, F.G.; Fuchs, P.C.; Lefering, R.; Yary, P.; Opländer, C.; Schulz, A.; Daniels, M. Comparison of Long-Term Skin Quality and Scar Formation in Partial-Thickness Burn Wounds Treated with Suprathel® and epicitehydro® Wound Dressings. Medicina 2022, 58, 1550. https://doi.org/10.3390/medicina58111550
Schiefer JL, Aretz FG, Fuchs PC, Lefering R, Yary P, Opländer C, Schulz A, Daniels M. Comparison of Long-Term Skin Quality and Scar Formation in Partial-Thickness Burn Wounds Treated with Suprathel® and epicitehydro® Wound Dressings. Medicina. 2022; 58(11):1550. https://doi.org/10.3390/medicina58111550
Chicago/Turabian StyleSchiefer, Jennifer Lynn, Friederike Genoveva Aretz, Paul Christian Fuchs, Rolf Lefering, Pouyan Yary, Christian Opländer, Alexandra Schulz, and Marc Daniels. 2022. "Comparison of Long-Term Skin Quality and Scar Formation in Partial-Thickness Burn Wounds Treated with Suprathel® and epicitehydro® Wound Dressings" Medicina 58, no. 11: 1550. https://doi.org/10.3390/medicina58111550
APA StyleSchiefer, J. L., Aretz, F. G., Fuchs, P. C., Lefering, R., Yary, P., Opländer, C., Schulz, A., & Daniels, M. (2022). Comparison of Long-Term Skin Quality and Scar Formation in Partial-Thickness Burn Wounds Treated with Suprathel® and epicitehydro® Wound Dressings. Medicina, 58(11), 1550. https://doi.org/10.3390/medicina58111550