
Implant Placement after Closure of Oroantral Communication by Sinus Bone Graft Using a Collagen Barrier Membrane in the Shape of a Pouch: A Case Report and Review of the Literature



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
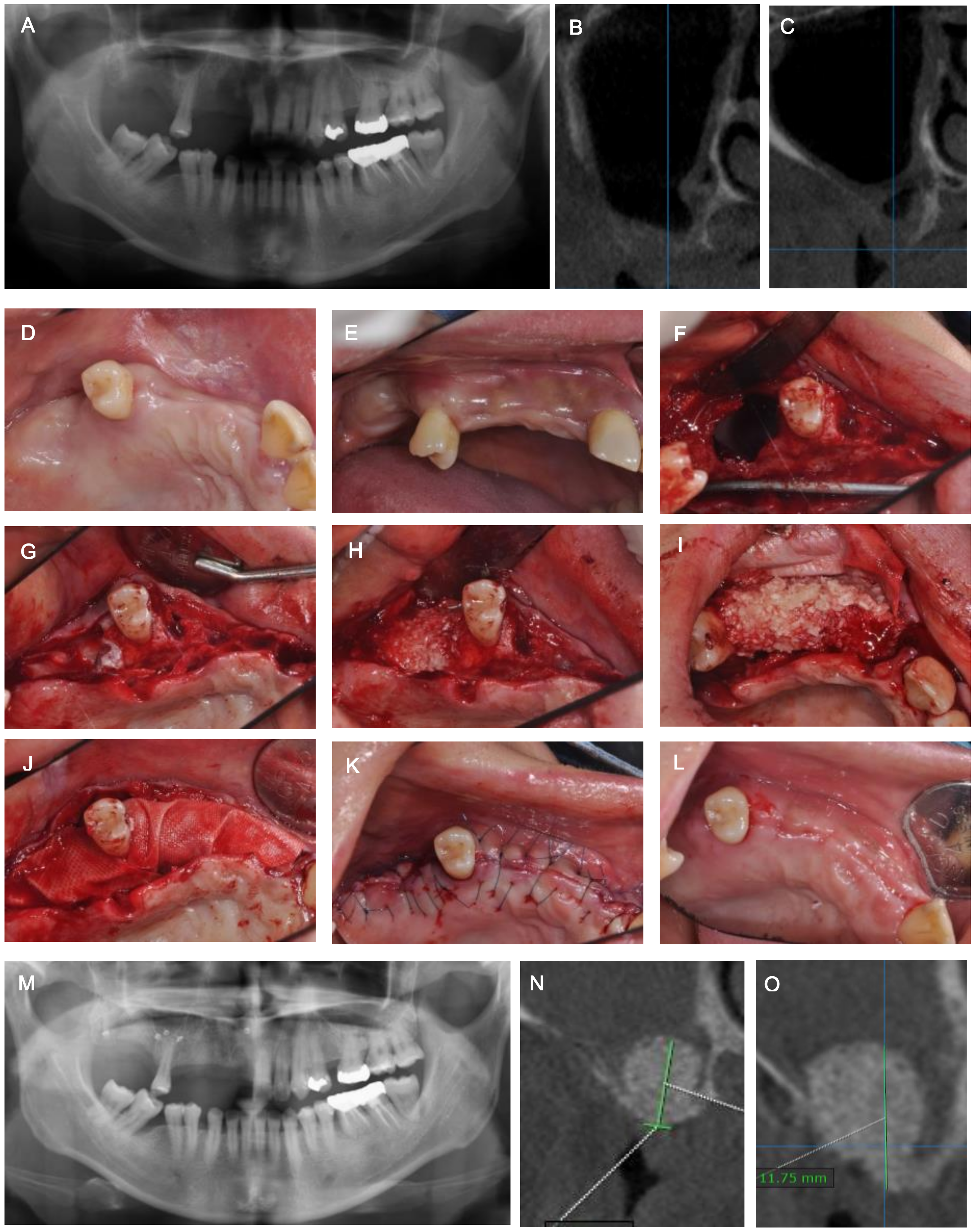
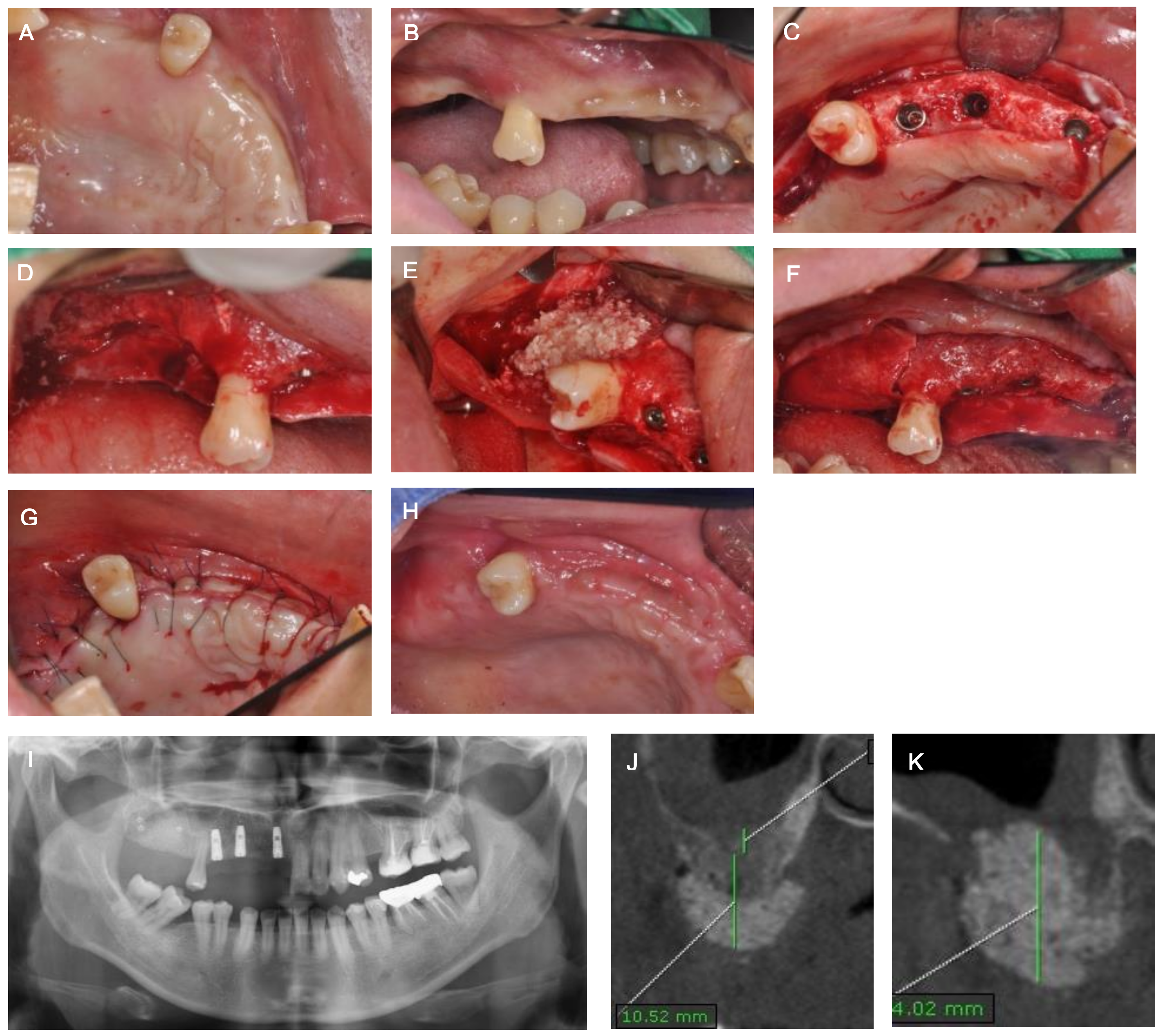
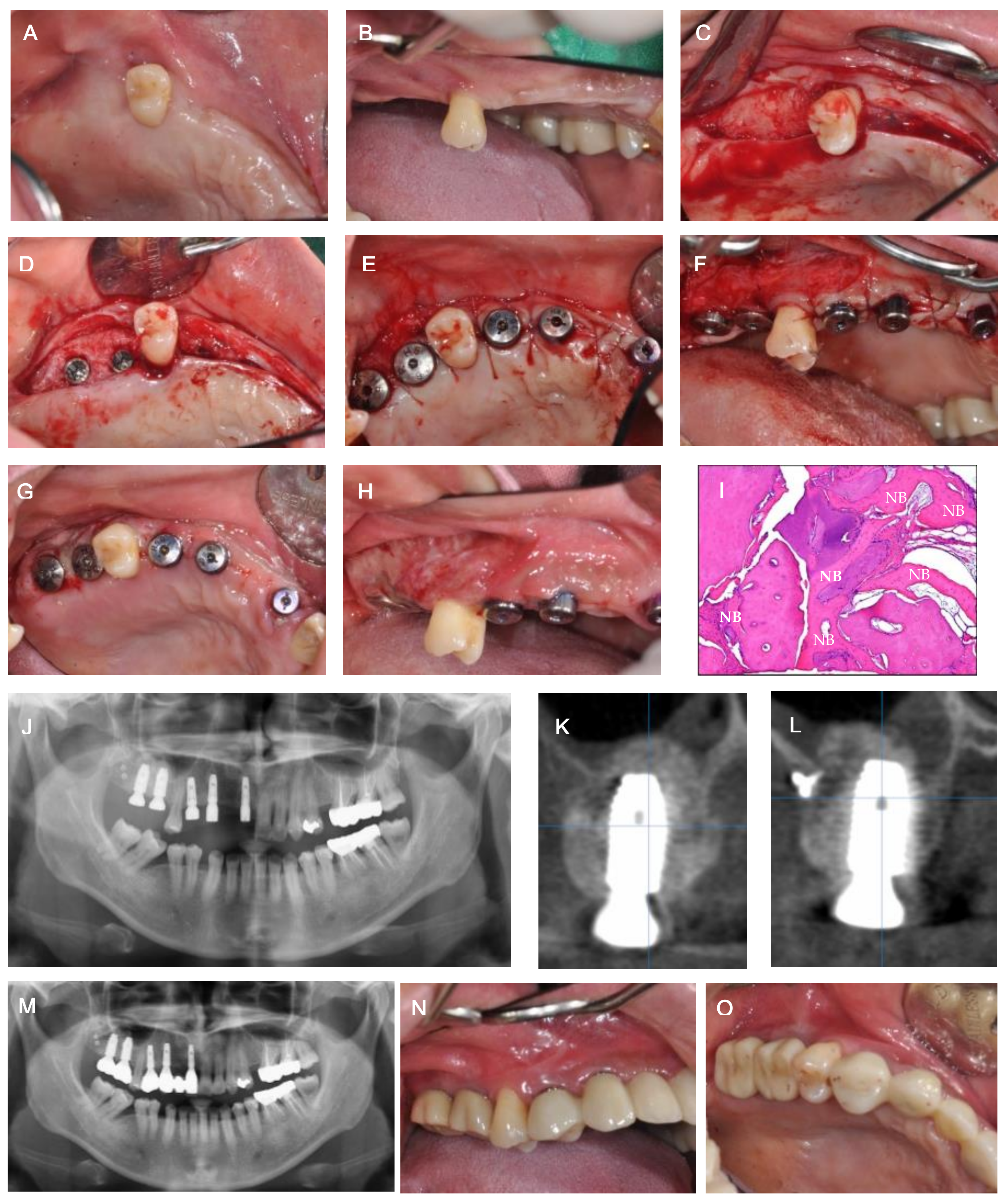
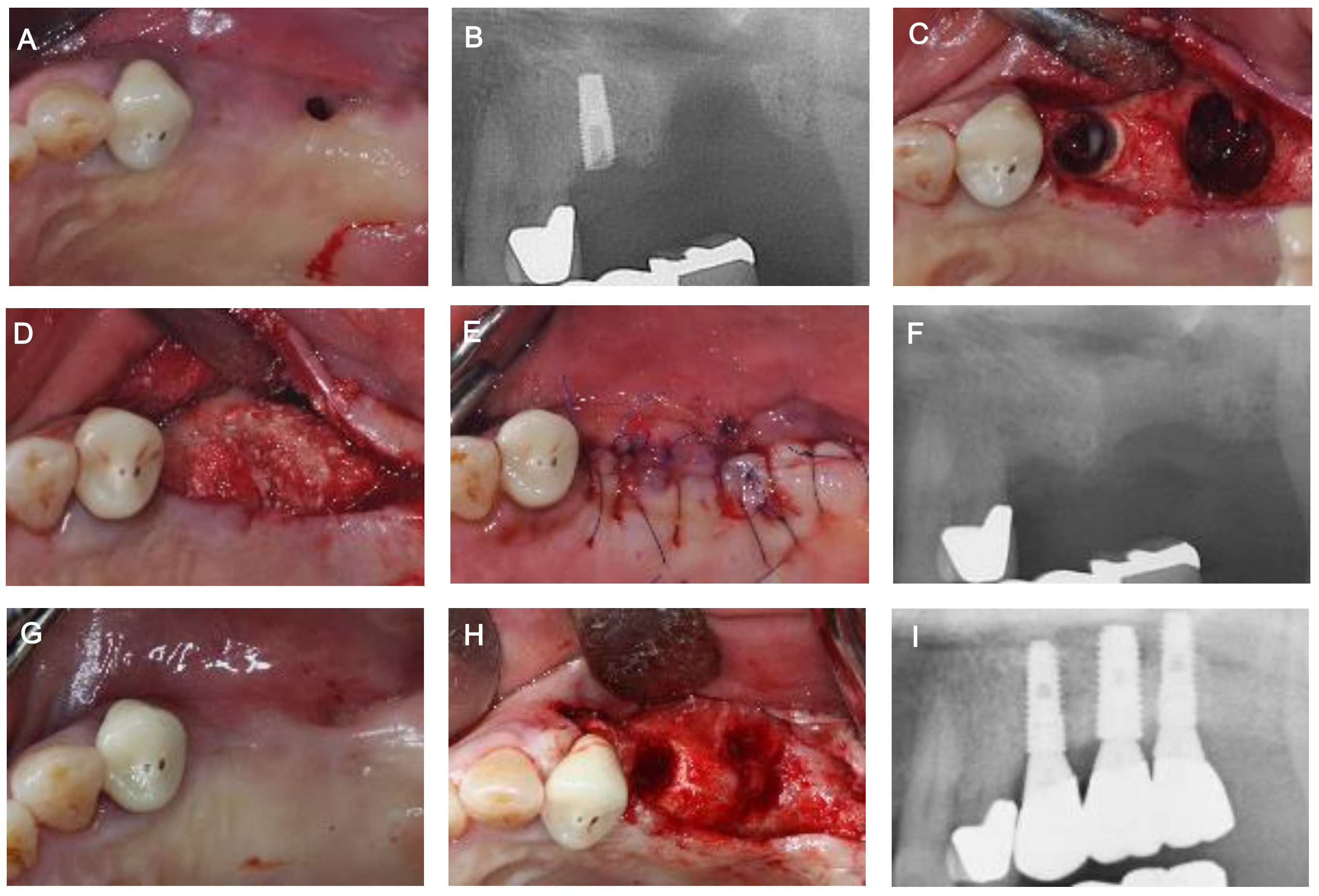
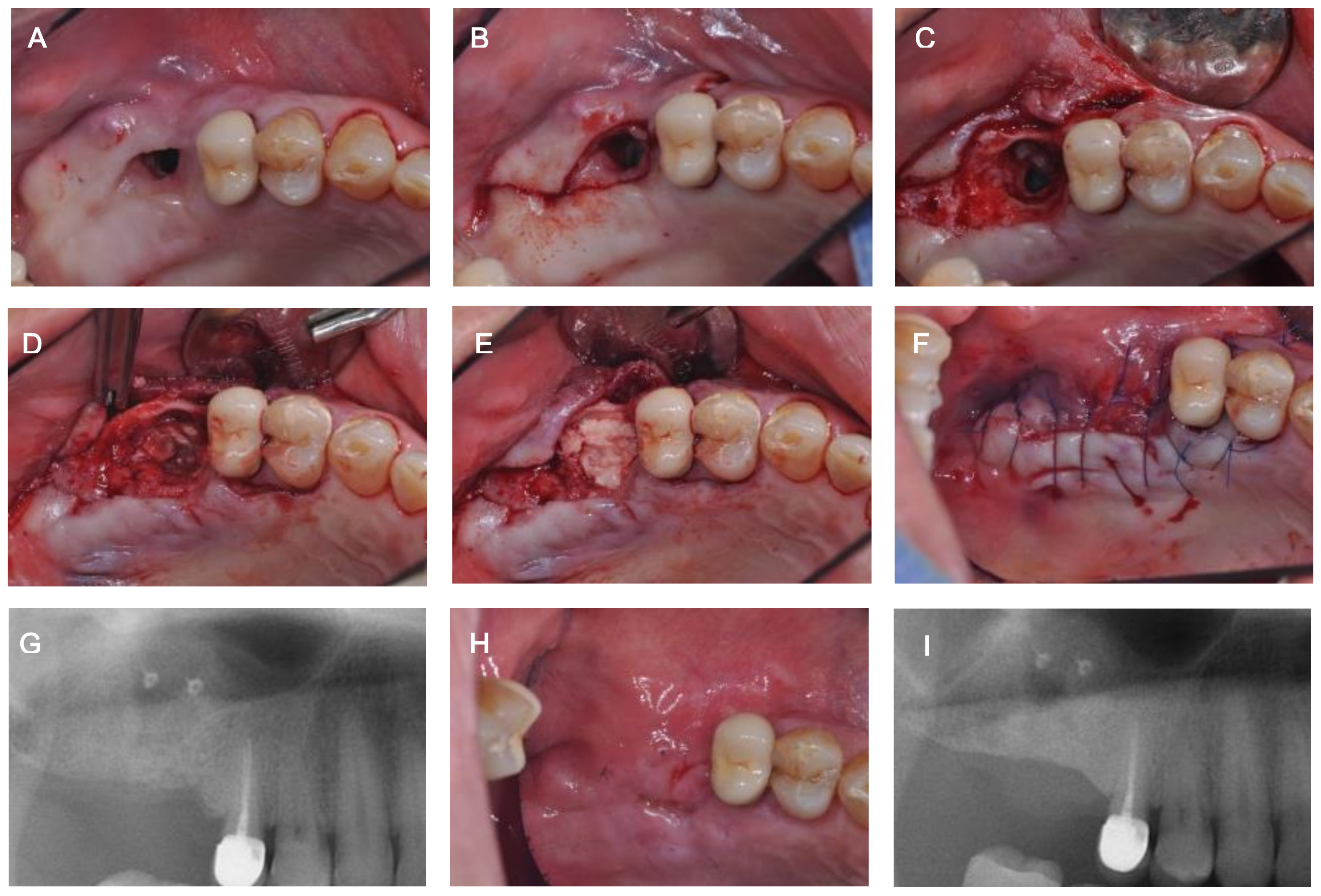
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Logan, R.M.; Coates, E.A. Non-surgical management of an oro-antral fistula in a patient with HIV infection. Aust. Dent. J. 2003, 48, 255–258. [Google Scholar] [PubMed]
- Yalcın, S.; Öncü, B.; Emes, Y.; Atalay, B.; Aktas, I. Surgical treatment of oroantral fistulas: A clinical study of 23 Cases. J. Oral Maxillofac. Surg. 2011, 69, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Parvini, P.; Obreja, K.; Sader, R.; Becker, J.; Schwarz, F.; Salti, L. Decision-making in closure of oroantral communication and fistula. Int. J. Implant Dent. 2019, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Parvini, P.; Obreja, K.; Sader, R.; Becker, J.; Schwarz, F.; Salti, L. Surgical options in oroantral fistula management: A narrative review. Int. J. Implant Dent. 2018, 4, 40. [Google Scholar] [CrossRef] [PubMed]
- Liversedge, R.L.; Wong, K. Use of the buccal fat pad in maxillary and sinus grafting of the severely atrophic maxilla preparatory to implant reconstruction of the partially or completely edentulous patient: Technical note. Int. J. Oral Maxillofac. Implant. 2002, 17, 424–428. [Google Scholar]
- Kraut, R.A.; Smith, R.V. Team approach for closure of oroantral and oronasal fistulae. Atlas Oral Maxillofac. Surg. Clin. N. Am. 2000, 8, 55–75. [Google Scholar] [CrossRef]
- Visscher, S.H.; Minnen, B.; Bos, R. Closure of oroantral communications: A review of the literature. J. Oral Maxillofac. Surg. 2010, 68, 1384–1391. [Google Scholar] [CrossRef] [PubMed]
- Nezafati, S.; Vafaii, A.; Ghojazadeh, M. Comparison of pedicled buccal fat pad flap with buccal flap for closure of oro-antral communication. Int. J. Oral Maxillofac. Surg. 2012, 41, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Borgonovo, A.E.; Berardinelli, F.V.; Favale, M.; Maiorana, C. Surgical Options in Oro-antral Fistula Treatment. Open Dent. J. 2012, 6, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Doobrow, J.H.; Leite, R.S.; Hirsch, H.Z. Concomitant oroantral communication repair and immediate implant placement: A five-year case report. Implant Dent. 2008, 17, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.P.; Kwon, Y.S. Vestibuloplasty around dental implants using modified periosteal fenestration (mPF): Case series. Implantology 2020, 24, 22–30. [Google Scholar] [CrossRef]
- Park, D.Y.; Lee, W.P. Vestibuloplasty around teeth and dental implants using simplified periosteal fenestration (sPF): Case Reports. J. Kor. Dent. Assoc. 2020, 59, 20–27. [Google Scholar] [CrossRef]
- Proctor, B. Bone graft closure of large or persistent oro-maxillary fistula. Laryngoscope 1969, 79, 822. [Google Scholar] [CrossRef] [PubMed]
- Isler, S.C.; Demircan, S.; Cansiz, E. Closure of oroantral fistula using auricular cartilage: A new method to repair an oroantral fistula. Br. J. Oral Maxillofac. Surg. 2011, 49, e86–e87. [Google Scholar] [CrossRef] [PubMed]
- Scattarella, A.; Ballini, A.; Grassi, F.R.; Carbonara, A.; Ciccolella, F.; Dituri, A.; Nardi, G.M.; Cantore, S.; Pettini, F. Treatment of oroantral fistula with autologous bone graft and application of a non-reabsorbable membrane. Int. J. Med. Sci. 2010, 7, 267–271. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ogunsalu, C. A new surgical management for oro-antral communication: The resorbable guided tissue regeneration membrane-bone substitute sandwich technique. West Indian Med. J. 2005, 54, 261–263. [Google Scholar] [CrossRef] [PubMed]
- Proussaefs, P.; Lozada, J. The “Loma Linda Pouch”: A Technique for Repairing the Perforated Sinus Membrane. Int. J. Periodontics Restor. Dent. 2003, 23, 593–597. [Google Scholar]
- Testori, T.; Wallace, S.S.; Del Fabbro, M.; Taschieri, S.; Trisi, P.; Capelli, M.; Weinstein, R.L. Repair of large sinus membrane perforations using stabilized collagen barrier membranes: Surgical techniques with histologic and radiographic evidence of success. Int. J. Periodontics Restor. Dent. 2008, 28, 9–17. [Google Scholar]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, J.-H.; Kim, B.-O.; Lee, W.-P. Implant Placement after Closure of Oroantral Communication by Sinus Bone Graft Using a Collagen Barrier Membrane in the Shape of a Pouch: A Case Report and Review of the Literature. Medicina 2021, 57, 626. https://doi.org/10.3390/medicina57060626
Baek J-H, Kim B-O, Lee W-P. Implant Placement after Closure of Oroantral Communication by Sinus Bone Graft Using a Collagen Barrier Membrane in the Shape of a Pouch: A Case Report and Review of the Literature. Medicina. 2021; 57(6):626. https://doi.org/10.3390/medicina57060626
Chicago/Turabian StyleBaek, Jae-Ha, Byung-Ock Kim, and Won-Pyo Lee. 2021. "Implant Placement after Closure of Oroantral Communication by Sinus Bone Graft Using a Collagen Barrier Membrane in the Shape of a Pouch: A Case Report and Review of the Literature" Medicina 57, no. 6: 626. https://doi.org/10.3390/medicina57060626
APA StyleBaek, J.-H., Kim, B.-O., & Lee, W.-P. (2021). Implant Placement after Closure of Oroantral Communication by Sinus Bone Graft Using a Collagen Barrier Membrane in the Shape of a Pouch: A Case Report and Review of the Literature. Medicina, 57(6), 626. https://doi.org/10.3390/medicina57060626