Incidence of Prostate Cancer in Inflammatory Bowel Disease: A Meta-Analysis


 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.2. Quality Assessment and Risk of Bias
3. Results
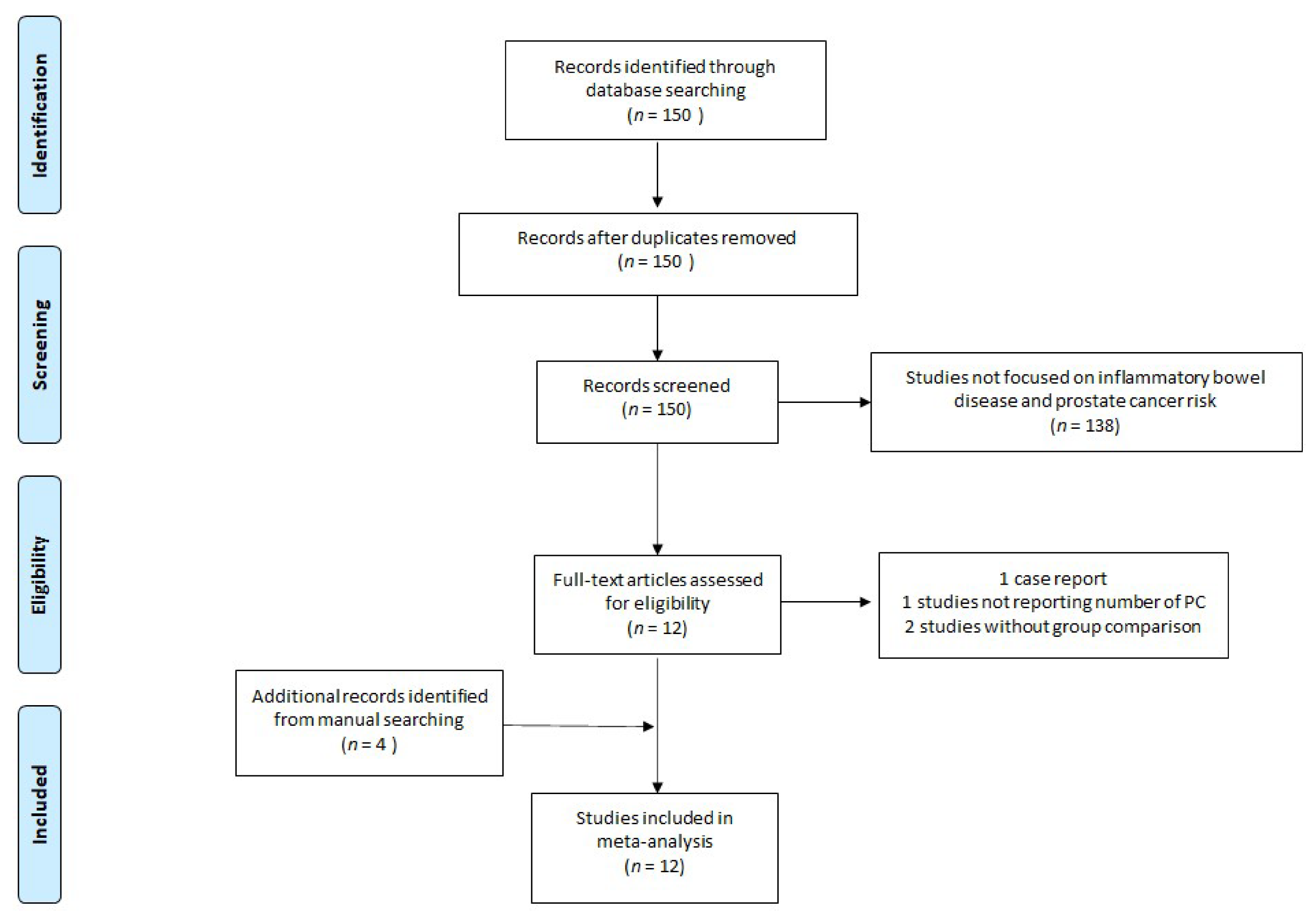
3.1. Studies Selected
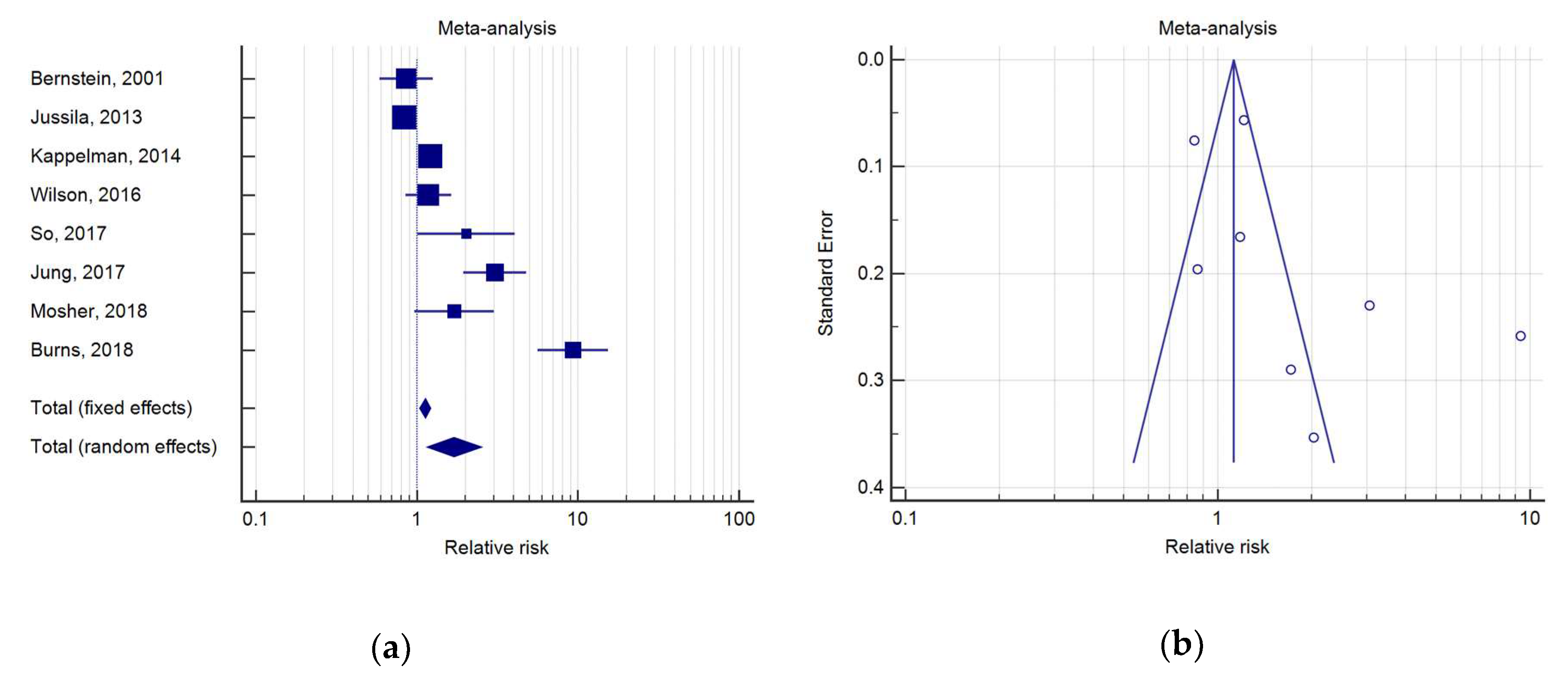
3.2. Prostate Cancer in IBD Patients
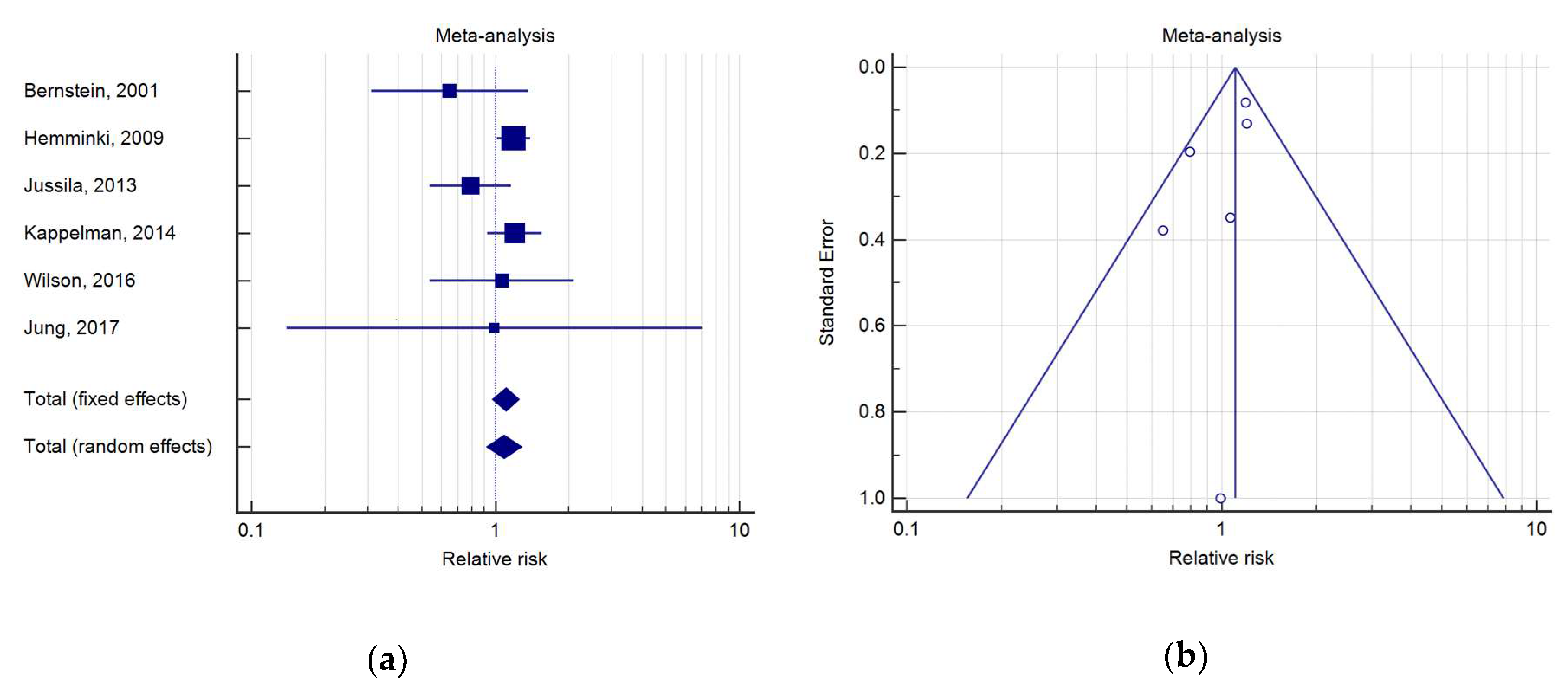
3.3. Prostate Cancer in CD Patients
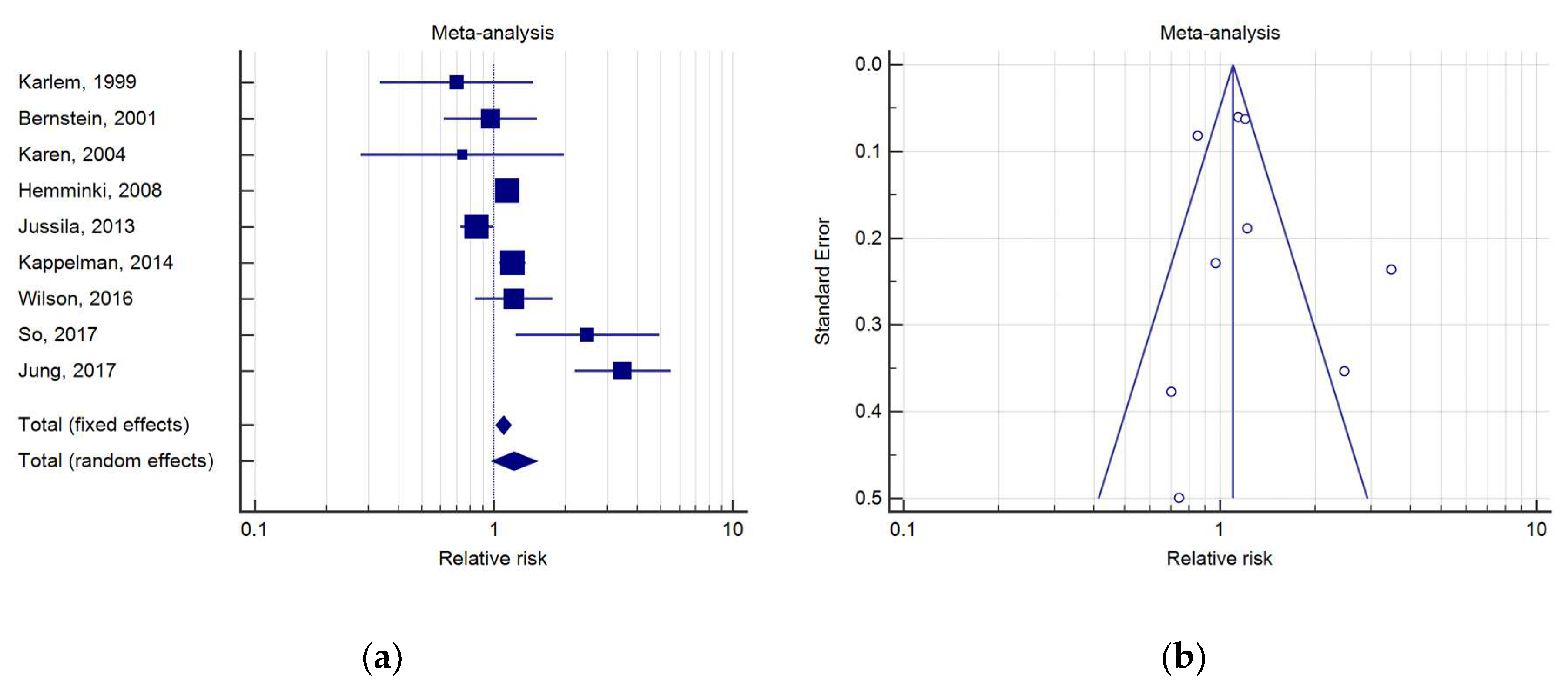
3.4. Prostate Cancer in UC Patients
3.5. Quality Subanalysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kappelman, M.D.; Rifas–Shiman, S.L.; Kleinman, K.; Ollendorf, D.; Bousvaros, A.; Grand, R.J.; Finkelstein, J.A. The Prevalence and Geographic Distribution of Crohn’s Disease and Ulcerative Colitis in the United States. Clin. Gastroenterol. Hepatol. 2007, 5, 1424–1429. [Google Scholar] [CrossRef] [PubMed]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. J. Crohn’s Colitis 2017, 11, 649–670. [Google Scholar] [CrossRef]
- Gomollón, F.; Dignass, A.; Annese, V.; Tilg, H.; Van Assche, G.; Lindsay, J.O.; Peyrin-Biroulet, L.; Cullen, G.J.; Daperno, M.; Kucharzik, T.; et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016: Part 1: Diagnosis and medical management. J. Crohn’s Colitis 2017, 11, 3–25. [Google Scholar] [CrossRef]
- Ribaldone, D.G.; Pellicano, R.; Actis, G.C. The gut and the inflammatory bowel diseases inside-out: Extra-intestinal manifestations. Minerva Gastroenterol. E Dietol. 2019, 65, 309–318. [Google Scholar] [CrossRef]
- Ananthakrishnan, A.N. Epidemiology and risk factors for IBD. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 205–217. [Google Scholar] [CrossRef]
- Kaplan, G.G. The global burden of IBD: From 2015 to 2025. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 720–727. [Google Scholar] [CrossRef]
- De Marzo, A.M.; Platz, E.A.; Sutcliffe, S.; Xu, J.; Grönberg, H.; Drake, C.G.; Nakai, Y.; Isaacs, W.B.; Nelson, W.G. Inflammation in prostate carcinogenesis. Nat. Rev. Cancer 2007, 7, 256–269. [Google Scholar] [CrossRef]
- Derikx, L.A.; Smits, L.J.; van Vliet, S.; Dekker, E.; Aalfs, C.M.; van Kouwen, M.C.; Nagengast, F.M.; Nagtegaal, I.D.; Hoogerbrugge, N.; Hoentjen, F. Colorectal Cancer Risk in Patients With Lynch Syndrome and Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2017, 15, 454–458. [Google Scholar] [CrossRef]
- Pedersen, N.; Duricova, D.; Elkjaer, M.; Gamborg, M.; Munkholm, P.; Jess, T. Risk of extra-intestinal cancer in inflammatory bowel disease: Meta-analysis of population-based cohort studies. Am. J. Gastroenterol. 2010, 105, 1480–1487. [Google Scholar] [CrossRef]
- Kappelman, M.D.; Farkas, D.K.; Long, M.D.; Erichsen, R.; Sandler, R.S.; Sørensen, H.T.; Baron, J.A. Risk of cancer in patients with inflammatory bowel diseases: A nationwide population-based cohort study with 30 years of follow-up evaluation. Clin. Gastroenterol. Hepatol. 2014, 12, 265–273. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca: A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.A.; Weiner, A.B.; Catalona, W.J.; Li, E.V.; Schaeffer, E.M.; Hanauer, S.B.; Strong, S.; Burns, J.; Hussain, M.H.; Kundu, S.D. Inflammatory Bowel Disease and the Risk of Prostate Cancer. Eur. Urol. 2019, 75, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Jussila, A.; Virta, L.J.; Pukkala, E.; Färkkilä, M.A. Malignancies in patients with inflammatory bowel disease: A nationwide register study in Finland. Scand. J. Gastroenterol. 2013, 48, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef]
- Karlen, P.; Lofberg, R.; Brostrom, O.; Leijonmarck, C.-E.; Hellers, G.; Persson, P.-G. Increased risk of cancer in ulcerative colitis: A population-based cohort study. Am. J. Gastroenterol. 1999, 94, 1047–1052. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Blanchard, J.F.; Kliewer, E.; Wajda, A. Cancer risk in patients with inflammatory bowel disease: A population-based study. Cancer 2001, 91, 854–862. [Google Scholar] [CrossRef]
- Winther, K.V.; Jess, T.; Langholz, E.; Munkholm, P.; Binder, V. Long-term risk of cancer in ulcerative colitis: A population-based cohort study from Copenhagen County. Clin. Gastroenterol. Hepatol. 2004, 2, 1088–1095. [Google Scholar] [CrossRef]
- Hemminki, K.; Li, X.; Sundquist, J.; Sundquist, K. Cancer risks in ulcerative colitis patients. Int. J. Cancer 2008, 123, 1417–1421. [Google Scholar] [CrossRef]
- Hemminki, K.; Li, X.; Sundquist, J.; Sundquist, K. Cancer risks in Crohn disease patients. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. 2009, 20, 574–580. [Google Scholar] [CrossRef]
- Wilson, J.C.; Furlano, R.I.; Jick, S.S.; Meier, C.R. A population-based study examining the risk of malignancy in patients diagnosed with inflammatory bowel disease. J. Gastroenterol. 2016, 51, 1050–1062. [Google Scholar] [CrossRef]
- Jung, Y.S.; Han, M.; Park, S.; Kim, W.H.; Cheon, J.H. Cancer Risk in the Early Stages of Inflammatory Bowel Disease in Korean Patients: A Nationwide Population-based Study. J. Crohn’s Colitis 2017, 11, 954–962. [Google Scholar] [CrossRef] [PubMed]
- So, J.; Tang, W.; Leung, W.K.; Li, M.; Lo, F.H.; Wong, M.T.; Sze, A.S.; Leung, C.M.; Tsang, S.W.; Shan, E.H.; et al. Cancer Risk in 2621 Chinese Patients with Inflammatory Bowel Disease: A Population-based Cohort Study. Inflamm. Bowel Dis. 2017, 23, 2061–2068. [Google Scholar] [CrossRef] [PubMed]
- Mosher, C.A.; Brown, G.R.; Weideman, R.A.; Crook, T.W.; Cipher, D.J.; Spechler, S.J.; Feagins, L.A. Incidence of Colorectal Cancer and Extracolonic Cancers in Veteran Patients With Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2018, 24, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Sutton, A.J.; Ioannidis, J.P.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef]
- Islam, M.M.; Iqbal, U.; Walther, B.; Atique, S.; Dubey, N.K.; Nguyen, P.A.; Poly, T.N.; Masud, J.H.; Li, Y.C.; Shabbir, S.A. Benzodiazepine Use and Risk of Dementia in the Elderly Population: A Systematic Review and Meta-Analysis. Neuroepidemiology 2016, 47, 181–191. [Google Scholar] [CrossRef]
- Ge, Y.; Shi, Q.; Yao, W.; Cheng, Y.; Ma, G. The association between inflammatory bowel disease and prostate cancer risk: A meta-analysis. Prostate Cancer Prostatic Dis. 2020, 23, 53–58. [Google Scholar] [CrossRef]
- Chen, M.; Yuan, C.; Xu, T. An increase in prostate cancer diagnosis during inflammatory bowel disease: A systematic review and meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2019. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | Selection | Comparability | Outcome | Overall Quality Score |
|---|---|---|---|---|
| Cohort study | ||||
| Karlen (1999) [15] | 4 | 0 | 1 | 5 |
| Bernstein (2001) [16] | 4 | 1 | 3 | 8 |
| Whinter (2004) [17] | 4 | 0 | 2 | 6 |
| Hemminki (2008) [18] | 4 | 1 | 2 | 7 |
| Hemminki (2009) [19] | 4 | 1 | 2 | 7 |
| Jussila (2013) [13] | 4 | 0 | 3 | 7 |
| Kappelman (2014) [10] | 4 | 1 | 3 | 8 |
| Wilson (2016) [20] | 4 | 2 | 2 | 8 |
| Jung (2017) [21] | 4 | 1 | 1 | 6 |
| So (2017) [22] | 4 | 2 | 3 | 9 |
| Case-control study | ||||
| Burns (2018) [12] | 4 | 2 | 2 | 8 |
| Mosher (2018) [23] | 4 | 0 | 2 | 6 |
| Author | Location | Region | Data Source | Year | PC/Patients with IBD | PC/Control Population | RR | 95%CI |
|---|---|---|---|---|---|---|---|---|
| Bernstein et al. [16] | Canada | Manitoba | C.R. | 2001 | 26/5526 | 6293/1,151,000 | 0.86 | 0.59–1.26 |
| Jussila et al. [13] | Finland | Finland | C.R. | 2013 | 176/21,964 | 51,045/5,351,000 | 0.84 | 0.73–0.97 |
| Kappelman et al. [10] | Denmark | Denmark | C.R. | 2014 | 316/42,717 | 33,960/5,554,844 | 1.21 | 1.08–1.35 |
| Wilson et al. [20] | UK | UK | CPRD | 2016 | 79/19,647 | 67/19,647 | 1.18 | 0.85–1.63 |
| Jung et al. [21] | Korea | Korea | HIRA-d | 2017 | 19/15,291 | 20,607/50,750,000 | 3.06 | 1.95–4.80 |
| So et al. [22] | H.K. | H.K. | IBD-d | 2018 | 8/2621 | 11,115/7,392,000 | 2.03 | 1.03–4.06 |
| Mosher et al. [23] | USA | North Texas | C.C. | 2018 | 12/2080 | 916/271,898 | 1.71 | 0.97–3.02 |
| Burns et al. [12] | USA | Northwestern | NMADR | 2018 | 30/1033 | 29/9306 | 9.32 | 5.62–15.46 |
| Author | Location | Region | Data source | Year | PC/Patients with CD | PC/Control Population | RR | 95%CI |
|---|---|---|---|---|---|---|---|---|
| Bernstein et al. [16] | Canada | Manitoba | C.R. | 2001 | 7/2857 | 4338/1,151,000 | 0.65 | 0.31–1.36 |
| Hemminki et al. [19] | Sweden | Sweden | C.R. | 2009 | 152/21,788 | 52,621/8,976,000 | 1.20 | 1.02–1.40 |
| Jussila et al. [13] | Finland | Finland | C.R. | 2013 | 26/5315 | 33,134/5,351,000 | 0.79 | 0.54–1.14 |
| Kappelman et al. [10] | Denmark | Denmark | C.R. | 2014 | 58/13,756 | 19,518/5,554,844 | 1.20 | 0.93–1.55 |
| Wilson et al. [20] | UK | UK | CPRD | 2016 | 79/19,647 | 67/19,647 | 1.18 | 0.85–1.63 |
| Jung et al. [21] | Korea | Korea | HIRA-d | 2017 | 19/15,291 | 20,607/50,750,000 | 3.06 | 1.95–4.80 |
| Author | Year | Location | Region | Data Source | n. of PC/Patients with UC | n. of PC/Control Population | RR | 95%CI |
|---|---|---|---|---|---|---|---|---|
| Karlèn et al. [15] | 1999 | Sweden | Stockholm | C.R. | 7/1547 | 11,526/1,783,000 | 0.70 | 0.33–1.47 |
| Bernstein et al. [16] | 2001 | Canada | Manitoba | C.R. | 19/2672 | 8438/1,151,000 | 0.97 | 0.62–1.52 |
| Winther et al. [17] | 2004 | Denmark | Copenhagen | P.B.C. | 4/1160 | 2598/557,500 | 0.74 | 0.28–1.94 |
| Hemminki et al. [18] | 2008 | Sweden | Sweden | C.R. | 277/27,606 | 79,005/8,976,000 | 1.14 | 1.01–1.28 |
| Jussila et al. [13] | 2013 | Finland | Finland | C.R. | 150/16,649 | 56,718/5,351,000 | 0.85 | 0.73–1.00 |
| Kappelman et al. [10] | 2014 | Denmark | Denmark | C.R. | 258/35,152 | 33,976/5,554,844 | 1.21 | 1.08–1.35 |
| Wilson et al. [20] | 2016 | UK | UK | CPRD | 62/11,797 | 51/11,797 | 1.21 | 0.84–1.76 |
| Jung et al. [21] | 2017 | Korea | Korea | HIRA-d | 18/9787 | 26,904/50,750,000 | 3.47 | 2.19–5.51 |
| So et al. [22] | 2017 | H.K. | H.K. | IBD-d | 8/1603 | 14,936/7,392,000 | 2.47 | 1.24–4.93 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carli, E.; Caviglia, G.P.; Pellicano, R.; Fagoonee, S.; Rizza, S.; Astegiano, M.; Saracco, G.M.; Ribaldone, D.G. Incidence of Prostate Cancer in Inflammatory Bowel Disease: A Meta-Analysis. Medicina 2020, 56, 285. https://doi.org/10.3390/medicina56060285
Carli E, Caviglia GP, Pellicano R, Fagoonee S, Rizza S, Astegiano M, Saracco GM, Ribaldone DG. Incidence of Prostate Cancer in Inflammatory Bowel Disease: A Meta-Analysis. Medicina. 2020; 56(6):285. https://doi.org/10.3390/medicina56060285
Chicago/Turabian StyleCarli, Edoardo, Gian Paolo Caviglia, Rinaldo Pellicano, Sharmila Fagoonee, Stefano Rizza, Marco Astegiano, Giorgio Maria Saracco, and Davide Giuseppe Ribaldone. 2020. "Incidence of Prostate Cancer in Inflammatory Bowel Disease: A Meta-Analysis" Medicina 56, no. 6: 285. https://doi.org/10.3390/medicina56060285
APA StyleCarli, E., Caviglia, G. P., Pellicano, R., Fagoonee, S., Rizza, S., Astegiano, M., Saracco, G. M., & Ribaldone, D. G. (2020). Incidence of Prostate Cancer in Inflammatory Bowel Disease: A Meta-Analysis. Medicina, 56(6), 285. https://doi.org/10.3390/medicina56060285