
Assessing Predictive Factors of COVID-19 Outcomes: A Retrospective Cohort Study in the Metropolitan Region of São Paulo (Brazil)

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics and Study Design
2.2. Patients and Primary Data Collection
2.3. Secondary Socioeconomic Data Extraction
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Johns Hopkins University & Medicine. COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Johns Hopkins Coronavirus Resour. Cent. 2020. Available online: https://coronavirus.jhu.edu/ (accessed on 27 July 2021).
- NCIRD. People with Certain Medical Conditions. Centers for Disease Control and Prevention. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 30 June 2021).
- Khalatbari-Soltani, S.; Cumming, R.C.; Delpierre, C.; Kelly-Irving, M. Importance of collecting data on socioeconomic determinants from the early stage of the COVID-19 outbreak onwards. J. Epidemiol. Community Health 2020, 74, 620–623. [Google Scholar] [CrossRef] [PubMed]
- Peres, I.T.; Bastos, L.S.L.; Gelli, J.G.M.; Marchesi, J.F.; Dantas, L.F.; Antunes, B.B.P.; Maçaira, P.M.; Baião, F.A.; Hamacher, S.; Bozza, F.A. Sociodemographic factors associated with COVID-19 in-hospital mortality in Brazil. Public Health 2021, 192, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Arcaya, M.C.; Arcaya, A.L.; Subramanian, S.V. Inequalities in health: Definitions, concepts, and theories. Glob. Health Action 2015, 8, 27106. [Google Scholar] [CrossRef] [PubMed]
- Lee, S. COVID-19 Amplifiers on Health Inequity Among the Older Populations. Front. Public Health 2021, 8, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Burstrom, B.; Tao, W. Social determinants of health and inequalities in COVID-19. Eur. J. Public Health 2020, 30, 617–618. [Google Scholar] [CrossRef]
- World Health Organization (WHO). A Conceptual Framework for Action on the Social Determinants of Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Fundação Sistema Estadual de Análise de Dados. Portal de Estatísticas do Estado de São Paulo. SEADE 2021. Available online: https://www.seade.gov.br/ (accessed on 25 May 2021).
- Fundação Sistema Estadual de Análise de Dados. Índice Paulista de Responsabilidade Social. SEADE 2019. Available online: http://www.iprs.seade.gov.br/ (accessed on 25 May 2021).
- Ministry of Health in Brazil. Portaria no 758, de 9 de Abril de 2020—Define o Procedimento para o Registro Obrigatório de Internações Hospitalares dos Casos Suspeitos e Confirmados de COVID-19, nos Estabelecimentos de Saúde Públicos e Privados que Prestam Serviços no SUS. Diário Oficial da União 2020; 9 abr. Available online: https://www.in.gov.br/en/web/dou/-/portaria-n-758-de-9-de-abril-de-2020-251970323 (accessed on 30 June 2021).
- Ministry of Health in Brazil. Guia de Vigilância Epidemiológica Emergência de Saúde Pública de Importância Nacional pela Doença pelo Coronavírus 2019-COVID-19. 2020. Available online: https://www.conasems.org.br/wp-content/uploads/2021/03/Guia-de-vigila%CC%82ncia-epidemiolo%CC%81gica-da-covid_19_15.03_2021.pdf (accessed on 20 June 2021).
- Ministry of Health in Brazil. Portaria no 1.792, de 17 de Julho de 2020. Altera a Portaria nº 356/GM/MS, de 11 de Março de 2020, para Dispor Sobre a Obrigatoriedade de Notificação ao Ministério da Saúde de Todos os Resultados de Testes Diagnóstico para SARS-CoV-2 Realizados por Laboratórios da Rede Pública, rede Privada, Universitários e Quaisquer Outros, em Todo Território Nacional. Diário Oficial da União 2020; 21 July. Available online: https://www.in.gov.br/en/web/dou/-/portaria-n-1.792-de-17-de-julho-de-2020-267730859 (accessed on 30 June 2021).
- Ministry of Health in Brazil. Estratégia e-SUS Atenção Primária. 2021. Available online: https://sisaps.saude.gov.br/esus/ (accessed on 26 May 2021).
- Barek, M.A.; Aziz, M.A.; Islam, M.S. Impact of age, sex, comorbidities and clinical symptoms on the severity of COVID-19 cases: A meta-analysis with 55 studies and 10014 cases. Heliyon 2020, 6, 1–24. [Google Scholar] [CrossRef]
- Organização Pan-Americana da Saúde. Folha Informativa Sobre COVID-19—OPAS 2021. Available online: https://www.paho.org/pt/covid19 (accessed on 27 May 2021).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Zheng, X.; Chen, J. Clinical progression and outcomes of 260 patients with severe COVID-19: An observational study. Sci. Rep. 2021, 11, 3166. [Google Scholar] [CrossRef]
- Pierce, C.A.; Preston-Hurlburt, P.; Dai, Y.; Aschner, C.B.; Cheshenko, N.; Galen, B.; Garforth, S.J.; Herrera, N.G.; Jangra, R.K.; Morano, N.C.; et al. Immune responses to SARS-CoV-2 infection in hospitalized pediatric and adult patients. Sci. Transl. Med. 2020, 12, eabd5487. [Google Scholar] [CrossRef]
- Dhochak, N.; Singhal, T.; Kabra, S.K.; Lodha, R. Pathophysiology of COVID-19: Why Children Fare Better than Adults? Indian J. Pediatr. 2020, 87, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Hospitalizations and Deaths of Younger People Soar due to COVID-19, PAHO Director Reports. PAHO/WHO 2021. Pan Am. Heal. Organ. Available online: https://www.paho.org/en/news/5-5-2021-hospitalizations-and-deaths-younger-people-soar-due-covid-19-paho-director-reports (accessed on 25 May 2021).
- Barreto, M.L.; Teixeira, M.G.; Bastos, F.I.P.M.; Ximenes, R.A.A.; Barata, R.C.B.; Rodrigues, L.C. Successes and failures in the control of infectious diseases in Brazil: Social and environmental context, policies, interventions, and research needs. Lancet 2011, 377, 1877–1889. [Google Scholar] [CrossRef]
- Estrela, F.M.; Soares, C.F.S.E.; da Cruz, M.A.; da Silva, A.F.; Santos, J.R.L.; Moreira, T.M.O.; Lima, A.B.; Silva, M.G. Covid-19 pandemic: Reflecting vulnerabilities in the light of gender, race and class. Cienc. Saude Colet. 2020, 25, 3431–3436. [Google Scholar] [CrossRef]
- Vilar-Compte, M.; Burrola-Méndez, S.; Lozano-Marrufo, A.; V Ferré-Eguiluz, I.; Flores, D.; Gaitán-Rossi, P.; Teruel, G.; Pérez-Escamilla, R. Urban poverty and nutrition challenges associated with accessibility to a healthy diet: A global systematic literature review. Int. J. Equity Health 2021, 20, 40. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Reed, A.B.; Ponzo, S.; Yasaee, A.; Aral, M.; Plans, D.; Labrinque, A.; Mohan, D. Population risk factors for severe disease and mortality in COVID-19: A global systematic review and meta-analysis. PLoS ONE 2021, 16, e0247461. [Google Scholar] [CrossRef]
- Ritter, A.; Kreis, N.N.; Louwen, F.; Yuan, J. Obesity and COVID-19: Molecular Mechanisms Linking Both Pandemics. Int. J. Mol. Sci. 2020, 21, 5793. [Google Scholar] [CrossRef]
- Corona, G.; Pizzocaro, A.; Vena, W.; Rastrelli, G.; Semeraro, F.; Isidori, A.M.; Pivonello, R.; Salonia, A.; Sforza, A.; Maggi, M. Diabetes is most important cause for mortality in COVID-19 hospitalized patients: Systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2021, 22, 275–296. [Google Scholar] [CrossRef]
- Lim, S.; Bae, J.H.; Kwon, H.S.; Nauck, M.A. COVID-19 and diabetes mellitus: From pathophysiology to clinical management. Nat. Rev. Endocrinol. 2021, 17, 11–30. [Google Scholar] [CrossRef]
- Knapp, S. Diabetes and Infection: Is There a Link? A Mini-Review. Gerontology 2013, 59, 99–104. [Google Scholar] [CrossRef]
- Codo, A.C.; Davanzo, G.G.; Monteiro, L.B.; de Souza, G.F.; Muraro, S.P.; Virgilio-da-Silva, J.V.; Prodonoff, J.S.; Carregari, V.C.; de Biagi, C.A.O., Jr.; Crunfli, F.; et al. Elevated Glucose Levels Favor SARS-CoV-2 Infection and Monocyte Response through a HIF-1α/Glycolysis-Dependent Axis. Cell Metab. 2020, 32, 437–446.e5, 498. [Google Scholar] [CrossRef]
- Sohrabi, M.R.; Amin, R.; Maher, A.; Bahadorimonfared, A.; Janbazi, S.; Hannani, K.; Kolahi, A.A.; Zali, A.R. Sociodemographic determinants and clinical risk factors associated with COVID-19 severity: A cross-sectional analysis of over 200,000 patients in Tehran, Iran. BMC Infect. Dis. 2021, 21, 474. [Google Scholar] [CrossRef]
- Gasmi, A.; Peana, M.; Pivina, L.; Srinath, S.; Benahmed, A.G.; Semenova, Y.; Menzel, A.; Dadar, M.; Bjørklund, G. Interrelations between COVID-19 and other disorders. Clin. Immunol. 2021, 224, 108651. [Google Scholar] [CrossRef]
- Malik, P.; Patel, U.; Patel, K.; Martin, M.; Shah, C.; Mehta, D.; Malik, F.A.; Sharma, A. Obesity a predictor of outcomes of COVID-19 hospitalized patients-A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 1188–1193. [Google Scholar] [CrossRef] [PubMed]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M. LICORN and the Lille COVID-19and Obesity study group. High Prevalence of Obesity in Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) Requiring InvasiveMechanical Ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef] [PubMed]
- Landecho, M.F.; Marin-Ot, M.; Recalde-Zamacona, B.; Bilbao, I.; Frühbeck, G. Obesity as an adipose tissue dysfunction disease and a risk factor for infections—Covid-19 as a case study. Eur. J. Intern. Med. 2021, 91, 3–9. [Google Scholar] [CrossRef]
- Gregor, M.F.; Hotamisligil, G.S. Inflammatory mechanisms in obesity. Annu. Rev. Immunol. 2011, 29, 415–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebello, C.J.; Kirwan, J.P.; Greenway, F.L. Obesity, the most common comorbidity in SARS-CoV-2: Is leptin the link? Int. J. Obes. 2020, 44, 1810–1817. [Google Scholar] [CrossRef]
- Brasil Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Análise em Saúde e Vigilância de Doenças Não Transmissíveis. Vigitel Brasil 2019: Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico: Estimativas Sobre Frequência e Distribuição Sociodemográfica de Fatores de Risco e Proteção para Doenças Crônicas nas Capitais dos 26 Estados Brasileiros e no Distrito Federal em 2019 [recurso eletrônico]/Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Análise em Saúde e Vigilância de Doenças não Transmissíveis.–Brasília: Ministério da Saúde. 2020. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/vigitel_brasil_2019_vigilancia_fatores_risco.pdf (accessed on 30 June 2021).


{kind=link}
| Secondary Data (n = 1036) | Death Outcome (n = 459) | Non-Death Outcome (n = 577) | |
|---|---|---|---|
| Individual data | |||
| Age (years) | mean (SD) | 69.02 (18.5) | 50.86 |
| range | 17–99 | 3–95 | |
| Hospitalization (yes) | % | 93.46 | 88.21 |
| Time between COVID-19 symptom onset and health care system admission | mean (SD) | 6.80 (6.20) | 7.79 (6.18) |
| Sociodemographic data | |||
| Schooling (>8 years) | % | 53.06 | 55.80 |
| Private health plan | % | 21.37 | 20.99 |
| Electricity | % | 99.08 | 99.03 |
| Water supply | % | 99.71 | 99.73 |
| Sewage network | % | 99.27 | 99.13 |
| Garbage collection | % | 99.92 | 99.91 |
| Income (up to 1 minimum wage) | % | 33.82 | 33.84 |
| Unemployment | % | 10.95 | 10.82 |
| Homeownership | % | 58.48 | 58.31 |
| Urban area | % | 99.37 | 99.38 |
| Primary Data (n = 515) | Death Outcome (n = 251) | Non-Death Outcome (n = 264) | |
| Individual data | |||
| Age (years) | mean (SD) | 69.59 (18.5) | 52.44 (17.94) |
| Range | 17–99 | 3–95 | |
| Schooling (>8 years) | % | 55.77 | 55.26 |
| Hospitalization (yes) | % | 93.23 | 88.26 |
| Time between COVID-19 symptom onset and health care system admission | mean (SD) | 6.38 (6.34) | 8.16 (6.33) |
| Diabetes | % | 40.64 | 23.1 |
| Hypertension | % | 50.77 | 36.36 |
| Obesity | % | 6.77 | 6.44 |
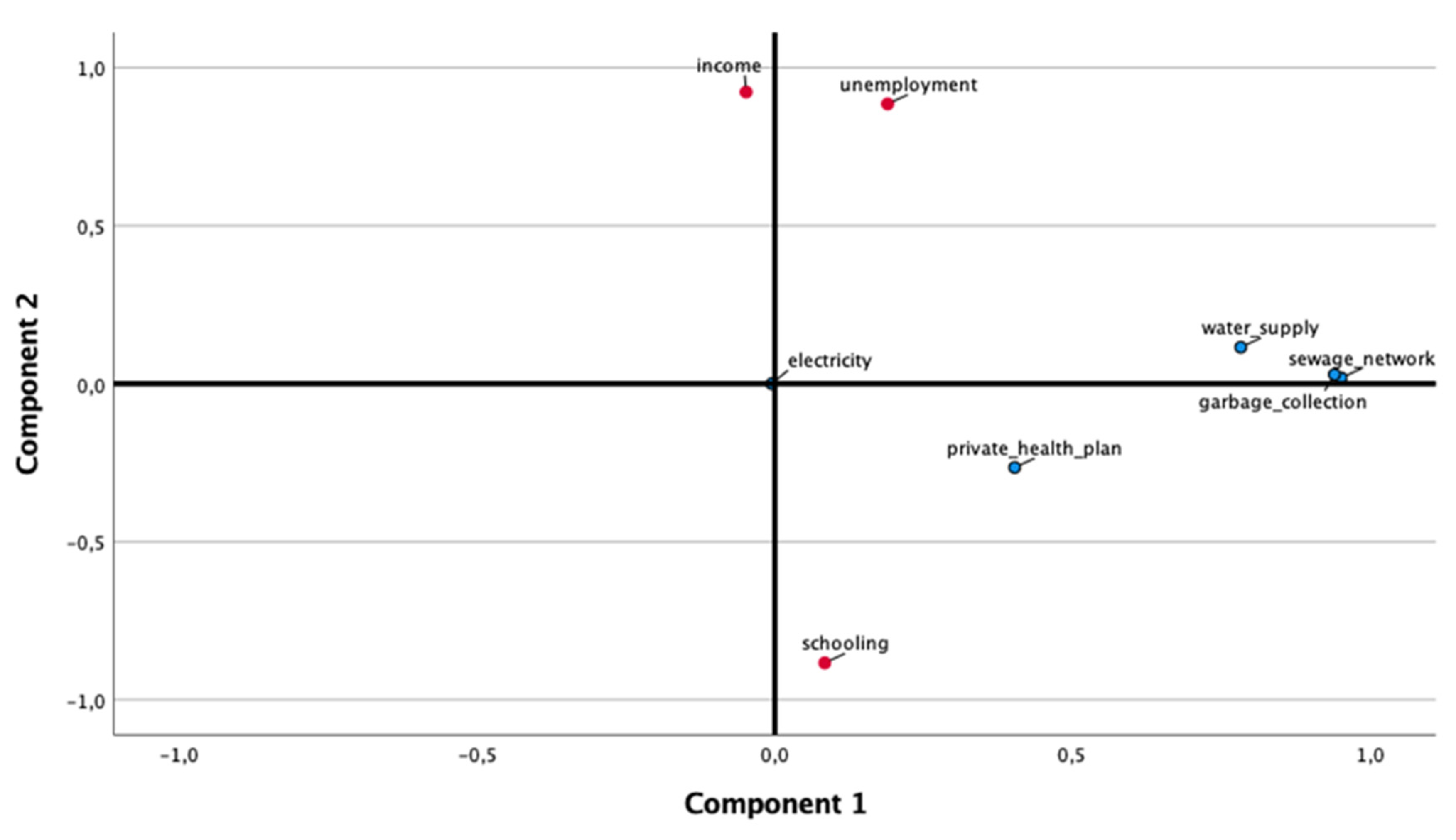
| Component | |||
|---|---|---|---|
| 1 | 2 | ||
| Environmental Aspects | Social Aspects | ||
| % | Variance explained | 34.9% | 28.8% |
| Schooling (>8 years) | −0.883 | ||
| Use of private health services | 0.403 | ||
| Electricity | |||
| Water supply | 0.783 | ||
| Sewage network | 0.952 | ||
| Garbage collection | 0.941 | ||
| Income (up to 1 minimum wage) | 0.923 | ||
| Unemployment | 0.885 | ||
| Independent Variable | B | Exp (B) | CI (95%) Exp (B) | Wald Chi-Square | p-Value |
|---|---|---|---|---|---|
| Intercept | 2.083 | 8.030 | 7.402–8.710 | 2518.81 | 0.000 |
| Age | −0.002 | 0.998 | 0.997–0.999 | 7.744 | 0.005 |
| Sex | 0.027 | 1.027 | 0.981–1.075 | 1.302 | 0.254 |
| Component 1 (environmental aspects) | −0.040 | 0.961 | 0.942–0.981 | 14.103 | 0.000 |
| Component 2 (social aspects) | −0.002 | 0.998 | 0.976–1.022 | 0.020 | 0.887 |
| Dependent Variable | Independent Variable | B | Exp (B) | CI (95%) Exp(B) | Wald Chi-Square | p-Value |
|---|---|---|---|---|---|---|
| Death outcome | Constant | −4.861 | - | - | 53.006 | 0.000 |
| Age | 0.076 | 1.079 | 1.057–1.101 | 55.319 | 0.000 | |
| Obesity | 1.060 | 2.885 | 1.092–7.620 | 4.573 | 0.032 | |
| Diabetes | 0.647 | 1.909 | 1.088–3.350 | 5.077 | 0.024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amato, J.N.; Castelo, P.M.; Cirino, F.M.S.B.; Meyer, G.; Pereira, L.J.; Sartori, L.C.; Aderaldo, N.S.; Silva, F.C.e. Assessing Predictive Factors of COVID-19 Outcomes: A Retrospective Cohort Study in the Metropolitan Region of São Paulo (Brazil). Medicina 2021, 57, 1068. https://doi.org/10.3390/medicina57101068
Amato JN, Castelo PM, Cirino FMSB, Meyer G, Pereira LJ, Sartori LC, Aderaldo NS, Silva FCe. Assessing Predictive Factors of COVID-19 Outcomes: A Retrospective Cohort Study in the Metropolitan Region of São Paulo (Brazil). Medicina. 2021; 57(10):1068. https://doi.org/10.3390/medicina57101068
Chicago/Turabian StyleAmato, Juliana Neide, Paula Midori Castelo, Ferla Maria Simas Bastos Cirino, Guilherme Meyer, Luciano José Pereira, Luís Cláudio Sartori, Natália Simões Aderaldo, and Fernando Capela e Silva. 2021. "Assessing Predictive Factors of COVID-19 Outcomes: A Retrospective Cohort Study in the Metropolitan Region of São Paulo (Brazil)" Medicina 57, no. 10: 1068. https://doi.org/10.3390/medicina57101068
APA StyleAmato, J. N., Castelo, P. M., Cirino, F. M. S. B., Meyer, G., Pereira, L. J., Sartori, L. C., Aderaldo, N. S., & Silva, F. C. e. (2021). Assessing Predictive Factors of COVID-19 Outcomes: A Retrospective Cohort Study in the Metropolitan Region of São Paulo (Brazil). Medicina, 57(10), 1068. https://doi.org/10.3390/medicina57101068