
A Systematic Review to Assess the Impact of Hyperbaric Oxygen Therapy on Glycaemia in People with Diabetes Mellitus

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
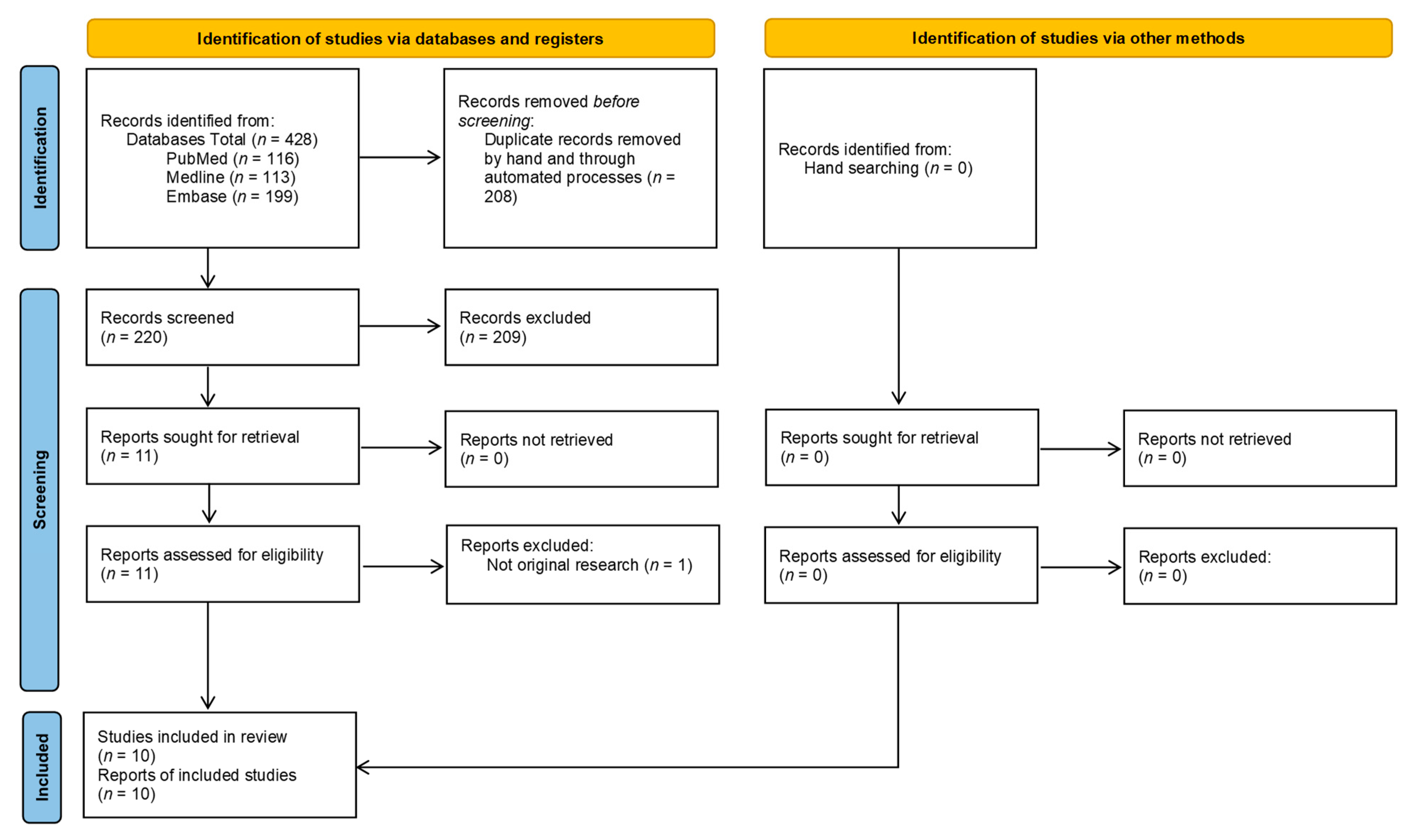
2.1. Study Selection
2.2. Data Extraction
2.3. Quality Assessment
2.4. Data Synthesis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Search Number | Query | Results |
|---|---|---|
| 17 | #15 AND #16 | 116 |
| 16 | #3 AND #6 | 931 |
| 15 | #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 | 624,093 |
| 14 | “hypoglycemia”[MeSH Terms] | 28,951 |
| 13 | hypoglycaemia[Title/Abstract] OR hypoglycemia[Title/Abstract] OR hypoglycaemic[Title/Abstract] OR hypoglycemic[Title/Abstract] | 59,161 |
| 12 | “hyperglycemia”[MeSH Terms] | 37,247 |
| 11 | hyperglycaemia[Title/Abstract] OR hyperglycemia[Title/Abstract] OR hyperglycaemic[Title/Abstract] OR hyperglycemic[Title/Abstract] | 65,507 |
| 10 | “glycemic control”[MeSH Terms] | 270 |
| 9 | glycemic[Title/Abstract] OR glycaemic[Title/Abstract] | 50,821 |
| 8 | “blood glucose”[MeSH Terms] | 168,266 |
| 7 | “blood sugar”[Title/Abstract] OR glucose[Title/Abstract] | 502,819 |
| 6 | #4 OR #5 | 16,145 |
| 5 | “Hyperbaric Oxygenation”[Mesh] | 12,056 |
| 4 | “hyperbaric oxygen*”[Title/Abstract] OR HBO2[Title/Abstract] OR HBO[Title/Abstract] | 12,164 |
| 3 | #1 OR #2 | 729,572 |
| 2 | “Diabetes Mellitus”[Mesh] | 440,904 |
| 1 | diabetes[Title/Abstract] OR diabetic*[Title/Abstract] | 669,965 |
| # | Query | Results |
|---|---|---|
| S17 | S15 AND S16 | 113 |
| S16 | S3 AND S6 | 919 |
| S15 | S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 | 597,728 |
| S14 | (MH “Hypoglycemia+”) | 28,914 |
| S13 | TI (hypoglycaemia OR hypoglycemia OR hypoglycaemic OR hypoglycemic) OR AB (hypoglycaemia OR hypoglycemia OR hypoglycaemic OR hypoglycemic) | 58,437 |
| S12 | (MH “Hyperglycemia+”) | 37,174 |
| S11 | TI (hyperglycaemia OR hyperglycemia OR hyperglycaemic OR hyperglycemic) OR AB (hyperglycaemia OR hyperglycemia OR hyperglycaemic OR hyperglycemic) | 63,950 |
| S10 | (MH “Glycemic Control”) | 257 |
| S9 | TI (glycemic OR glycaemic) OR AB (glycemic OR glycaemic) | 50,265 |
| S8 | (MH “Blood Glucose”) | 167,965 |
| S7 | TI (“blood sugar” OR glucose) OR AB (“blood sugar” OR glucose) | 473,206 |
| S6 | S4 OR S5 | 15,885 |
| S5 | (MH “Hyperbaric Oxygenation”) | 12,048 |
| S4 | TI (“hyperbaric oxygen*” OR HBO2 OR HBO) OR AB (“hyperbaric oxygen*” OR HBO2 OR HBO) | 11,723 |
| S3 | S1 OR S2 | 727,311 |
| S2 | (MH “Diabetes Mellitus+”) | 439,985 |
| S1 | TI (diabetes OR diabetic*) OR AB (diabetes OR diabetic*) | 663,799 |
| # | Query | Results |
|---|---|---|
| 17 | 15 and 16 | 199 |
| 16 | 3 and 6 | 1303 |
| 15 | 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 | 864,384 |
| 14 | exp hypoglycemia/ | 82,561 |
| 13 | (hypoglycaemia or hypoglycemia or hypoglycaemic or hypoglycemic).ti. or (hypoglycaemia or hypoglycemia or hypoglycaemic or hypoglycemic).ab. | 86,203 |
| 12 | exp hyperglycemia/ | 101,038 |
| 11 | (hyperglycaemia or hyperglycemia or hyperglycaemic or hyperglycemic).ti. or (hyperglycaemia or hyperglycemia or hyperglycaemic or hyperglycemic).ab. | 94,423 |
| 10 | exp glycemic control/ | 53,870 |
| 9 | (glycemic or glycaemic).ti. or (glycemic or glycaemic).ab. | 81,559 |
| 8 | exp glucose blood level/ | 260,424 |
| 7 | ((blood adj1 sugar) or glucose).ti. or ((blood adj1 sugar) or glucose).ab. | 658,030 |
| 6 | 4 or 5 | 14,749 |
| 5 | exp hyperbaric oxygen/ or exp hyperbaric oxygen therapy/ | 3230 |
| 4 | ((hyperbaric adj1 oxygen*) or HBO2 or HBO).ti. or ((hyperbaric adj1 oxygen*) or HBO2 or HBO).ab. | 13,775 |
| 3 | 1 or 2 | 1,195,748 |
| 2 | exp diabetes mellitus/ | 1,014,391 |
| 1 | (diabetes or diabetic*).ti. or (diabetes or diabetic*).ab. | 995,738 |
References
- Mathieu, D.; Marroni, A.; Kot, J. Tenth European Consensus Conference on Hyperbaric Medicine: Recommendations for accepted and non-accepted clinical indications and practice of hyperbaric oxygen treatment. Diving Hyperb. Med. J. 2017, 47, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Kaya, A.; Aydin, F.; Altay, T.; Karapinar, L.; Ozturk, H.; Karakuzu, C. Can major amputation rates be decreased in diabetic foot ulcers with hyperbaric oxygen therapy? Int. Orthop. 2008, 33, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duzgun, A.P.; Satır, H.Z.; Ozozan, O.; Saylam, B.; Kulah, B.; Coskun, F. Effect of Hyperbaric Oxygen Therapy on Healing of Diabetic Foot Ulcers. J. Foot Ankle Surg. 2008, 47, 515–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flood, M. Hyperbaric oxygen therapy for diabetic foot ulcers. J. Lanc. Gen. Hosp. 2007, 2, 140–145. [Google Scholar]
- Bhutani, S.; Vishwanath, G. Hyperbaric oxygen and wound healing. Indian J. Plast. Surg. 2012, 45, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Skyler, J.S. Effects of Glycemic Control on Diabetes Complications and on the Prevention of Diabetes. Clin. Diabetes 2004, 22, 162–166. [Google Scholar] [CrossRef] [Green Version]
- Ketema, E.B.; Kibret, K.T. Correlation of fasting and postprandial plasma glucose with HbA1c in assessing glycemic control; systematic review and meta-analysis. Arch. Public Health 2015, 73, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heyboer III, M.; Wojcik, S.M.; Swaby, J.; Boes, T. Blood glucose levels in diabetic patients undergoing hyperbaric oxygen therapy. Undersea Hyperb. Med. 2019, 46, 437–445. [Google Scholar]
- Trytko, B.; Bennett, M.H. Blood sugar changes in diabetic patients undergoing hyperbaric oxygen therapy. South Pac. Underw. Med. Soc. J. 2003, 33, 62–69. [Google Scholar]
- Vote, D.; Ekanayake, L.; Doolette, D. Blood sugar levels and hyperbaric oxygen. South Pac. Underw. Med. Soc. J. 2001, 31, 81–82. [Google Scholar]
- Peleg, R.K.; Fishlev, G.; Bechor, Y.; Bergan, J.; Friedman, M.; Koren, S.; Tirosh, A.; Efrati, S. Effects of hyperbaric oxygen on blood glucose levels in patients with diabetes mellitus, stroke or traumatic brain injury and healthy volunteers: A prospective, crossover, controlled trial. Diving Hyperb. Med. J. 2013, 43, 218–221. [Google Scholar]
- Ekanayake, L.; Doolette, D. Effects of hyperbaric oxygen treatment on blood sugar levels and insulin levels in diabetics. South Pac. Underw. Med. Soc. J. 2001, 31, 16–20. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Irawan, H.; Semadi, I.N.; Widiana, I.G.R. A Pilot Study of Short-Duration Hyperbaric Oxygen Therapy to Improve HbA1c, Leukocyte, and Serum Creatinine in Patients with Diabetic Foot Ulcer Wagner 3–4. Sci. World J. 2018, 2018, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Xu, Q.; Wei, Y.-T.; Fan, S.-B.; Wang, L.; Zhou, X.-P. Repetitive hyperbaric oxygen treatment increases insulin sensitivity in diabetes patients with acute intracerebral hemorrhage. Neuropsychiatr. Dis. Treat. 2017, 13, 421–426. [Google Scholar] [CrossRef]
- Vera-Cruz, P.; Guerreiro, F.; Ribeiro, M.J.; Guarino, M.P.; Conde, S.V. Hyperbaric Oxygen Therapy Improves Glucose Homeostasis in Type 2 Diabetes Patients: A Likely Involvement of the Carotid Bodies. Adv. Exp. Med. Biol. 2015, 860, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.L.; Narr, A.J.; Claus, P.L.; Millman, M.P.; Steinkraus, L.W.; Shields, R.C.; Buchta, W.G.; Haddon, R.; Wang, Z.; Murad, M.H. The incidence of hypoglycemia during HBO2 therapy: A retrospective review. Undersea Hyperb. Med. 2015, 42, 191–196. [Google Scholar] [PubMed]
- Wilkinson, D.; Chapman, I.M.; Heilbronn, L.K. Hyperbaric oxygen therapy improves peripheral insulin sensitivity in humans. Diabet. Med. 2012, 29, 986–989. [Google Scholar] [CrossRef] [PubMed]
- Al-Waili, N.S.; Butler, G.J.; Beale, J.; Abdullah, M.S.; Finkelstein, M.; Merrow, M.; Rivera, R.; Petrillo, R.; Carrey, Z.; Lee, B.; et al. Influences of Hyperbaric Oxygen on Blood Pressure, Heart Rate and Blood Glucose Levels in Patients with Diabetes Mellitus and Hypertension. Arch. Med. Res. 2006, 37, 991–997. [Google Scholar] [CrossRef] [PubMed]

| Study Design | Number of Studies | Percentage of Studies (%) |
|---|---|---|
| Prospective cohort | 7 | 70 |
| Randomised placebo-controlled trial | 1 | 10 |
| Retrospective analysis | 2 | 20 |
| Study Location | Number of Studies |
|---|---|
| United States | 3 |
| Australia | 3 |
| China | 1 |
| Indonesia | 1 |
| Israel | 1 |
| Portugal | 1 |
| Data Collection | Study Design | Study Location | Sample Size | Sub-Population | Length of HBOT | Controls | Statistically Significant Outcomes | Other Notable Outcomes | |
|---|---|---|---|---|---|---|---|---|---|
| Heyboer et al.2019 [8] | Single Centre | Retrospective analysis | United States | 77 patients | Patients with diabetes mellitus undergoing HBOT for various indications | Median 19 sessions (IQR = 31) | None | Statistically significant greater percentage of treatments of patients with T2DM resulted in a decrease in blood glucose levels (77.5%) vs. T1DM (p < 0.001) | Blood glucose decreased in 75.4% of treatments in this group with a median decrease of 25 mg/dL (IQR = 54 mg/dL) |
| Irawan et al. 2018 [14] | Single Centre | Prospective cohort study | Indonesia | 15 patients | Patients with diabetes mellitus and diabetic foot ulcers | 10 sessions | No HBOT | Significant decrease in HbA1c after 10 session from 10.98 ± 2.37 % to 9.70 ± 2.46 % (p = 0.006) | None |
| Xu et al. 2017 [15] | Single Centre | Randomised, prospective, placebo controlled | China | 23 patients | Patients with T2DM suffering from intracerebral haemorrhage | 30 sessions | Normobaric oxygen therapy | A significant increase in insulin sensitivity during the HBOT sessions after 30 sessions (p < 0.05). Significant decreases in insulin, fasting glucose (11.3 ± 1.5 vs. 9.6 ± 1.1 mmol/L), and HbA1c (9.2 ± 1.6 vs. 7.8 ± 1.3%) in the HBOT group after 30 sessions (p < 0.05) | No change in insulin sensitivity, fasting plasma glucose of HbA1c in normobaric conditions. |
| Vera-Cruz et al. 2015 [16] | Single Centre | Prospective cohort study | Portugal | 16 patients | Patients with T2DM and indications for HBOT | 20 sessions | Patients without T2DM | Glycaemia measured following OGTT significantly decreased from 280.25 ± 22.29 mg/dL to 185.78 ± 11.70 mg/dL after 20 sessions of HBOT in patients with T2DM | HBOT decreased fasting plasma glucose levels to 119.1 ± 4.80 mg/dL in patients with T2DM, however without reaching statistical significance (p = 0.089) |
| Stevens et al. 2015 [17] | Single Centre | Retrospective analysis | United States | 190 patients | Patients with diabetes mellitus receiving HBOT for various indications | 1 session | None | None relevant | In-chamber glucose was higher than pre-HBOT glucose in 1708 of the 3136 HBOT sessions (54%) |
| Peleg et al. 2013 [11] | Single Centre | Prospective cohort crossover study | Israel | 13 patients | Patients with insulin- and non-insulin-dependent diabetes mellitus with HBOT indicated for non-healing wound | 1 session | Room air conditions at sea level pressure13 patients with traumatic brain injury or stroke treatedfor neurological deficit13 healthy volunteers | The non-insulin dependent diabetes mellitus patients had a significant decrease in their blood glucose levels during both sessions; from 9.2 ± 3.0 mmol/L to 7.3 ± 3.0 mmol/L during HBOT and from 9.9 ± 2.9 to 7.8 ± 3.4 mmol/L (p = 0.004) during the control normobaric session | The insulin-dependent patients had no change in blood glucose either during HBOT (13.0 ± 4.0 mmol/L before to 13.2 ± 5.7 mmol/L after, p = 0.88) or during the control session (13.15 ± 2.7 before to 13.2 ± 4.7 mmol/L after, p = 0.96) |
| Wilkinson et al. 2012 [18] | Single Centre | Prospective cohort study | Australia | 5 patients | Obese patients with T2DM and indications for HBOT | 30 sessions | Non-obese individuals without T2DM | Peripheral insulin sensitivity was significantly increased by HBOT at 3 and 30 visits in patients with T2DM. (p = 0.008).HbA1c wassignificantly reduced only in subjects without diabetes (p< 0.05 | No significant change in HbA1c after 30 visits in patients with T2DM. No change in fasting plasma glucose and insulin after 30 visits |
| Al-Waili et al. 2006 [19] | Single Centre | Prospective cohort study | United States | 23 patients | Patients with diabetes mellitus and indications for HBOT | 15–30 sessions | None | HBOT caused a significant dropin mean blood glucose approximately to the same extent in patients with diabetes mellitus alone or in patients with both diabetes mellitus and hypertension | Significant drop in blood glucose in 12 patients without HTN, and diabetes mellitus. |
| Trytko & Bennet. 2003 [9] | Single Centre | Prospective cohort study | Australia | 27 patients | Patients over 18 years old with diabetes mellitus and indications for HBOT | Up to 10 consecutive sessions | None | Mean reduction in blood glucose for each individual following HBOT of 2.04 (p < 0.0001) | T2DM were 102 of the recorded sessions and 80 of these had a reduction in blood glucose. Mean blood glucose reduction following HBOT did not significantly alter with treatment number during the course. In 17/23 patients who completed 10 sessions, there was a small and non-significant reduction in the mean HbA1c by 0.22% (p = 0.06) |
| Ekanayake & Doolette. 2001 [12] | Single Centre | Prospective cohort crossover study | Australia | 5 patients | Patients with diabetes mellitus of >6 years duration and indications for HBOT | 1 session | Normobaric air conditions 5 patients without diabetes mellitus | Decline in glucose levels in both HBOT and normobaric conditions in patients with diabetes mellitus. Decline only reaches significance between time points after 45 min in HBOT | No change in serum insulin levels under any condition |
| Year | Study Reference | Impact on Fasting Blood Glucose | Change in Insulin Levels | Peripheral Insulin Sensitivity | Impact on OGTT 2-h Glucose Level | HbA1c Change |
|---|---|---|---|---|---|---|
| 2019 | Heyboer et al. [8] | Decrease * | NA | NA | NA | NA |
| 2018 | Irawan et al. [14] | NA | NA | NA | NA | Decrease * |
| 2017 | Xu et al. [15] | Decrease * | Decrease * | Increased * | NA | Decrease * |
| 2015 | Vera-Cruz et al. [16] | Decrease | NA | NA | Decrease * | NA |
| 2015 | Stevens et al. [17] | Increase † | NA | NA | NA | NA |
| 2013 | Peleg et al. [11] | Decrease * | NA | NA | NA | NA |
| 2012 | Wilkinson et al. [18] | No change | No change | Increased * | NA | No change |
| 2006 | Al-Waili et al. [19] | Decrease * | NA | NA | NA | NA |
| 2003 | Trytko & Bennet. [9] | Decrease * | NA | NA | NA | Decrease |
| 2001 | Ekanayake & Doolette. [12] | Decrease * | No change | NA | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baitule, S.; Patel, A.H.; Murthy, N.; Sankar, S.; Kyrou, I.; Ali, A.; Randeva, H.S.; Robbins, T. A Systematic Review to Assess the Impact of Hyperbaric Oxygen Therapy on Glycaemia in People with Diabetes Mellitus. Medicina 2021, 57, 1134. https://doi.org/10.3390/medicina57101134
Baitule S, Patel AH, Murthy N, Sankar S, Kyrou I, Ali A, Randeva HS, Robbins T. A Systematic Review to Assess the Impact of Hyperbaric Oxygen Therapy on Glycaemia in People with Diabetes Mellitus. Medicina. 2021; 57(10):1134. https://doi.org/10.3390/medicina57101134
Chicago/Turabian StyleBaitule, Sudhanshu, Aaran H. Patel, Narasimha Murthy, Sailesh Sankar, Ioannis Kyrou, Asad Ali, Harpal S. Randeva, and Tim Robbins. 2021. "A Systematic Review to Assess the Impact of Hyperbaric Oxygen Therapy on Glycaemia in People with Diabetes Mellitus" Medicina 57, no. 10: 1134. https://doi.org/10.3390/medicina57101134
APA StyleBaitule, S., Patel, A. H., Murthy, N., Sankar, S., Kyrou, I., Ali, A., Randeva, H. S., & Robbins, T. (2021). A Systematic Review to Assess the Impact of Hyperbaric Oxygen Therapy on Glycaemia in People with Diabetes Mellitus. Medicina, 57(10), 1134. https://doi.org/10.3390/medicina57101134