
Pulmonary Sclerosing Pneumocytoma: A Pre and Intraoperative Diagnostic Challenge. Report of Two Cases and Review of the Literature

 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
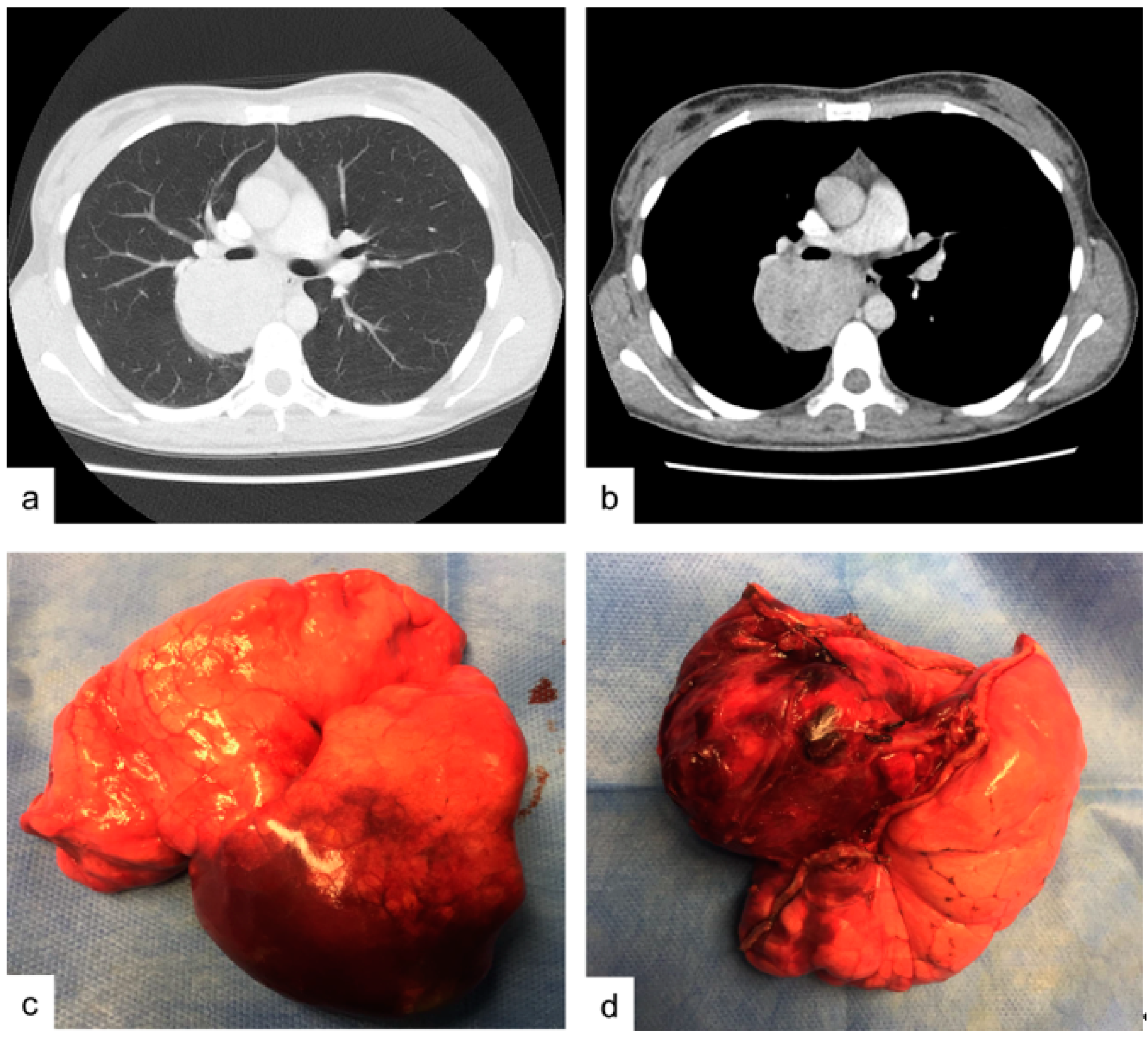
2.1. Macroscopic Findings.
2.2. Microscopic Findings
3. Case Report 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Liebow, A.A.; Hubbell, D.S. Sclerosing hemangioma (histiocytoma, xanthoma) of the lung. Cancer 1956, 9, 53–75. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef]
- Devouassoux-Shisheboran, M.; Hayashi, T.; Linnoila, R.I.; Koss, M.N.; Travis, W.D. A clinicopathologic study of 100 cases of pulmonary sclerosing hemangioma with immunohistochemical studies: TTF-1 is expressed in both round and surface cells, suggesting an origin from primitive respiratory epithelium. Am. J. Surg. Pathol. 2000, 24, 906–916. [Google Scholar] [CrossRef]
- Shin, S.Y.; Kim, M.Y.; Oh, S.Y.; Lee, H.J.; Hong, S.A.; Jang, S.J.; Kim, S.S. Pulmonary sclerosing pneumocytoma of the lung: CT characteristics in a large series of a tertiary referral center. Medicine 2015, 94, e498. [Google Scholar] [CrossRef]
- Khanna, A.; Alshabani, K.; Mukhopadhyay, S.; Lam, L.; Ghosh, S. Sclerosing pneumocytoma: Case report of a rare endobronchial presentation. Medicine 2019, 98, e15038. [Google Scholar] [CrossRef]
- Sakai, T.; Miyoshi, T.; Umemura, S.; Suzuki, J.; Nakasone, S.; Okada, S.; Tane, K.; Aokage, K.; Goto, K.; Motoi, N.; et al. Large pulmonary sclerosing pneumocytoma with massive necrosis and vascular invasion: A case report. Oxf. Med Case Rep. 2019, 2019, omz066. [Google Scholar] [CrossRef]
- Keylock, M.C.P.T.J.B.; Galvin, J.R.; Franks, T.J. Sclerosing Hemangioma of the Lung. Arch. Pathol. Lab. Med. 2009, 133, 820–825. [Google Scholar] [CrossRef]
- Yuan, Z.-Q.; Wang, Q.; Bao, M. Symptomatic pulmonary sclerosing hemangioma: A rare case of a solitary pulmonary nodule in a woman of advanced age. J. Int. Med Res. 2019, 47, 2302–2308. [Google Scholar] [CrossRef]
- Yalcin, B.; Bekci, T.T.; Kozacioglu, S.; Bolukbas, O. Pulmonary sclerosing pneumocytoma, a rare tumor of the lung. Respir. Med. Case Rep. 2019, 26, 285–287. [Google Scholar] [CrossRef]
- Low, S.Y.; Teo, F.; Eng, P.; Tan, P.H. Pulmonary sclerosing hemangioma: Pitfalls in management. Asian Cardiovasc Thorac Ann. 2011, 19, 139–142. [Google Scholar] [CrossRef]
- Gal, A.A.; Nassar, V.H.; Miller, J.I. Cytopathologic diagnosis of pulmonary sclerosing hemangioma. Diagn. Cytopathol. 2002, 26, 163–166. [Google Scholar] [CrossRef]
- Zeng, J.; Zhou, F.; Wei, X.J.; Kovacs, S.; Simsir, A.; Shi, Y. Sclerosing hemangioma: A diagnostic dilemma in fine needle aspiration cytology. Cytojournal 2016, 13, 9. [Google Scholar] [CrossRef]
- Ng, W.K.; Fu, K.H.; Wang, E.; Tang, V. Sclerosing hemangioma of lung: A close cytologic mimicker of pulmonary adenocarcinoma. Diagn. Cytopathol. 2001, 25, 316–320. [Google Scholar] [CrossRef]
- Dettrick, A.; Meikle, A.; Fong, K.M. Fine-needle aspiration diagnosis of sclerosing hemangioma (pneumocytoma): Report of a case and review of the literature. Diagn. Cytopathol. 2014, 42, 242–246. [Google Scholar] [CrossRef]
- Shiba, M.; Odaka, E.; Mitsunaga, S.; Yamakawa, H.; Yamaguchi, Y. A clinicopathological study of resected sclerosing hemangioma of the lung- its preoperative cytodiagnosis. J. Jpn. Soc. Clin. Cytol. 1992, 31, 378–385. [Google Scholar] [CrossRef][Green Version]
- Kalhor, N.; Staerkel, G.A.; Moran, C.A. So-called sclerosing hemangioma of lung: Current concept. Ann. Diagn. Pathol. 2010, 14, 60–67. [Google Scholar] [CrossRef]
- Iyoda, A.; Hiroshima, K.; Shiba, M.; Haga, Y.; Moriya, Y.; Sekine, Y.; Shibuya, K.; Iizasa, T.; Fujisawa, T. Clinicopathological analysis of pulmonary sclerosing hemangioma. Ann. Thorac. Surg. 2004, 78, 1928–1931. [Google Scholar] [CrossRef]
- Salemis, N.S.; Seretis, C.; Nakos, G.; Kantounakis, I.; Stoumpos, C.; Spiliopoulos, K. Synchronous occurrence of breast cancer and pulmonary sclerosing hemangioma: Management and review of the literature. Breast Dis. 2013, 34, 61–65. [Google Scholar] [CrossRef]
- Saha, K.; Sit, N.K.; Jash, D.; Maji, A. Diagnosis of sclerosing hemangioma of lung: Don’t rely on fine-needle aspiration cytology diagnosis alone. J. Cancer Res. Ther. 2013, 9, 748–750. [Google Scholar] [CrossRef]
- Onorati, M.; Nicola, M.; Bianchi, C.L.; Bini, F.; Bellaviti, N.; Di Nuovo, F. Pitfalls and Key Features of a Case of Sclerosing Pneumocytoma: A Cytological Challenge? Acta Cytol. 2016, 60, 85–88. [Google Scholar] [CrossRef]
- Hissong, E.; Rao, R. Pneumocytoma (sclerosing hemangioma), a potential pitfall. Diagn. Cytopathol. 2017, 45, 744–749. [Google Scholar] [CrossRef]
- Zhou, J. Covinsky MH. Sclerosing Pneumocytoma: A Carcinoma Mimicker. A Case Report and Literature Review. Ann. Clin. Lab. Sci. 2017, 47, 103–105. [Google Scholar] [PubMed]
- Lee, K.; Sasaki, M.; Kakimoto, T.; Morinaga, S.; Yamamoto, T.; Iwamaru, A.; Ogata, K.; Minematsu, N. Pulmonary sclerosing pneumocytoma demonstrating intratumoral hematoma. Respir. Med. Case Rep. 2019, 28, 100870. [Google Scholar] [CrossRef]
- Le, H.Y.; Pham, D.P.; Nguyen, K.T.; Hoang, V.A.; Trinh, T.S.; Do, Q. Pulmonary sclerosing pneumocytoma in an 18-year-old male patient: A case report and literature review. Medicine 2020, 99, e20869. [Google Scholar] [CrossRef] [PubMed]
- Shiina, Y.; Sakairi, Y.; Wada, H.; Tamura, H.; Fujiwara, T.; Nakajima, T.; Suzuki, H.; Chiyo, M.; Ota, M.; Ota, S.; et al. Sclerosing pneumocytoma diagnosed by preoperative endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA). Surg. Case Rep. 2018, 4, 20. [Google Scholar] [CrossRef]
- Kosmas, K.; Vamvakaris, I.; Psychogiou, E.; Megas, P.; Riga, D. Pulmonary sclerosing pneumocytoma mimicking malignancy in EBUS-TBNA: A case report. Cytopathology 2020, 32, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Blanco, L.Z.; Heagley, D.E.; Montebelli, F.; Gabrielli, E.; Reddy, V.; Ghai, R.; Gattuso, P. Cytologic features of sclerosing hemangioma of the lung on crush preparations. Diagn. Cytopathol. 2013, 41, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, N.; Ohara, M.; Mizuno, K.; Yorita, K. Imprint cytologic and immunocytochemical findings of sclerosing pneumocytoma. Diagn. Cytopathol. 2017, 45, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Wang, J.; Chang, N.Y. A Comparative Study of Intraoperative Cytology and Frozen Sections of Sclerosing Pneumocytoma. Int. J. Surg. Pathol. 2016, 24, 600–606. [Google Scholar] [CrossRef]
- Yang, C.H.; Lee, L.Y. Pulmonary sclerosing pneumocytoma remains a diagnostic challenge using frozen sections: A clinicopathological analysis of 59 cases. Histopathology 2018, 72, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Wang, T.; Jiang, L.; Yang, P.; Hu, J.; Jiang, J. Sclerosing pneumocytoma mixed with a columnar clear cell adenoma and a typical carcinoid: Case report and review of literature. Int. J. Clin. Exp. Pathol. 2020, 13, 2599–2607. [Google Scholar] [PubMed]
- Chan, A.C.; Chan, J.K. Can pulmonary sclerosing haemangioma be accurately diagnosed by intra-operative frozen section? Histopathology 2002, 41, 392–403. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Stromal Cuboidal/Round Cells | Surface Cells | |
|---|---|---|
| Size | small to intermediate | large |
| Architecture | papillary clusters or flat sheets | pavement-type pattern, resembling pneumocytes |
| Cytoplasm | moderate/abundant eosinophilic cytoplasm | foamy cytoplasm |
| Nuclei | round to oval bland nuclei, nuclear pleomorphism | intranuclear inclusions, coarser chromatin |
| Nucleoli | inconspicuous nucleoli | small and occasional |
| N/C ratio | high | low |
| Author | Year | Cases | Final Cytologic Diagnosis | No. of Patterns | Hemorragic Background | Mytosis/Necrosis | IHC | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vimentin | CK7 | EMA | TTF-1 | PR | Napsin-A | ER | CK AE1/AE3 | Ki67 | |||||||
| Dettrick [14] | 2012 | 1 | PSP | 3 | Y | N | + (both) | + (surface) | + (both) | + (both) | + (both) | + (surface) | + | low | |
| Saha [19] | 2013 | 1 | AC | 3 | Y | / | + (both) | <5% | |||||||
| Salemis [18] | 2013 | 1 | PSP | 3 | / | / | + (both) | + (both) | + (both) | + (stromal) | + (stromal) | ||||
| Onorati [20] | 2016 | 1 | PSP | 3 | Y | N | + (both) | + (both) | + (surface) | 5% | |||||
| Zeng [12] | 2016 | 1 | PSP | 3 | Y | N | + (both) | + (stromal) | + (surface) | <3% | |||||
| Hissong [21] | 2017 | 1 | AC | 3 | Y | / | + (surface) | + (both) | + (surface) | ||||||
| Zhou [22] | 2017 | 1 | AC | 2 | / | / | + (both) | + (surface) | |||||||
| Lee [23] | 2019 | 1 | PSP | 4 | / | / | + (surface) | + (both) | + (surface) | ||||||
| Sakai [24] | 2019 | 1 | PSP | 2 | / | / | + (both) | <5% | |||||||
| Le [25] | 2020 | 1 | PSP | 4 | / | / | + (both) | + (both) | + (stromal) | - | + (surface) | <1% | |||
| Author | Year | Cases | ROSE | Final Cytologic Diagnosis | IHC | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vimentin | CK7 | TTF-1 | PR | Napsin-A | Neuroendocrine Markers | p63 | Ki67 | |||||
| Shiina [26] | 2018 | 1 | N | PSP | + (stromal) | + (both) | + (both) | + (surface) | ||||
| Kosmas [27] | 2020 | 1 | N | SM | - | - | - | |||||
| Our case | 2020 | 1 | N | AC | + (both) | + (both) | - | <3% | ||||
| Author | Year | Cases | Final Diagnosis | No. of Patterns | Mytosis/Necrosis | Growth Patterns | Hemorragic Background | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Papillary | Sclerosing | Solid | Hemorragic | |||||||
| Blanco [28] | 2011 | 2 | PSP | 2 | N | + | - | - | + | Y |
| Kuroda [29] | 2016 | 3 | PSP (3) | 2 | / | + | - | + | - | / |
| Wu [30] | 2016 | 14 | PSP (7) AC (1) Benign (3) Deferred (3) | 2 | N | + | - | + | - | / |
| Yang [31] | 2017 | 59 | PSP (26) Malignancy (10) Benign (14) Deferred (9) | 2 to 4 | N | + (10) | + (14) | + (21) | + (14) | / |
| Cai [32] | 2020 | 1 | PSP | 3 | N | + | + | - | + | Y |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trabucco, S.M.R.; Brascia, D.; Cazzato, G.; De Iaco, G.; Colagrande, A.; Signore, F.; Ingravallo, G.; Resta, L.; Marulli, G. Pulmonary Sclerosing Pneumocytoma: A Pre and Intraoperative Diagnostic Challenge. Report of Two Cases and Review of the Literature. Medicina 2021, 57, 524. https://doi.org/10.3390/medicina57060524
Trabucco SMR, Brascia D, Cazzato G, De Iaco G, Colagrande A, Signore F, Ingravallo G, Resta L, Marulli G. Pulmonary Sclerosing Pneumocytoma: A Pre and Intraoperative Diagnostic Challenge. Report of Two Cases and Review of the Literature. Medicina. 2021; 57(6):524. https://doi.org/10.3390/medicina57060524
Chicago/Turabian StyleTrabucco, Senia Maria Rosaria, Debora Brascia, Gerardo Cazzato, Giulia De Iaco, Anna Colagrande, Francesca Signore, Giuseppe Ingravallo, Leonardo Resta, and Giuseppe Marulli. 2021. "Pulmonary Sclerosing Pneumocytoma: A Pre and Intraoperative Diagnostic Challenge. Report of Two Cases and Review of the Literature" Medicina 57, no. 6: 524. https://doi.org/10.3390/medicina57060524
APA StyleTrabucco, S. M. R., Brascia, D., Cazzato, G., De Iaco, G., Colagrande, A., Signore, F., Ingravallo, G., Resta, L., & Marulli, G. (2021). Pulmonary Sclerosing Pneumocytoma: A Pre and Intraoperative Diagnostic Challenge. Report of Two Cases and Review of the Literature. Medicina, 57(6), 524. https://doi.org/10.3390/medicina57060524