
Allograft Vesicoureteral Reflux after Kidney Transplantation

 , , , , and
, , , , and 
Abstract
1. Introduction
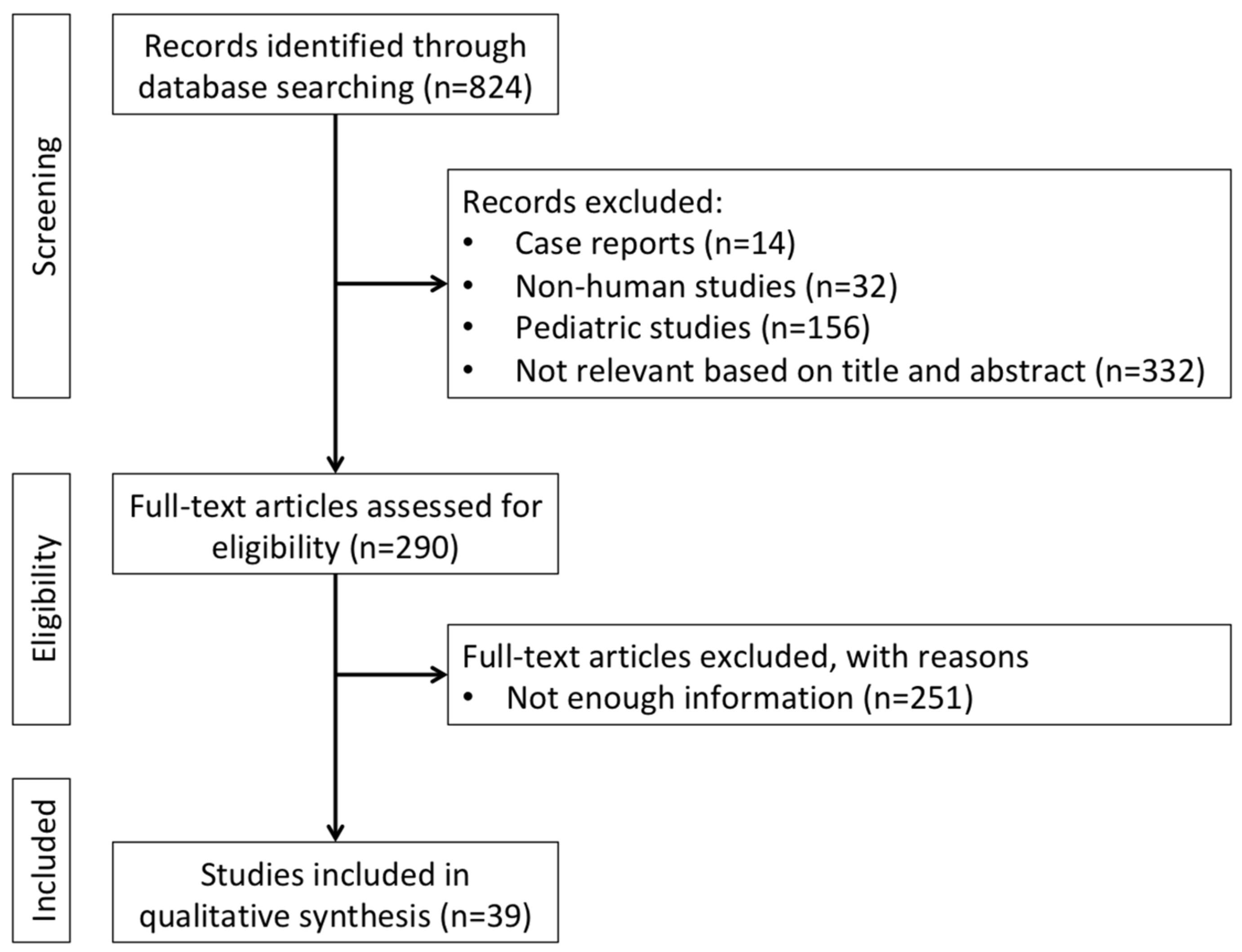
2. Literature Research
3. Epidemiology, Etiology, and Risk Factors for Post-Transplant VUR
4. Clinical Presentation, Diagnosis, and Grading of Post-Transplant VUR
5. Management of Post-Transplant VUR
6. Impact of Post-Transplant VUR on Allograft Function and Survival
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Whang, M.; Yballe, M.; Geffner, S.; Fletcher, H.S.; Palekar, S.; Mulgaonkar, S. Urologic complications in more than 2500 kidney transplantations performed at the Saint Barnabas healthcare system. Transplant. Proc. 2011, 43, 1619. [Google Scholar] [CrossRef] [PubMed]
- Nie, Z.L.; Zhang, K.Q.; Li, Q.S.; Jin, F.S.; Zhu, F.Q.; Huo, W.Q. Urological Complications in 1223 Kidney Transplantations. Urol. Int. 2009, 83, 337–341. [Google Scholar] [CrossRef]
- Zavos, G.; Pappas, P.; Karatzas, T.; Karidis, N.; Bokos, J.; Stravodimos, K.; Theodoropoulou, E.; Boletis, J.; Kostakis, A. Urological Complications: Analysis and Management of 1525 Consecutive Renal Transplantations. Transplant. Proc. 2008, 40, 1386–1390. [Google Scholar] [CrossRef] [PubMed]
- Williams, G.; Fletcher, J.T.; Alexander, S.I.; Craig, J.C. Vesicoureteral Reflux. J. Am. Soc. Nephrol. 2008, 19, 847–862. [Google Scholar] [CrossRef]
- Tekgül, S.; Riedmiller, H.; Hoebeke, P.; Kočvara, R.; Nijman, R.J.; Radmayr, C.; Stein, R.; Dogan, H.S. EAU Guidelines on Vesicoureteral Reflux in Children. Eur. Urol. 2012, 62, 534–542. [Google Scholar] [CrossRef]
- Mattoo, T.K.; Chesney, R.W.; Greenfield, S.P.; Hoberman, A.; Keren, R.; Mathews, R.; Gravens-Mueller, L.; Ivanova, A.; Carpenter, M.A.; Moxey-Mims, M.; et al. RIVUR Trial Investigators. Renal Scarring in the Randomized Intervention for Children with Vesicoureteral Reflux (RIVUR). Trial. Clin. J. Am. Soc. Nephrol. 2016, 11, 54–61. [Google Scholar] [CrossRef]
- Gołębiewska, J.; Dębska-Ślizień, A.; Komarnicka, J.; Samet, A.; Rutkowski, B. Urinary tract infections in renal trans-plant recipients. Transplant. Proc. 2011, 43, 2985–2990. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Transplant. 2009, 9 (Suppl. 3), S1–S155. [Google Scholar]
- Ostrowski, M.; Włodarczyk, Z.; Wesołowski, T.; Gracz, H.; Sluzar, T.; Sieńko, J.; Lubikowski, J.; Bohatyrewicz, R. Influence of ureterovesical anastomosis technique on the incidence of vesicoureteral reflux in renal transplant recipients. Ann. Transplant. 1999, 4, 54–58. [Google Scholar]
- Mastrosimone, S.; Pignata, G.; Maresca, M.C.; Calconi, G.; Rabassini, A.; Butini, R.; Fandella, A.; Di Falco, G.; Chiara, G.; Caldato, C. Clinical significance of vesicoureteral reflux after kidney transplantation. Clin. Nephrol. 1993, 40, 38–45. [Google Scholar]
- Sui, W.; Lipsky, M.J.; Matulay, J.T.; Robins, D.J.; Onyeji, I.C.; James, M.B.; Theofanides, M.C.; Wenske, S. Timing and Predictors of Early Urologic and Infectious Complications After Renal Transplant: An Analysis of a New York Statewide Database. Exp. Clin. Transplant. 2018, 16, 665–670. [Google Scholar]
- Whang, M.; Benson, M.; Salama, G.; Geffner, S.; Sun, H.; Aitchison, S.; Mulgaonkar, S. Urologic Complications in 4000 Kidney Transplants Performed at the Saint Barnabas Health Care System. Transplant. Proc. 2020, 52, 186–190. [Google Scholar] [CrossRef]
- Gołębiewska, J.; Dębska-Ślizień, A.; Zadrożny, D.; Rutkowski, B. Acute Graft Pyelonephritis During the First Year After Renal Transplantation. Transplant. Proc. 2014, 46, 2743–2747. [Google Scholar] [CrossRef]
- Dinckan, A.; Aliosmanoglu, I.; Kocak, H.; Gunseren, F.; Mesci, A.; Ertug, Z.; Yucel, S.; Suleymanlar, G.; Gurkan, A. Surgical correction of vesico-ureteric reflux for recurrent febrile urinary tract infections after kidney transplantation. BJU Int. 2013, 112, E366. [Google Scholar] [CrossRef]
- Farr, A.; Györi, G.; Mühlbacher, F.; Husslein, P.; Böhmig, G.A.; Margreiter, M. Gender has no influence on VUR rates after renal transplantation. Transpl. Int. 2014, 27, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-L.; Lee, M.-C.; Kuo, H.-C. Reduction of cystometric bladder capacity and bladder compliance with time in patients with end-stage renal disease. J. Formos. Med. Assoc. 2012, 111, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Serrano, D.P.; Flechner, S.M.; Modlin, C.S.; Wyner, L.M.; Novick, A.C. Transplantation into the long-term defunctionalized bladder. J. Urol. 1996, 156, 885–888. [Google Scholar] [CrossRef]
- Hotta, K.; Miura, M.; Wada, Y.; Fukuzawa, N.; Iwami, D.; Sasaki, H.; Seki, T.; Harada, H. Atrophic bladder in long-term dialysis patients increases the risk for urological complications after kidney transplantation. Int. J. Urol. 2017, 24, 314–319. [Google Scholar] [CrossRef]
- Inoue, T.; Satoh, S.; Saito, M.; Numakura, K.; Tsuruta, H.; Obara, T.; Narita, S.; Horikawa, Y.; Tsuchiya, N.; Habuchi, T. Correlations Between Pretransplant Dialysis Duration, Bladder Capacity, and Prevalence of Vesicoureteral Reflux to the Graft. Transplant 2011, 92, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Satoh, S.; Obara, T.; Saito, M.; Numakura, K.; Narita, S.; Tsuchiya, N.; Habuchi, T. Cystometric evaluation of recovery in hypocompliant defunctionalized bladder as a result of long-term dialysis after kidney transplantation. Int. J. Urol. 2016, 23, 694–700. [Google Scholar] [CrossRef]
- Gregoir, W. Congenital vesico-ureteral reflux. Acta Urol. Belg. 1962, 30, 286–300. [Google Scholar] [CrossRef] [PubMed]
- Lich, R., Jr.; Howerton, L.W.; Davis, L.A. Childhood urosepsis. J. Ky Med. Assoc. 1961, 59, 1177–1179. [Google Scholar]
- Politano, V.A.; Leadbetter, W.F. An operative technique for the correction of vesicoureteral reflux. J. Urol. 1958, 79, 932–941. [Google Scholar] [CrossRef]
- Kayler, L.; Kang, D.; Molmenti, E.; Howard, R. Kidney transplant ureteroneocystostomy techniques and complications: Review of the literature. Transplant. Proc. 2010, 42, 1413–1420. [Google Scholar] [CrossRef] [PubMed]
- Shanfield, I. New experimental methods for implantation of the ureter in bladder and conduit. Transplant. Proc. 1972, 4, 637–638. [Google Scholar] [PubMed]
- Duty, B.D.; Barry, J.M. Diagnosis and management of ureteral complications following renal transplantation. Asian J. Urol. 2015, 2, 202–207. [Google Scholar] [CrossRef][Green Version]
- Alberts, V.P.; Idu, M.M.; Legemate, D.A.; Pes, M.P.L.; Minnee, R.C. Ureterovesical anastomotic techniques for kidney transplantation: A systematic review and meta-analysis. Transpl. Int. 2014, 27, 593–605. [Google Scholar] [CrossRef] [PubMed]
- Cash, H.; Slowinski, T.; Buechler, A.; Grimm, A.; Friedersdorff, F.; Schmidt, D.; Miller, K.; Giessing, M.; Fuller, T.F. Impact of surgeon experience on complication rates and functional outcomes of 484 deceased donor renal transplants: A single-centre retrospective study. BJU Int. 2012, 110, E368–E373. [Google Scholar] [CrossRef]
- Gołębiewska, J.E.; Dębska-Ślizień, A.; Rutkowski, B. Urinary tract infections during the first year after renal transplantation: One center’s experience and a review of the literature. Clin. Transplant. 2014, 28, 1263–1270. [Google Scholar] [CrossRef]
- Margreiter, M.; Györi, G.P.; Böhmig, G.A.; Trubel, S.; Mühlbacher, F.; Steininger, R. Value of routine voiding cystourethrography after renal transplantation. Am. J. Transplant. 2013, 13, 130–135. [Google Scholar] [CrossRef]
- Lebowitz, R.L.; Olbing, H.; Parkkulainen, K.V.; Smellie, J.M.; Tamminen-Möbius, T.E. International system of radio-graphic grading of vesicoureteric reflux. International Reflux Study in Children. Pediatr. Radiol. 1985, 15, 105–109. [Google Scholar] [CrossRef]
- Stenberg, A.; Lackgren, G. A New Bioimplant for the Endoscopic Treatment of Vesicoureteral Reflux: Experimental and Short-term Clinical Results. J. Urol. 1995, 154, 800–803. [Google Scholar] [CrossRef]
- Yang, K.K.; Moinzadeh, A.; Sorcini, A. Minimally-Invasive Ureteral Reconstruction for Ureteral Complications of Kidney Transplants. Urology 2019, 126, 227–231. [Google Scholar] [CrossRef]
- Di Carlo, H.N.; Darras, F.S. Urologic considerations and complications in kidney transplant recipients. Adv. Chronic Kidney Dis. 2015, 22, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Kim, K.; Choi, S.; Bae, W.; Hong, S.; Lee, J.; Kim, J.; Kim, S.; Chung, B.; Yang, C.; et al. Ureteral Complications in Kidney Transplantation: Analysis and Management of 853 Consecutive Laparoscopic Living-Donor Nephrectomies in a Single Center. Transplant. Proc. 2016, 48, 2684–2688. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.; Geffner, S.; Sun, H.; Whang, M. Surgical Treatment of Vesicoureteral Reflux in Kidney Transplant Patients with Symptomatic Urinary Tract Infection: A Single Institution Review of 123 Patients. Clin. Surg. 2016, 1, 1160. [Google Scholar]
- Turunç, V.; Eroğlu, A.; Tabandeh, B.; Erol, A. Comparison of Surgical Correction Techniques for Post-Renal Transplantation Vesicoureteral Reflux. Transplant. Proc. 2017, 49, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Lucas, B.A.; McRoberts, J.W.; Curtis, J.J.; Luke, R.G. Controversy in Renal Transplantation: Antireflux Versus Non-Antireflux Ureteroneocystostomy. J. Urol. 1979, 121, 156–158. [Google Scholar] [CrossRef]
- Jung, G.O.; Chun, J.M.; Park, J.B.; Choi, G.S.; Kwon, C.H.; Joh, J.W.; Lee, S.K.; Kim, S.J. Clinical significance of posttransplan-tation vesicoureteral reflux during short-term period after kidney transplantation. Transplant. Proc. 2008, 40, 2339–2341. [Google Scholar] [CrossRef]
- Favi, E.; Spagnoletti, G.; Valentini, A.; Tondolo, V.; Nanni, G.; Citterio, F.; Castagneto, M. Long-Term Clinical Impact of Vesicoureteral Reflux in Kidney Transplantation. Transplant. Proc. 2009, 41, 1218–1220. [Google Scholar] [CrossRef]
- Coulthard, M.G.; Keir, M.J. Reflux Nephropathy in Kidney Transplants, Demonstrated by Dimercaptosuccinic Acid Scanning. Transplantaton 2006, 82, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Ohba, K.; Matsuo, M.; Noguchi, M.; Nishikido, M.; Koga, S.; Kanetake, H.; Nazneen, A.; Liu, D.; Razzaque, M.S.; Taguchi, T. Clinicopathological study of vesicoureteral reflux (VUR)-associated pyelonephritis in renal transplantation. Clin. Transplant. 2004, 18 (Suppl. 11), 34–38. [Google Scholar] [CrossRef]
- Mathew, T.H.; Mathews, D.C.; Hobbs, J.B.; Kincaid-Smith, P. Glomerular lesions after renal transplantation. Am. J. Med. 1975, 59, 177–190. [Google Scholar] [CrossRef]
- Kmetec, A.; Buturović-Ponikvar, J.; Kandus, A.; Bren, A.F. The value of renal resistive index for the detection of vesicoureteral reflux in renal transplant recipients. Transplant. Proc. 2001, 33, 3385–3387. [Google Scholar] [CrossRef]
- Praz, V.; Leisinger, H.-J.; Pascual, M.; Jichlinski, P. Urological Complications in Renal Transplantation from Cadaveric Donor Grafts: A Retrospective Analysis of 20 Years. Urol. Int. 2005, 75, 144–149. [Google Scholar] [CrossRef]
- Obara, T.; Satoh, S.; Inoue, T.; Komine, N.; Numakura, K.; Narita, S.; Horikawa, Y.; Tsuchiya, N.; Habuchi, T. Impact of Pretransplant Dialysis Duration, Bladder Capacity and Length of Submucosal Tunnel of Ureteroneocystostomy on the Prevalence of Vesicoureteral Reflux to the Graft. In Meeting Abstracts of the 24th International Congress of the Transplantation Society, Berlin, Germany, 14–19 July 2012. Transplantation 2012, 94, 269. [Google Scholar] [CrossRef]
- Sandhu, K.; Masters, J.; Ehrlich, Y. Ureteropyelostomy using the native ureter for the management of ureteric obstruction or symptomatic reflux following renal transplantation. Urology 2012, 79, 929–932. [Google Scholar] [CrossRef]
- Li Marzi, V.; Del Popolo, G.; Filocamo, M.T.; Milanesi, M.; Cocci, A.; Tosto, A.; Nicita, G. Our experience related to uro-dynamic assessment in renal transplant recipients. In Abstracts from the 37th Annual Congress of the Italian Urodynamic Society, Latina, Italy, 20–22 June 2013. Neurourol. Urodyn. 2013, 32, S1–S58. [Google Scholar]
- Riediger, C.; Müller, M.W.; Bachmann, J.; Novotny, A.; Thorban, S.; Matevossian, E.; Friess, H.; Stangl, M. Native ureteropyelostomy: An effective therapy for urinary tract complications following kidney transplantation. ANZ J. Surg. 2014, 84, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Soliman, M.; Ghazanfar, A.; Bagul, A.; Salem, A.; Ali, A.; Wadoodi, A.; Heap, S.; Morsy, M. Incidence and outcome of post-transplant urological complications in kidney transplantation after expanding acceptance criteria: Single centre experience. In Abstracts of the 2016 TTS Congress, Hong Kong, China, 18–23 August. Transplantation 2016, 100, S641. [Google Scholar]
- Koçak, T.; Nane, I.; Ander, H.; Ziylan, O.; Oktar, T.; Ozsoy, C. Urological and surgical complications in 789 consecutive living related donor kidney transplantations. In Proceedings of the Abstracts of the 18th Congress of the European Society for Organ Transplantation, Barcelona, Spain, 24–27 September 2017. Urol. Int. 2004, 72, 252–256. [Google Scholar] [CrossRef]
- Gutiérrez-Jiménez, A.A.; Jiménez-López, L.A.; Ricardez-Espinosa, A.A.; Santos-Uscanga, J.P.; Aguilar-Sandoval, E.G.; Vega-Tepos, I.E.; George-Micceli, E. Endourological application of polydimetilsiloxane in patients with symptomatic vesicoureteral reflux in the kidney graft. Actas Urol. Esp. (Engl. Ed.) 2019, 43, 262. [Google Scholar] [CrossRef] [PubMed]
- Di Lascio, G.; Di Pierro, G.B.; Angelini, F.; Cantisani, V.; Drudi, F.M.; Lemma, A.; Cristini, C. Contrast-Enhanced voiding ultrasonography in the evaluation of vesicoureteral reflux: Comparison with voiding cystourethrography and proposal of a new classification system. In Abstracts from the 93rd National Congress of the Italian Society of Urology, Rome, Italy, 17–18 October. Eur. Urol. Open Sci. 2020, 20, S98. [Google Scholar]
- Ladhari, N.; Azzabi, A.; Sahtout, W.; Guedri, Y.; Mrabet, S.; Fradi, A.; Zallema, D.; Abdellatif, A. Nosocomial infections in kidney transplant patients: A single center experience. In Abstracts from the 2021 ISN World Congress of Nephrology, Montreal, Canada, 15–19 April 2021. Kidney Int. Rep. 2021, 6, S341. [Google Scholar] [CrossRef]


{kind=link}
| Unmodifiable Risk Factors |
|---|
| Female sex |
| Non-Caucasian ethnicity |
| Age at transplant |
| Lower urinary tract abnormalities |
| Atrophic bladder |
| Dialysis vintage |
| Hypertension |
| Type 2 Diabetes mellitus |
| Modifiable risk factors |
| Surgical technique for ureteral implantation |
| Surgical expertise |
| Diagnosis | Pros | Cons |
|---|---|---|
| Doppler US scan | ready-to-use | non-functional evaluation |
| non-invasive | operator dependent | |
| Contrast-enhanced CT scan | high resolution | non-functional evaluation |
| reproducible | contrast-induced nephropathy | |
| radiation exposure | ||
| Voiding VCUG | gold standard | availability/expertise |
| lack of standardized protocols | ||
| radiation exposure | ||
| Management | Pros | Cons |
| Wait and see | non-invasive | risk of future infections |
| Antibiotic suppression | non-invasive | does not affect reflux |
| antibiotic resistance | ||
| drug-induced side effects | ||
| Endoscopic polymer injection | minimally invasive | Grade I-III reflux |
| high success rate | availability/expertise | |
| repeatable | ||
| Ureteral reimplantation | very high success rate | invasive |
| Grade IV-V reflux | expertise |
| Authors | Year | Period | Participants (n) | Type of Population | Cases with VUR (n, M/F) | Incidence (%) | Mean Age at KT (Years) | Mean HD Duration (Months) | Cases with Symptoms (n) |
|---|---|---|---|---|---|---|---|---|---|
| Mathew TH et al. [43] | 1975 | - | 72 | recipients | 27 | 38 | - | - | - |
| Lucas BA et al. [38] | 1979 | 1972–1975 | 112 | allografts | - | <10 | - | - | - |
| Matrosimone S et al. [10] | 1993 | 1985–1991 | 103 | recipients | 89 (63/26) | 86 | 40 | 65 ± 10 | 4 |
| Ostrowski M et al. [9] | 1999 | 1984–1996 | 39 | recipients | 12 | 31 | - | - | 0 |
| Kmetec A et al. [44] | 2001 | - | 23 | recipients with UTI | 16 | 70 | 39 | - | 23 |
| Ohba K et al. [42] | 2004 | 1990–2001 | 131 | renal biopsies | 7 | 5 | - | - | 12 |
| Praz V e al. [45] | 2005 | 1979–1999 | 277 | allografts | 4 | 1 | 45 | - | - |
| Coulthard MG et al. [41] | 2006 | 1994–2005 | 30 | recipients | 19 | 63 | 10 | - | - |
| Jung GO et al. [39] | 2008 | 2005–2006 | 75 | recipients | 47 | 63 | 42 | 36 vs. 30 | - |
| Nie ZL et al. [2] | 2009 | 1993–2007 | 1223 | recipients | 14 | 1 | - | - | - |
| Favi E et al. [40] | 2009 | - | 37 | recipients | 15 (9/6) | 41 | 41 ± 13 | - | - |
| Kayler L et al. [24] | 2010 | review | - | - | - | - | - | - | - |
| Whang M et al. [1] | 2011 | 1993–2009 | 2548 | recipients | 78 (16/72) | 3 | - | - | 78 |
| Gołębiewska J et al. [7] | 2011 | 2009–2010 | 89 | recipients | 7 | 8 | 48 ± 14 | 25 ± 24 | 58 |
| Inoue T et al. [19] | 2011 | 2010–2011 | 101 | recipients | 30 | 30 | 42 | 32 | - |
| Obara T et al. [46] | 2012 | 1998–2006 | 164 | recipients | 36 | 22 | 46 | 60 | - |
| Sandhu K et al. [47] | 2012 | 2000–2009 | - | - | 2 | - | 31 | - | - |
| Dinckan A et al. [14] | 2013 | 2000–2008 | 1673 | recipients | 60 (28/32) | 4 | - | - | - |
| Margreiter M et al. [30] | 2013 | 1999–2007 | 646 | recipients | 263 | 41 | 53 | - | - |
| Marzi VL et al. [48] | 2013 | 2002–2012 | 14 | recipients | 2 | 14 | 38 | 13 | - |
| Gołębiewska J et al. [13] | 2014 | 2007–2009 | 209 | recipients | - | - | 46 ± 14 | - | - |
| Farr A et al. [15] | 2014 | 2001–2007 | 598 | recipients | 237 (167/70) | 40 | 54 | - | 237 |
| Alberts VP et al. [27] | 2014 | review | - | - | - | - | - | - | - |
| Gołębiewska J et al. [29] | 2014 | 2007–2009 | 209 | recipients | 19 | 9 | 48 ± 14 | 29 ± 35 | 19 |
| Riediger C et al. [49] | 2014 | 2001–2009 | 646 | allografts | 10 (3/7) | 2 | 55 | - | - |
| Duty BD et al. [26] | 2015 | review | - | - | - | - | - | - | - |
| Di Carlo HN et al. [34] | 2015 | review | - | - | - | - | - | - | - |
| Inoue T et al. [20] | 2016 | 2009–2012 | 61 | recipients | 16 | 26 | - | 22 | - |
| Choi YS et al. [35] | 2016 | 2000–2014 | 853 | recipients | 24 | 3 | - | - | - |
| Soliman M et al. [50] | 2016 | 2013–2014 | 203 | allografts | 1 | 0 | - | - | - |
| Hotta K et al. [18] | 2017 | 1996–2011 | 347 | recipients | 191 | 55 | 43 ± 14 | - | 32 |
| Turunç V et al. [37] | 2017 | 2010–2014 | 812 | recipients | 38 (26/12) | 5 | 45 | - | 38 |
| Nane I et al. [51] | 2017 | 1983–2017 | 789 | allografts | 9 | 1 | - | - | 9 |
| Sui W et al. [11] | 2018 | 2005–2013 | 9038 | recipients | 99 | 1 | 52 ± 14 | - | - |
| Yang KK et al. [33] | 2019 | 2011–2018 | 262 | recipients | - | - | - | - | 3 |
| Gutiérrez-Jiménez AA et al. [52] | 2019 | 2010–2018 | 23 | recipients with UTI | 23 (10/13) | 100 | 34 | - | 23 |
| Whang M et al. [12] | 2020 | 1993–2016 | 3890 | recipients | 168 (44/124) | 4 | 48 | - | - |
| Di Lascio G et al. [53] | 2020 | 2017–2019 | 84 | allografts | 84 | 100 | - | - | - |
| Ladhari N et al. [54] | 2021 | 2007–2018 | 209 | allografts | 31 (19/12) | 15 | 28 | 12 | 10 |
| Authors | Clinical Manifestation | Diagnosis | Classification | Grade (n) | Treatment (n) | Success (%) | Graft Survival a (%) | Loss of Function | Patient Survival a (%) |
|---|---|---|---|---|---|---|---|---|---|
| Mathew TH et al. [43] | - | - | - | - | - | - | - | - | - |
| Lucas BA et al. [38] | - | - | - | - | - | - | 58 | - | - |
| Matrosimone S et al. [10] | recurrent UTIs hypertension | VCUG | Ransley PG et al. [54] | I-II (62) III (27) | antibiotics | - | 100 | no | 99 |
| Ostrowski M et al. [9] | - | VCUG | - | - | - | - | - | - | |
| Kmetec A et al. [44] | recurrent UTIs | VCUG | - | I-II (9) III (7) | - | - | - | - | - |
| Ohba K et al. [42] | pyuria pyelonephritis | VCUG | - | - | - | - | - | - | - |
| Praz V et al. [45] | - | - | - | - | - | - | - | - | - |
| Coulthard MG et al. [41] | UTIs nephropathy | VCUG MAG3 DMSA scan | - | - | - | - | - | - | - |
| Jung GO et al. [39] | UTIs rejection loss of function | VCUG | IRCS | I (6) II (22) III (17) IV (2) | - | - | - | -- | |
| Nie ZL et al. [2] | - | VCUG | - | - | antibiotics (8) surgery (6) | 93 | 100 | 88 | |
| Favi E et al. [40] | UTIs, loss of renal function | VCUG | IRCS | I II III | - | - | 91 | no | 84 |
| Kayler L et al. [24] | - | - | - | - | - | - | - | - | - |
| Whang M et al. [1] | UTIs | VCUG | - | - | Antibiotics copolymer injection surgery | 26, 0, 74 | - | - | - |
| Gołębiewska J et al. [7] | lower UTIs upper UTIs bacteremia | - | - | - | antibiotics | - | - | - | - |
| Inoue T et al. [19] | loss of function | VCUG | IRSC | - | - | - | - | - | - |
| Obara T et al. [46] | - | VCUG | - | - | - | - | - | - | - |
| Sandhu K et al. [47] | AGPN | - | - | - | ureteropyelostomy (native ureter) | 100 | 100 | no | 100 |
| Dinckan A et al. [14] | recurrent UTIs | VCUG | - | III (8) IV (40) V (12) | reconstruction | - | 100 | - | - |
| Margreiter M et al. [30] | UTIs loss of function | VCUG | IRCS | I (51) II (128) III (66) IV (18) | - | - | - | yes | - |
| Marzi VL et al. [48] | - | VCUG | - | - | - | - | - | - | - |
| Gołębiewska J et al. [13] | - | - | - | - | - | - | - | - | - |
| Farr A et al. [15] | UTIs hydronephrosis | VCUG US | - | I (46) II (120) III (54) IV (17) | - | - | - | - | - |
| Alberts VP et al. [27] | - | - | - | - | - | - | - | - | - |
| Gołębiewska J et al. [29] | recurrent UTIs AGPN sepsis | - | - | - | - | - | - | - | - |
| Riediger C et al. [49] | - | - | - | - | ureteropyelostomy (native ureter) | 100 | 80 | no | 90 |
| Duty BD et al. [26] | - | - | - | - | - | - | - | - | - |
| Di Carlo HN et al. [34] | - | - | - | - | - | - | - | - | - |
| Inoue T et al. [20] | - | VCUG max IV pressure | IRSC | I-II (11) III-IV (5) | - | - | - | - | - |
| Choi YS et al. [35] | UTIs | VCUG | - | - | copolymer injection | 71 | - | - | - |
| Soliman M et al. [50] | - | - | - | - | medical treatment | - | - | no | - |
| Hotta K et al. [18] | UTIs graft scarring | VCUG | - | - | - | - | - | - | - |
| Turunç V et al. [37] | recurrent UTIs | VCUG | IRCS | - | surgery | 95 | 100 | - | 100 |
| Nane I et al. [51] | - | - | - | - | - | - | - | - | - |
| Sui W et al. [11] | UTIs | - | - | - | - | - | - | - | - |
| Yang KK et al. [33] | AGPN | VCUG | IRCS | III (3) | copolymer injection surgery | 0 100 | - | - | - |
| Gutiérrez-Jiménez AA et al. [52] | AGPN | VCUG | IRCS | II (3) III (11) IV (9) | copolymer injection | 78 | 74 | - | - |
| Whang M et al. [12] | UTIs loss of function | VCUG | - | - | antibiotics copolymer injection surgery | - 0 - | - | - | - |
| Di Lascio G et al. [53] | - | VCUG CEUS | - | I (18) II (47) III (7) | - | - | - | - | - |
| Ladhari N et al. [54] | recurrent UTIs | - | - | - | - | - | 60 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brescacin, A.; Iesari, S.; Guzzo, S.; Alfieri, C.M.; Darisi, R.; Perego, M.; Puliatti, C.; Ferraresso, M.; Favi, E. Allograft Vesicoureteral Reflux after Kidney Transplantation. Medicina 2022, 58, 81. https://doi.org/10.3390/medicina58010081
Brescacin A, Iesari S, Guzzo S, Alfieri CM, Darisi R, Perego M, Puliatti C, Ferraresso M, Favi E. Allograft Vesicoureteral Reflux after Kidney Transplantation. Medicina. 2022; 58(1):81. https://doi.org/10.3390/medicina58010081
Chicago/Turabian StyleBrescacin, Alessandra, Samuele Iesari, Sonia Guzzo, Carlo Maria Alfieri, Ruggero Darisi, Marta Perego, Carmelo Puliatti, Mariano Ferraresso, and Evaldo Favi. 2022. "Allograft Vesicoureteral Reflux after Kidney Transplantation" Medicina 58, no. 1: 81. https://doi.org/10.3390/medicina58010081
APA StyleBrescacin, A., Iesari, S., Guzzo, S., Alfieri, C. M., Darisi, R., Perego, M., Puliatti, C., Ferraresso, M., & Favi, E. (2022). Allograft Vesicoureteral Reflux after Kidney Transplantation. Medicina, 58(1), 81. https://doi.org/10.3390/medicina58010081