
Immune Reconstitution Inflammatory Syndrome Induced by Mycobacterium avium Complex Infection Presenting as Chronic Inflammatory Demyelinating Polyneuropathy in a Young AIDS Patient


Abstract
1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Palella, F.J., Jr.; Delaney, K.M.; Moorman, A.C.; Loveless, M.O.; Fuhrer, J.; Satten, G.A.; Aschman, D.J.; Holmberg, S.D. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N. Engl. J. Med. 1998, 338, 853–860. [Google Scholar] [CrossRef]
- Cinti, S.K.; Kaul, D.R.; Sax, P.E.; Crane, L.R.; Kazanjian, P.H. Recurrence of Mycobacterium avium infection in patients receiving highly active antiretroviral therapy and antimycobacterial agents. Clin. Infect. Dis. 2000, 30, 511–514. [Google Scholar] [CrossRef][Green Version]
- Kishida, S.; Ajisawa, A. Probable cerebral Mycobacterium avium complex-related immune reconstitution inflammatory syndrome in an HIV-infected patient. Intern. Med. 2008, 47, 1349–1354. [Google Scholar] [CrossRef][Green Version]
- Lee, Y.C.; Lu, C.L.; Lai, C.C.; Tseng, Y.T.; Sun, H.Y.; Hung, C.C. Mycobacterium avium complex infection-related immune reconstitution inflammatory syndrome of the central nervous system in an HIV-infected patient: Case report and review. J. Microbiol. Immunol. Infect. 2013, 46, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Murray, R.; Mallal, S.; Heath, C.; French, M. Cerebral mycobacterium avium infection in an HIV-infected patient following immune reconstitution and cessation of therapy for disseminated mycobacterium avium complex infection. Eur. J. Clin. Microbiol. Infect. Dis. 2001, 20, 199–201. [Google Scholar] [CrossRef]
- Fortin, C.; Rouleau, D. Cerebral Mycobacterium avium abscesses: Late immune reconstitution syndrome in an HIV-1-infected patient receiving highly active antiretroviral therapy. Can. J. Infect. Dis. Med. Microbiol. 2005, 16, 187–189. [Google Scholar] [CrossRef][Green Version]
- Haddow, L.J.; Easterbrook, P.J.; Mosam, A.; Khanyile, N.G.; Parboosing, R.; Moodley, P.; Moosa, M.Y. Defining immune reconstitution inflammatory syndrome: Evaluation of expert opinion versus 2 case definitions in a South African cohort. Clin. Infect. Dis. 2009, 49, 1424–1432. [Google Scholar] [CrossRef] [PubMed]
- Robertson, J.; Meier, M.; Wall, J.; Ying, J.; Fichtenbaum, C.J. Immune reconstitution syndrome in HIV: Validating a case definition and identifying clinical predictors in persons initiating antiretroviral therapy. Clin. Infect. Dis. 2006, 42, 1639–1646. [Google Scholar] [CrossRef]
- Meintjes, G.; Lawn, S.D.; Scano, F.; Maartens, G.; French, M.A.; Worodria, W.; Elliott, J.H.; Murdoch, D.; Wilkinson, R.J.; Seyler, C.; et al. Tuberculosis-associated immune reconstitution inflammatory syndrome: Case definitions for use in resource-limited settings. Lancet Infect. Dis. 2008, 8, 516–523. [Google Scholar] [CrossRef]
- Piliero, P.J.; Fish, D.G.; Preston, S.; Cunningham, D.; Kinchelow, T.; Salgo, M.; Qian, J.; Drusan, G.L. Guillain-Barré syndrome associated with immune reconstitution. Clin. Infect. Dis. 2003, 36, e111–e114. [Google Scholar] [CrossRef] [PubMed]
- Fantauzzi, A.; Digiulio, M.A.; Cavallari, E.N.; d’Ettorre, G.; Vullo, V.; Mezzaroma, I. Guillain Barre syndrome in an HIV-1-infected patient after the beginning of combined antiretroviral therapy: An immune reconstitution inflammatory syndrome? New Microbiol. 2014, 37, 103–107. [Google Scholar]
- Makela, P.; Howe, L.; Glover, S.; Ferguson, I.; Pinto, A.; Gompels, M. Recurrent Guillain-Barre syndrome as a complication of immune reconstitution in HIV. J. Infect. 2002, 44, 47–49. [Google Scholar] [CrossRef]
- Arcila-Londono, X.; Lewis, R.A. Multifocal motor neuropathy. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2013; Volume 115, pp. 429–442. [Google Scholar]
- Cats, E.A.; Jacobs, B.C.; Yuki, N.; Tio-Gillen, A.P.; Piepers, S.; Franssen, H.; van Asseldonk, J.-T.; van den Berg, L.H.; van der Pol, V.-L. Multifocal motor neuropathy: Association of anti-GM1 IgM antibodies with clinical features. Neurology 2010, 75, 1961–1967. [Google Scholar] [CrossRef]
- Nobile-Orazio, E.; Cappellari, A.; Priori, A. Multifocal motor neuropathy: Current concepts and controversies. Muscle Nerve 2005, 31, 663–680. [Google Scholar] [CrossRef]
- European Federation of Neurological Societies; Peripheral Nerve Society. Guideline on management of multifocal motor neuropathy. Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society—First revision. J. Peripher. Nerv. Syst. 2010, 15, 295–301. [Google Scholar]
- Niermeijer, J.M.; Fischer, K.; Eurelings, M.; Franssen, H.; Wokke, J.H.J.; Notermans, N.C. Prognosis of polyneuropathy due to IgM monoclonal gammopathy: A prospective cohort study. Neurology 2010, 74, 406–412. [Google Scholar] [CrossRef]
- Nobile-Orazio, E.; Manfredini, E.; Carpo, M.; Meucci, N.; Monaco, S.; Ferrari, S.; Bonetti, B.; Cavaletti, G.; Gemignani, F.; Durelli, L.; et al. Frequency and clinical correlates of anti-neural IgM antibodies in neuropathy associated with IgM monoclonal gammopathy. Ann. Neurol. 1994, 36, 416–424. [Google Scholar] [CrossRef]
- Van den Bergh, P.Y.; Hadden, R.D.M.; Bouche, P.; Cornblath, D.R.; Hahn, A.; Illa, I.; Koski, C.L.; Léger, J.-M.; Nobile-Orazio, E.; Pollard, J.; et al. European Federation of Neurological Societies/Peripheral Nerve Society guideline on management of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society—First revision. Eur. J. Neurol. 2010, 17, 356–363. [Google Scholar]
- Willison, H.; O’Leary, C.P.; Veitch, J.; Blumhardt, L.D.; Busby, M.; Donaghy, M.; Fuhr, P.; Ford, H.; Hahn, A.; Renaud, S.; et al. The clinical and laboratory features of chronic sensory ataxic neuropathy with anti-disialosyl IgM antibodies. Brain 2001, 124, 1968–1977. [Google Scholar] [CrossRef]
- Kam, C.; Balaratnam, M.S.; Purves, A.; Mills, K.R.; Riordan-Eva, P.; Pollock, S.; Bodi, I.; Munro, N.A.R.; Bennett, D.L.H. Canomad presenting without ophthalmoplegia and responding to intravenous immunoglobulin. Muscle Nerve 2011, 44, 829–833. [Google Scholar] [CrossRef]
- Phillips, P.; Bonner, S.; Gataric, N.; Bai, T.; Wilcox, P.; Hogg, R.; O’Shaughnessy, M.; Montaner, J. Nontuberculous mycobacterial immune reconstitution syndrome in HIV-infected patients: Spectrum of disease and long-term follow-up. Clin. Infect. Dis. 2005, 41, 1483–1497. [Google Scholar] [CrossRef]
- Breglio, K.F.; Vinhaes, C.L.; Arriaga, M.B.; Nason, M.; Roby, G.; Adelsberge, J.; Andrade, B.B.; Sheikh, V.; Sereti, I. Clinical and Immunologic Predictors of Mycobacterium avium Complex Immune Reconstitution Inflammatory Syndrome in a Contemporary Cohort of Patients with Human Immunodeficiency Virus. J. Infect. Dis. 2021, 223, 2124–2135. [Google Scholar] [CrossRef]
- Mathey, E.K.; Park, S.B.; Hughes, R.A.C.; Pollard, J.D.; Armati, P.J.; Barnett, M.H.; Taylor, B.V.; Dyck, P.J.B.; Kiernan, M.C.; Lin, C.S.-Y. Chronic inflammatory demyelinating polyradiculoneuropathy: From pathology to phenotype. J. Neurol. Neurosurg. Psychiatry 2015, 86, 973–985. [Google Scholar] [CrossRef]
- Rentzos, M.; Angeli, A.V.; Rombos, A.; Kyrozis, A.; Nikolaou, C.; Zouvelou, V.; Dimitriou, A.; Zoga, M.; Evangelopoulos, M.-E.; Tsatsi, A.; et al. Proinflammatory cytokines in serum and cerebrospinal fluid of CIDP patients. Neurol. Res. 2012, 34, 842–846. [Google Scholar] [CrossRef] [PubMed]
- Kiefer, R.; Kieseier, B.C.; Stoll, G.; Hartung, H.P. The role of macrophages in immune-mediated damage to the peripheral nervous system. Prog. Neurobiol. 2001, 64, 109–127. [Google Scholar] [CrossRef]
- Schneider-Hohendorf, T.; Schneider-Hohendorf, T.; Schwab, N.; Üçeyler, N.; Göbel, K.; Sommer, C.; Wiendl, H. CD8+ T-cell immunity in chronic inflammatory demyelinating polyradiculoneuropathy. Neurology 2012, 78, 402–408. [Google Scholar] [CrossRef]
- Sanvito, L.; Makowska, A.; Mahdi-Rogers, M.; Hadden, R.D.; Peakman, M.; Gregson, N.; Nemni, R.; Hughes, R.A.C. Humoral and cellular immune responses to myelin protein peptides in chronic inflammatory demyelinating polyradiculoneuropathy. J. Neurol. Neurosurg. Psychiatry 2009, 80, 333–338. [Google Scholar] [CrossRef]
- Querol, L.; Devaux, J.; Rojas-Garcia, R.; Illa, I. Autoantibodies in chronic inflammatory neuropathies: Diagnostic and therapeutic implications. Nat. Rev. Neurol. 2017, 13, 533–547. [Google Scholar] [CrossRef]
- Delmont, E.; Manso, C.; Querol, L.; Cortese, A.; Berardinelli, A.; Lozza, A.; Belghazi, M.; Malissart, P.; Labauge, P.; Taieb, G.; et al. Autoantibodies to nodal isoforms of neurofascin in chronic inflammatory demyelinating polyneuropathy. Brain 2017, 140, 1851–1858. [Google Scholar] [CrossRef] [PubMed]
- Stathopoulos, P.; Alexopoulos, H.; Dalakas, M.C. Autoimmune antigenic targets at the node of Ranvier in demyelinating disorders. Nat. Rev. Neurol. 2015, 11, 143–156. [Google Scholar] [CrossRef]
- Vural, A.; Doppler, K.; Meinl, E. Autoantibodies Against the Node of Ranvier in Seropositive Chronic Inflammatory Demyelinating Polyneuropathy: Diagnostic, Pathogenic, and Therapeutic Relevance. Front. Immunol. 2018, 9, 1029. [Google Scholar] [CrossRef]
- Sheu, T.T.; Chiang, B.L. Lymphopenia, Lymphopenia-Induced Proliferation, and Autoimmunity. Int. J. Mol. Sci. 2021, 22, 4152. [Google Scholar] [CrossRef]
- Walker, L.S.; Sansom, D.M. The emerging role of CTLA4 as a cell-extrinsic regulator of T cell responses. Nat. Rev. Immunol. 2011, 11, 852–863. [Google Scholar] [CrossRef]
- Scalapino, K.J.; Daikh, D.I. CTLA-4: A key regulatory point in the control of autoimmune disease. Immunol. Rev. 2008, 223, 143–155. [Google Scholar] [CrossRef]
- Stone, S.F.; Price, P.; French, M.A. Dysregulation of CD28 and CTLA-4 expression by CD4 T cells from previously immunodeficient HIV-infected patients with sustained virological responses to highly active antiretroviral therapy. HIV Med. 2005, 6, 278–283. [Google Scholar] [CrossRef]
- Saverino, D.; Brizzolara, R.; Simone, R.; Chiappori, A.; Milintenda-Floriani, F.; Pesce, G.; Bagnasco, M. Soluble CTLA-4 in autoimmune thyroid diseases: Relationship with clinical status and possible role in the immune response dysregulation. Clin. Immunol. 2007, 123, 190–198. [Google Scholar] [CrossRef]
- Oaks, M.K.; Hallett, K.M. Cutting edge: A soluble form of CTLA-4 in patients with autoimmune thyroid disease. J. Immunol. 2000, 164, 5015–5018. [Google Scholar] [CrossRef]
- Belkaid, Y.; Tarbell, K. Regulatory T cells in the control of host-microorganism interactions. Annu. Rev. Immunol. 2009, 27, 551–589. [Google Scholar] [CrossRef]
- Seddiki, N.; Sasson, S.C.; Santner-Nanan, B.; Munier, M.; van Bockel, D.; Ip, S.; Marriott, D.; Pett, S.; Nanan, R.; Cooper, D.A.; et al. Proliferation of weakly suppressive regulatory CD4+ T cells is associated with over-active CD4+ T-cell responses in HIV-positive patients with mycobacterial immune restoration disease. Eur. J. Immunol. 2009, 39, 391–403. [Google Scholar] [CrossRef]
- Chi, L.J.; Wang, H.B.; Wang, W.Z. Impairment of circulating CD4+CD25+ regulatory T cells in patients with chronic inflammatory demyelinating polyradiculoneuropathy. J. Peripher. Nerv. Syst. 2008, 13, 54–63. [Google Scholar] [CrossRef]
- Sanvito, L.; Makowska, A.; Gregson, N.; Nemni, R.; Hughes, R.A. Circulating subsets and CD4(+)CD25(+) regulatory T cell function in chronic inflammatory demyelinating polyradiculoneuropathy. Autoimmunity 2009, 42, 667–677. [Google Scholar] [CrossRef]
- Kale, H.A.; Sklar, E. Magnetic resonance imaging findings in chronic inflammatory demyelinating polyneuropathy with intracranial findings and enhancing, thickened cranial and spinal nerves. Australas. Radiol. 2007, 51, B21–B24. [Google Scholar] [CrossRef] [PubMed]
- Ormerod, I.E.; Waddy, H.M.; Kermode, A.G.; Murray, N.M.; Thomas, P.K. Involvement of the central nervous system in chronic inflammatory demyelinating polyneuropathy: A clinical, electrophysiological and magnetic resonance imaging study. J. Neurol. Neurosurg. Psychiatry 1990, 53, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Mendell, J.R.; Kolkin, S.; Kissel, J.T.; Weiss, K.L.; Chakeres, D.W.; Rammohan, K.W. Evidence for central nervous system demyelination in chronic inflammatory demyelinating polyradiculoneuropathy. Neurology 1987, 37, 1291–1294. [Google Scholar] [CrossRef]
- Pineda, A.A.; Ogata, K.; Osoegawa, M.; Murai, H.; Shigeto, H.; Yoshiura, T.; Tobimatsu, S.; Kira, J.-I. A distinct subgroup of chronic inflammatory demyelinating polyneuropathy with CNS demyelination and a favorable response to immunotherapy. J. Neurol. Sci. 2007, 255, 1–6. [Google Scholar] [CrossRef]
- Lortholary, O.; Fontanet, A.; Mémain, N.; Martin, A.; Sitbon, K.; Dromer, F.; French Cryptococcosis Study Group. Incidence and risk factors of immune reconstitution inflammatory syndrome complicating HIV-associated cryptococcosis in France. Aids 2005, 19, 1043–1049. [Google Scholar] [CrossRef]
- Grant, P.M.; Komarow, L.; Andersen, J.; Sereti, I.; Pahwa, S.; Lederman, M.M.; Eron, J.; Sanne, I.; Powderly, W.; Hogg, E.; et al. Risk factor analyses for immune reconstitution inflammatory syndrome in a randomized study of early vs. deferred ART during an opportunistic infection. PLoS ONE 2010, 5, e11416. [Google Scholar]
- Yang, M.; Rainone, A.; Shi, X.Q.; Fournier, S.; Zhang, J. A new animal model of spontaneous autoimmune peripheral polyneuropathy: Implications for Guillain-Barré syndrome. Acta Neuropathol. Commun. 2014, 2, 5. [Google Scholar] [CrossRef]
- Matsumuro, K.; Izumo, S.; Umehara, F.; Osame, M. Chronic inflammatory demyelinating polyneuropathy: Histological and immunopathological studies on biopsied sural nerves. J. Neurol. Sci. 1994, 127, 170–178. [Google Scholar] [CrossRef]
- Mausberg, A.K.; Dorok, M.; Stettner, M.; Müller, M.; Hartung, H.P.; Dehmel, T.; Warnke, C.; zu Hörste, G.M.; Kieseier, B.C. Recovery of the T-cell repertoire in CIDP by IV immunoglobulins. Neurology 2013, 80, 296–303. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reference | Age/Sex | CD4 T-Cell Count at Baseline (Cells/μL) | CD4 T-Cell Count at IRIS Diagnosis (Cells/μL) | Plasma HIV RNA Load. at Baseline (Copies/mL) | Plasma HIV RNA Load. at IRIS Diagnosis (Copies/mL) | Time to IRIS Diagnosis from ART Initiation (Month) | MAC Related IRIS Presentation | Image Findings | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| 4 | 24/M | 2 | 70 | 77,600 | <50 | 17 months | MAC meningoencephalitis and myelitis with drowsy, stumbling, and progressive paraplegia (Paradoxical IRIS) | Multiple enhancing nodules in the cerebral and cerebellar hemispheres, gray matter, brain stem and whole spinal cord. | Levofloxacin + clarithromycin ethambutol + rifabutin + dexamathasone | Significantly improved paraplegia and consciousness after 5 days of anti-MAC therapy |
| 5 | 35/M | <10 | 210 | 382,987 | <400 | 25 months | Cerebral MAC infection with headache, fever, dizziness, vomiting (Paradoxical IRIS) | A solitary 3 cm lesion in the left frontal lobe of brain with perifocal edema and mass effect |
| MAC-IRIS resolved 18 days after anti-MAC therapy |
| 6 | 36/M | 10 | 170 | 217,163 | <50 | 29 months | Cerebral MAC abscesses with headache and aphasia (Paradoxical IRIS) | Two hypodense lesions with ring enhancement and edema in the right temporal lobe and left temporoparietal area | Azithromycin+ ethambutol + rifabutin | Complete regression of lesions 10 months after anti-MAC therapy |
| 3 | 51/M | 20 | 10 | 17,000 | <50 | 3 months | Cerebral MAC infection with fever, disturbance of consciousness (Paradoxical IRIS) | Ring enhanced lesions with perifocal edema in the left temporal lobe | Ethambutol + isoniazid + levofloxacin + amikacin + dexamathasone | Died soon after onset of neurological symptoms |
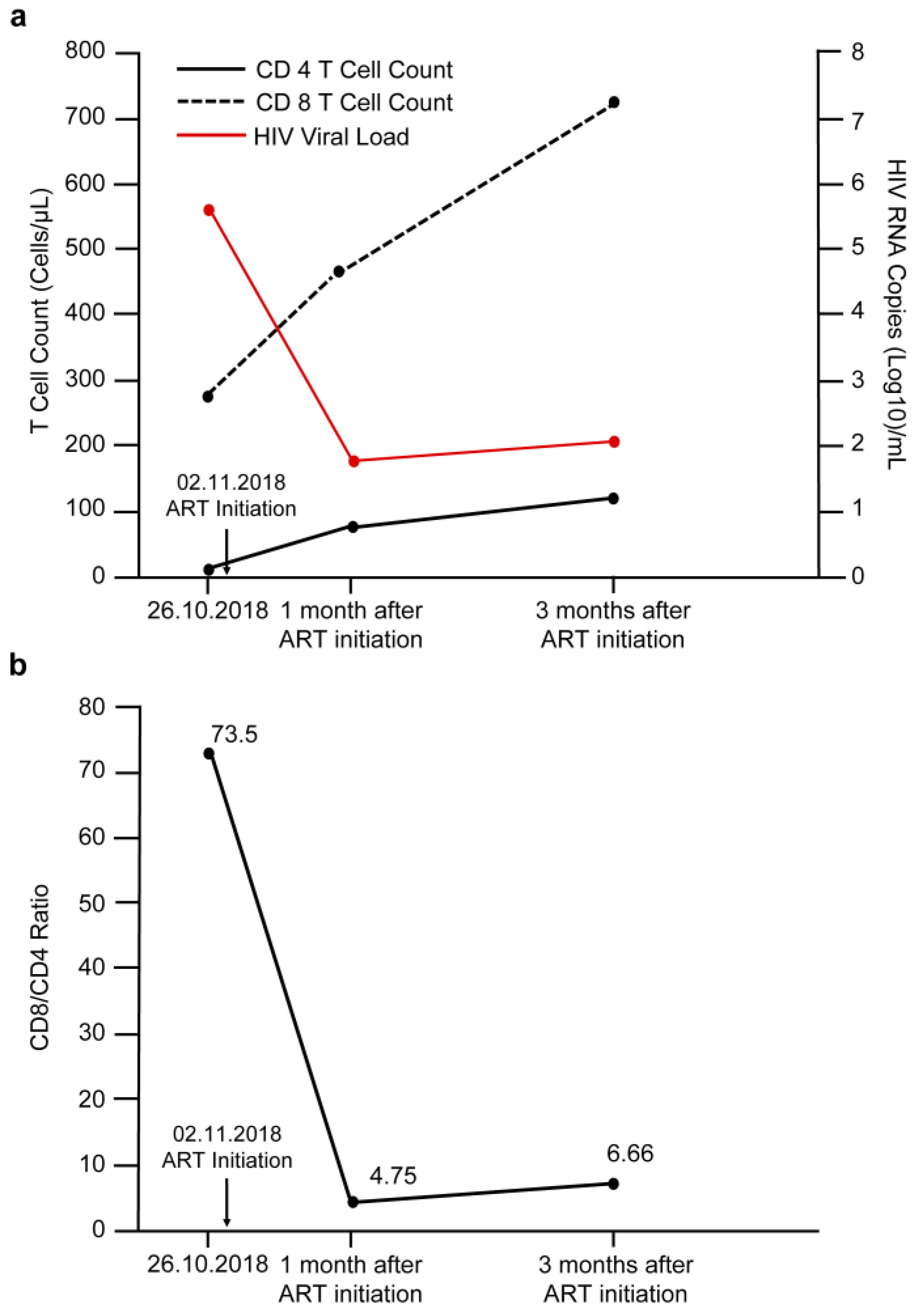
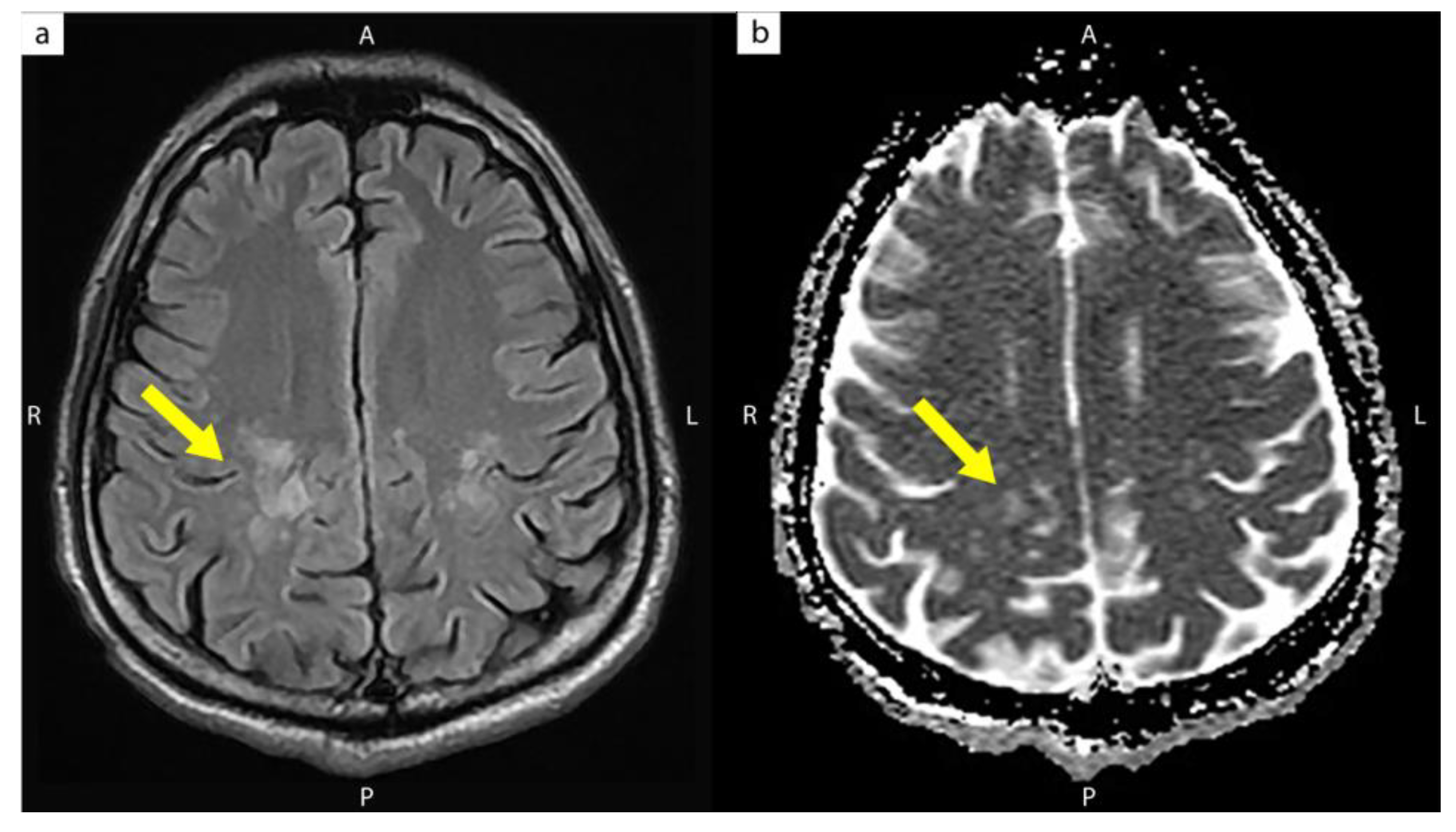
| The present case | 31/M | 4 | 109 | 586,300 | 113 | 3 months | CIDP with progressive quadriparesis (Unmasking IRIS) | High signal intensities over both the posterior corona radiata and centrum semiovale |
| Significantly improved quadriparesis 3 months after anti-MAC and Plasma exchange + IVIG |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, A.-C.; Lin, T.-Y.; Wang, N.-C. Immune Reconstitution Inflammatory Syndrome Induced by Mycobacterium avium Complex Infection Presenting as Chronic Inflammatory Demyelinating Polyneuropathy in a Young AIDS Patient. Medicina 2022, 58, 110. https://doi.org/10.3390/medicina58010110
Cheng A-C, Lin T-Y, Wang N-C. Immune Reconstitution Inflammatory Syndrome Induced by Mycobacterium avium Complex Infection Presenting as Chronic Inflammatory Demyelinating Polyneuropathy in a Young AIDS Patient. Medicina. 2022; 58(1):110. https://doi.org/10.3390/medicina58010110
Chicago/Turabian StyleCheng, An-Che, Te-Yu Lin, and Ning-Chi Wang. 2022. "Immune Reconstitution Inflammatory Syndrome Induced by Mycobacterium avium Complex Infection Presenting as Chronic Inflammatory Demyelinating Polyneuropathy in a Young AIDS Patient" Medicina 58, no. 1: 110. https://doi.org/10.3390/medicina58010110
APA StyleCheng, A.-C., Lin, T.-Y., & Wang, N.-C. (2022). Immune Reconstitution Inflammatory Syndrome Induced by Mycobacterium avium Complex Infection Presenting as Chronic Inflammatory Demyelinating Polyneuropathy in a Young AIDS Patient. Medicina, 58(1), 110. https://doi.org/10.3390/medicina58010110