
Compliance with Prescription Guidelines for Glucose-Lowering Therapies According to Renal Function: Real-Life Study in Inpatients of Internal Medicine, Endocrinology and Cardiology Units

 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
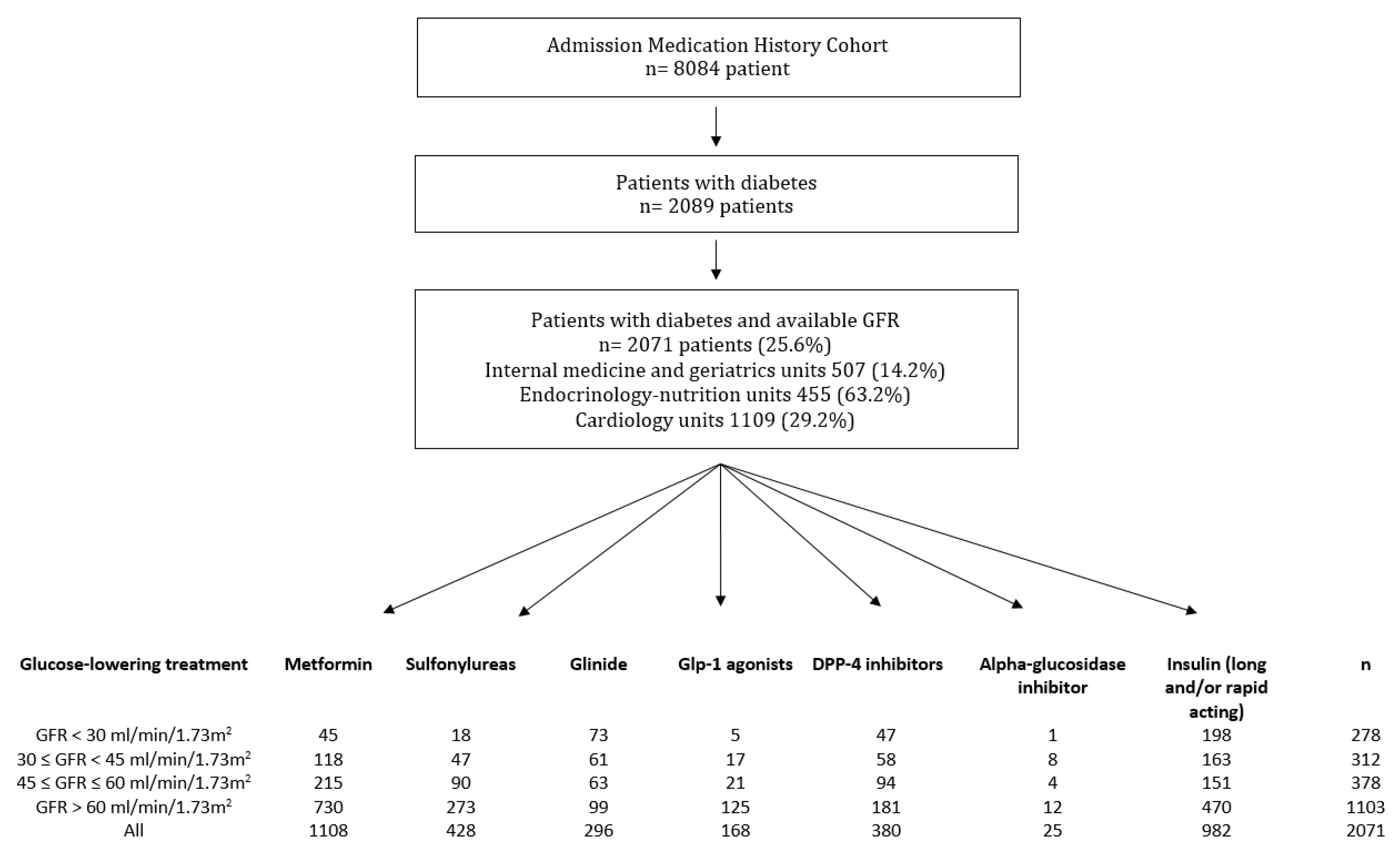
2.1. Study Design, Setting and Participants
2.2. Medication History Cohort Design
2.3. Data Collection
2.4. Statistical Analysis
2.5. Ethical Statement
3. Results
3.1. Characteristics of the Study Population
3.2. Inappropriate Prescription of Glucose-Lowering Treatment According to the Glomerular Filtration Rate
3.3. Variables Associated with an Excessive Daily Dose of Glucose-Lowering Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dei Cas, A.; Khan, S.S.; Butler, J.; Mentz, R.J.; Bonow, R.O.; Avogaro, A.; Tschoepe, D.; Doehner, W.; Greene, S.J.; Senni, M.; et al. Impact of diabetes on epidemiology, treatment, and outcomes of patients with heart failure. JACC Heart Fail. 2015, 3, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Kenny, H.C.; Abel, E.D. Heart Failure in Type 2 Diabetes Mellitus. Circ. Res. 2019, 124, 121–141. [Google Scholar] [CrossRef] [PubMed]
- Gheith, O.; Farouk, N.; Nampoory, N.; A Halim, M.; Al-Otaibi, T. Diabetic kidney disease: World wide difference of prevalence and risk factors. J. Nephropharmacol. 2016, 5, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Dean, J. Organising care for people with diabetes and renal disease. J. Ren. Care 2012, 38 (Suppl. 1), 23–29. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Jick, S.; Gopalakrishnan, C.; Heide-Jørgensen, U.; Nørrelund, H.; Sørensen, H.T.; Christiansen, C.F.; Ehrenstein, V. Metformin use and risk of lactic acidosis in people with diabetes with and without renal impairment: A cohort study in Denmark and the UK. Diabet. Med. 2017, 34, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Inzucchi, S.E.; Lipska, K.J.; Mayo, H.; Bailey, C.J.; McGuire, D.K. Metformin in patients with type 2 diabetes and kidney disease: A systematic review. JAMA 2014, 312, 2668–2675. [Google Scholar] [CrossRef] [PubMed]
- Alsahli, M.; Gerich, J.E. Hypoglycemia in Patients with Diabetes and Renal Disease. J. Clin. Med. 2015, 4, 948–964. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.J.; D’Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.; Buse, J.B. Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2018, 61, 2461–2498. [Google Scholar] [CrossRef] [PubMed]
- Darmon, P.; Bauduceau, B.; Bordier, L.; Bringer, J.; Chabrier, G.; Charbonnel, B.; Detournay, B.; Fontaine, P.; Grimaldi, A.; Gourdy, P.; et al. Prise de position de la Société Francophone du Diabète (SFD) sur la prise en charge médicamenteuse de l’hyperglycémie du patient diabétique de type 2. Méd. Mal. Métab. 2017, 11, 577–593. [Google Scholar] [CrossRef]
- Kajbaf, F.; Arnouts, P.; de Broe, M.; Lalau, J.-D. Metformin therapy and kidney disease: A review of guidelines and proposals for metformin withdrawal around the world. Pharmacoepidemiol. Drug Saf. 2013, 22, 1027–1035. [Google Scholar] [CrossRef]
- Food and Drug Administration. Drug Safety Communication: FDA Revises Warnings Regarding Use of the Diabetes Medicine Metformin in Certain Patients with Reduced Kidney Function. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-revises-warnings-regarding-use-diabetes-medicine-metformin-certain (accessed on 17 December 2021).
- European Medicines Agency. Use of Metformin to Treat Diabetes now Expanded to Patients with Moderately Reduced Kidney Function. Available online: https://www.ema.europa.eu/en/news/use-metformin-treat-diabetes-now-expanded-patients-moderately-reduced-kidney-function (accessed on 17 December 2021).
- Bergman, A.J.; Cote, J.; Yi, B.; Marbury, T.; Swan, S.K.; Smith, W.; Gottesdiener, K.; Wagner, J.; Herman, G.A. Effect of Renal Insufficiency on the Pharmacokinetics of Sitagliptin, a Dipeptidyl Peptidase-4 Inhibitor. Diabetes Care 2007, 30, 1862–1864. [Google Scholar] [CrossRef] [PubMed]
- He, Y.-L. Clinical Pharmacokinetics and Pharmacodynamics of Vildagliptin. Clin. Pharmacokinet. 2012, 51, 147–162. [Google Scholar] [CrossRef] [PubMed]
- Bittle, P.A. The use of dipeptidyl peptidase-4 inhibitors in patients with type 2 diabetes & chronic kidney disease. Nurse Pract. 2017, 42, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Dejager, S.; Penfornis, A.; Blickle, J.-F.; Fiquet, B.; Quere, S. How are patients with type 2 diabetes and renal disease monitored and managed? Insights from the observational OREDIA study. Vasc. Heal. Risk Manag. 2014, 10, 341–352. [Google Scholar] [CrossRef][Green Version]
- Becquemont, L.; Bauduceau, B.; Benattar-Zibi, L.; Al-Salameh, A.; Berrut, G.; Bertin, P.; Bucher, S.; Corruble, E.; Danchin, N.; Derumeaux, G.; et al. Cardiovascular Drugs and Metformin Drug Dosage According to Renal Function in Non-Institutionalized Elderly Patients. Basic Clin. Pharmacol. Toxicol. 2016, 118, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Douros, A.; Ebert, N.; Jakob, O.; Martus, P.; Kreutz, R.; Schaeffner, E. Estimating kidney function and use of oral antidiabetic drugs in elderly. Fundam. Clin. Pharmacol. 2015, 29, 321–328. [Google Scholar] [CrossRef]
- Solini, A.; Penno, G.; Bonora, E.; Fondelli, C.; Orsi, E.; Trevisan, R.; Vedovato, M.; Cavalot, F.; Cignarelli, M.; Morano, S.; et al. Age, Renal Dysfunction, Cardiovascular Disease, and Antihyperglycemic Treatment in Type 2 Diabetes Mellitus: Findings from the Renal Insufficiency and Cardiovascular Events Italian Multicenter Study. J. Am. Geriatr. Soc. 2013, 61, 1253–1261. [Google Scholar] [CrossRef]
- Detournay, B.; Simon, D.; Guillausseau, P.J.; Joly, D.; Verges, B.; Attali, C.; Clement, O.; Briand, Y.; Delaitre, O. Chronic kidney disease in type 2 diabetes patients in France: Prevalence, influence of glycaemic control and implications for the pharmacological management of diabetes. Diabetes Metab. 2012, 38, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Breuker, C.; Macioce, V.; Mura, T.; Castet-Nicolas, A.; Audurier, Y.; Boegner, C.; Jalabert, A.; Villiet, M.; Avignon, A.; Sultan, A. Medication Errors at Hospital Admission and Discharge: Risk Factors and Impact of Medication Reconciliation Process to Improve Healthcare. J. Patient Saf. 2021, 17, e645–e652. [Google Scholar] [CrossRef] [PubMed]
- Min, T.; Davies, G.I.; Rice, S.; Chess, J.; Stephens, J.W. Treatment choices for the glycaemic management of patients with type 2 diabetes and chronic kidney disease: Analysis of the SAIL patient linked dataset. Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 12, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, C.; Ehrenstein, V.; Heide-Jørgensen, U.; Skovbo, S.; Nørrelund, H.; Sørensen, H.T.; Li, L.; Jick, S. Metformin initiation and renal impairment: A cohort study in Denmark and the UK. BMJ Open 2015, 5, e008531. [Google Scholar] [CrossRef]
- Assogba, G.; Couchoud, C.; Roudier, C.; Pornet, C.; Fosse, S.; Romon, I.; Druet, C.; Stengel, B.; Fagot-Campagna, A. Prevalence, screening and treatment of chronic kidney disease in people with type 2 diabetes in France: The ENTRED surveys (2001 and 2007). Diabetes Metab. 2012, 38, 558–566. [Google Scholar] [CrossRef]
- McGovern, A.P.; Rusholme, B.; Jones, S.; Van Vlymen, J.N.; Liyanage, H.; Gallagher, H.; Tomson, C.R.V.; Khunti, K.; Harris, K.; De Lusignan, S. Association of chronic kidney disease (CKD) and failure to monitor renal function with adverse outcomes in people with diabetes: A primary care cohort study. BMC Nephrol. 2013, 14, 198. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.R.; Defilippi, J.; Braun, A. Unleash metformin: Reconsideration of the contraindication in patients with renal impairment. Ann. Pharmacother. 2013, 47, 1488–1497. [Google Scholar] [CrossRef] [PubMed]
- Lalau, J.D.; Kajbaf, F.; Bennis, Y.; Hurtel-Lemaire, A.S.; Belpaire, F.; De Broe, M.E. Metformin Treatment in Patients with Type 2 Diabetes and Chronic Kidney Disease Stages 3A, 3B, or 4. Diabetes Care 2018, 41, 547–553. [Google Scholar] [CrossRef]
- Van Dalem, J.; Brouwers, M.C.; Stehouwer, C.D.; Krings, A.; Leufkens, H.G.; Driessen, J.H.; de Vries, F.; Burden, A.M. Risk of hypoglycaemia in users of sulphonylureas compared with metformin in relation to renal function and sulphonylurea metabolite group: Population based cohort study. Br. Med. J. 2016, 354, i3625. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Seaquist, E.R.; Anderson, J.; Childs, B.; Cryer, P.; Dagogo-Jack, S.; Fish, L.; Heller, S.; Rodriguez, H.; Rosenzweig, J.; Vigersky, R. Hypoglycemia and Diabetes: A Report of a Workgroup of the American Diabetes Association and The Endocrine Society. J. Clin. Endocrinol. Metab. 2013, 98, 1845–1859. [Google Scholar] [CrossRef] [PubMed]
- Lohan, L.; Clément, F.; Duflos, C.; Villiet, M.; Castet-Nicolas, A.; Boegner, C.; Avignon, A.; Sultan, A.; Breuker, C. Hypoglycemia While Driving in Insulin-Treated Patients: Incidence and Risk Factors. J. Patient Saf. 2020, 17, e1034–e1039. [Google Scholar] [CrossRef] [PubMed]
- Buse, J.B.; Wexler, D.J.; Tsapas, A.; Rossing, P.; Mingrone, G.; Mathieu, C.; D’Alessio, D.A.; Davies, M.J. 2019 Update to: Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020, 43, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.-F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. New Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, M.K. Diabetic nephropathy: Recent advances in pathophysiology and challenges in dietary management. Diabetol. Metab. Syndr. 2019, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Class | Drug | Contraindication (GFR mL/min/1.73 m2) | Dose Adjustment (GFR mL/min/1.73 m2) |
|---|---|---|---|
| Biguanides | Metformin | <30 | ≥30–<60 Dose ≤ 1500 mg/day * |
| Sulfonylureas | Glimepiride | <30 | ≥30–<60 Dose < 6 mg/day ** |
| Gliclazide | <30 | None | |
| Glibenclamide | <30 | ≥30–<60 Dose < 15 mg/day ** | |
| Glinides | Repaglinide | None | <30 Dose < 12 mg/day ** |
| DPP-4 inhibitors | Vildagliptin | None | <60 Dose ≤ 50 mg/day * |
| Sitagliptin | None | <45 Dose ≤ 50 mg/day ** (30–44) Dose = 25 mg/day ** (<30) | |
| Saxagliptin | <15 | ≥15–<60 Dose ≤ 2.5 mg/day * | |
| GLP-1 agonists | Dulaglutide | <30 | None |
| Liraglutide | <15 | None | |
| Exenatide immediate release | <30 | ≥30–<50 Dose ≤ 2.5 mg/day * | |
| SGLT2i # | Dapagliflozin | <45 | <60 should not be initiated ** |
| Empagliflozin | <45 | <60 initiation not recommended ** ≥45–<60 Dose 10 mg/day ** | |
| Canagliflozin | <45 | <60 initiation not recommended ** ≥45–<60 Dose 100 mg/day ** | |
| Ertugliflozin | <30 | <60 initiation not recommended ** Continued use not recommended with persistent GFR 30–60 mL/min/1.73 m2 |
| GFR Categories (mL/min/1.73 m2) | All | <30 | 30–44 | 45–60 | >60 | p |
|---|---|---|---|---|---|---|
| n (%) | 2071 (100) | 278 (13.4) | 312 (15.1) | 378 (18.3) | 1103 (53.3) | |
| Age (years) | 71.0 ± 13.9 | 78.2 ± 11.6 | 77.2 ± 10.2 | 75.2 ± 10.5 | 65.9 ± 14.3 | <0.001 |
| Gender–Male | 1230 (59.4) | 141 (50.7) | 180 (57.7) | 230 (60.9) | 679 (61.6) | 0.009 |
| HbA1c (%) * | 7.8 ± 1.6 | 7.4 ± 1.1 | 7.5 ± 1.4 | 7.4 ± 1.4 | 8.0 ± 1.8 | <0.001 |
| GFR (mL/min/1.73 m2) | 63.2 ± 27.4 | 20.2 ±6.9 | 37.8 ±4.3 | 52.4 ±4.5 | 84.9 ± 15.0 | <0.001 |
| Admission units | <0.001 | |||||
| Internal medicine and geriatrics | 507 (24.5) | 99 (35.6) | 88 (28.2) | 102 (27.0) | 218 (19.8) | |
| Endocrinology-nutrition | 455 (22.0) | 20 (7.2) | 22 (7.1) | 48 (12.7) | 365 (33.1) | |
| Cardiology | 1109 (53.5) | 159 (57.2) | 202 (64.7) | 228 (60.3) | 520 (47.1) | |
| Number of treatments on admission | 9.6 ± 4.0 | 11.5 ± 3.9 | 10.8 ± 3.5 | 9.9 ± 3.5 | 8.6 ± 4.0 | <0.001 |
| Number of glucose-lowering treatments on admission | <0.001 | |||||
| 1 | 824 (39.8) | 94 (33.8) | 129 (41.4) | 162 (42.9) | 439 (39.8) | |
| 2 | 765 (36.9) | 143 (51.4) | 134 (42.9) | 129 (34.1) | 359 (32.6) | |
| 3 | 350 (16.9) | 38 (13.7) | 34 (10.9) | 62 (16.4) | 216 (19.6) | |
| ≥4 | 132 (6.4) | 3 (1.1) | 15 (4.8) | 25 (6.6) | 89 (8.1) |
| GFR Categories (mL/min/1.73 m2) | All | <30 | 30–44 | 45–60 | >60 |
|---|---|---|---|---|---|
| Biguanides | 211/1108 (19.0) | 45/45 (100) | 58/118 (49.2) | 108/215 (50.3) | 0/730 (0) |
| Sulfonylureas | 27/427 (6.3) | 18/18 (100) | 2/47 (4.3) | 7/90 (7.8) | 0/273 (0) |
| Glinides | 12/296 (4.1) | 12/73 (16.4) | 0/61 (0) | 0/63 (0) | 0/99 (0) |
| GLP1 agonists | 0/168 (0) | 0/5 (0) | 0/17 (0) | 0/21 (0) | 0/125 (0) |
| DPP-4 inhibitors | 57/380 (15.0) | 21/47 (44.7) | 31/58 (53.4) | 5/94 (5.3) | 0/181 (0) |
| Biguanides (n = 333) | Sulfonylureas (n = 137) | DPP-4 Inhibitors (n = 199) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Appropriate (n = 167) | Excessive (n = 166) | p | Appropriate (n = 128) | Excessive (n = 9) | p | Appropriate (n = 142) | Excessive (n = 57) | p | |
| Age (years) | 75.9 (±10.7) | 73.2 (±9.9) | 0.011 | 77.1 (±10.2) | 72.0 (±7.9) | 0.089 | 77.1 (±10.4) | 78.5 (±9.0) | 0.47 |
| Gender–Male | 56.3 | 69.3 | 0.014 | 65.6 | 44.4 | 0.28 | 63.4 | 68.4 | 0.50 |
| HbA1c (%) | 7.1 (±1.2) | 7.51 (±1.4) | 0.033 | 7.4 (±1.5) | 8.5 (±1.8) | 0.10 | 7.3 (±1.2) | 7.4 (±1.6) | 0.84 |
| GFR | 47.3 (±8.4) | 48.0 (±7.8) | 0.50 | 47.8 (±8.1) | 49.4 (±6.5) | 0.65 | 43.8 (±12.8) | 33.8 (±10.1) | <0.001 |
| Units | 0.15 | 0.016 | 0.50 | ||||||
| Internal medicine/geriatrics | 56 (33.5) | 40 (24.1) | 39 (30.5) | 1 (11.1) | 45 (31.7) | 14 (24.6) | |||
| Endocrinology-nutrition | 18 (10.8) | 18 (10.8) | 12 (9.4) | 4 (44.4) | 13 (9.2) | 3 (5.3) | |||
| Cardiology | 93 (55.7) | 108 (65.1) | 77 (60.2) | 4 (44.4) | 84 (59.2) | 40 (70.2) | |||
| Number of treatments | 10.1 (±3.3) | 9.9 (±3.5) | 0.65 | 10.1 (±3.3) | 10.8 (±2.2) | 0.56 | 10.8 (±3.6) | 10.6 (±3.9) | 0.65 |
| Number of glucose-lowering treatments at home | 0.015 | 0.009 | 0.12 | ||||||
| 1 | 78 (46.7) | 50 (30.1) | 42 (32.8) | 0 (0.0) | 18 (12.7) | 14 (24.6) | |||
| 2 | 45 (26.9) | 61 (36.7) | 50 (39.1) | 2 (22.2) | 53 (37.3) | 22 (38.6) | |||
| 3 | 30 (18.0) | 33 (19.9) | 20 (15.6) | 4 (44.4) | 50 (35.2) | 17 (29.8) | |||
| ≥4 | 14 (8.4) | 22 (13.2) | 16 (12.5) | 3 (33.3) | 21 (14.8) | 4 (7.0) | |||
| Insulin treatment–Yes | 39 (23.3) | 51 (30.7) | 0.13 | 24 (18.7) | 6 (66.7) | 0.004 | 57 (40.1) | 15 (26.3) | 0.067 |
| Basal insulin | 33 (19.8) | 43 (25.9) | 0.18 | 21 (16.4) | 6 (66.7) | 0.002 | 50 (35.2) | 13 (22.8) | 0.089 |
| Prandial insulin | 16 (9.6) | 22 (13.2) | 0.29 | 5 (3.9) | 1 (11.1) | 0.34 | 25 (17.6) | 5 (8.8) | 0.11 |
| Biguanides | Sulfonylureas | DPP-4 Inhibitors | ||||
|---|---|---|---|---|---|---|
| OR IC95% | p | OR IC95% | p | OR IC95% | p | |
| Age | 0.96 (0.93–0.99) | 0.007 | 1.08 (0.08–14.13) | 0.95 | - | - |
| Gender–Female vs. Male | 0.80 (0.44–1.44) | 0.46 | - | - | - | - |
| HbA1c | 1.2 (0.91–1.49) | 0.23 | 3.30 (0.37–29.24) | 0.28 | - | |
| GFR | - | - | - | - | 0.93 (0.90–0.96) | <0.001 |
| Internal medicine/geriatrics vs. cardiology units | 0.56 (0.30–1.05) | 0.070 | 1.01 (0.94–1.10) | 0.72 | - | - |
| Endocrinology-nutrition vs. cardiology units | 0.46 (0.19–1.14) | 0.093 | 1.23 (0.69–2.19) | 0.48 | - | - |
| Number of antidiabetic treatment | ||||||
| 1 | 1 | - | - | 1.37 (0.53–3.51) | 0.51 | |
| 2 | 1.92 (0.94–3.91) | 0.074 | - | - | 1 | |
| 3 | 1.80 (0.65–4.99) | 0.26 | - | - | 1.17 (0.46–2.95) | 0.74 |
| 4 | 1.74 (0.50–5.99) | 0.38 | - | - | 2.16 (0.45–10.36) | 0.33 |
| Insulin treatment–Yes vs. No | 1.09 (0.45–2.61) | 0.85 | 14.18 (1.39–144.70) | 0.025 | 0.26 (0.09–0.78) | 0.016 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lohan, L.; Galtier, F.; Manson, T.; Mura, T.; Castet-Nicolas, A.; Faure, D.; Chapet, N.; Leclercq, F.; Pasquié, J.L.; Roubille, F.; et al. Compliance with Prescription Guidelines for Glucose-Lowering Therapies According to Renal Function: Real-Life Study in Inpatients of Internal Medicine, Endocrinology and Cardiology Units. Medicina 2021, 57, 1376. https://doi.org/10.3390/medicina57121376
Lohan L, Galtier F, Manson T, Mura T, Castet-Nicolas A, Faure D, Chapet N, Leclercq F, Pasquié JL, Roubille F, et al. Compliance with Prescription Guidelines for Glucose-Lowering Therapies According to Renal Function: Real-Life Study in Inpatients of Internal Medicine, Endocrinology and Cardiology Units. Medicina. 2021; 57(12):1376. https://doi.org/10.3390/medicina57121376
Chicago/Turabian StyleLohan, Laura, Florence Galtier, Thibault Manson, Thibault Mura, Audrey Castet-Nicolas, Delinger Faure, Nicolas Chapet, Florence Leclercq, Jean Luc Pasquié, François Roubille, and et al. 2021. "Compliance with Prescription Guidelines for Glucose-Lowering Therapies According to Renal Function: Real-Life Study in Inpatients of Internal Medicine, Endocrinology and Cardiology Units" Medicina 57, no. 12: 1376. https://doi.org/10.3390/medicina57121376
APA StyleLohan, L., Galtier, F., Manson, T., Mura, T., Castet-Nicolas, A., Faure, D., Chapet, N., Leclercq, F., Pasquié, J. L., Roubille, F., Roubille, C., Blain, H., Guilpain, P., Villiet, M., Avignon, A., Sultan, A., & Breuker, C. (2021). Compliance with Prescription Guidelines for Glucose-Lowering Therapies According to Renal Function: Real-Life Study in Inpatients of Internal Medicine, Endocrinology and Cardiology Units. Medicina, 57(12), 1376. https://doi.org/10.3390/medicina57121376