
Necrotizing Fasciitis of the Thigh as Unusual Colonoscopic Polypectomy Complication: Review of the Literature with Case Presentation

 ,
, 
 , ,
, ,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Case Report
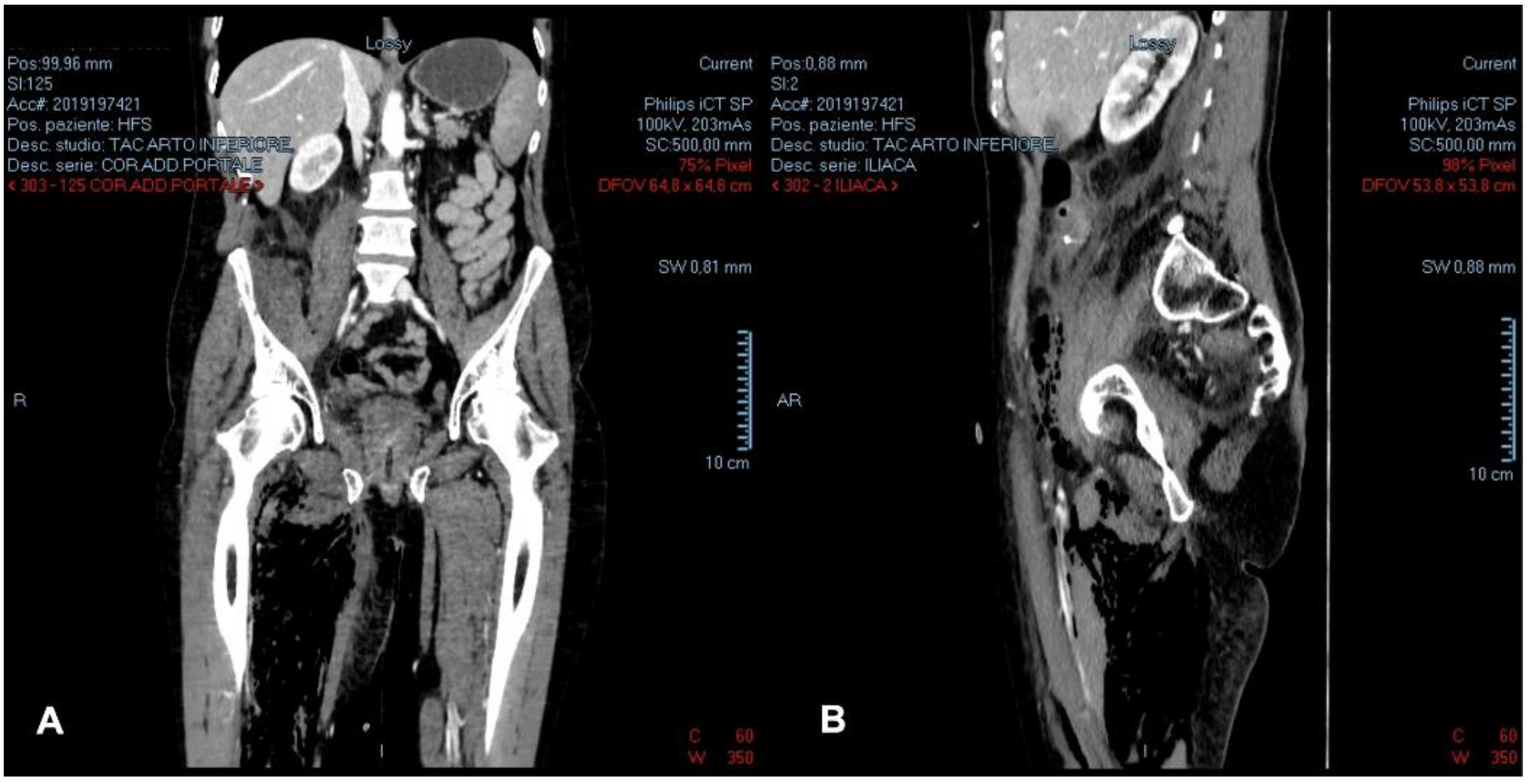
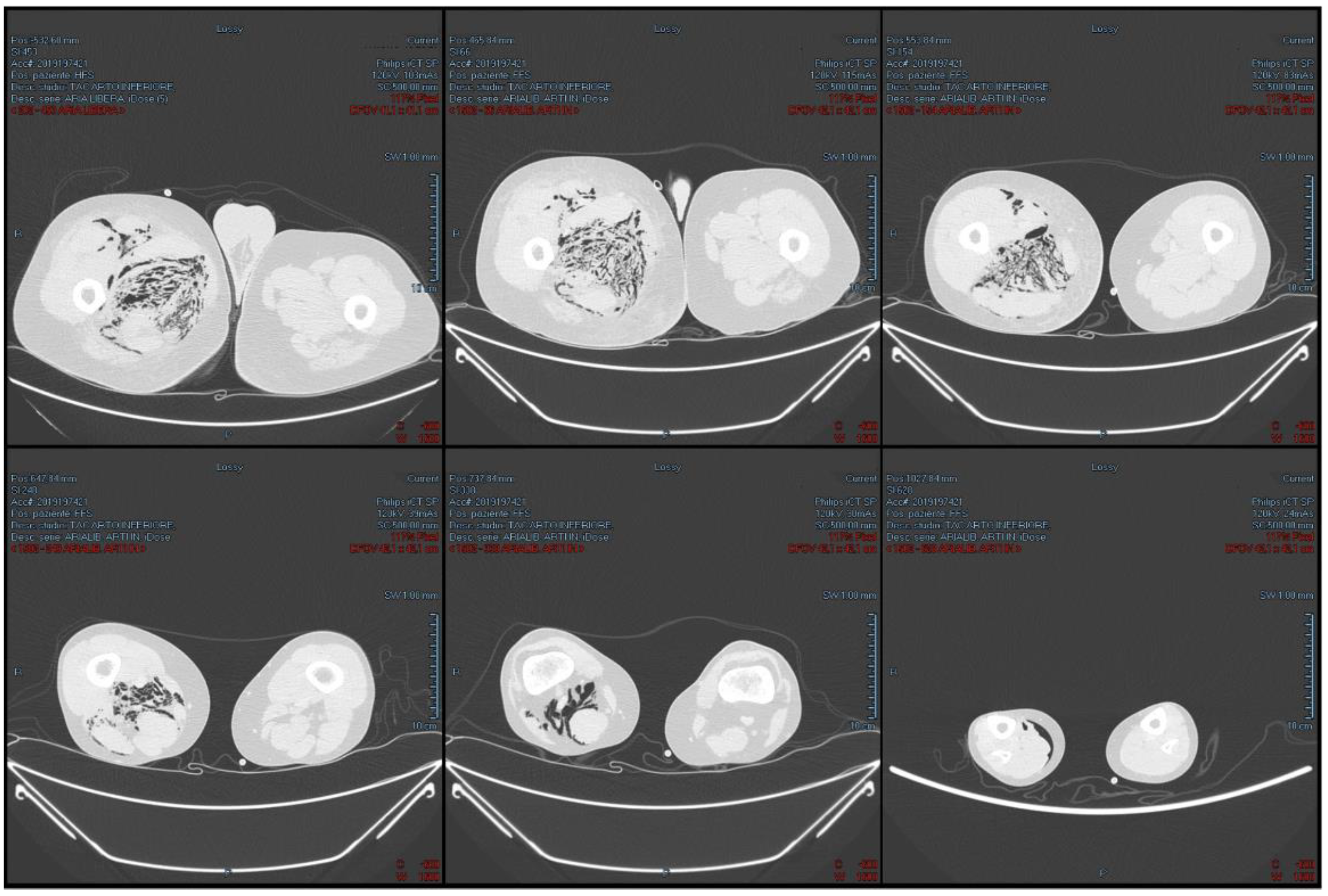
2.1. The Clinical, Surgical, and Radiological Data
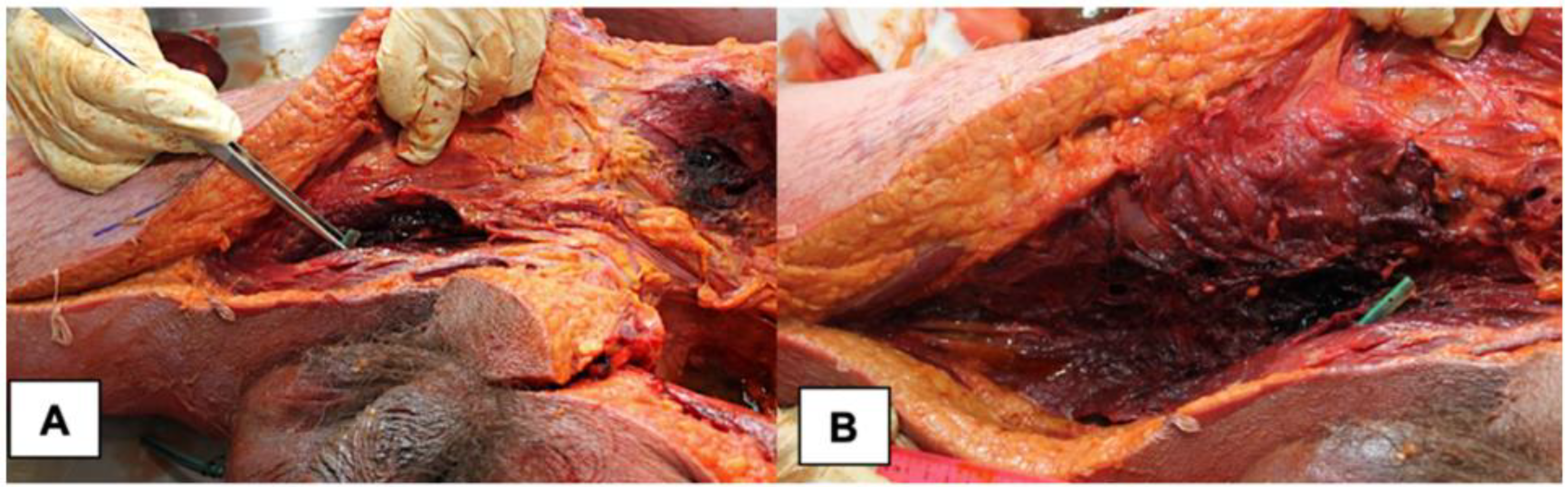
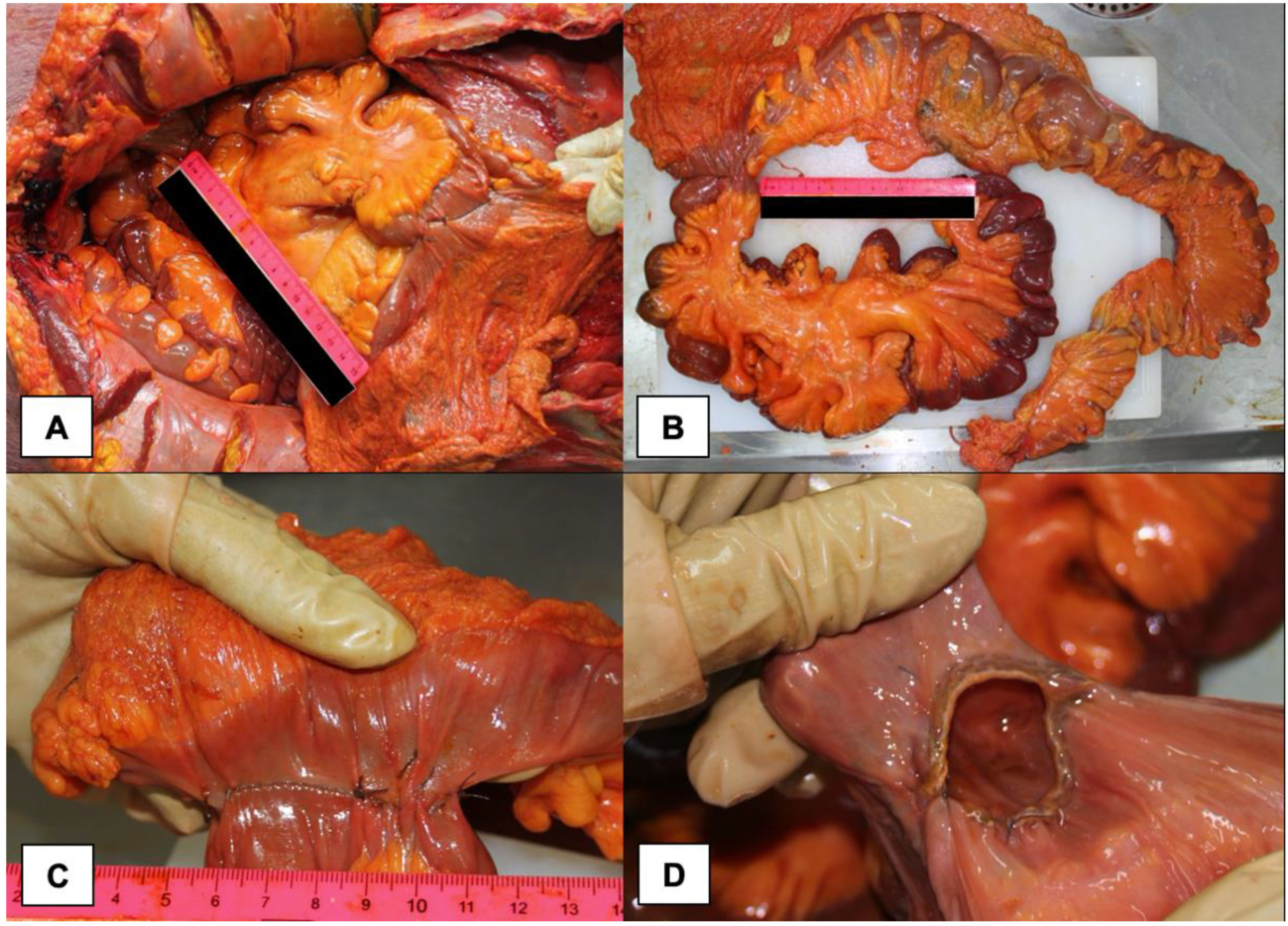
2.2. Autopsy and Histopathology Findings
3. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, L.L.; Fasolka, B.; Treacy, C. Necrotizing fasciitis: A comprehensive review. Nursing 2020, 50, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Kaul, R.; McGeer, A.; Low, D.E.; Green, K.; Schwartz, B. Population-based surveillance for group A streptococcal necrotizing fasciitis: Clinical features, prognostic indicators, and microbiologic analysis of seventy-seven cases. Am. J. Med. 1997, 103, 18–24. [Google Scholar] [CrossRef]
- Levine, E.G.; Manders, S.M. Life-threatening necrotizing fasciitis. Clin. Dermatol. 2005, 23, 144–147. [Google Scholar] [CrossRef]
- Catena, F.; Moore, F. Expression of concern: Necrotizing fasciitis, literature review of contemporary strategies for diagnosing and management with three case reports: Torso, abdominal wall, upper and lower limbs. World J. Emerg. Surg. 2012, 7, 1–17. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sorensen, M.D.; Krieger, J.N.; Rivara, F.P.; Klein, M.B.; Wessells, H. Fournier’s Gangrene: Management and Mortality Predictors in a Population Based Study. J. Urol. 2009, 182, 2742–2747. [Google Scholar] [CrossRef]
- Wiberg, A.; Carapeti, E.; Greig, A. Necrotising fasciitis of the thigh secondary to colonic perforation: The femoral canal as a route for infective spread. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 1731–1733. [Google Scholar] [CrossRef]
- Lonie, S.; Rozen, W.N.; Seifman, M. Necrotizing fasciitis following colonoscopy in the setting of ulcerative colitis. ANZ J. Surg. 2019, 89, E546–E547. [Google Scholar] [CrossRef]
- Sun, W.-C.; Tsai, T.-J.; Chen, W.-C. Fournier’s Gangrene Secondary to Necrotizing Pancreatitis After Endoscopic Retrograde Cholangiopancreatography. Am. J. Gastroenterol. 2021, 116, 1373. [Google Scholar] [CrossRef]
- Stevens, D.L.; Bryant, A.E. Necrotizing soft-tissue infections. New Eng. J. Med. 2017, 377, 2253–2265. [Google Scholar] [CrossRef]
- Andreasen, T.J.; Green, S.D.; Childers, B.J. Massive infectious soft-tissue injury: Diagnosis and management of necrotizing fasciitis and purpura fulminans. Plast. Reconstr. Surg. 2001, 107, 1025–1035. [Google Scholar] [CrossRef]
- Stamenkovic, I.; Lew, P.D. Early recognition of potentially fatal necrotizing fasciitis: The use of frozen section biopsy. New Engl. J. Med. 1984, 310, 1689–1693. [Google Scholar] [CrossRef] [PubMed]
- Shiroff, A.M.; Herlitz, G.N.; Gracias, V.H. Necrotizing soft tissue infections. J. Intensive Care Med. 2014, 29, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Misiakos, E.P.; Bagias, G.; Patapis, P.; Sotiropoulos, D.; Kanavidis, P.; Machairas, A. Current Concepts in the Management of Necrotizing Fasciitis. Front. Surg. 2014, 1, 36. [Google Scholar] [CrossRef]
- Kimura, A.C.; Higa, J.I.; Levin, R.M.; Simpson, G.; Vargas, Y.; Vugia, D.J. Outbreak of necrotizing fasciitis due to Clostridium sordellii among black-tar heroin users. Clin. Infect. Dis. 2004, 38, 87–91. [Google Scholar] [CrossRef]
- Chen, J.-H.; Chang, P.-Y.; Ho, C.-L.; Chen, Y.-C.; Kao, W.-Y. Retroperitoneal Metastatic Adenocarcinoma Complicated with Necrotizing Fasciitis of the Thigh in a Patient with Advanced Rectal Colon Cancer. Case Rep. Oncol. 2010, 3, 304–309. [Google Scholar] [CrossRef]
- Haemers, K.; Peters, R.; Braak, S.; Wesseling, F. Necrotising fasciitis of the thigh. BMJ Case Rep. 2013, 2013, 10–13. [Google Scholar] [CrossRef]
- Sato, K.; Yamamura, H.; Sakamoto, Y.; Morohashi, H.; Miura, T.; Yoshikawa, T.; Hakamada, K. Necrotizing fasciitis of the thigh due to penetrated descending colon cancer: A case report. J. Surg. Case Rep. 2018, 4, 136. [Google Scholar] [CrossRef] [PubMed]
- Metastatic, U.; Colorectal, P.; Chan, C.C.; Williams, M. Fournier Gangrene as a Manifestation of Undiagnosed Metastatic Perforated Colorectal Cancer. Int. Surg. 2013, 98, 43–48. [Google Scholar] [CrossRef]
- Nowicki, J.; Rego, M.; Dean, N.R. A case report of a sub-clinical necrotising lower limb infection secondary to pelvic anastomotic leak and chronic corticosteroid use. JPRAS Open 2019, 21, 14–18. [Google Scholar] [CrossRef]
- Rupp, M.; Knapp, G.; Weisweiler, D.; Heiss, C.; Alt, V. Intestinal Perforation by a Toothpick as Reason for Necrotizing Fasciitis. J. Bone Jt. Infect. 2018, 3, 226–229. [Google Scholar] [CrossRef][Green Version]
- Yiasemidou, M.; Majumder, S.; Basheer, M. Necrotising fasciitis after laparoscopic rectal cancer surgery. Ann. R. Coll. Surg. Eng. 2017, 99, e123–e124. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wall, D.B.; de Virgilio, C.; Black, S.; Klein, S.R. Objective criteria may assist in distinguishing necrotizing fasciitis from non-necrotizing soft tissue infection. Am. J. Surg. 2000, 179, 17–21. [Google Scholar] [CrossRef]
- Wall, D.B.; Klein, S.R.; Black, S.; de Virgilio, C. A simple model to help distinguish necrotizing from non-necrotizing soft tissue infection. J. Am. Coll. Surg. 2000, 191, 227–231. [Google Scholar] [CrossRef]
- Wong, C.H.; Khin, L.W.; Heng, K.S.; Tan, K.C.; Low, C.O. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: A tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit. Care Med. 2004, 32, 1535–1541. [Google Scholar] [CrossRef]
- Wong, C.H.; Wang, Y.S. The diagnosis of necrotizing fasciitis. Curr. Opin. Infect. Dis. 2005, 18, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.; Hung, Y.S.; Shie, S.S.; Lin, T.L. Fulminant necrotizing fasciitis caused by Aeromonas sobria in neutropenic patients. Intern. Med. 2012, 51, 3287–3290. [Google Scholar] [CrossRef][Green Version]
- Tsai, Y.H.; Huang, K.C.; Huang, T.J.; Hsu, R.W. Case reports: Fatal necrotizing fasciitis caused by Aeromonas sobria in two diabetic patients. Clin. Orthop. Relat. Res. 2009, 467, 846–849. [Google Scholar] [CrossRef]
- Abder-Rahman, H.; Habash, I.; Alami, R.; Alnimer, T.; Al-Abdallat, I. Medico-legal importance of necrotizing fasciitis. J. Forensic Leg. Med. 2020, 74, 102019. [Google Scholar] [CrossRef]
- Kim, M.J.; Shin, S.H.; Park, J.Y. Medicolegal implications from litigations involving necrotizing fasciitis. Ann. Surg. Treat. Res. 2020, 99, 131–137. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sablone, S.; Lagouvardou, E.; Cazzato, G.; Carravetta, F.; Maselli, R.; Merlanti, F.; Bavaro, D.F.; De Donno, A.; Introna, F.; Caputi Iambrenghi, O. Necrotizing Fasciitis of the Thigh as Unusual Colonoscopic Polypectomy Complication: Review of the Literature with Case Presentation. Medicina 2022, 58, 131. https://doi.org/10.3390/medicina58010131
Sablone S, Lagouvardou E, Cazzato G, Carravetta F, Maselli R, Merlanti F, Bavaro DF, De Donno A, Introna F, Caputi Iambrenghi O. Necrotizing Fasciitis of the Thigh as Unusual Colonoscopic Polypectomy Complication: Review of the Literature with Case Presentation. Medicina. 2022; 58(1):131. https://doi.org/10.3390/medicina58010131
Chicago/Turabian StyleSablone, Sara, Elpiniki Lagouvardou, Gerardo Cazzato, Francesco Carravetta, Roberto Maselli, Francesco Merlanti, Davide Fiore Bavaro, Antonio De Donno, Francesco Introna, and Onofrio Caputi Iambrenghi. 2022. "Necrotizing Fasciitis of the Thigh as Unusual Colonoscopic Polypectomy Complication: Review of the Literature with Case Presentation" Medicina 58, no. 1: 131. https://doi.org/10.3390/medicina58010131
APA StyleSablone, S., Lagouvardou, E., Cazzato, G., Carravetta, F., Maselli, R., Merlanti, F., Bavaro, D. F., De Donno, A., Introna, F., & Caputi Iambrenghi, O. (2022). Necrotizing Fasciitis of the Thigh as Unusual Colonoscopic Polypectomy Complication: Review of the Literature with Case Presentation. Medicina, 58(1), 131. https://doi.org/10.3390/medicina58010131