A Six-Year Analysis of Biological Therapy for Severe Psoriasis in a Lithuanian Reference Centre of Dermatovenereology

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Demographic and Other Clinical Characteristics
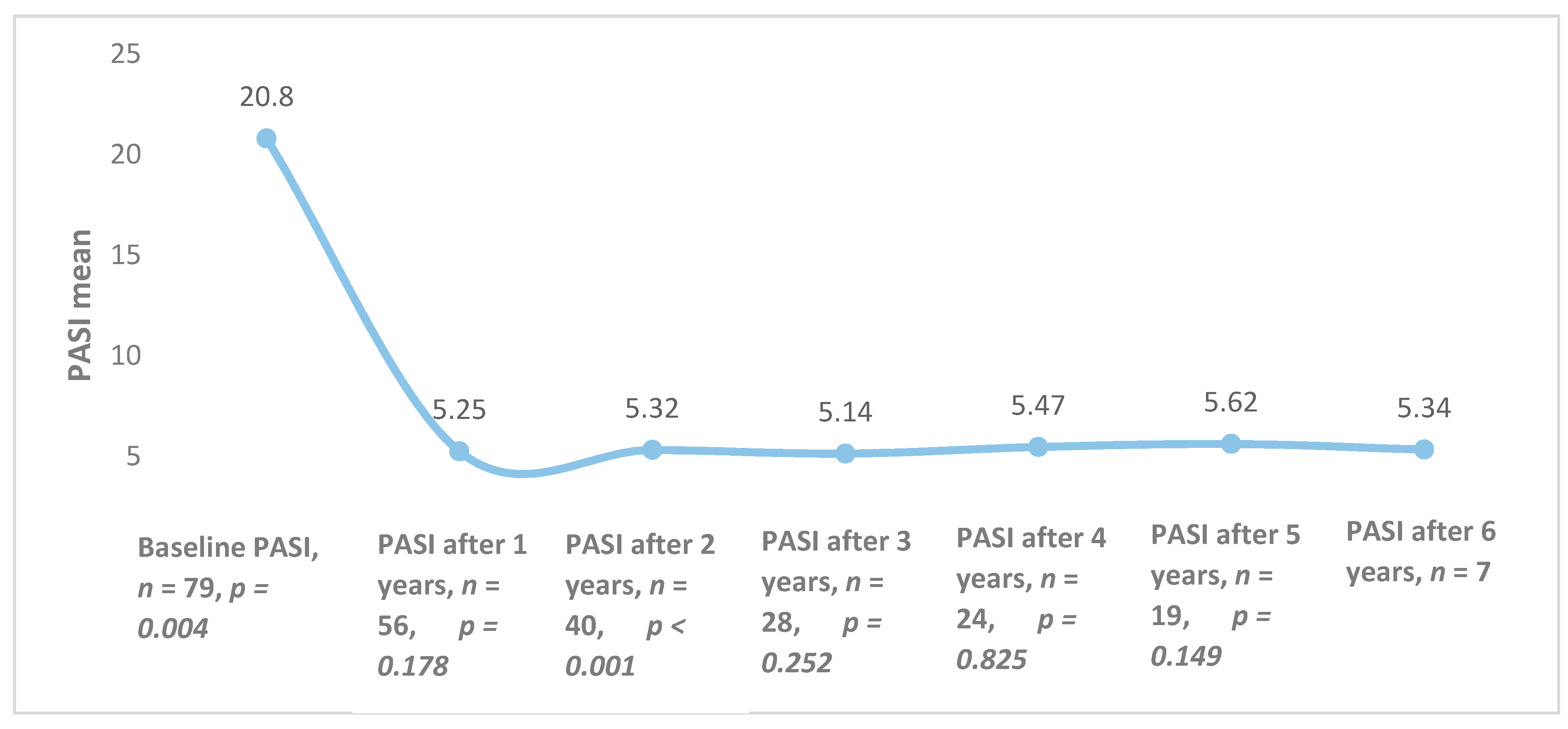
3.2. Baseline PASI and Changes during Treatment
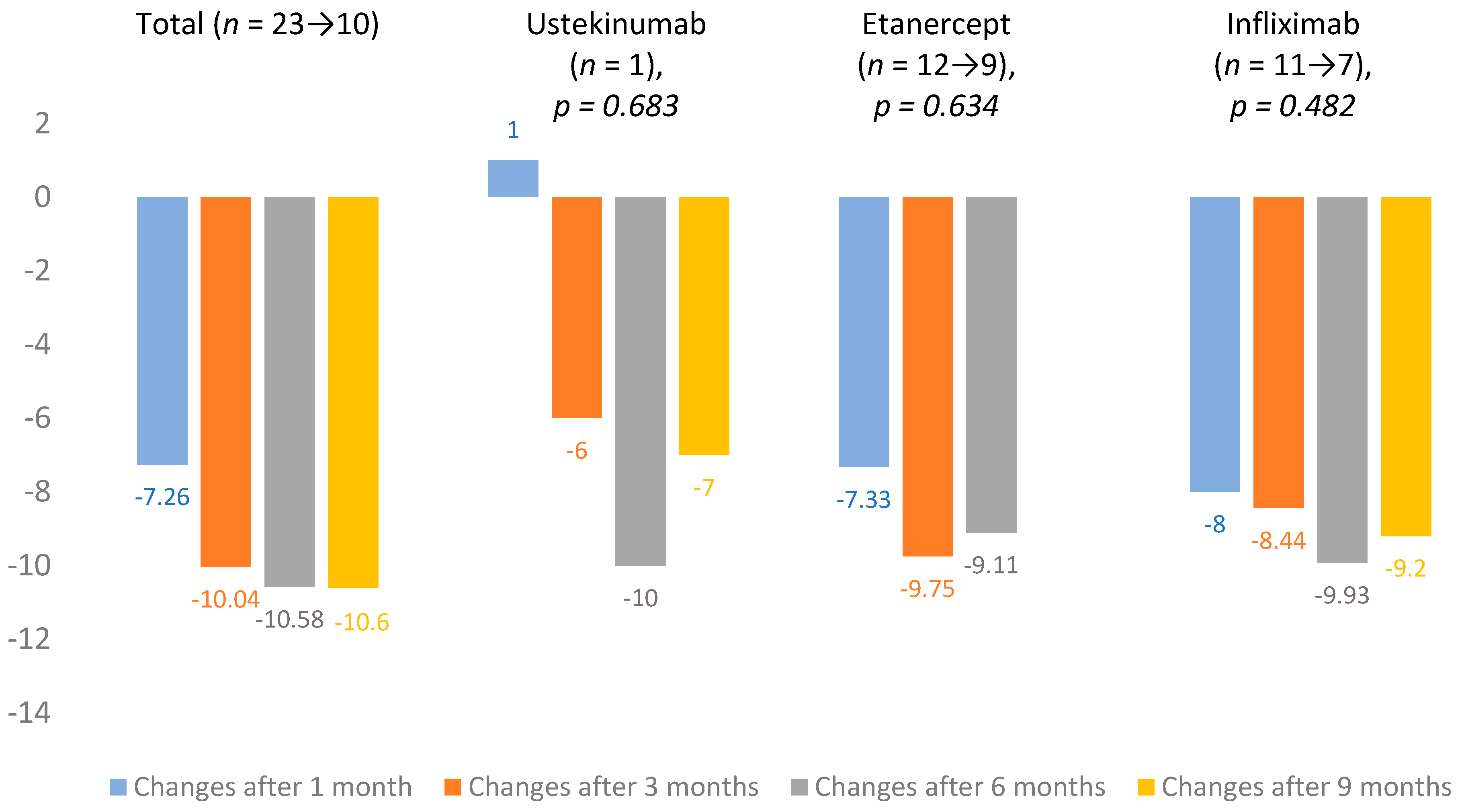
3.3. Efficacy of Different Biological Agents
3.4. Baseline DLQI and Its Changes during Treatment
3.5. Baseline BMI and Changes over the Course of Biological Therapy
3.6. Laboratory and Instrumental Tests
Changes in Complete Blood Count
3.7. Adverse Effects of Biological Therapy
3.8. Switching of Biologics
3.9. Comorbidities
3.10. Additional Topical Treatment and Phototherapy
3.11. The Use of Methotrexate before and during Biological Therapy
3.12. Consultations by other Specialists and Medications Used
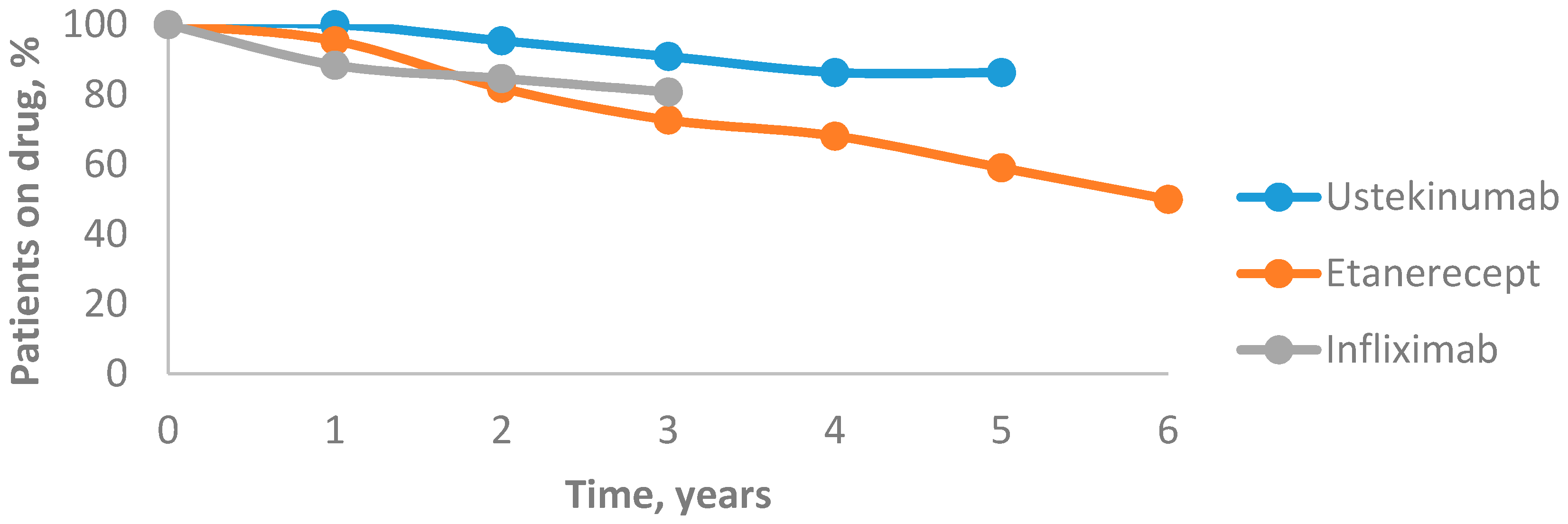
3.13. Drug Survival Rates of Biological Agents
4. Discussion
4.1. Efficacy
4.2. DLQI
4.3. BMI
4.4. Changes in Laboratory and Instrumental Tests
4.5. Safety
4.6. Drug Survival
4.7. Switching of Biologics
4.8. Comorbidities
4.9. Additional Psoriasis Treatment with Topical Medications, Phototherapy, and Methotrexate
4.10. Comorbidities Treatment and Consultations of other Specialists
4.11. Future Perspectives
4.12. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Honda, H.; Umezawa, Y.; Kikuchi, S.; Yanaba, K.; Fukuchi, O.; Ito, T.; Nobeyama, Y.; Asahina, A.; Nakagawa, H. Switching of biologics in psoriasis: Reasons and results. J. Dermatol. 2017, 44, 1015–1019. [Google Scholar] [CrossRef] [PubMed]
- Olszewska, B.; Adamski, Z.; Czarnecka-Operacz, M. Que vadis, biological treatment for psoriasis and psoriatic arthritis? Adv. Dermatol. Allergol. 2018, 35, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Bonanad, C.; González-Parra, E.; Rivera, R.; Carrascosa, J.M.; Daudén, E.; Olveira, A.; Estrada, R.B. Clinical, diagnostic, and therapeutic implications in psoriasis associated with cardiovascular disease. Actas Dermosifiliogr. 2017, 108, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Feldman, S.R.; Rastogi, S.; Lin, J. Effect of prior biologic use on cost-effectiveness of brodalumab vs. ustekinumab for treatment of moderate-to-severe psoriasis in the United States. Dermatol. Ther. 2018, 8, 441–453. [Google Scholar] [CrossRef]
- Ergen, E.N.; Yusuf, N. Inhibition of interleukin-12 and/or interleukin-23 for the treatment of psoriasis: What is the evidence for an effect on malignancy? Exp. Dermatol. 2018, 27, 737–747. [Google Scholar] [CrossRef]
- Dėl Psoriazės Gydymo Vaistais, Kurių Įsigijimo Išlaidos Apmokamos Privalomojo Sveikatos Draudimo fondo Biudžeto Lėšomis, Tvarkos Aprašo Patvirtinimo. Available online: http://www.vlk.lt/veikla/veiklos-sritys/kompensuojamieji-vaistai/Documents/SAM%20psoriaz%C4%97s%20V-1014_RedakcijaNr_1_.pdf (accessed on 3 June 2020).
- Wu, D.; Hou, S.Y.; Zhao, S.; Hou, L.-X.; Jiao, T.; Xu, N.-N.; Zhang, N. Efficacy and safety of interleukin-17 antagonists in patients with plaque psoriasis: A meta-analysis from phase 3 randomized controlled trials. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 992–1003. [Google Scholar] [CrossRef]
- Golbari, N.M.; Porter, M.L.; Kimball, A.B. Current guidelines for psoriasis treatment: A work in progress. Cutis 2018, 101, 10–12. [Google Scholar]
- Jasaitienė, D.; Beliauskienė, A.; Karmazienė, T.; Marčiukaitienė, I.O.; Grigaitienė, J.; Bylaitė-Bučinskienė, M. Žvynelinės Gydymo Rekomendacijos. Mokomoji Knyga; Vilniaus Universitetas: Lietuvos Dermatovenerologų DraugijaL Vilnius, Lietuva, 2017; pp. 10–12. [Google Scholar]
- Leisner, M.Z.; Lindorff Riis, J.; Gniadecki, R.; Iversen, L.; Olsen, M. Psoriasis and risk of myocardial infarction before and during an era with biological therapy: A population-based follow-up study. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 2185–2190. [Google Scholar] [CrossRef]
- Zschocke, I.; Ortland, C.; Reich, K. Evaluation of adherence predictors for the treatment of moderate to severe psoriasis with biologics: The importance of physician-patient interaction and communication. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1014–1020. [Google Scholar] [CrossRef]
- Sherman, S.; Hodak, E.; Pavlovsky, L. Can etanercept treatment failure in moderate-to-severe psoriasis be overcome by addition of low-dose methotrexate? A single-center experience. J. Dermatol. Treat. 2018, 29, 666–670. [Google Scholar] [CrossRef]
- Sbidian, E.; Giboin, C.; Bachelez, H.; Paul, C.; Beylot-Barry, M.; Dupuy, A.; Viguier, M.; Lacour, J.-P.; Schmutz, J.-L.; Bravard, P.; et al. Factors associated with the choice of the first biologic in psoriasis: Real-life analysis from the Psobioteq cohort. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 2046–2054. [Google Scholar] [CrossRef] [PubMed]
- Nast, A.; Jacobs, A.; Rosumeck, S.; Wemer, R.N. Efficacy and safety of systemic long-term treatments for moderate-to-severe psoriasis: A systemic review and meta-analysis. J. Investig. Dermatol. 2015, 135, 2641–2648. [Google Scholar] [CrossRef] [PubMed]
- Puig, L.; Lopez, A.; Vilarrasa, E.; Garcia, I. Efficacy of biologics in the treatment of moderate-to severe plaque psoriasis: A systematic review and meta-analysis of randomized controlled trials with different time points. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 1633–1653. [Google Scholar] [CrossRef] [PubMed]
- Kerdel, F.; Zaiac, M. An evolution in switching therapy for psoriasis patients who fail to meet treatment goal. Dermatol. Ther. 2015, 28, 390–403. [Google Scholar] [CrossRef] [PubMed]
- Sbidian, E.; Chaimani, A.; Garcia-Doval, I.; Do, G.; Hua, C.; Mazaud, C.; Droitcourt, C.; Hughes, C.; Ingram, J.R.; Naldi, L.; et al. Systemic pharmacological treatments for chronic plaque psoriasis: A network meta-analysis. Cochrane Database Syst. Rev. 2017, 12, 1–499. [Google Scholar] [CrossRef]
- Chaptini, C.; Quinn, S.; Marshman, G. Durable dermatology life quality index improvements in patients on biologics associated with psoriasis areas and severity index: A longitudinal study. Australas. J. Dermatol. 2016, 57, 72–75. [Google Scholar] [CrossRef]
- Mattei, P.L.; Corey, K.C.; Kimball, A.B. Psoriasis Area Severity Index (PASI) and the Dermatology Life Quality Index (DLQI): The correlation between disease severity and psychological burden in patients treated with biological therapies. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 333–337. [Google Scholar] [CrossRef]
- Jungo, P.; Maul, J.T.; Djamei, V.; von Felten, S.; Kolios, A.G.A.; Czernielewsk, J.; Yawalkar, N.; Odermatt, O.; Laffitte, E.; Anliker, M.; et al. Superiority in quality of life improvement of biologics over conventional systemic drugs in a Swiss real-life psoriasis registry. Dermatology 2016, 232, 655–663. [Google Scholar] [CrossRef]
- Kaushik, S.B.; Lebwohl, M.G. Review of safety and efficacy of approved systemic psoriasis therapies. Int. J. Dermatol. 2019, 58, 649–658. [Google Scholar] [CrossRef]
- Takamura, S.; Takahashi, A.; Inoue, Y.; Teraki, Y. Effects of tumor necrosis factor-α, interleukin-23 and interleukin-17A inhibitors on bodyweight and body mass index in patients with psoriasis. J. Dermatol. 2018, 45, 1130–1134. [Google Scholar] [CrossRef]
- Gavrilă, B.I.; Ciofu, C.; Stoica, V.; Panaitescu, E. The efficiency of biologic therapy in a group of patients with rheumatoid arthritis. J. Med. Life 2015, 8, 79–84. [Google Scholar] [PubMed]
- Chen, D.Y.; Chen, Y.M.; Hsieh, T.Y.; Hsieh, C.W.; Lin, C.C.; Lan, J.L. Significant effects of biologic therapy on lipid profiles and insulin resistance in patients with rheumatoid arthritis. Arthritis Res. Ther. 2015, 17, 52. [Google Scholar] [CrossRef] [PubMed]
- Snekvik, I.; Nilsen, T.I.L.; Romundstad, P.R.; Saunes, M. Psoriasis and cardiovascular disease risk factor: The HUNT study, Norway. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Schadler, E.D.; Ortel, B.; Mehlis, S.L. Biologics for primary care physician: Review and treatment of psoriasis. Dis. Mon. 2019, 65, 51–90. [Google Scholar] [CrossRef] [PubMed]
- Tran-Minh, M.L.; Sousa, P.; Maillet, M.; Allez, M.; Gornet, J.M. Hepatic complications induced by immunosuppressants and biologics in inflammatory bowel disease. World J. Hepatol. 2017, 9, 613–626. [Google Scholar] [CrossRef]
- Sârbu, M.I.; Tampa, M.; Mitran, M.I.; Mitran, C.I.; Limbău, A.M. Adverse reactions of biological therapies in patients with psoriasis. J. Mind Med. Sci. 2017, 4, 4–12. [Google Scholar] [CrossRef]
- Sivamani, R.K.; Goodarzi, H.; Shirakawa, M.; Raychaudhuri, S.P.; Wehrli, L.N.; Ono, Y.; Maverakis, E. Biologic therapies in the treatment of psoriasis: A comprehensive evidence-based basic science and clinical review and a practical guide to tuberculosis monitoring. Clin. Rev. Allergy Immunol. 2013, 44, 121–140. [Google Scholar] [CrossRef]
- Nisar, M.K.; Rafiq, A.; Östör, A.J.K. Biologic therapy for inflammatory arthritis and latent tuberculosis: Reall world experience from a high prevalence area in the United Kingdom. Clin. Rheumatol. 2015, 34, 2141–2145. [Google Scholar] [CrossRef]
- World Health Organization. Latent Tuberculosis Infection: Updated and Consolidated Guidelines for Programmatic Management; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Menter, A.; Papp, K.A.; Gooderham, M.; Pariser, D.M.; Augustin, M.; Kerdel, F.A.; Fakharzadeh, S.; Goyal, K.; Calabro, S.; Langholff, W.; et al. Drug survival of biologic therapy in a large, disease-based registry of patients with psoriasis: Results from the Psoriasis Longitudinal Assessment and Registry (PSOLAR). J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1148–1158. [Google Scholar] [CrossRef]
- Warren, R.B.; Smith, C.H.; Yiu, Z.Z.N.; Ashcroft, D.M.; Barker, J.N.W.N.; Burden, A.D.; Lunt, M.; McElhone, K.; Ormerod, A.D.; Owen, C.M.; et al. Differential drug survival of biologic therapies for the treatment of psoriasis: A prospective observational cohort study from the British Association of Dermatologists Biologic Interventions Register (BADBIR). J. Investig. Dermatol. 2015, 135, 2632–2640. [Google Scholar] [CrossRef]
- Pérez-Plaza, A.; Carretero, G.; Ferrandiz, C.; Vanaclocha, F.; Gómez-García, F.J.; Herrera-Ceballos, E.; de la Cueva-Dobao, P.; Belinchón, I.; Sánchez-Carazo, J.L.; Alsina, M.; et al. Comparison of phenotype, comorbidities, therapy and adverse events between psoriatic patients with and without psoriatic arthritis. Biobaderm registry. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-N.; Han, K.; Song, S.-W.; Lee, J.H. Hypertension and risk of psoriasis incidence: An 11-year nationwide population-based cohort study. PLoS ONE 2018, 13, e0202854. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Han, J.; Li, W.Q. Hypertension, antihypertensive medication use and risk of psoriasis. JAMA Dermatol. 2014, 150, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Haberka, M.; Bańska-Kisiel, K.; Bergler-Czop, B.; Biedroń, M.; Brzezińska-Wcisło, L.; Okopień, B.; Gąsior, Z. Mild to moderate psoriasis is associated with oxidative stress, subclinical atherosclerosis and endothelial dysfunction. Pol. Arch. Intern. Med. 2018, 128, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.R.; Danila, M.I.; Chen, L.; Chan, B.; Ehst, B.; Xie, F.; Winthrop, K.L.; Yun, H. Risk of cardiovascular outcomes among psoriasis patients treated with biologics and other systemic agents. J. Psoriasis Psoriatic Arthritis. 2016, 1, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, J.M. Commentary: Does biologic treatment of psoriasis lower the risk of cardiovascular events and mortality? A critical question that we are only just beginning to answer. J. Am. Acad. Dermatol. 2018, 79, 60–68. [Google Scholar] [CrossRef]
- Nguyen, T.; Wu, J.J. Relationship between tumor necrosis factor-α inhibitors and cardiovascular disease in psoriasis: A review. Perm J. 2014, 18, 49–54. [Google Scholar] [CrossRef]
- Caiazzo, G.; Fabbrocini, G.; Di Caprio, R.; Raimondo, A.; Scala, E.; Balato, N.; Balato, A. Psoriasis, cardiovascular events and biologics: Lights and shadows. Front. Immunol. 2018, 9, 1668. [Google Scholar] [CrossRef]
- Kaushik, S.B.; Lebwohl, M.G. Psoriasis: Which therapy for which patient: Psoriasis comorbidities and preferred systemic agents. J. Am. Acad. Dermatol. 2019, 80, 27–40. [Google Scholar] [CrossRef]
- Kaushik, S.B.; Lebwohl, M.G. Psoriasis: Which therapy for which patient: Focus on special populations and chronic infections. J. Am. Acad. Dermatol. 2019, 80, 43–53. [Google Scholar] [CrossRef]
- Jensen, J.D.; Delcambre, M.R.; Nguyen, G.; Sami, N. Biologic therapy with or without topical treatment in psoriasis: What does the current evidence say? Am. J. Clin. Dermatol. 2014, 15, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Cather, J.C.; Crowley, J.J. Use of biologic agent in combination with other therapies for the treatment of psoriasis. Am. J. Clin. Dermatol. 2014, 15, 467–478. [Google Scholar] [CrossRef]
- Wu, J.J.; Lynde, C.W.; Kleyn, C.E.; Iversen, L.; van der Walt, J.M.; Carvalho, A.; Kirby, B.; Bissonnette, R. Identification of key research needs for topical therapy treatment of psoriasis-a consensus paper by International Psoriasis Council. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1115–1119. [Google Scholar] [CrossRef] [PubMed]
- Papp, K.A.; Barber, K.; Bissonnette, R.; Bourcier, M.; Lynde, C.W.; Poulin, Y.; Shelton, J.; Garces, K.; Toole, J.; Poulin-Costello, M. Improvements in patient-reported outcomes in patients with psoriasis receiving etanercept plus topical therapies: Results from REFINE. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1555–1561. [Google Scholar] [CrossRef] [PubMed]
- Iversen, L.; Lange, M.M.; Bissonette, R.; Carvalho, A.V.E.; van de Kerkhof, P.C.; Kirby, B.; Kleyn, C.E.; Lynde, C.W.; van der Walt, J.M.; Wu, J.J. Topical treatment of psoriasis: Questionnaire results on topical therapy accessibility and influence of body surface area on usage. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1186–1195. [Google Scholar] [CrossRef]
- Bath, R.K.; Brar, N.K.; Forouhar, F.A.; Wu, G.Y. A review of methotrexate-associated hepatotoxicity. J. Dig. Dis. 2014, 15, 517–524. [Google Scholar] [CrossRef]
- Dalkilic, E.; Coskun, B.N.; Yagiz, B.; Tufan, A.N.; Ermurat, S.; Pehlivan, Y. Methotrexate intoxications: Beyond the adverse events. Int. J. Rheum. Dis. 2018, 21, 1557–1562. [Google Scholar] [CrossRef]
- Gulliver, W.P.; Young, H.M.; Bachelez, H.; Randell, S.; Gulliver, S.; Al-Mutairi, N. Psoriasis patients treated with biologics and methotrexate have a reduced rate of myocardial infarction: A collaborative analysis using international cohorts. J. Cutan. Med. Surg. 2016, 20, 550–554. [Google Scholar] [CrossRef]
- Al-Janabi, A.; Jabbar-Lopez, Z.K.; Griffiths, C.E.M.; Yiu, Z.Z.N. Risankizumab vs. ustekinumab for plaque psoriasis: A critical appraisal. Br. J. Dermatol. 2019, 180, 1348–1351. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Demographic and Clinical Characteristics | Ustekinumab | Etanercept | Infliximab | p Value | Total |
|---|---|---|---|---|---|
| Number of patients treated by the first biologic, n (%) | 19 (24.1) | 29 (36.7) | 31 (39.2) | 0.900 | 79 (100) |
| Males, n (%) | 14 (73.7) | 21 (72.4) | 24 (77.4) | 59 (74.7) | |
| Females, n (%) | 5 (26.3) | 8 (27.6) | 7 (22.6) | 20 (25.3) | |
| Age at enrolment, mean, years (SD) | 49.5 (10.6) | 48.1 (12.3) | 45.5 (11.1) | 0.461 | 47.4 (11.3) |
| Family history of psoriasis, n (%), | |||||
| Positive Negative No data | 5 (26.3) 4 (21.1) 10 (52.6) | 7 (24.1) 3 (10.3) 19 (65.5) | 14 (45.2) 8 (25.8) 9 (29.0) | 0.74 | 26 (100) 15 (100) 38 (100) |
| Current smokers, n (%) | 1 (5.3) | 4 (13.8) | 5 (16.1) | 0.519 | 10 (12.7) |
| Baseline BMI, kg/m2 (SD) | 27.8 (4.2) | 26.5 (5.1) | 28.7 (7.4) | 0.36 | 27.7 (5.6) |
| Mean morbidity at baseline, years (SD) | 33.5 (13.9) | 24.4 (11.6) | 22.1 (10.5) | 0.005 | 25.7 (13) |
| Duration of first biological treatment, mean, weeks (SD) | 219.1 (95.7) | 156.2 (137.4) | 85.9 (50.2) | <0.001 | 143.7 (112.4) |
| Second biologic, n (%) | 2 (25) | 3 (37) | 3 (38) | - | 8 (100) |
| Third biologic, n (%) | 2 (100) | - | - | - | 2 (100) |
| Psoriatic arthropathy, n (%) | 11 (57.9) | 20 (69) | 26 (83.9) | 0.123 | 57 (72.2) |
| Psoriatic onychodystrophy, n (%) | 17 (89.5) | 23 (79.3) | 24 (77.4) | 0.549 | 64 (81) |
| Laboratory Parameters | Baseline Count, Mean (SD) | After 1 Year, Mean (SD) | After 2 Years, Mean (SD) | After 3 Years, Mean (SD) | After 4 Years, Mean (SD) | After 5 Years, Mean (SD) | After 6 Years, Mean (SD) |
|---|---|---|---|---|---|---|---|
| WBC (×109/L) | 6.7 (2.2) | 6.1 (1.4) | 6.6 (3.2) | 6.3 (1.5) | 6.2 (1.4) | 6.2 (1.2) | 6.3 (0.9) |
| RBC (×1012/L) | 4.8 (0.6) | 4.9 (0.5) | 4.9 (0.4) | 5.0 (0.4) | 4.9 (0.4) | 5.0 (0.4) | 4.7 (0.5) |
| Hemoglobin (g/L) | 144.8 (16) | 147.8 (13.8) | 149.9 (12.3) | 151.1 (14.5) | 149.2 (13.5) | 149.9 (12.6) | 143.1 (16.6) |
| Platelet count (×109/L) | 235.7 (59.3) | 222.5 (42.5) | 223.4 (40.6) | 219.5 (36.9) | 221.6 (40.4) | 217.3 (34.2) | 261.9 (62.3) |
| ESR (mm/h) | 12.8 (14.8) | 9.5 (9.5) | 9 (10.3) | 7.5 (8.5) | 9.9 (10.2) | 12 (12.5) | 13.6 (18.9) |
| CRP (mmol/L) | 7 (15.04) | 2.4 (3.4) | 6.5 (27.6) | 1.8 (2.4) | 1.6 (2.4) | 2.3 (4.6) | 1.7 (1.9) |
| Glucose (mmol/L) | 5.3 (1.1) | 5.3 (0.7) | 5.3 (0.8) | 5.5 (0.9) | 5.4 (0.78) | 5.7 (1) | 6.1 (1.2) |
| Cholesterol (mmol/L) | 5.1 (0.8) | 5.2 (0.8) | 5.4 (0.8) | 5.4 (0.7) | 5.4 (0.8) | 5.5 (0.8) | 5.5 (0.6) |
| AST (U/L) | 24.6 (14.7) | 28 (17.3) | 25 (8.1) | 29.7 (25.2) | 25.8 (9.4) | 25.2 (6.4) | 21.8 (5.3) |
| ALT (U/L) | 35.4 (42.1) | 37.4 (20.1) | 35.8 (20.2) | 39.2 (25.3) | 33.1 (18.1) | 31 (14.4) | 23.1 (6) |
| ALP (U/L) | 78 (23.6) | 75.5 (25.6) | 78.1 (39.6) | 76.7 (27.8) | 74.3 (22.8) | 74.5 (20.9) | 79.7 (20.2) |
| GGT (U/L) | 32.3 (37.8) | 40.1 (39.3) | 44.3 (61.8) | 37.8 (25.6) | 42 (39.7) | 46.3 (56.8) | 33.4 (22.3) |
| Adverse Effects | Ustekinumab, Cases Per Patient Year | Etanercept, Cases Per Patient Year | Infliximab, Cases Per Patient Year |
|---|---|---|---|
| Upper respiratory tract infections | 0.337 | 0.436 | 0.151 |
| Dizziness | - | 0.011 | - |
| Nausea | - | 0.011 | - |
| Mood swings | - | - | 0.042 |
| Fever | - | 0.011 | - |
| Latent tuberculosis | 0.037 | 0.022 | - |
| Dermatological Comorbidities, n (%), p = 0.062 | Non-Dermatological Comorbidities, n (%), p = 0.867 | ||
|---|---|---|---|
| Verruca vulgaris | 8 (10.1) | Hypertension | 32 (40.5) |
| Seborrheic dermatitis | 8 (10.1) | Dyslipidemia | 11 (13.9) |
| Onychomycosis | 5 (6.3) | Obesity | 10 (12.7) |
| Pityriasis versicolor | 4 (5.1) | Hypertensive cardiomyopathy | 8 (10.1) |
| Melanocytic nevus | 4 (5.1) | Latent tuberculosis infection | 8 (10.1) |
| Acne vulgaris | 3 (3.8) | Diabetes mellitus, type 2 | 4 (5.1) |
| Actinic keratosis | 2 (2.5) | Metabolic syndrome | 3 (3.8) |
| Total | 25 (31.6) | Total | 50 (63.3) |
| Additional Topical Treatment, n (%) | Phototherapy, n (%) | ||
|---|---|---|---|
| Emollients | 78 (98.7) | UVB311 phototherapy whole-body | 36 (45.6) |
| Topical glucocorticoids | 67 (84.8) | UVB311 for hands | 10 (12.7) |
| Keratolytics | 41 (51.9) | UVB311 comb | 6 (7.6) |
| Topical combination of vitamin D analogue and glucocorticoids | 20 (25.3) | UVB311 for feet | 5 (6.3) |
| Vitamin D analogues | 8 (10.1) | Combination therapy of UVA and UVB | 3 (3.8) |
| Calcineurin inhibitors | 4 (5.1) | Topical PUVA therapy | 1 (1.3) |
| Total | 79 (100) | Total | 37 (46.8) |
| Medications Used, n (%) | Other Specialist Consultations, n (%) | ||
|---|---|---|---|
| Antihypertensives | 30 (38) | Cardiologists | 30.4 (24) |
| Hepatoprotectors | 24 (30.4) | Rheumatologists | 8.9 (7) |
| Antifungals | 14 (17.7) | Gastroenterologists | 7.7 (6) |
| NSAIDs | 13 (16.5) | Endocrinologists | 3 (3.8) |
| Systemic glucocorticoids | 10 (12.7) | Gynaecologists | 1 (1.3) |
| Topical antibiotics | 8 (10.1) | Psychiatrists | 1 (1.3) |
| Total | 23 (29.1) | Total | 33 (41.8) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raudonis, T.; Gliebute, A.; Grigaityte, A.G.; Lukosiunaite, Z.; Karmaziene, T.; Grigaitiene, J. A Six-Year Analysis of Biological Therapy for Severe Psoriasis in a Lithuanian Reference Centre of Dermatovenereology. Medicina 2020, 56, 275. https://doi.org/10.3390/medicina56060275
Raudonis T, Gliebute A, Grigaityte AG, Lukosiunaite Z, Karmaziene T, Grigaitiene J. A Six-Year Analysis of Biological Therapy for Severe Psoriasis in a Lithuanian Reference Centre of Dermatovenereology. Medicina. 2020; 56(6):275. https://doi.org/10.3390/medicina56060275
Chicago/Turabian StyleRaudonis, Tadas, Akvile Gliebute, Anna Greta Grigaityte, Zivile Lukosiunaite, Tatjana Karmaziene, and Jurate Grigaitiene. 2020. "A Six-Year Analysis of Biological Therapy for Severe Psoriasis in a Lithuanian Reference Centre of Dermatovenereology" Medicina 56, no. 6: 275. https://doi.org/10.3390/medicina56060275
APA StyleRaudonis, T., Gliebute, A., Grigaityte, A. G., Lukosiunaite, Z., Karmaziene, T., & Grigaitiene, J. (2020). A Six-Year Analysis of Biological Therapy for Severe Psoriasis in a Lithuanian Reference Centre of Dermatovenereology. Medicina, 56(6), 275. https://doi.org/10.3390/medicina56060275