Factors that Decrease Sedentary Behavior in Community-Dwelling Elderly People: A Longitudinal Study


Abstract
1. Introduction
2. Materials and Methods
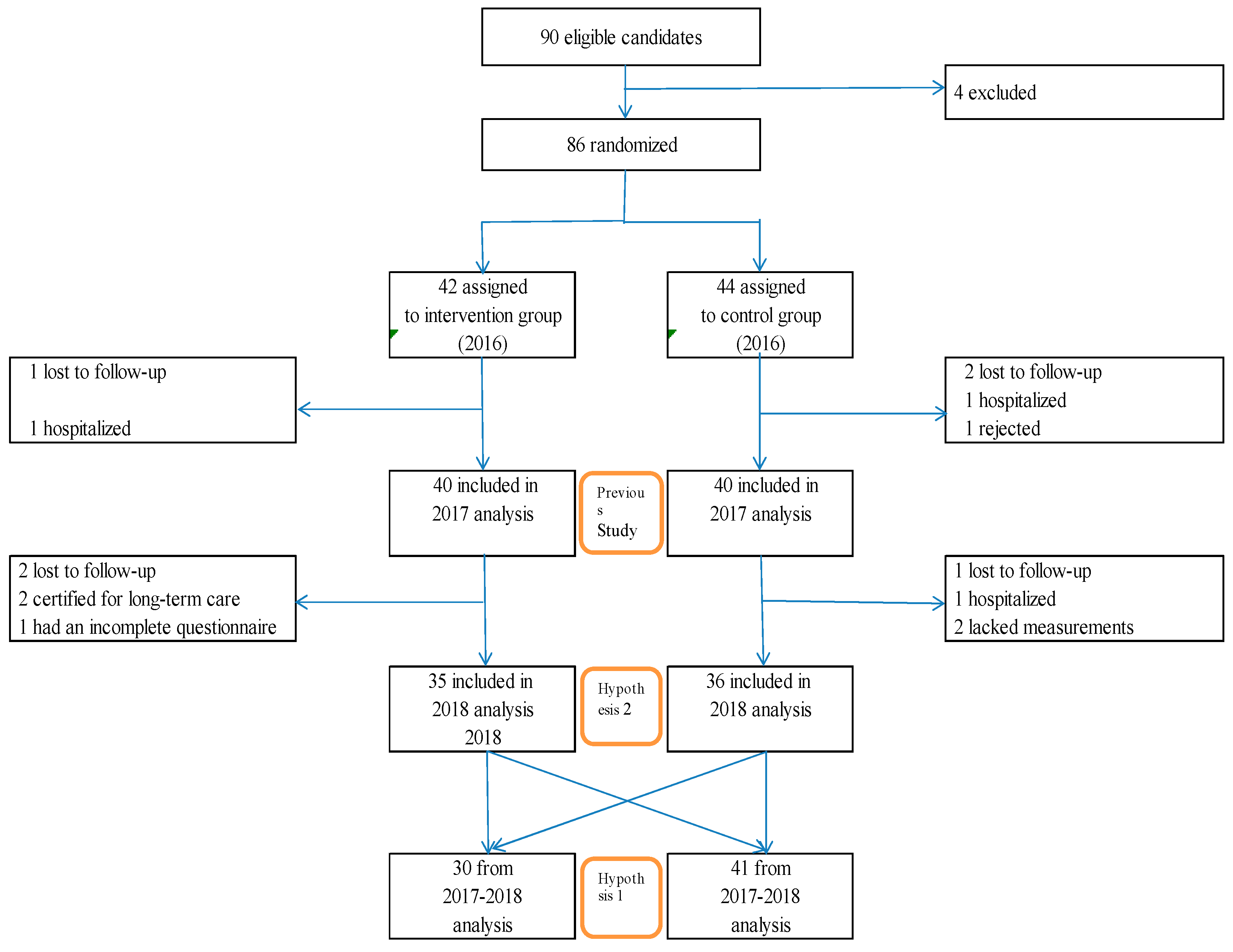
2.1. Study Design
2.2. Participants and Data Collection
2.3. Assessment of Factors
2.3.1. Basic Attributes
2.3.2. Health Class
2.3.3. Physical Activity
2.3.4. Active Guide
2.3.5. Hypothesis 1 Methods
2.3.6. Hypothesis 2 Methods
2.3.7. Previous Study Methods
2.4. Statistical Analyses
2.5. Ethical Consideration
3. Results
3.1. Hypothesis 1 Results
3.2. Hypothesis 2 Results
3.3. Previous Results
4. Discussion
4.1. Hypothesis 1
4.2. Hypothesis 2
4.3. Previous Study 3
5. Conclusions
Funding
Conflicts of Interest
References
- Bauman, A.; Ainsworth, B.E.; Sallis, J.F.; Hagströmer, M.; Craig, C.L.; Bull, F.C.; Pratt, M.; Venugopal, K.; Chau, J.; Sjöström, M.; et al. The descriptive epidemiology of sitting: A 20-country comparison using the International Physical Activity Questionnaire (IPAQ). Am. J. Prev. Med. 2011, 41, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Honda, T.; Chen, S.; Kishimoto, H.; Narazaki, K.; Kumagai, S. Identufying associations between sedentary time and cardio-metabolic risk factors in working adults using objective and subjective measures a cross-sectional analysis. BMC Public Health 2014, 14, 1307. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Clark, B.K.; Winkler, E.A.; Gardiner, P.A.; Brown, W.J.; Matthews, C.E. Measurement of adults’ sedentary time in population-based studies. Am. J. Prev. Med. 2011, 41, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too Much Sitting: The Population-Health Science of Sedentary Behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Sedentary Behavior Research Network. Standardized use of the terms “sedentary” and “sedentary behaviours”. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542. [Google Scholar] [CrossRef]
- Kesse-Guyot, E.; Charreire, H.; Andreeva, V.A.; Touvier, M.; Hercberg, S.; Galan, P.; Oppert, J.M. Cross-sectional and longitudinal associations of different sedentary behaviors with cognitive performance in older adults. PLoS ONE 2012, 7, e47831. [Google Scholar] [CrossRef]
- Pavey, T.G.; Peeters, G.G.; Brown, W.J. Sitting-time and 9-year all-cause mortality in older women. Br. J. Sports Med. 2015, 49, 95–99. [Google Scholar] [CrossRef]
- León-Muñoz, L.M.; Martínez-Gómez, D.; Balboa-Castillo, T.; López-García, E.; Guallar-Castillón, P.; Rodríguez-Artalejo, F. Continued sedentariness, change in sitting time, and mortality in older adults. Med. Sci. Sports Exerc. 2013, 45, 1501–1507. [Google Scholar] [CrossRef]
- Martínez-Gómez, D.; Guallar-Castillón, P.; León-Muñoz, L.M.; López-García, E.; Rodríguez-Artalejo, F. Combined impact of traditional and non-traditional health behaviors on mortality: A national prospective cohort study in Spanish older adults. BMC Med. 2013, 22, 47. [Google Scholar] [CrossRef]
- Van der Ploeg, H.P.; Chey, T.; Korda, R.J.; Banks, E.; Bauman, A. Sitting time and all-cause mortality risk in 222 497 Australian adults. Arc. Intern. Med. 2012, 172, 494–500. [Google Scholar] [CrossRef]
- Geda, Y.E.; Silber, T.C.; Roberts, R.O.; Knopman, D.S.; Christianson, T.J.; Pankratz, V.S.; Boeve, B.F.; Tangalos, E.G.; Petersen, R.C. Computer activities, physical exercise, aging, and mild cognitive impairment: A population-based study. Mayo Clin. Proc. 2012, 87, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Siddarth, P.; Burggren, A.C.; Eyre, H.A.; Small, G.W.; Merrill, D.A. Sedentary behavior associated with reduced medial temporal lobe thickness in middle-aged and older adults. PLoS ONE 2018, 13, e0195549. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare. 2018 White Paper on Aging Society (Whole Version). Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2018/html/zenbun/s1_1_1.html (accessed on 1 March 2020). (In Japanese)
- Rosenberg, D.E.; Norman, G.J.; Wagner, N.; Patrick, K.; Calfas, K.J.; Sallis, J.F. Reliability and validity of the sedentary behavior questionnaire (SBQ) for adults. J. Phys. Act. Health 2010, 7, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, P.A.; Eakin, E.G.; Healy, G.N.; Owen, N. Feasibility of reducing older adults’ sedentary time. Am. J. Prev. Med. 2011, 41, 174–177. [Google Scholar] [CrossRef]
- Fitzsimons, C.F.; Kirk, A.; Baker, G.; Michie, F.; Kane, C.; Mutrie, N. Using an individualised consultation and activPAL™ feedback to reduce sedentary time in older Scottish adults: Results of a feasibility and pilot study. Prev. Med. 2013, 57, 718–720. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, H.; Inoue, S.; Sugiyama, T.; Owen, N.; Oka, K.; Nakaya, T.; Shimomitsu, T. Distinct associations of different sedentary behaviors with health-related attributes among older adults. Prev. Med. 2014, 67, 335–339. [Google Scholar] [CrossRef]
- Miyachi, M.; Tripette, J.; Kawakami, R.; Murakami, H. “+10 min of Physical Activity per Day”: Japan Is Looking for Efficient but Feasible Recommendations for Its Population. J. Nutr. Sci. Vitaminol. 2015, 61, S7–S9. [Google Scholar] [CrossRef]
- Owari, Y.; Suzuki, H.; Miyatake, N. “Active Guide” Brochure Reduces Sedentary Behavior of Elderly People: A Randomized Controlled Trial. Acta Med. Okayama 2019, 73, 427–432. [Google Scholar]
- Owari, Y.; Miyatake, N.; Kataoka, H. Relationship between social participation, physical activity and psychological distress in apparently healthy elderly people: A pilot study. Acta Med. Okayama 2018, 72, 31–37. [Google Scholar]
- Oshima, Y.; Kawaguchi, K.; Tanaka, S.; Ohkawara, K.; Hikihara, Y.; Ishikawa-Takata, K.; Tabata, I. Classifying household and locomotive activities using a triaxial accelerometer. Gait Posture 2010, 31, 370–374. [Google Scholar] [CrossRef]
- Ohkawara, K.; Oshima, Y.; Hikihara, Y.; Ishikawa-Takata, K.; Tabata, I.; Tanaka, S. Real-time estimation of daily physical activity intensity by a triaxial accelerometer and a gravity-removal classification algorithm. Br. J. Nutr. 2011, 105, 1681–1691. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Ishikawa-Takata, K.; Tanaka, S.; Bessyo, K.; Tanaka, S.; Kimura, T. Accuracy of Estimating Step Counts and Intensity Using Accelerometers in Older People with or Without Assistive Devices. J. Aging Phys. Act. 2017, 25, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, H.; Inoue, S.; Fukushima, N.; Takamiya, T.; Odagiri, Y.; Ohya, Y.; Amagasa, S.; Oka, K.; Owen, N. Social participation among older adults not engaged in full- or part-time work is associated with more physical activity and less sedentary time. Geriatr. Gerontol. Int. 2017, 17, 1921–1927. [Google Scholar] [CrossRef]
- Honda, T.; Chen, S.; Yonemoto, K.; Kishimoto, H.; Chen, T.; Narazaki, K.; Haeuchi, Y.; Kumagai, S. Sedentary bout durations and metabolic syndrome among working adults: A prospective cohort study. BMC Public Health 2016, 16, 888. [Google Scholar] [CrossRef] [PubMed]
- Berkman, L.F.; Kawachi, I.; Glymour, M.M. (Eds.) Social Epidemiology, 2nd ed.; Oxford University Press: Oxford, UK, 2014. [Google Scholar]


{kind=link}
| Intervention Group | Control Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | ± | SD | Minimum | Maximum | Mean | ± | SD | Minimum | Maximum | P | |
| Number of subjects | 40 (12 men, 28 women) | 40 (12 men, 28 women) | |||||||||
| Age (years) | 72.6 | ± | 5.5 | 65 | 85 | 71.1 | ± | 5.5 | 65 | 85 | 0.197 |
| BMI (kg/m2) | 21.8 | ± | 2.6 | 14.9 | 26.7 | 23.5 | ± | 2.7 | 18.7 | 29.1 | <0.001 |
| Exercise (METs h/w) | 5.1 | ± | 2.2 | 0.4 | 9.7 | 5.2 | ± | 2.2 | 1.6 | 9.7 | 0.800 |
| Number of steps (steps/d) | 5728.2 | ± | 2818 | 569.9 | 12,230.1 | 5746.5 | ± | 2339 | 1585.4 | 10,915.9 | 0.975 |
| Walking time (minutes/d) | 83.2 | ± | 38.3 | 20.9 | 177.7 | 87.4 | ± | 26.9 | 31.3 | 146.7 | 0.572 |
| ≤1.5 METs (%/d) | 54.9 | ± | 9.7 | 35.4 | 75.5 | 55.2 | ± | 10.2 | 38.3 | 79.9 | 0.856 |
| 1.6~2.9 METs (%/d) | 35.5 | ± | 7.0 | 19.4 | 49.0 | 34.9 | ± | 8.5 | 16.9 | 52.3 | 0.719 |
| 3~5.9 METs (%/d) | 8.9 | ± | 3.9 | 2.8 | 17.0 | 9.2 | ± | 3.5 | 0.8 | 15.6 | 0.831 |
| Group A | Group B | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | ± | SD | Minimum | Maximum | Mean | ± | SD | Minimum | Maximum | P | |
| Number of subjects | 30 (8 men, 22 women) | 41 (14 men, 27 women) | |||||||||
| Age (years) | 74.2 | ± | 5.9 | 67 | 87 | 73.7 | ± | 5.2 | 67 | 87 | 0.696 |
| BMI (kg/m2) | 22.6 | ± | 2.7 | 17.4 | 26.4 | 22.7 | ± | 2.9 | 14.9 | 26.8 | 0.878 |
| Exercise (METs h/w) | 4.8 | ± | 2.2 | 1.6 | 9.7 | 5.9 | ± | 2.9 | 1.3 | 9.6 | 0.078 |
| Number of steps (steps/d) | 5751.6 | ± | 2639.2 | 1374.9 | 11,291.0 | 6460.0 | ± | 3001.9 | 985.4 | 13,973.3 | 0.305 |
| Walking time (min/d) | 79.7 | ± | 31.5 | 38.6 | 167.4 | 92.6 | ± | 41.2 | 20.9 | 177.7 | 0.157 |
| ≤1.5 METs (%/d) | 47.9 | ± | 10.0 | 30.2 | 66.9 | 52.7 | ± | 14.2 | 23.8 | 83.5 | 0.160 |
| Changes in ≤1.5 METs (%/d) | −6.7 | ± | 8.0 | −23.6 | 11.2 | −2.4 | ± | 7.0 | −23.4 | 13.6 | 0.041 |
| 1.6~2.9 METs (%/d) | 35.5 | ± | 6.9 | 18.9 | 14.7 | 34.4 | ± | 8.4 | 13.1 | 28.7 | 0.373 |
| Changes in 1.6~2.9 METs (%/d) | 6.4 | ± | 5.8 | −9.3 | 14.7 | 5.3 | ± | 7.7 | −10.9 | 28.7 | 0.486 |
| 3~5.9 METs (%/d) | 8.4 | ± | 3.5 | 2.8 | 15.2 | 8.9 | ± | 4.7 | 2.9 | 22.5 | 0.622 |
| Changes in 3~5.9 METs (%/d) | 2.0 | ± | 4.9 | −1.8 | 1.3 | 3.4 | ± | 3.0 | −1.6 | 1.2 | 0.147 |
| Intervention Group | Control Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | ± | SD | Minimum | Maximum | Mean | ± | SD | Minimum | Maximum | P | |
| Number of subjects | 35 (12 men, 23 women) | 36 (10 men, 26 women) | |||||||||
| Age (years) | 73.5 | ± | 5.7 | 67 | 87 | 74.3 | ± | 5.3 | 67 | 87 | 0.613 |
| BMI (kg/m2) | 22.7 | ± | 2.7 | 14.9 | 26.8 | 22.6 | ± | 2.5 | 14.9 | 26.6 | 0.980 |
| Exercise (METs h/w) | 5.3 | ± | 2.3 | 1.6 | 9.7 | 5.2 | ± | 2.2 | 1.8 | 9.7 | 0.886 |
| Number of steps (steps/d) | 5728.1 | ± | 2395.4 | 1585.4 | 10,915.9 | 5916.0 | ± | 2824.6 | 923.7 | 12,230.1 | 0.764 |
| Walking time (min/d) | 88.3 | ± | 27.9 | 31.3 | 146.7 | 85.6 | ± | 38.9 | 20.9 | 177.7 | 0.739 |
| ≤1.5 METs (%/d) | 50.7 | ± | 12.8 | 30.2 | 73.1 | 50.6 | ± | 14.4 | 23.8 | 83.5 | 0.872 |
| Changes in ≤1.5 METs (%/d) | −2.1 | ± | 8.2 | −23.6 | 11.2 | −7.0 | ± | 10.9 | −50.4 | 13.6 | 0.034 |
| 1.6~2.9 METs (%/d) | 42.8 | ± | 12.4 | 22.9 | 18.4 | 43.8 | ± | 11.6 | 13.1 | 28.7 | 0.117 |
| Changes in 1.6~2.9 METs (%/d) | 6.4 | ± | 7.7 | −3.4 | 14.7 | 10.1 | ± | 9.7 | −10.9 | 22.5 | 0.041 |
| 3~5.9 METs (%/d) | 8.8 | ± | 4.1 | 2.8 | 17.0 | 10.6 | ± | 4.5 | 4.1 | 22.5 | 0.094 |
| Changes in 3~5.9 METs (%/d) | −1.5 | ± | 2.2 | −0.4 | 0.2 | 2.1 | ± | 2.6 | −1.8 | 1.3 | 0.044 |
| Intervention Group | Control Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | ± | SD | Minimum | Maximum | Mean | ± | SD | Minimum | Maximum | P | |
| Number of subjects | 40 (12 men, 28 women) | 40 (12 men, 28 women) | |||||||||
| Age (years) | |||||||||||
| BMI (kg/m2) | 21.9 | ± | 2.7 | 14.9 | 26.7 | 23.3 | ± | 2.6 | 19.1 | 29.1 | <0.001 |
| Exercise (METs h/w) | 5.5 | ± | 2.8 | 0.5 | 10.9 | 5.0 | ± | 2.5 | 0.9 | 10.7 | 0.340 |
| Number of steps (steps/d) | 6138.5 | ± | 3188 | 845.1 | 13,973.3 | 5784.3 | ± | 2503 | 985.4 | 11,291.0 | 0.582 |
| Walking time (minutes/d) | 87.3 | ± | 42.8 | 32.7 | 192.1 | 84.3 | ± | 31.5 | 38.6 | 167.4 | 0.717 |
| ≤1.5 METs (%/d) | 52.7 | ± | 10.9 | 35.4 | 75.5 | 57.7 | ± | 9.8 | 36.5 | 74.3 | 0.033 |
| Changes in ≤1.5 METs (%/d) | −2.2 | ± | 5.9 | 16.6 | 8.0 | 2.5 | ± | 8.8 | −8.6 | 23.3 | 0.007 |
| 1.6~2.9 METs (%/d) | 36.4 | ± | 8.0 | 19.4 | 49.0 | 33.7 | ± | 7.4 | 19.6 | 47.4 | 0.117 |
| Changes in 1.6~2.9 METs (%/d) | 0.9 | ± | 4.1 | 2.6 | −1.9 | −1.2 | ± | 6.3 | −2.4 | 1.1 | 0.098 |
| 3~5.9 METs (%/d) | 10.3 | ± | 4.6 | 2.8 | 17.0 | 8.5 | ± | 4.0 | 1.9 | 15.8 | 0.067 |
| Changes in 3~5.9 METs (%/d) | 1.4 | ± | 2.2 | −0.4 | 0.2 | −0.7 | ± | 1.9 | −1.8 | 1.3 | 0.061 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owari, Y. Factors that Decrease Sedentary Behavior in Community-Dwelling Elderly People: A Longitudinal Study. Medicina 2020, 56, 157. https://doi.org/10.3390/medicina56040157
Owari Y. Factors that Decrease Sedentary Behavior in Community-Dwelling Elderly People: A Longitudinal Study. Medicina. 2020; 56(4):157. https://doi.org/10.3390/medicina56040157
Chicago/Turabian StyleOwari, Yutaka. 2020. "Factors that Decrease Sedentary Behavior in Community-Dwelling Elderly People: A Longitudinal Study" Medicina 56, no. 4: 157. https://doi.org/10.3390/medicina56040157
APA StyleOwari, Y. (2020). Factors that Decrease Sedentary Behavior in Community-Dwelling Elderly People: A Longitudinal Study. Medicina, 56(4), 157. https://doi.org/10.3390/medicina56040157