
Long Term Clinical–Functional and Ultrasound Outcomes in Recreational Athletes after Achilles Tendon Rupture: Ma and Griffith versus Tenolig

 ,
, 
 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Inclusion and Exclusion Criteria
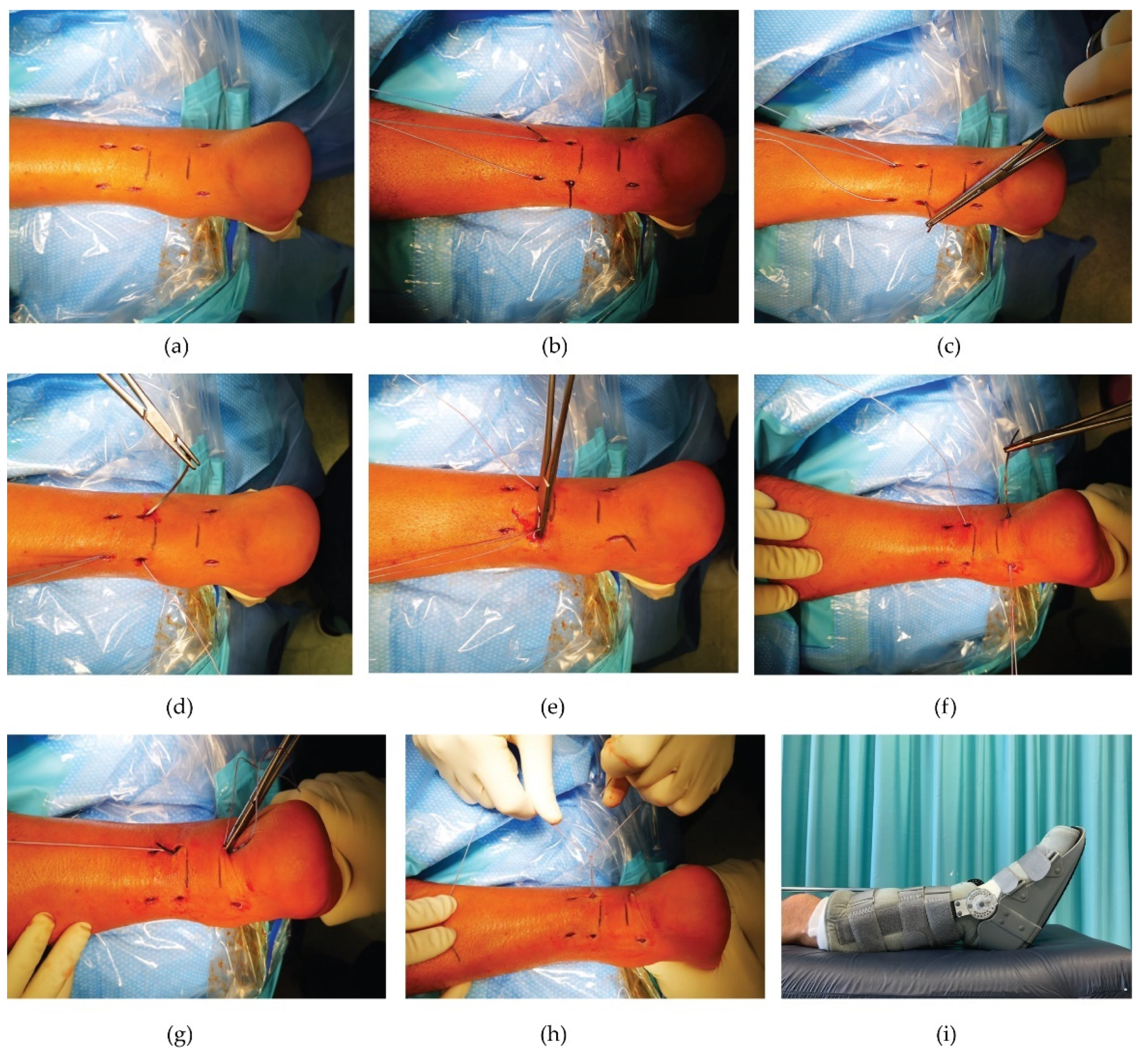
2.3. Surgical Percutaneous Techniques
2.3.1. Ma and Griffith Technique (M&G)
2.3.2. Tenolig Technique (TT)
2.4. Post-Operative Protocol of Both Procedures
2.5. Patient Assessment
2.6. Clinical and Functional Outcome Measures
2.7. Ultrasound Outcome Measures
2.8. Complications
2.9. Statistical Analysis
3. Results
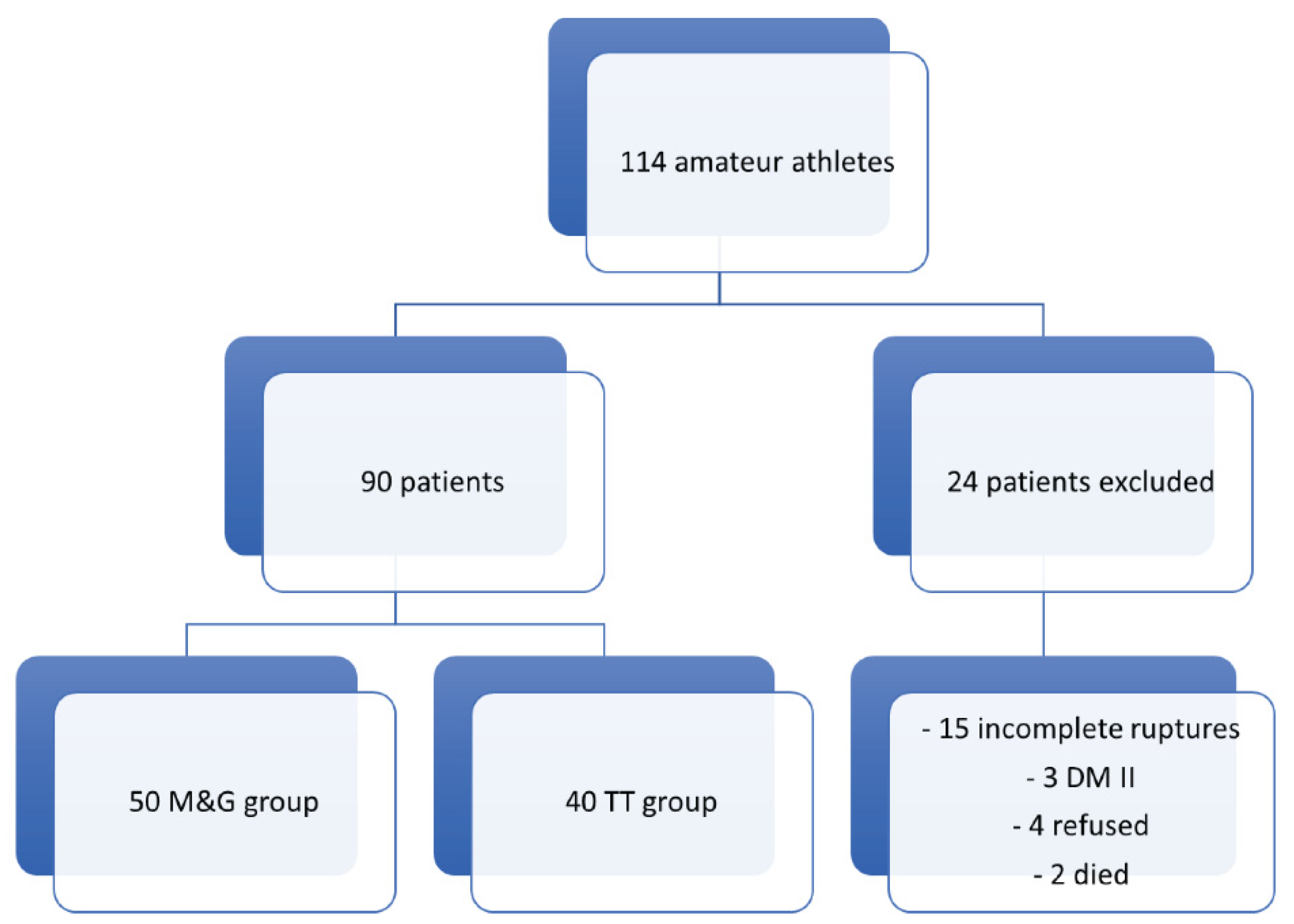
3.1. Patient Data
3.2. Demographic, Clinical, and Functional Outcomes between M&G and T Group
3.3. Ultrasound Outcomes between M&G and T Group
3.4. Complications
3.5. Multivariate Logistic Regression Analysis
4. Discussion
Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gross, C.E.; Nunley, J.A. Acute Achilles Tendon Ruptures. Foot Ankle Int. 2015, 37, 233–239. [Google Scholar] [CrossRef]
- Pedowitz, D.; Kirwan, G. Achilles tendon ruptures. Curr. Rev. Musculoskelet. Med. 2013, 6, 285–293. [Google Scholar] [CrossRef] [Green Version]
- Movin, T.; Ryberg, Å.; McBride, D.J.; Maffulli, N. Acute Rupture of the Achilles Tendon. Foot Ankle Clin. 2005, 10, 331–356. [Google Scholar] [CrossRef]
- Raikin, S.M.; Garras, D.N.; Krapchev, P.V. Achilles tendon injuries in a United States population. Foot Ankle Int. 2013, 34, 475–480. [Google Scholar] [CrossRef]
- Park, S.-H.; Lee, H.S.; Young, K.W.; Seo, S.G. Treatment of Acute Achilles Tendon Rupture. Clin. Orthop. Surg. 2020, 12, 1–8. [Google Scholar] [CrossRef]
- Huttunen, T.T.; Kannus, P.; Rolf, C.; Felländer-Tsai, L.; Mattila, V.M. Acute achilles tendon ruptures: Incidence of injury and surgery in Sweden between 2001 and 2012. Am. J. Sports Med. 2014, 42, 2419–2423. [Google Scholar] [CrossRef] [PubMed]
- Lerch, T.D.; Schwinghammer, A.; Schmaranzer, F.; Anwander, H.; Ecker, T.M.; Schmid, T.; Weber, M.; Krause, F. Return to Sport and Patient Satisfaction at 5-Year Follow-up After Nonoperative Treatment for Acute Achilles Tendon Rupture. Foot Ankle Int. 2020, 41, 784–792. [Google Scholar] [CrossRef]
- Thevendran, G.; Sarraf, K.M.; Patel, N.K.; Sadri, A.; Rosenfeld, P. The ruptured Achilles tendon: A current overview from biology of rupture to treatment. Musculoskelet. Surg. 2013, 97, 9–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiodo, C.P.; Wilson, M.G. Current Concepts Review: Acute Ruptures of the Achilles Tendon. Foot Ankle Int. 2006, 27, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Longo, U.G.; Kadakia, A.; Spiezia, F. Achilles tendinopathy. Foot Ankle Surg. 2020, 26, 240–249. [Google Scholar] [CrossRef]
- Singh, D. Acute Achilles tendon rupture. Br. J. Sports Med. 2017, 51, 1158–1160. [Google Scholar] [CrossRef] [PubMed]
- Romero-Morales, C.; Bravo-Aguilar, M.; Ruiz-Ruiz, B.; Almazán-Polo, J.; López-López, D.; Blanco-Morales, M.; Téllez-González, P.; Calvo-Lobo, C. Current advances and research in ultrasound imaging to the assessment and management of musculoskeletal disorders. Disease-a-Month 2021, 67, 101050. [Google Scholar] [CrossRef] [PubMed]
- Romero-Morales, C.; Martín-Llantino, P.J.; Calvo-Lobo, C.; Almazán-Polo, J.; López-López, D.; de la Cruz-Torres, B.; Palomo-López, P.; Rodríguez-Sanz, D. Intrinsic foot muscles morphological modifications in patients with Achilles’ tendinopathy: A novel case-control research study. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2019, 40, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Romero-Morales, C.; Martín-Llantino, P.J.; Calvo-Lobo, C.; Palomo-López, P.; López-López, D.; Pareja-Galeano, H.; Rodríguez-Sanz, D. Comparison of the sonographic features of the Achilles Tendon complex in patients with and without achilles tendinopathy: A case-control study. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2019, 35, 122–126. [Google Scholar] [CrossRef]
- Deng, S.; Sun, Z.; Zhang, C.; Chen, G.; Li, J. Surgical Treatment Versus Conservative Management for Acute Achilles Tendon Rupture: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2017, 56, 1236–1243. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Lin, L.; Li, H.; Zhao, Y.; Liu, L.; Jia, Z.; Wang, D.; He, Q.; Ruan, D. Is surgical intervention more effective than non-surgical treatment for acute Achilles’ tendon rupture? A systematic review of overlapping meta-analyses. Int. J. Surg. 2016, 36, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, D.; Palermi, S.; Sirico, F.; Corrado, B. Achilles Tendon Rupture: Mechanisms of Injury, Principles of Rehabilitation and Return to Play. J. Funct. Morphol. Kinesiol. 2020, 5, 95. [Google Scholar] [CrossRef]
- Oliva, F.; Bernardi, G.; De Luna, V.; Farsetti, P.; Gasparini, M.; Marsilio, E.; Piccirilli, E.; Tarantino, U.; Rugiero, C.; De Carli, A. IS Mu. LT Achilles tendon ruptures guidelines. Muscles Ligaments Tendons J. 2018, 8, 310–363. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Meng, H.; Quan, Q.; Peng, J.; Lu, S.; Wang, A. Management of acute Achilles’ tendon ruptures: A review. Bone Jt. Res. 2018, 7, 561–569. [Google Scholar] [CrossRef]
- Stavrou, M.; Seraphim, A.; Al-Hadithy, N.; Mordecai, S.C. Review article: Treatment for Achilles tendon ruptures in athletes. J. Orthop. Surg. 2013, 21, 232–235. [Google Scholar] [CrossRef]
- Khan, R.J.; Fick, D.; Brammar, T.J.; Crawford, J.; Parker, M.J. Interventions for treating acute Achilles’ tendon ruptures. Cochrane Database Syst. Rev. 2004, 3, CD003674. [Google Scholar] [CrossRef]
- Ma, G.W.; Griffith, T.G. Percutaneous repair of acute closed ruptured achilles tendon: A new technique. Clin. Orthop. Relat. Res. 1977, 128, 247–255. [Google Scholar] [CrossRef]
- Carmont, M.R.; Maffulli, N. Modified percutaneous repair of ruptured Achilles’ tendon. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2008, 16, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; D'Addona, A.; Maffulli, G.D.; Gougoulias, N.; Oliva, F. Delayed (14–30 Days) Percutaneous Repair of Achilles Tendon Ruptures Offers Equally Good Results as Compared with Acute Repair. Am. J. Sports Med. 2020, 48, 1181–1188. [Google Scholar] [CrossRef]
- Lacoste, S.; Féron, J.M.; Cherrier, B. Percutaneous Tenolig (®) repair under intra-operative ultrasonography guidance in acute Achilles’ tendon rupture. Orthop. Traumatol. Surg. Res. 2014, 100, 925–930. [Google Scholar] [CrossRef] [Green Version]
- Zellers, J.A.; Carmont, M.R.; Grävare Silbernagel, K. Return to play post-Achilles’ tendon rupture: A systematic review and meta-analysis of rate and measures of return to play. Br. J. Sports Med. 2016, 50, 1325–1332. [Google Scholar] [CrossRef]
- Taglialavoro, G.; Biz, C.; Mastrangelo, G.; Aldegheri, R. The repair of the Achilles tendon rupture: Comparison of two percutaneous techniques. Strateg. Trauma Limb Reconstr. 2011, 6, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Padulo, J.; Oliva, F.; Frizziero, A.; Maffulli, N. Muscles, Ligaments and Tendons Journal-Basic principles and recommendations in clinical and field Science Research: 2016 Update. Muscles Ligaments Tendons J. 2016, 6, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Matles, A.L. Rupture of the tendo achilles: Another diagnostic sign. Bull. Hosp. Jt. Dis. 1975, 36, 48–51. [Google Scholar]
- Maffulli, N. The clinical diagnosis of subcutaneous tear of the Achilles tendon. A prospective study in 174 patients. Am. J. Sports Med. 1998, 26, 266–270. [Google Scholar] [CrossRef]
- Thompson, T.C.; Doherty, J.H. Spontaneous rupture of tendon of Achilles: A new clinical diagnostic test. J. Trauma 1962, 2, 126–129. [Google Scholar] [CrossRef]
- van Sterkenburg, M.N.; van Dijk, C.N. Mid-portion Achilles’ tendinopathy: Why painful? An evidence-based philosophy. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1367–1375. [Google Scholar] [CrossRef] [Green Version]
- Bressel, E.; Larsen, B.T.; McNair, P.J.; Cronin, J. Ankle joint proprioception and passive mechanical properties of the calf muscles after an Achilles tendon rupture: A comparison with matched controls. Clin. Biomech. 2004, 19, 284–291. [Google Scholar] [CrossRef]
- Nilsson-Helander, K.; Thomeé, R.; Grävare-Silbernagel, K.; Thomeé, P.; Faxén, E.; Eriksson, B.I.; Karlsson, J. The Achilles Tendon Total Rupture Score (ATRS): Development and Validation. Am. J. Sports Med. 2007, 35, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Vascellari, A.; Spennacchio, P.; Combi, A.; Grassi, A.; Patella, S.; Bisicchia, S.; Canata, G.L.; Zaffagnini, S. Cross-cultural adaptation and multi-centric validation of the Italian version of the Achilles tendon Total Rupture Score (ATRS). Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2018, 26, 854–861. [Google Scholar] [CrossRef]
- Cöster, M.C.; Rosengren, B.E.; Bremander, A.; Brudin, L.; Karlsson, M.K. Comparison of the self-reported foot and ankle score (SEFAS) and the American Orthopedic Foot and Ankle Society score (AOFAS). Foot Ankle Int. 2014, 35, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Leigheb, M.; Vaiuso, D.; Rava, E.; Pogliacomi, F.; Samaila, E.M.; Grassi, F.A.; Sabbatini, M. Translation, cross-cultural adaptation, reliability, and validation of the Italian version of the American Orthopaedic Foot and Ankle Society-MetaTarsoPhalangeal-InterPhalangeal Scale (AOFAS-MTP-IP) for the hallux. Acta BioMed. Atenei Parm. 2019, 90, 118–126. [Google Scholar] [CrossRef]
- Maffulli, N.; Via, A.G.; Oliva, F. Chronic Achilles Tendon Rupture. Open Orthop. J. 2017, 11, 660–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maffulli, N.; Peretti, G.M. Surgery or conservative management for Achilles’ tendon rupture? BMJ 2019, 364, k5344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metz, R.; Verleisdonk, E.J.; van der Heijden, G.J.; Clevers, G.J.; Hammacher, E.R.; Verhofstad, M.H.; van der Werken, C. Acute Achilles tendon rupture: Minimally invasive surgery versus nonoperative treatment with immediate full weightbearing--a randomized controlled trial. Am. J. Sports Med. 2008, 36, 1688–1694. [Google Scholar] [CrossRef] [PubMed]
- Hsu, A.R.; Jones, C.P.; Cohen, B.E.; Davis, W.H.; Ellington, J.K.; Anderson, R.B. Clinical Outcomes and Complications of Percutaneous Achilles Repair System Versus Open Technique for Acute Achilles Tendon Ruptures. Foot Ankle Int. 2015, 36, 1279–1286. [Google Scholar] [CrossRef] [PubMed]
- Idarraga, A.J.; Bohl, D.D.; Barnard, E.; Movassaghi, K.; Hamid, K.S.; Schiff, A.P. Adverse Events Following Minimally Invasive Achilles Tendon Repair. Foot Ankle Spec. 2020, 25, 1938640020950895. [Google Scholar] [CrossRef]
- Jackson, G.; Sinclair, V.F.; McLaughlin, C.; Barrie, J. Outcomes of functional weight-bearing rehabilitation of Achilles tendon ruptures. Orthopedics 2013, 36, e1053–e1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bleakney, R.R.; Tallon, C.; Wong, J.K.; Lim, K.P.; Maffulli, N. Long-term ultrasonographic features of the Achilles tendon after rupture. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2002, 12, 273–278. [Google Scholar] [CrossRef]
- Brorsson, A.; Grävare Silbernagel, K.; Olsson, N.; Nilsson Helander, K. Calf Muscle Performance Deficits Remain 7 Years After an Achilles Tendon Rupture. Am. J. Sports Med. 2018, 46, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.S.; Lees, D.; Gwynne-Jones, D.P. Functional Outcome of Acute Achilles Tendon Rupture with and Without Operative Treatment Using Identical Functional Bracing Protocol. Foot Ankle Int. 2017, 38, 1331–1336. [Google Scholar] [CrossRef] [PubMed]
- Karabinas, P.K.; Benetos, I.S.; Lampropoulou-Adamidou, K.; Romoudis, P.; Mavrogenis, A.F.; Vlamis, J. Percutaneous versus open repair of acute Achilles’ tendon ruptures. Eur. J. Orthop. Surg. Traumatol. Orthop. Traumatol. 2014, 24, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Rouvillain, J.L.; Navarre, T.; Labrada-Blanco, O.; Garron, E.; Daoud, W. Percutaneous suture of acute Achilles’ tendon rupture. A study of 60 cases. Acta Orthop. Belg. 2010, 76, 237–242. [Google Scholar]
- Jallageas, R.; Bordes, J.; Daviet, J.C.; Mabit, C.; Coste, C. Evaluation of surgical treatment for ruptured Achilles’ tendon in 31 athletes. Orthop. Traumatol. Surg. Res. OTSR 2013, 99, 577–584. [Google Scholar] [CrossRef]
- Zayni, R.; Coursier, R.; Zakaria, M.; Desrousseaux, J.F.; Cordonnier, D.; Polveche, G. Activity level recovery after acute Achilles’ tendon rupture surgically repaired: A series of 29 patients with a mean follow-up of 46 months. Muscles Ligaments Tendons J. 2017, 7, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassi, A.; Rossi, G.; D'Hooghe, P.; Aujla, R.; Mosca, M.; Samuelsson, K.; Zaffagnini, S. Eighty-two per cent of male professional football (soccer) players return to play at the previous level two seasons after Achilles’ tendon rupture treated with surgical repair. Br. J. Sports Med. 2020, 54, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Jack, R.A., 2nd; Sochacki, K.R.; Gardner, S.S.; McCulloch, P.C.; Lintner, D.M.; Cosculluela, P.E.; Varner, K.E.; Harris, J.D. Performance and Return to Sport After Achilles Tendon Repair in National Football League Players. Foot Ankle Int. 2017, 38, 1092–1099. [Google Scholar] [CrossRef] [PubMed]
- Zellers, J.A.; Cortes, D.H.; Pohlig, R.T.; Silbernagel, K.G. Tendon morphology and mechanical properties assessed by ultrasound show change early in recovery and potential prognostic ability for 6-month outcomes. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2019, 27, 2831–2839. [Google Scholar] [CrossRef]
- Yang, B.; Liu, Y.; Kan, S.; Zhang, D.; Xu, H.; Liu, F.; Ning, G.; Feng, S. Outcomes and complications of percutaneous versus open repair of acute Achilles’ tendon rupture: A meta-analysis. Int. J. Surg. 2017, 40, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Maes, R.; Copin, G.; Averous, C. Is percutaneous repair of the Achilles tendon a safe technique? A study of 124 cases. Acta Orthop. Belg. 2006, 72, 179–183. [Google Scholar]
- Maffulli, N.; Oliva, F.; Maffulli, G.D.; Buono, A.D.; Gougoulias, N. Surgical management of chronic Achilles’ tendon ruptures using less invasive techniques. Foot Ankle Surg. Off. J. Eur. Soc. Foot Ankle Surg. 2018, 24, 164–170. [Google Scholar] [CrossRef]
- Gigante, A.; Moschini, A.; Verdenelli, A.; Del Torto, M.; Ulisse, S.; de Palma, L. Open versus percutaneous repair in the treatment of acute Achilles’ tendon rupture: A randomized prospective study. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2008, 16, 204–209. [Google Scholar] [CrossRef]
- Liu, J.Y.; Duan, W.F.; Shen, S.; Ye, Y.; Sun, Y.Q.; He, W. Achillon versus modified minimally invasive repair treatment in acute Achilles’ tendon rupture. J. Orthop. Surg. 2020, 28, 2309499020908354. [Google Scholar] [CrossRef] [Green Version]
- Del Buono, A.; Volpin, A.; Maffulli, N. Minimally invasive versus open surgery for acute Achilles’ tendon rupture: A systematic review. Br. Med Bull. 2014, 109, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Liu, H.; Li, D.; Luo, Z.; Li, Y.; Zhang, F. Modified Bunnell suture repair versus bundle-to-bundle suture repair for acute Achilles’ tendon rupture: A prospective comparative study of patients aged <45 years. BMC Musculoskelet. Disord. 2020, 21, 580. [Google Scholar] [CrossRef]
- Longo, U.G.; Petrillo, S.; Maffulli, N.; Denaro, V. Acute achilles tendon rupture in athletes. Foot Ankle Clin. 2013, 18, 319–338. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Age (years), mean ± SD | 40.90 ± 7.59 |
| Gender, number (%) | |
| Male | 74 (82.2%) |
| Female | 16 (17.8%) |
| Affected Side, number (%) | |
| Right | 50 (55.6%) |
| Left | 40 (44.4%) |
| Tendinopathy | 15 (16.7%) |
| FKT (weeks), mean ± SD | 3.65 ± 1.80 |
| Follow-up (years), mean ± SD | 9.7 ± 2.4 |
| Satisfaction of intervention, mean ± SD | 7.46 ± 1.54 |
| Return to work (weeks), mean ± SD | 4.80 ± 2.64 |
| Return to sports and physical activity (weeks), mean ± SD | 28.84 ± 10.20 |
| Return to pre-injury physical activity, number (%) | |
| No | 9 (10.0%) |
| Partially | 29 (32.2%) |
| Yes | 52 (57.8%) |
| Heel rise test (operated side) | 14 (15.6%) |
| Heel rise test (healthy test) | 4 (4.4%) |
| ROM, mean ± SD | −2.21 ± 4.22 |
| VAS score, mean ± SD | 1.44 ± 0.75 |
| ATRS score, mean ± SD | 90.52 ± 3.53 |
| AOFAS score, mean ± SD | 90.61 ± 4.27 |
| Calf circumference difference (cm) | 2.89 ± 1.08 |
| Echographic diameter of operated tendon (mm) | 14.26 ± 1.78 |
| Echographic hypoechogenicity (operated side) | 47 (52.2%) |
| Echographic calcifications (operated side) | 18 (20.0%) |
| Echo-Doppler tendinitis | 49 (54.4%) |
| Echographic abnormal fibrillar architecture | 66 (73.3%) |
| Complications | 10 (11.1%) |
| Parameter | Intervention | p-Value | |
|---|---|---|---|
| M&G (50 patients) | TT (40 patients) | ||
| Age, mean ± SD | 39.68 ± 7.95 | 41.88 ± 7.22 | 0.172 |
| Gender, number (%) | 0.951 | ||
| Male | 41 (82.0%) | 33 (82.5%) | |
| Female | 9 (18.0%) | 7 (17.5%) | |
| Affected Side, number (%) | 0.345 | ||
| Right | 30 (60.0%) | 20 (50.0%) | |
| Left | 20 (40.0%) | 20 (50.0%) | |
| Tendinopathy | 11 (22.0%) | 4 (10.0%) | 0.121 |
| FKT (weeks), Mean ± SD | 3.88 ± 1.86 | 3.38 ± 1.72 | 0.193 |
| Satisfaction of intervention, mean ± SD | 7.08 ± 1.75 | 7.76 ± 1.29 | 0.035 |
| Return to work (weeks), mean ± SD | 5.03 ± 2.79 | 4.62 ± 2.52 | 0.472 |
| Return to sports and physical activity (weeks), mean ± SD | 32.30 ± 9.43 | 26.08 ± 10.03 | 0.003 |
| Return to pre-injury physical activity, number (%) | 0.918 | ||
| No | 5 (10.0%) | 4 (10.0%) | |
| Partially | 17 (34.0%) | 12 (30.0%) | |
| Yes | 28 (56.0%) | 24 (60.0%) | |
| Heel rise test (operated side) | 8 (16.0%) | 6 (15.0%) | 0.897 |
| Heel rise test (healthy test) | 2 (4.0%) | 2 (5.0%) | 0.820 |
| ROM, mean ± SD | −2.64 ± 4.23 | −1.68 ± 4.20 | 0.283 |
| VAS score, mean ± SD | 1.58 ± 0.75 | 1.34 ± 0.75 | 0.141 |
| ATRS score, mean ± SD | 90.70 ± 3.55 | 90.38 ± 3.54 | 0.671 |
| AOFAS score, mean ± SD | 91.03 ± 4.71 | 90.28 ± 3.90 | 0.414 |
| Calf circumference difference (cm) | 3.30 ± 1.02 | 2.40 ± 0.96 | <0.0001 |
| Complications | 5 (10.0%) | 5 (12.5%) | 0.709 |
| Parameter | Intervention | p-Value | |
|---|---|---|---|
| M&G (50 patients) | TT (40 patients) | ||
| Echographic diameter of operated tendon (mm) | 14.97 ± 1.90 | 13.39 ± 1.16 | <0.0001 |
| Echographic hypoechogenicity (operated side) | 28 (56.0%) | 19 (47.5%) | 0.425 |
| Presence of calcifications (operated side) | 11 (22.0%) | 7 (17.5%) | 0.598 |
| Echo-Doppler tendinitis | 32 (64.0%) | 17 (42.5%) | 0.043 |
| Echographic abnormal fibrillar architecture | 43 (86.0%) | 23 (57.5%) | 0.001 |
| Parameter | Regression Coefficient | Standard Error | Wald Coefficient | OR | 95%CI | p-Value |
|---|---|---|---|---|---|---|
| Return to sports/physical activity | 1.50 | 0.47 | 10.44 | 4.50 | 1.81−11.21 | 0.001 |
| Calf circumference difference | 1.24 | 0.47 | 7.07 | 3.45 | 1.39−8.61 | 0.008 |
| Echographic diameter of operated tendon | 1.32 | 0.45 | 8.56 | 3.75 | 1.55−9.09 | 0.003 |
| Echo-Doppler Tendinitis | −0.88 | 0.44 | 4.07 | 0.42 | 0.18−0.98 | 0.044 |
| Abnormal fibrillar architecture | −1.67 | 0.54 | 9.51 | 0.19 | 0.07−0.54 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biz, C.; Cerchiaro, M.; Belluzzi, E.; Bragazzi, N.L.; De Guttry, G.; Ruggieri, P. Long Term Clinical–Functional and Ultrasound Outcomes in Recreational Athletes after Achilles Tendon Rupture: Ma and Griffith versus Tenolig. Medicina 2021, 57, 1073. https://doi.org/10.3390/medicina57101073
Biz C, Cerchiaro M, Belluzzi E, Bragazzi NL, De Guttry G, Ruggieri P. Long Term Clinical–Functional and Ultrasound Outcomes in Recreational Athletes after Achilles Tendon Rupture: Ma and Griffith versus Tenolig. Medicina. 2021; 57(10):1073. https://doi.org/10.3390/medicina57101073
Chicago/Turabian StyleBiz, Carlo, Mariachiara Cerchiaro, Elisa Belluzzi, Nicola Luigi Bragazzi, Giacomo De Guttry, and Pietro Ruggieri. 2021. "Long Term Clinical–Functional and Ultrasound Outcomes in Recreational Athletes after Achilles Tendon Rupture: Ma and Griffith versus Tenolig" Medicina 57, no. 10: 1073. https://doi.org/10.3390/medicina57101073
APA StyleBiz, C., Cerchiaro, M., Belluzzi, E., Bragazzi, N. L., De Guttry, G., & Ruggieri, P. (2021). Long Term Clinical–Functional and Ultrasound Outcomes in Recreational Athletes after Achilles Tendon Rupture: Ma and Griffith versus Tenolig. Medicina, 57(10), 1073. https://doi.org/10.3390/medicina57101073