
Increase of Myocardial Ischemia Time and Short-Term Prognosis of Patients with Acute Myocardial Infarction during the First COVID-19 Pandemic Wave


Abstract
:1. Introduction
2. Methods
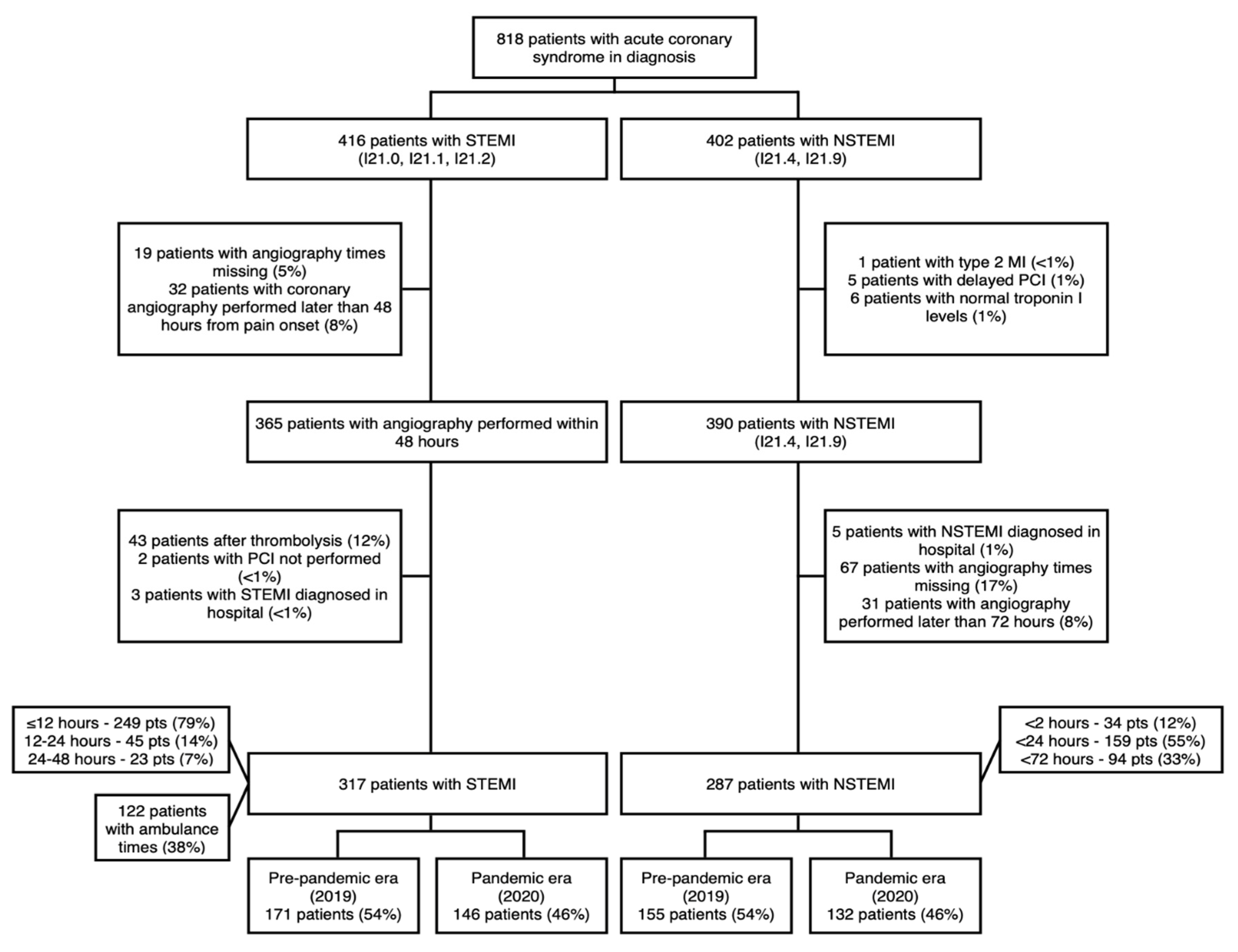
- Diagnosis of STEMI and NSTEMI
- Coronary angiography performed
- Symptom onset time < 48 h for patients with STEMI
- Type 2 myocardial infarction
- Coronary angiography not performed
- Nonobstructive coronary artery disease
- STEMI or NSTEMI diagnosed while admitted to hospital for other reason
- Thrombolysis performed
3. Statistical Analysis
4. Results
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. COVID-19 Dashboard; World Health Organization: Geneva, Switzerland, 2020; Available online: https://covid19.who.int. (accessed on 13 October 2021).
- De Rosa, S.; Spaccarotella, C.; Basso, C.; Calabrò, M.P.; Curcio, A.; Filardi, P.P.; Mancone, M.; Mercuro, G.; Muscoli, S.; Nodari, S.; et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur. Heart J. 2020, 41, 2083–2088. [Google Scholar] [CrossRef]
- De Filippo, O.; D’Ascenzo, F.; Angelini, F.; Bocchino, P.P.; Conrotto, F.; Saglietto, A.; Secco, G.G.; Campo, G.; Gallone, G.; Verardi, R.; et al. Reduced rate of hospital admissions for acs during COVID-19 outbreak in northern Italy. N. Engl. J. Med. 2020, 383, 88–89. [Google Scholar] [CrossRef] [PubMed]
- Metzler, B.; Siostrzonek, P.; Binder, R.K.; Bauer, A.; Reinstadler, S.J. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19: The pandemic response causes cardiac collateral damage. Eur. Heart J. 2020, 41, 1852–1853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, S.J.; Connolly, M.J.; Elghamry, Z.; Cosgrove, C.; Firoozi, S.; Lim, P.; Sharma, R.; Spratt, J.C. Effect of the COVID-19 pandemic on ST-segment-elevation myocardial infarction presentations and in-hospital outcomes. Circ. Cardiovasc. Interv. 2020, 13, e009438. [Google Scholar] [CrossRef] [PubMed]
- Mafham, M.M.; Spata, E.; Goldacre, R.; Gair, D.; Curnow, P.; Bray, M.; Hollings, S.; Roebuck, C.; Gale, C.P.; Mamas, M.A.; et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet Lond Engl. 2020, 396, 381–389. [Google Scholar] [CrossRef]
- Mesnier, J.; Cottin, Y.; Coste, P.; Ferrari, E.; Schiele, F.; Lemesle, G.; Thuaire, C.; Angoulvant, D.; Cayla, G.; Bouleti, C.; et al. Hospital admissions for acute myocardial infarction before and after lockdown according to regional prevalence of COVID-19 and patient profile in France: A registry study. Lancet Public Health 2020, 5, e536–e542. [Google Scholar] [CrossRef]
- Sokolski, M.; Gajewski, P.; Zymlinski, R.; Biegus, J.; Berg, J.M.T.; Bor, W.; Braunschweig, F.; Caldeira, D.; Cuculi, F.; D’elia, E.; et al. Impact of coronavirus disease 2019 (COVID-19) outbreak on acute admissions at the emergency and cardiology departments across Europe. Am. J. Med. 2020, 134, 482–489. [Google Scholar] [CrossRef]
- Rashid, M.; Gale, C.P.; Curzen, N.; Ludman, P.; De Belder, M.; Timmis, A.; Mohamed, M.O.; Luscher, T.F.; Hains, J.; Wu, J.; et al. Impact of COVID19 pandemic on the incidence and management of out of hospital cardiac arrest in patients presenting with acute myocardial infarction in England. J. Am. Heart Assoc. 2020, 9, e018379. [Google Scholar]
- Fardman, A.; Oren, D.; Berkovitch, A.; Segev, A.; Levy, Y.; Beigel, R.; Matetzky, S. Post COVID-19 acute myocardial infarction rebound. Can. J. Cardiol. 2020, 36, 1832.e15–1832.e16. [Google Scholar] [CrossRef]
- Xiang, D.; Xiang, X.; Zhang, W.; Yi, S.; Zhang, J.; Gu, X.; Xu, Y.; Huang, K.; Su, X.; Yu, B.; et al. Management and outcomes of patients with STEMI during the COVID-19 pandemic in China. J. Am. Coll. Cardiol. 2020, 76, 1318–1324. [Google Scholar] [CrossRef]
- Zaleski, A.L.; Taylor, B.A.; McKay, R.G.; Thompson, P.D. Declines in acute cardiovascular emergencies during the COVID-19 pandemic. Am. J. Cardiol. 2020, 129, 124–125. [Google Scholar] [CrossRef]
- Folino, A.F.; Zorzi, A.; Cernetti, C.; Marchese, D.; Pasquetto, G.; Roncon, L.; Sacca, S.; Themistoclakis, S.; Turiano, G.; Verlato, R.; et al. Impact of COVID-19 epidemic on coronary care unit accesses for acute coronary syndrome in Veneto region, Italy. Am. Heart J. 2020, 226, 26–28. [Google Scholar] [CrossRef]
- Advani, I.; Gunge, D.; Banks, S.; Mehta, S.; Park, K.; Patel, M.; Malhotra, A.; Alexander, L.E.C. Is increased sleep responsible for reductions in myocardial infarction during the COVID-19 pandemic? Am. J. Cardiol. 2020, 131, 128–130. [Google Scholar] [CrossRef]
- Gluckman, T.J.; Wilson, M.A.; Chiu, S.-T.; Penny, B.W.; Chepuri, V.B.; Waggoner, J.W.; Spinelli, K.J. Case rates, treatment approaches, and outcomes in acute myocardial infarction during the Coronavirus disease 2019 pandemic. JAMA Cardiol. 2020, 5, 1419–1424. [Google Scholar] [CrossRef] [PubMed]
- Braiteh, N.; Rehman, W.U.; Alom, M.; Skovira, V.; Breiteh, N.; Rehman, I.; Yarkoni, A.; Kahsou, H.; Rehman, A. Decrease in acute coronary syndrome presentations during the COVID-19 pandemic in upstate New York. Am. Heart J. 2020, 226, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Khot, U.N.; Reimer, A.P.; Brown, A.; Hustey, F.M.; Hussain, M.S.; Kapadia, S.R.; Svensson, L.G. Impact of COVID-19 pandemic on critical care transfers for ST-segment-elevation myocardial infarction, stroke, and aortic emergencies. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e006938. [Google Scholar] [CrossRef]
- Solomon, M.D.; McNulty, E.J.; Rana, J.S.; Leong, T.K.; Lee, C.; Sung, S.-H.; Ambrosy, A.P.; Sidney, S.; Go, A.S. The COVID-19 Pandemic and the incidence of acute myocardial infarction. N. Engl. J. Med. 2020, 383, 691–693. [Google Scholar] [CrossRef] [PubMed]
- Lotfi, A.S.; Capatina, A.; Kugelmass, A.D. Assessment of ST-segment elevation myocardial infarction volume trends during the COVID-19 pandemic. Am. J. Cardiol. 2020, 131, 132–133. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, H.K.; Abdelrahman, A.; Nabi, A.; Debski, M.; Mentias, A.; Choudhury, T.; Patel, B.; Saad, M. Impact of COVID-19 pandemic on patients with ST-segment elevation myocardial infarction: Insights from a British cardiac center. Am. Heart J. 2020, 226, 45–48. [Google Scholar] [CrossRef]
- Garcia, S.; Albaghdadi, M.S.; Meraj, P.M.; Schmidt, C.; Garberich, R.; Jaffer, F.A.; Dixon, S.; Rade, J.J.; Tannenbaum, M.; Chambers, J.; et al. Reduction in ST-segment elevation cardiac catheterization laboratory activations in the United States during COVID-19 pandemic. J. Am. Coll. Cardiol. 2020, 75, 2871–2872. [Google Scholar] [CrossRef]
- Mohammad, M.A.; Koul, S.; Olivecrona, G.K.; Gӧtberg, M.; Tydén, P.; Rydberg, E.; Schersten, F.; Alfredsson, J.; Vasko, P.; Omerovic, E.; et al. Incidence and outcome of myocardial infarction treated with percutaneous coronary intervention during COVID-19 pandemic. Heart Br. Card Soc. 2020, 106, 1812–1818. [Google Scholar] [CrossRef]
- Available online: https://ourworldindata.org/coronavirus (accessed on 13 October 2021).
- Kwok, C.S.; Gale, C.P.; Kinnaird, T.; Curzen, N.; Ludman, P.; Kontopantelis, E.; Wu, J.; Denwood, T.; Fazal, N.; Deanfield, J.; et al. Impact of COVID-19 on percutaneous coronary intervention for ST-elevation myocardial infarction. Heart Br. Card Soc. 2020, 106, 1805–1811. [Google Scholar] [CrossRef]
- Baldi, E.; Sechi, G.M.; Mare, C.; Canevari, F.; Brancaglione, A.; Primi, R.; Klersy, C.; Palo, A.; Contri, E.; Ronchi, V.; et al. Out-of-hospital cardiac arrest during the COVID-19 outbreak in Italy. N. Engl. J. Med. 2020, 383, 496–498. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Tumminello, G.; Barbieri, L.; Lucreziotti, S.; Gentile, D.; Conconi, B.; Centola, M.; Mafrici, A.; Carugo, S. Impact of COVID-19 on STEMI: Second youth for fibrinolysis or time to centralized approach? IJC Heart Vasc. 2020, 30, 100600. [Google Scholar] [CrossRef] [PubMed]
- Baigent, C.; Windecker, S.; Andreini, D.; Arbelo, E.; Barbato, E.; Bartorelli, A.L.; Baumbach, A.; Behr, E.R.; Berti, S.; Bueno, H.; et al. ESC guidance for the diagnosis and management of CV disease during the COVID-19 pandemic. Eur. Heart J. 2021, 119. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | STEMI Patients | NSTEMI Patients | ||||
|---|---|---|---|---|---|---|
| 2019 (n = 171) | 2020 (n = 146) | p | 2019 (n = 155) | 2020 (n = 132) | p | |
| Age | 67.0 [59.0–76.5] | 65.0 [57.0–74.0] | 0.01 | 68.0 [59.0–78.0] | 68.5 [59.0–76.0] | 0.71 |
| Female sex | 48 (28.1) | 34 (23.3) | 0.40 | 57 (36.8) | 46 (34.8) | 0.83 |
| Previous MI | 26 (15.2) | 18 (12.3) | 0.57 | 37 (23.9) | 34 (25.8) | 0.82 |
| Previous PCI | 19 (11.1) | 18 (12.3) | 0.57 | 24 (15.5) | 29 (22.0) | 0.42 |
| Previous CABG | 2 (1.2) | 1 (0.7) | 3 (1.9) | 3 (2.3) | ||
| Arterial Hypertension | 126 (73.7) | 123 (84.8) | 0.02 | 141 (91.0) | 120 (90.9) | 1.00 |
| Dyslipidemia | 136 (80.5) | 130 (89.7) | 0.04 | 134 (86.5) | 115 (87.1) | 1.00 |
| Diabetes mellitus (Type 2) | 23 (13.5) | 21 (14.4) | 0.27 | 26 (16.8) | 37 (28.0) | 0.04 |
| Smoking | 50 (56.2) | 48 (76.2) | 0.02 | 36 (63.2) | 22 (45.8) | 0.11 |
| Chronic kidney disease (eGFR < 60 ml/min/1.73m2) | 42 (24.7) | 26 (17.9) | 0.19 | 32 (20.6) | 32 (24.2) | 0.56 |
| Characteristic | STEMI Patients | NSTEMI Patients | ||||
|---|---|---|---|---|---|---|
| 2019 (n = 171) | 2020 (n = 146) | p | 2019 (n = 155) | 2020 (n = 132) | p | |
| MI localization | ||||||
| Anterior | 71 (41.5) | 72 (49.3) | 0.37 | 37 (48.7) | 27 (50.0) | 0.39 |
| Inferior | 91 (53.2) | 68 (46.6) | 15 (19.7) | 15 (27.8) | ||
| Other | 9 (5.3) | 6 (4.1) | 24 (31.6) | 12 (22.2) | ||
| Killip class | ||||||
| I | 103 (60.2) | 99 (67.8) | 0.04 | 131 (84.5) | 103 (78.0) | 0.13 |
| II | 41 (24.0) | 31 (21.2) | 15 (9.7) | 24 (18.2) | ||
| III | 4 (2.3) | 8 (5.5) | 6 (3.9) | 2 (1.5) | ||
| IV | 23 (13.5) | 8 (5.5) | 3 (1.9) | 3 (2.3) | ||
| Out-of-hospital cardiac arrest | 7 (4.1) | 5 (3.4) | 0.99 | 2 (1.3) | 2 (1.5) | 1.00 |
| Peak hs-TnI, ng/l | 22,448 [5339–64,349] | 22,133 [4405–97,113] | 0.69 | 1681 [376–9828] | 1938 [499–6763] | 0.82 |
| LV EF, % | 40 [35–47] | 40 [35–47] | 0.87 | 50 [45–55] | 50 [40–55] | 0.32 |
| Length of hospital stay, days | 8 [5–22] | 7 [5–15] | 0.58 | 6 [3–9] | 6 [3–8] | 0.96 |
| Referral to cardiac rehab | 112 (72.3) | 80 (56.7) | 0.008 | 83 (57.6) | 46 (35.9) | 0.001 |
| Characteristic | STEMI Patients | NSTEMI Patients | ||||
|---|---|---|---|---|---|---|
| 2019 (n = 171) | 2020 (n = 146) | p | 2019 (n = 155) | 2020 (n = 132) | p | |
| No. of diseased coronary arteries | ||||||
| 1 | 59 (34.5) | 50 (34.2) | 0.72 | 27 (17.4) | 32 (24.2) | 0.17 |
| 2 | 52 (30.4) | 50 (34.2) | 67 (43.2) | 44 (33.3) | ||
| 3 | 60 (35.1) | 46 (31.5) | 61 (39.4) | 56 (42.4) | ||
| Total occlusion of coronary artery | 119 (69.6) | 94 (64.4) | 0.39 | 31 (20.0) | 30 (22.7) | 0.68 |
| Culprit artery | ||||||
| LAD | 68 (39.8) | 69 (47.3) | 0.62 | 55 (38.2) | 53 (41.7) | 0.65 |
| LCX | 33 (19.3) | 24 (16.4) | 49 (34.0) | 37 (29.1) | ||
| RCA | 67 (39.2) | 51 (34.9) | 29 (20.1) | 28 (22.0) | ||
| LM | 2 (1.2) | 2 (1.4) | 2 (1.4) | 4 (3.1) | ||
| Graft | 1 (0.6) | 0 (0.0) | 9 (6.2) | 5 (3.9) | ||
| TIMI flow pre-PCI | ||||||
| 0 | 115 (67.3) | 91 (62.8) | 0.78 | 24 (15.5) | 22 (17.2) | 0.93 |
| 1 | 9 (5.3) | 11 (7.6) | 7 (4.5) | 6 (4.7) | ||
| 2 | 15 (8.8) | 13 (9.0) | 19 (12.3) | 18 (14.1) | ||
| 3 | 32 (18.7) | 30 (20.7) | 105 (67.7) | 82 (64.1) | ||
| TIMI flow post-PCI | ||||||
| 0 | 3 (1.8) | 2 (1.4) | 0.98 | 1 (0.6) | 1 (0.8) | 0.56 |
| 1 | 2 (1.2) | 2 (1.4) | 0 (0.0) | 1 (0.8) | ||
| 2 | 8 (4.7) | 8 (5.5) | 1 (0.6) | 0 (0.0) | ||
| 3 | 158 (92.4) | 133 (91.7) | 153 (98.7) | 126 (98.4) | ||
| Conservative treatment | 0 (0.0) | 1 (0.7) | 0.94 | 0 (0.0) | 5 (3.8) | 0.03 |
| Complications related to PCI | ||||||
| Distal embolisation | 5 (2.9) | 1 (0.7) | 0.10 | |||
| Coronary artery dissection | 0 (0.0) | 1 (0.7) | ||||
| Coronary artery perforation | 1 (0.6) | 0 (0.0) | ||||
| Side branch occlusion | 4 (2.3) | 0 (0.0) | ||||
| Without complications | 161 (94.2) | 142 (98.6) | 155 (100.0) | 128 (99.2) | 0.93 | |
| Revascularisation status after PCI | ||||||
| Full revascularisation achieved | 46 (27.2) | 51 (35.2) | 0.13 | 25 (16.1) | 23 (17.8) | 0.09 |
| Second procedure planned for other lesions | 27 (16.0) | 28 (19.3) | 15 (9.7) | 4 (3.1) | ||
| Conservative treatment for other lesions | 96 (56.8) | 66 (45.5) | 115 (74.2) | 102 (79.1) | ||
| IABP or ECMO | 7 (4.1) | 4 (2.7) | 0.73 | 2 (1.3) | 0 (0.0) | 0.55 |
| Staged revascularisation during index hospital stay | 14 (8.2) | 17 (11.7) | 0.39 | 6 (3.9) | 4 (3.1) | 0.96 |
| Adverse Event | STEMI Patients | NSTEMI Patients | ||||
|---|---|---|---|---|---|---|
| 2019 (n = 171) | 2020 (n = 146) | p | 2019 (n = 155) | 2020 (n = 132) | p | |
| Worsening of heart failure during hospital stay | 19 (11.1) | 11 (7.5) | 0.37 | 4 (2.6) | 4 (3.0) | 1.00 |
| Stroke during hospital stay | 0 (0.0) | 0 (0.0) | NA | 0 (0.0) | 0 (0.0) | NA |
| Recurrent MI during hospital stay | 0 (0.0) | 0 (0.0) | NA | 0 (0.0) | 0 (0.0) | NA |
| In-hospital death | 15 (9.4) | 5 (3.4) | 0.059 | 2 (1.3) | 1 (0.8) | 1.00 |
| Death at 3 months follow-up | 18 (10.5) | 10 (6.8) | 0.34 | 4 (2.6) | 7 (5.3) | 0.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Budrys, P.; Lizaitis, M.; Cerlinskaite-Bajore, K.; Bajoras, V.; Rodevic, G.; Martinonyte, A.; Dieckus, L.; Badaras, I.; Serpytis, P.; Gurevicius, R.; et al. Increase of Myocardial Ischemia Time and Short-Term Prognosis of Patients with Acute Myocardial Infarction during the First COVID-19 Pandemic Wave. Medicina 2021, 57, 1296. https://doi.org/10.3390/medicina57121296
Budrys P, Lizaitis M, Cerlinskaite-Bajore K, Bajoras V, Rodevic G, Martinonyte A, Dieckus L, Badaras I, Serpytis P, Gurevicius R, et al. Increase of Myocardial Ischemia Time and Short-Term Prognosis of Patients with Acute Myocardial Infarction during the First COVID-19 Pandemic Wave. Medicina. 2021; 57(12):1296. https://doi.org/10.3390/medicina57121296
Chicago/Turabian StyleBudrys, Povilas, Mindaugas Lizaitis, Kamile Cerlinskaite-Bajore, Vilhelmas Bajoras, Greta Rodevic, Aurelija Martinonyte, Laurynas Dieckus, Ignas Badaras, Pranas Serpytis, Romualdas Gurevicius, and et al. 2021. "Increase of Myocardial Ischemia Time and Short-Term Prognosis of Patients with Acute Myocardial Infarction during the First COVID-19 Pandemic Wave" Medicina 57, no. 12: 1296. https://doi.org/10.3390/medicina57121296
APA StyleBudrys, P., Lizaitis, M., Cerlinskaite-Bajore, K., Bajoras, V., Rodevic, G., Martinonyte, A., Dieckus, L., Badaras, I., Serpytis, P., Gurevicius, R., Visinskiene, R., Buivydas, R., Volodko, A., Urbonaite, E., Celutkiene, J., & Davidavicius, G. (2021). Increase of Myocardial Ischemia Time and Short-Term Prognosis of Patients with Acute Myocardial Infarction during the First COVID-19 Pandemic Wave. Medicina, 57(12), 1296. https://doi.org/10.3390/medicina57121296