Trauma Coagulopathy and Its Outcomes

 ,
, 
 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Study Population
2.4. Statistical Analysis
3. Results
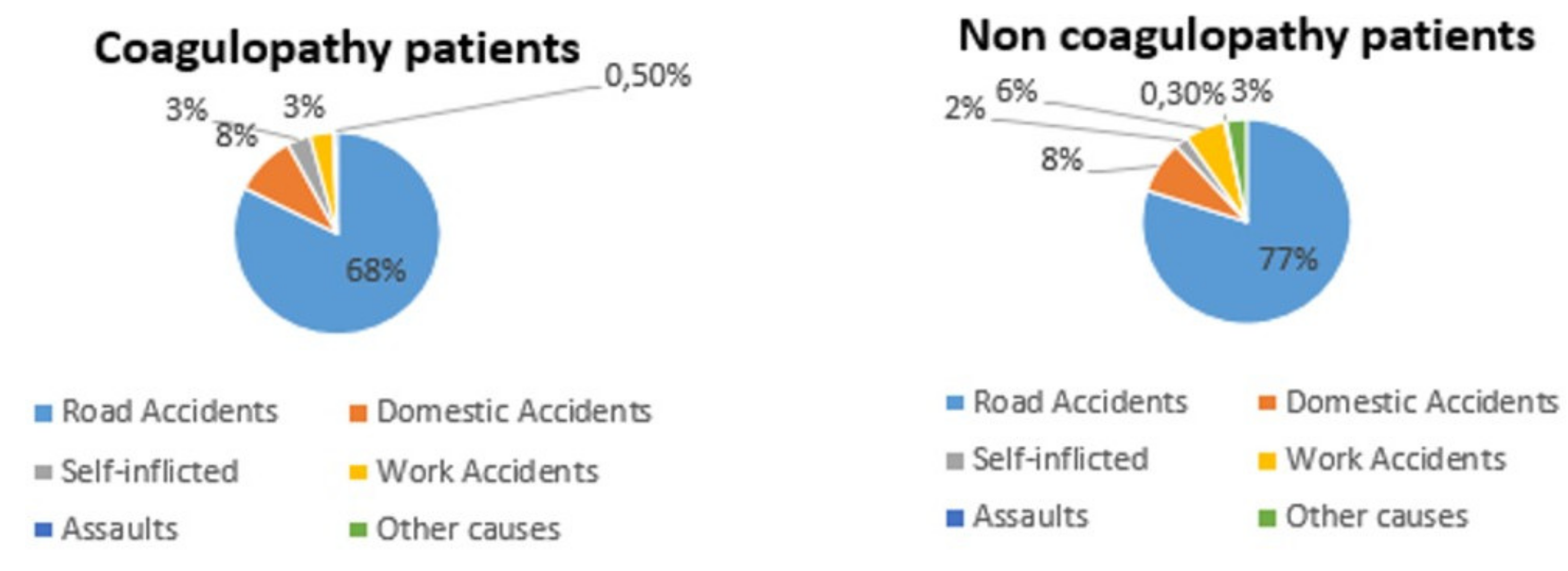
3.1. Study Population
3.1.1. Group 1
3.1.2. Group 2
3.2. Outcomes
3.2.1. Hemotransfusion Rate
3.2.2. Hemodynamic Instability
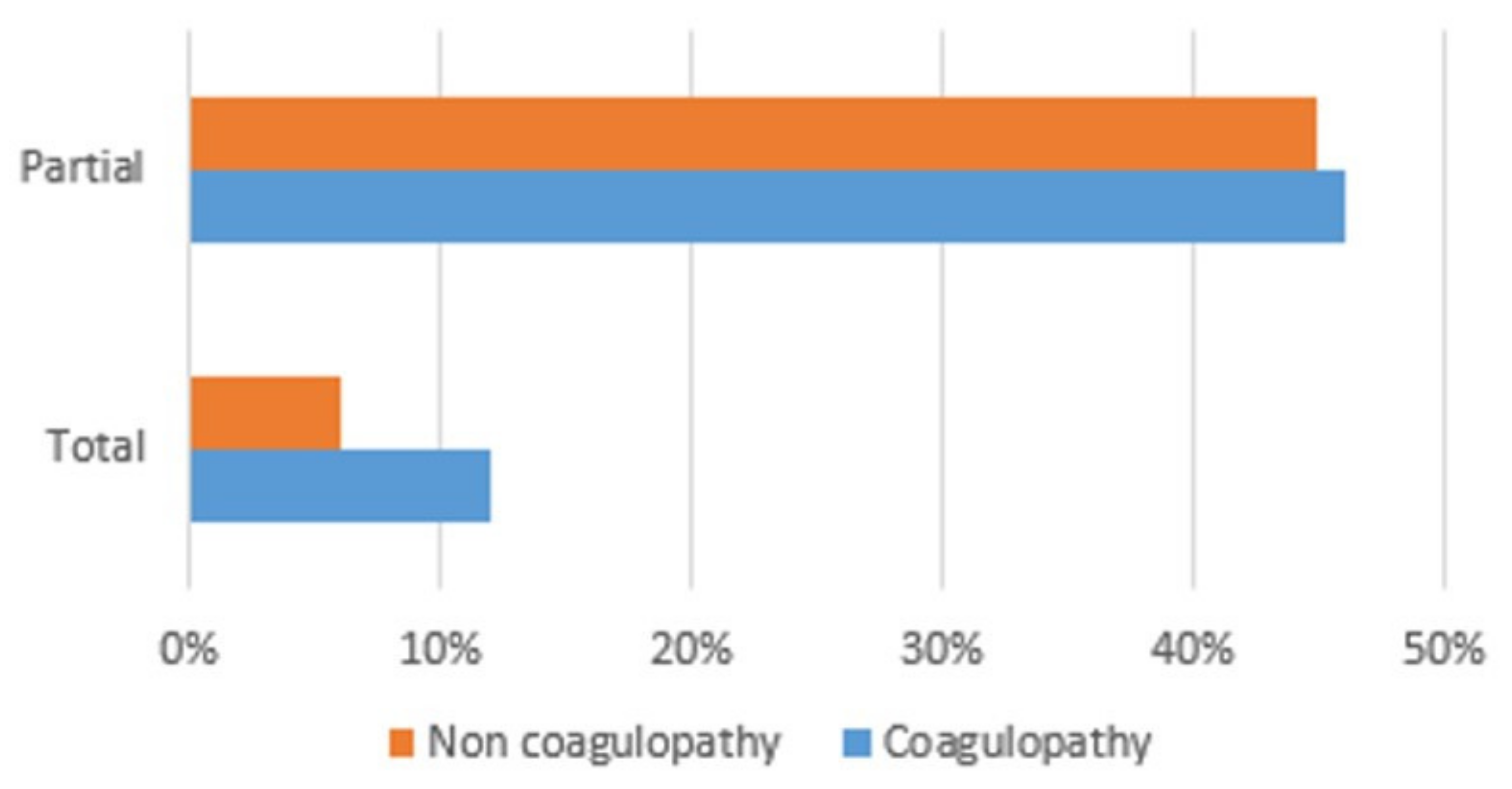
3.2.3. Anatomical Outcomes
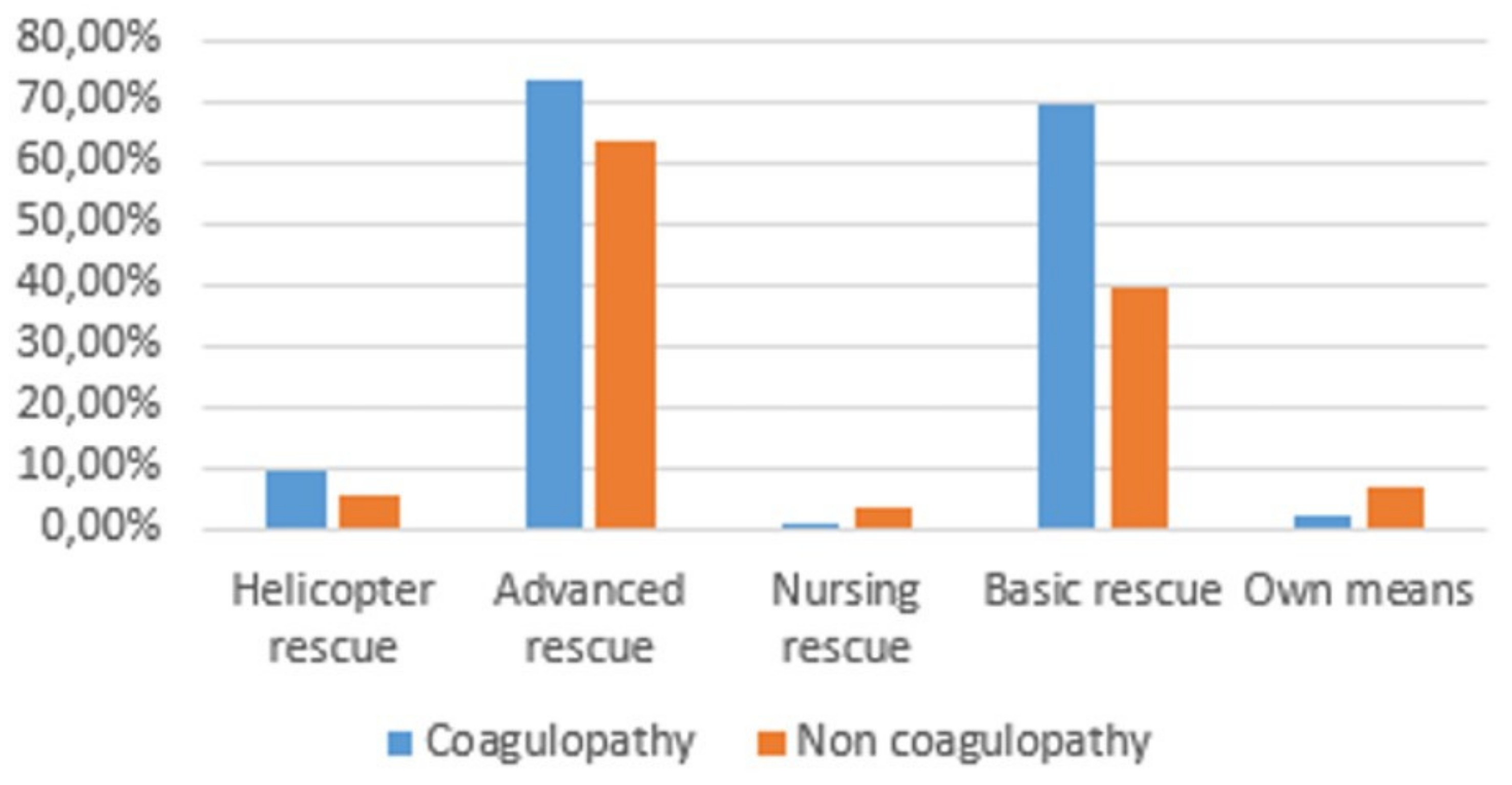
3.2.4. Use of Resources
3.2.5. Mortality
3.2.6. Correlation with Other Unfavorable Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Department of Violence and Injury Prevention and Disability. World Health Organization. Injuries and Violence: The Facts. Available online: http://whqlibdoc.who.int/publications/2010/9789241599375_eng.pdf (accessed on 22 February 2020).
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 385, 117–171. [Google Scholar] [CrossRef]
- Soreide, K. Epidemiology of major trauma. Br. J. Surg. 2009, 96, 697–698. [Google Scholar] [CrossRef] [PubMed]
- Cianci, P.; Fersini, A.; Tartaglia, N.; Altamura, A.; Lizzi, V.; Stoppino, L.P.; Macarini, L.; Ambrosi, A.; Neri, V. Spleen assessment after laparoscopic transperitoneal left adrenalectomy: Preliminary results. Surg. Endosc. 2016, 30, 1503–1507. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cianci, P.; Fersini, A.; Tartaglia, N.; Ambrosi, A.; Neri, V. Are there differences between the right and left laparoscopic adrenalectomy? Our experience. Ann. Ital. Chir. 2016, 87, 242–246. [Google Scholar]
- Cianci, P.; Tartaglia, N.; Altamura, A.; Di Lascia, A.; Fersini, A.; Neri, V.; Ambrosi, A. Cervical Esophagotomy for Foreign Body Extraction: A Case Report and Extensive Literature Review of the Last 20 Years. Am. J. Case Rep. 2018, 19, 400–405. [Google Scholar] [CrossRef]
- Di Lascia, A.; Tartaglia, N.; Fersini, A.; Petruzzelli, F.; Ambrosi, A. Endoscopy for treating minor post-cholecystectomy biliary fistula A review of the literature. Ann. Ital. Chir. 2018, 89, 270–277. [Google Scholar]
- Tartaglia, N.; Petruzzelli, F.; Vovola, F.; Fersini, A.; Ambrosi, A. Antegrade cholecystectomy before ligating the elements. A technique that reduces complications. Ann. Ital. Chir. 2019, 90, 162–164. [Google Scholar]
- Del Maestro, M.; Luzzi, S.; Gallieni, M.; Trovarelli, D.; Giordano, A.V.; Gallucci, M.; Ricci, A.; Galzio, R. Surgical Treatment of Arteriovenous Malformations: Role of Preoperative Staged Embolization. Acta Neurochir. Suppl. 2018, 129, 109–113. [Google Scholar] [CrossRef]
- Gallieni, M.; Del Maestro, M.; Luzzi, S.; Trovarelli, D.; Ricci, A.; Galzio, R. Endoscope-Assisted Microneurosurgery for Intracranial Aneurysms: Operative Technique, Reliability, and Feasibility Based on 14 Years of Personal Experience. Acta Neurochir. Suppl. 2018, 129, 19–24. [Google Scholar] [CrossRef]
- Luzzi, S.; Del Maestro, M.; Bongetta, D.; Zoia, C.; Giordano, A.V.; Trovarelli, D.; Raysi Dehcordi, S.; Galzio, R.J. Onyx Embolization Before the Surgical Treatment of Grade III Spetzler-Martin Brain Arteriovenous Malformations: Single-Center Experience and Technical Nuances. World Neurosurg. 2018, 116, e340–e353. [Google Scholar] [CrossRef]
- Luzzi, S.; Del Maestro, M.; Elbabaa, S.K.; Galzio, R. Letter to the Editor Regarding “One and Done: Multimodal Treatment of Pediatric Cerebral Arteriovenous Malformations in a Single Anesthesia Event”. World Neurosurg. 2020, 134, 660. [Google Scholar] [CrossRef] [PubMed]
- Luzzi, S.; Del Maestro, M.; Galzio, R. Letter to the Editor. Preoperative embolization of brain arteriovenous malformations. J. Neurosurg. 2019, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Luzzi, S.; Elia, A.; Del Maestro, M.; Morotti, A.; Elbabaa, S.K.; Cavallini, A.; Galzio, R. Indication, Timing, and Surgical Treatment of Spontaneous Intracerebral Hemorrhage: Systematic Review and Proposal of a Management Algorithm. World Neurosurg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Luzzi, S.; Gallieni, M.; Del Maestro, M.; Trovarelli, D.; Ricci, A.; Galzio, R. Giant and Very Large Intracranial Aneurysms: Surgical Strategies and Special Issues. Acta Neurochir. Suppl. 2018, 129, 25–31. [Google Scholar] [CrossRef]
- Ricci, A.; Di Vitantonio, H.; De Paulis, D.; Del Maestro, M.; Raysi, S.D.; Murrone, D.; Luzzi, S.; Galzio, R.J. Cortical aneurysms of the middle cerebral artery: A review of the literature. Surg. Neurol. Int. 2017, 8, 117. [Google Scholar] [CrossRef]
- Luzzi, S.; Del Maestro, M.; Trovarelli, D.; De Paulis, D.; Dechordi, S.R.; Di Vitantonio, H.; Di Norcia, V.; Millimaggi, D.F.; Ricci, A.; Galzio, R.J. Endoscope-Assisted Microneurosurgery for Neurovascular Compression Syndromes: Basic Principles, Methodology, and Technical Notes. Asian J. Neurosurg. 2019, 14, 193–200. [Google Scholar] [CrossRef]
- Luzzi, S.; Maestro, M.D.; Elia, A.; Vincitorio, F.; Perna, G.D.; Zenga, F.; Garbossa, D.; Elbabaa, S.K.; Galzio, R. Morphometric and Radiomorphometric Study of the Correlation Between the Foramen Magnum Region and the Anterior and Posterolateral Approaches to Ventral Intradural Lesions. Turk. Neurosurg. 2019, 29, 875–886. [Google Scholar] [CrossRef]
- Luzzi, S.; Zoia, C.; Rampini, A.D.; Elia, A.; Del Maestro, M.; Carnevale, S.; Morbini, P.; Galzio, R. Lateral Transorbital Neuroendoscopic Approach for Intraconal Meningioma of the Orbital Apex: Technical Nuances and Literature Review. World Neurosurg. 2019, 131, 10–17. [Google Scholar] [CrossRef]
- Zoia, C.; Bongetta, D.; Dorelli, G.; Luzzi, S.; Maestro, M.D.; Galzio, R.J. Transnasal endoscopic removal of a retrochiasmatic cavernoma: A case report and review of literature. Surg. Neurol. Int. 2019, 10, 76. [Google Scholar] [CrossRef]
- Arnaout, M.M.; Luzzi, S.; Galzio, R.; Aziz, K. Supraorbital keyhole approach: Pure endoscopic and endoscope-assisted perspective. Clin. Neurol. Neurosurg. 2020, 189, 105623. [Google Scholar] [CrossRef]
- Frith, D.; Goslings, J.C.; Gaarder, C.; Maegele, M.; Cohen, M.J.; Allard, S.; Johansson, P.I.; Stanworth, S.; Thiemermann, C.; Brohi, K. Definition and drivers of acute traumatic coagulopathy: Clinical and experimental investigations. J. Thromb. Haemost. 2010, 8, 1919–1925. [Google Scholar] [CrossRef] [PubMed]
- Maegele, M.; Lefering, R.; Yucel, N.; Tjardes, T.; Rixen, D.; Paffrath, T.; Simanski, C.; Neugebauer, E.; Bouillon, B.; The AG Polytrauma of the German Trauma Society (DGU). Early coagulopathy in multiple injury: An analysis from the German Trauma Registry on 8724 patients. Injury 2007, 38, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Brohi, K.; Singh, J.; Heron, M.; Coats, T. Acute traumatic coagulopathy. J. Trauma 2003, 54, 1127–1130. [Google Scholar] [CrossRef] [PubMed]
- MacLeod, J.B.; Lynn, M.; McKenney, M.G.; Cohn, S.M.; Murtha, M. Early coagulopathy predicts mortality in trauma. J. Trauma 2003, 55, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Schochl, H.; Nienaber, U.; Maegele, M.; Hochleitner, G.; Primavesi, F.; Steitz, B.; Arndt, C.; Hanke, A.; Voelckel, W.; Solomon, C. Transfusion in trauma: Thromboelastometry-guided coagulation factor concentrate-based therapy versus standard fresh frozen plasma-based therapy. Crit. Care 2011, 15, R83. [Google Scholar] [CrossRef] [PubMed]
- Schochl, H.; Frietsch, T.; Pavelka, M.; Jambor, C. Hyperfibrinolysis after major trauma: Differential diagnosis of lysis patterns and prognostic value of thrombelastometry. J. Trauma 2009, 67, 125–131. [Google Scholar] [CrossRef]
- Maegele, M.; Schochl, H.; Cohen, M.J. An update on the coagulopathy of trauma. Shock 2014, 41 (Suppl. 1), 21–25. [Google Scholar] [CrossRef]
- Khan, S.; Davenport, R.; Raza, I.; Glasgow, S.; De’Ath, H.D.; Johansson, P.I.; Curry, N.; Stanworth, S.; Gaarder, C.; Brohi, K. Damage control resuscitation using blood component therapy in standard doses has a limited effect on coagulopathy during trauma hemorrhage. Intensive Care Med. 2015, 41, 239–247. [Google Scholar] [CrossRef]
- Curry, N.; Hopewell, S.; Doree, C.; Hyde, C.; Brohi, K.; Stanworth, S. The acute management of trauma hemorrhage: A systematic review of randomized controlled trials. Crit. Care 2011, 15, R92. [Google Scholar] [CrossRef]
- Rossaint, R.; Bouillon, B.; Cerny, V.; Coats, T.J.; Duranteau, J.; Fernandez-Mondejar, E.; Filipescu, D.; Hunt, B.J.; Komadina, R.; Nardi, G.; et al. The European guideline on management of major bleeding and coagulopathy following trauma: Fourth edition. Crit. Care 2016, 20, 100. [Google Scholar] [CrossRef]
- American College of Surgeons. Advanced Trauma Life Support (ATLS®), 10th ed.; American College of Surgeons: Chicago, IL, USA, 2018. [Google Scholar]
- Derakhshanfar, H.; Vafaei, A.; Tabatabaey, A.; Noori, S. Prevalence and Associated Factors of Acute Traumatic Coagulopathy; a Cross Sectional Study. Emergency 2017, 5, e58. [Google Scholar] [PubMed]
- Raysi Dehcordi, S.; Ricci, A.; Di Vitantonio, H.; De Paulis, D.; Luzzi, S.; Palumbo, P.; Cinque, B.; Tempesta, D.; Coletti, G.; Cipolloni, G.; et al. Stemness Marker Detection in the Periphery of Glioblastoma and Ability of Glioblastoma to Generate Glioma Stem Cells: Clinical Correlations. World Neurosurg. 2017, 105, 895–905. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.Y.; Shetty, R.; Sekhar, L.N. Microsurgical Resection of a Large Intraventricular Trigonal Tumor: 3-Dimensional Operative Video. Oper. Neurosurg. 2018, 15, E92–E93. [Google Scholar] [CrossRef]
- Luzzi, S.; Crovace, A.M.; Lacitignola, L.; Valentini, V.; Francioso, E.; Rossi, G.; Invernici, G.; Galzio, R.J.; Crovace, A. Engraftment, neuroglial transdifferentiation and behavioral recovery after complete spinal cord transection in rats. Surg. Neurol. Int. 2018, 9, 19. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, P.; Lombardi, F.; Siragusa, G.; Dehcordi, S.R.; Luzzi, S.; Cimini, A.; Cifone, M.G.; Cinque, B. Involvement of NOS2 Activity on Human Glioma Cell Growth, Clonogenic Potential, and Neurosphere Generation. Int. J. Mol. Sci. 2018, 19, 2801. [Google Scholar] [CrossRef]
- Zoia, C.; Bongetta, D.; Guerrini, F.; Alicino, C.; Cattalani, A.; Bianchini, S.; Galzio, R.J.; Luzzi, S. Outcome of elderly patients undergoing intracranial meningioma resection: A single center experience. J. Neurosurg. Sci. 2018. [Google Scholar] [CrossRef]
- Bellantoni, G.; Guerrini, F.; Del Maestro, M.; Galzio, R.; Luzzi, S. Simple schwannomatosis or an incomplete Coffin-Siris? Report of a particular case. eNeurologicalSci 2019, 14, 31–33. [Google Scholar] [CrossRef]
- Luzzi, S.; Crovace, A.M.; Del Maestro, M.; Giotta Lucifero, A.; Elbabaa, S.K.; Cinque, B.; Palumbo, P.; Lombardi, F.; Cimini, A.; Cifone, M.G.; et al. The cell-based approach in neurosurgery: Ongoing trends and future perspectives. Heliyon 2019, 5, e02818. [Google Scholar] [CrossRef]
- Luzzi, S.; Elia, A.; Del Maestro, M.; Elbabaa, S.K.; Carnevale, S.; Guerrini, F.; Caulo, M.; Morbini, P.; Galzio, R. Dysembryoplastic Neuroepithelial Tumors: What You Need to Know. World Neurosurg. 2019, 127, 255–265. [Google Scholar] [CrossRef]
- Luzzi, S.; Giotta Lucifero, A.; Del Maestro, M.; Marfia, G.; Navone, S.E.; Baldoncini, M.; Nunez, M.; Campero, A.; Elbabaa, S.K.; Galzio, R. Anterolateral Approach for Retrostyloid Superior Parapharyngeal Space Schwannomas Involving the Jugular Foramen Area: A 20-Year Experience. World Neurosurg. 2019, 132, e40–e52. [Google Scholar] [CrossRef]
- Palumbo, P.; Lombardi, F.; Augello, F.R.; Giusti, I.; Luzzi, S.; Dolo, V.; Cifone, M.G.; Cinque, B. NOS2 inhibitor 1400W Induces Autophagic Flux and Influences Extracellular Vesicle Profile in Human Glioblastoma U87MG Cell Line. Int. J. Mol. Sci. 2019, 20, 3010. [Google Scholar] [CrossRef] [PubMed]
- Spena, G.; Roca, E.; Guerrini, F.; Panciani, P.P.; Stanzani, L.; Salmaggi, A.; Luzzi, S.; Fontanella, M. Risk factors for intraoperative stimulation-related seizures during awake surgery: An analysis of 109 consecutive patients. J. Neurooncol. 2019, 145, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Antonosante, A.; Brandolini, L.; d’Angelo, M.; Benedetti, E.; Castelli, V.; Maestro, M.D.; Luzzi, S.; Giordano, A.; Cimini, A.; Allegretti, M. Autocrine CXCL8-dependent invasiveness triggers modulation of actin cytoskeletal network and cell dynamics. Aging (Albany NY) 2020, 12, 1928–1951. [Google Scholar] [CrossRef] [PubMed]
- Campanella, R.; Guarnaccia, L.; Cordiglieri, C.; Trombetta, E.; Caroli, M.; Carrabba, G.; La Verde, N.; Rampini, P.; Gaudino, C.; Costa, A.; et al. Tumor-Educated Platelets and Angiogenesis in Glioblastoma: Another Brick in the Wall for Novel Prognostic and Targetable Biomarkers, Changing the Vision from a Localized Tumor to a Systemic Pathology. Cells 2020, 9, 294. [Google Scholar] [CrossRef] [PubMed]
- Zoia, C.; Lombardi, F.; Fiore, M.R.; Montalbetti, A.; Iannalfi, A.; Sansone, M.; Bongetta, D.; Valvo, F.; Del Maestro, M.; Luzzi, S.; et al. Sacral solitary fibrous tumour: Surgery and hadrontherapy, a combined treatment strategy. Rep. Pract. Oncol. Radiother. 2020, 25, 241–244. [Google Scholar] [CrossRef]
- Elsawaf, Y.; Anetsberger, S.; Luzzi, S.; Elbabaa, S.K. Early Decompressive Craniectomy as Management for Severe TBI in the Pediatric Population: A Comprehensive Literature Review. World Neurosurg. 2020. [Google Scholar] [CrossRef]
- Hess, J.R.; Brohi, K.; Dutton, R.P.; Hauser, C.J.; Holcomb, J.B.; Kluger, Y.; Mackway-Jones, K.; Parr, M.J.; Rizoli, S.B.; Yukioka, T.; et al. The coagulopathy of trauma: A review of mechanisms. J. Trauma 2008, 65, 748–754. [Google Scholar] [CrossRef]
- Brohi, K. Trauma induced coagulopathy. J. R. Army Med. Corps 2009, 155, 320–322. [Google Scholar] [CrossRef]
- Johansson, P.I.; Sorensen, A.M.; Perner, A.; Welling, K.L.; Wanscher, M.; Larsen, C.F.; Ostrowski, S.R. Disseminated intravascular coagulation or acute coagulopathy of trauma shock early after trauma? An observational study. Crit. Care 2011, 15, R272. [Google Scholar] [CrossRef]
- Frith, D.; Brohi, K. The pathophysiology of trauma-induced coagulopathy. Curr. Opin. Crit. Care 2012, 18, 631–636. [Google Scholar] [CrossRef]
- Hagemo, J.S.; Christiaans, S.C.; Stanworth, S.J.; Brohi, K.; Johansson, P.I.; Goslings, J.C.; Naess, P.A.; Gaarder, C. Detection of acute traumatic coagulopathy and massive transfusion requirements by means of rotational thromboelastometry: An international prospective validation study. Crit. Care 2015, 19, 97. [Google Scholar] [CrossRef] [PubMed]
- Hagemo, J.S.; Stanworth, S.; Juffermans, N.P.; Brohi, K.; Cohen, M.; Johansson, P.I.; Roislien, J.; Eken, T.; Naess, P.A.; Gaarder, C. Prevalence, predictors and outcome of hypofibrinogenaemia in trauma: A multicentre observational study. Crit. Care 2014, 18, R52. [Google Scholar] [CrossRef] [PubMed]
- Brohi, K.; Cohen, M.J.; Ganter, M.T.; Schultz, M.J.; Levi, M.; Mackersie, R.C.; Pittet, J.F. Acute coagulopathy of trauma: Hypoperfusion induces systemic anticoagulation and hyperfibrinolysis. J. Trauma 2008, 64, 1211–1217. [Google Scholar] [CrossRef]
- Rugeri, L.; Levrat, A.; David, J.S.; Delecroix, E.; Floccard, B.; Gros, A.; Allaouchiche, B.; Negrier, C. Diagnosis of early coagulation abnormalities in trauma patients by rotation thrombelastography. J. Thromb. Haemost. 2007, 5, 289–295. [Google Scholar] [CrossRef]
- Hess, J.R.; Lawson, J.H. The coagulopathy of trauma versus disseminated intravascular coagulation. J. Trauma 2006, 60, S12–S19. [Google Scholar] [CrossRef] [PubMed]
- Spahn, D.R.; Rossaint, R. Coagulopathy and blood component transfusion in trauma. Br. J. Anaesth. 2005, 95, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Hussmann, B.; Lefering, R.; Waydhas, C.; Touma, A.; Kauther, M.D.; Ruchholtz, S.; Lendemans, S.; Trauma Registry of the German Society for Trauma Surgery. Does increased prehospital replacement volume lead to a poor clinical course and an increased mortality? A matched-pair analysis of 1896 patients of the Trauma Registry of the German Society for Trauma Surgery who were managed by an emergency doctor at the accident site. Injury 2013, 44, 611–617. [Google Scholar] [CrossRef]
- Frith, D.; Davenport, R.; Brohi, K. Acute traumatic coagulopathy. Curr. Opin. Anaesthesiol. 2012, 25, 229–234. [Google Scholar] [CrossRef]
- Spivey, M.; Parr, M.J. Therapeutic approaches in trauma-induced coagulopathy. Minerva Anestesiol. 2005, 71, 281–289. [Google Scholar]
- Millimaggi, D.F.; Norcia, V.D.; Luzzi, S.; Alfiero, T.; Galzio, R.J.; Ricci, A. Minimally Invasive Transforaminal Lumbar Interbody Fusion with Percutaneous Bilateral Pedicle Screw Fixation for Lumbosacral Spine Degenerative Diseases. A Retrospective Database of 40 Consecutive Cases and Literature Review. Turk. Neurosurg. 2018, 28, 454–461. [Google Scholar] [CrossRef]
- Bongetta, D.; Zoia, C.; Luzzi, S.; Maestro, M.D.; Peri, A.; Bichisao, G.; Sportiello, D.; Canavero, I.; Pietrabissa, A.; Galzio, R.J. Neurosurgical issues of bariatric surgery: A systematic review of the literature and principles of diagnosis and treatment. Clin. Neurol. Neurosurg. 2019, 176, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Pisano, P.; Guerrini, F.; Custodi, V.; Del Maestro, M.; Galzio, R.; Luzzi, S. Tonic-clonic seizures as a possible complication for cerebrospinal fluid leakage after intradural spinal surgery, a case report. Interdiscip. Neurosurg. Adv. Tech. Case Manag. 2020, 19, 100576. [Google Scholar] [CrossRef]
- Floccard, B.; Rugeri, L.; Faure, A.; Saint Denis, M.; Boyle, E.M.; Peguet, O.; Levrat, A.; Guillaume, C.; Marcotte, G.; Vulliez, A.; et al. Early coagulopathy in trauma patients: An on-scene and hospital admission study. Injury 2012, 43, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Mitra, B.; Cameron, P.A.; Mori, A.; Fitzgerald, M. Acute coagulopathy and early deaths post major trauma. Injury 2012, 43, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Dick, W.F.; Baskett, P.J. Recommendations for uniform reporting of data following major trauma--the Utstein style. A report of a working party of the International Trauma Anaesthesia and Critical Care Society (ITACCS). Resuscitation 1999, 42, 81–100. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physiological Criteria | Anatomical Criteria | Dynamic Criteria |
|---|---|---|
| Eject from the vehicle | Penetrating head/neck/throat/abdomen/pelvic/armpit/groin trauma | Systolic blood pressure <90 mmHg |
| Motorcyclist thrown from the vehicle | Amputations above the wrist or ankle | Respiratory or breathlessness rate <10 or >29 acts/min |
| Died in the same vehicle | Chest trauma with flap/costal volet | State of consciousness (GCS) <13 |
| Intruding of the cockpit >30 cm | Neurological injury with paralysis of even a single limb | |
| Fall from height >2 m | Fractures of two or more subxinextising bones | |
| Pedestrian projected or rolled or hit at speed >10 km/h | Suspected unstable fracture king of pelvis: Suspected unstable fracture | |
| High-energy impact (speed >65 km/h) | Skull fracture scuttled | |
| Vehicle coat | Burn >20% of body surface or airway/face | |
| Extrication time >20 min |
| Coagulopathy | Non-Coagulopathy | |
|---|---|---|
| ISS >15 | 21.26% | 15.7% |
| MSI >1.3 | 9.8% | 4.76% |
| ASI >50 | 7.84% | 5.49% |
| Coagulopathy | Non-Coagulopathy | ||
|---|---|---|---|
| % Hospitalization | 76% | 58% | p = 0.016 |
| % ICU | 22% | 14.8% | |
| ICU Stay (day) | 12.5% | 9.8% | |
| % Operation theatre | 19.2% | 17.2% | |
| Intrahospital mortality | 3.92% | 0.98% |
| Coagulopathy | Non-Coagulopathy | |
|---|---|---|
| pH <7.35 | 5.5% | 1.32% |
| % ICU | 29.5% | 2.32% |
| ICU Stay (day) | 1.97% | 0% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savioli, G.; Ceresa, I.F.; Macedonio, S.; Gerosa, S.; Belliato, M.; Iotti, G.A.; Luzzi, S.; Del Maestro, M.; Mezzini, G.; Giotta Lucifero, A.; et al. Trauma Coagulopathy and Its Outcomes. Medicina 2020, 56, 205. https://doi.org/10.3390/medicina56040205
Savioli G, Ceresa IF, Macedonio S, Gerosa S, Belliato M, Iotti GA, Luzzi S, Del Maestro M, Mezzini G, Giotta Lucifero A, et al. Trauma Coagulopathy and Its Outcomes. Medicina. 2020; 56(4):205. https://doi.org/10.3390/medicina56040205
Chicago/Turabian StyleSavioli, Gabriele, Iride Francesca Ceresa, Sarah Macedonio, Sebastiano Gerosa, Mirko Belliato, Giorgio Antonio Iotti, Sabino Luzzi, Mattia Del Maestro, Gianluca Mezzini, Alice Giotta Lucifero, and et al. 2020. "Trauma Coagulopathy and Its Outcomes" Medicina 56, no. 4: 205. https://doi.org/10.3390/medicina56040205
APA StyleSavioli, G., Ceresa, I. F., Macedonio, S., Gerosa, S., Belliato, M., Iotti, G. A., Luzzi, S., Del Maestro, M., Mezzini, G., Giotta Lucifero, A., Lafe, E., Simoncelli, A., Manzoni, F., Cobianchi, L., Mosconi, M., Cuzzocrea, F., Benazzo, F., Ricevuti, G., & Bressan, M. A. (2020). Trauma Coagulopathy and Its Outcomes. Medicina, 56(4), 205. https://doi.org/10.3390/medicina56040205