Estimation of Caries Treatment Needs in First Permanent Molars of Lithuanian 5–6-Year-Old Children, Based on Caries Lesion Activity Assessment



Abstract
1. Introduction
2. Materials and Methods
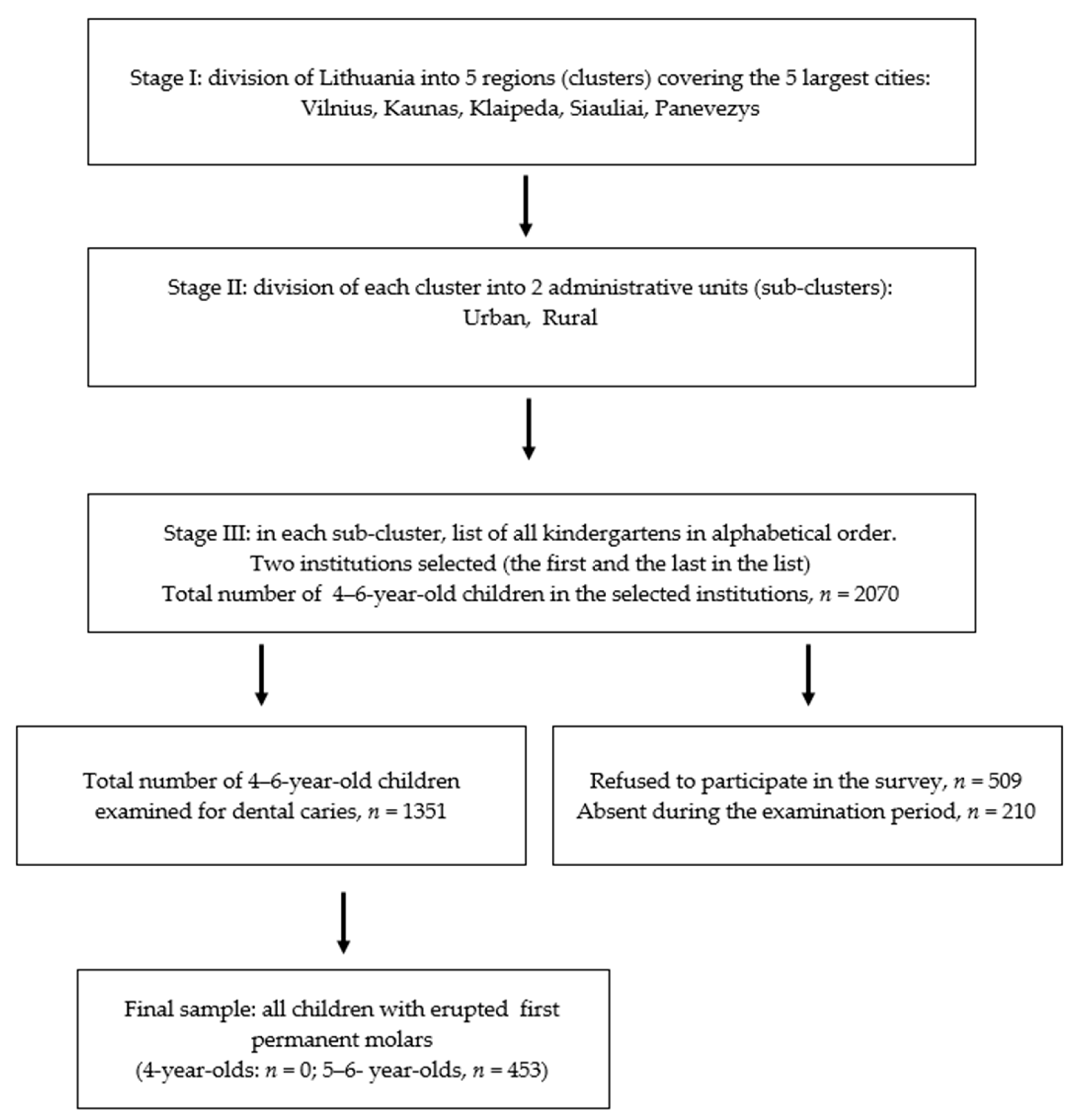
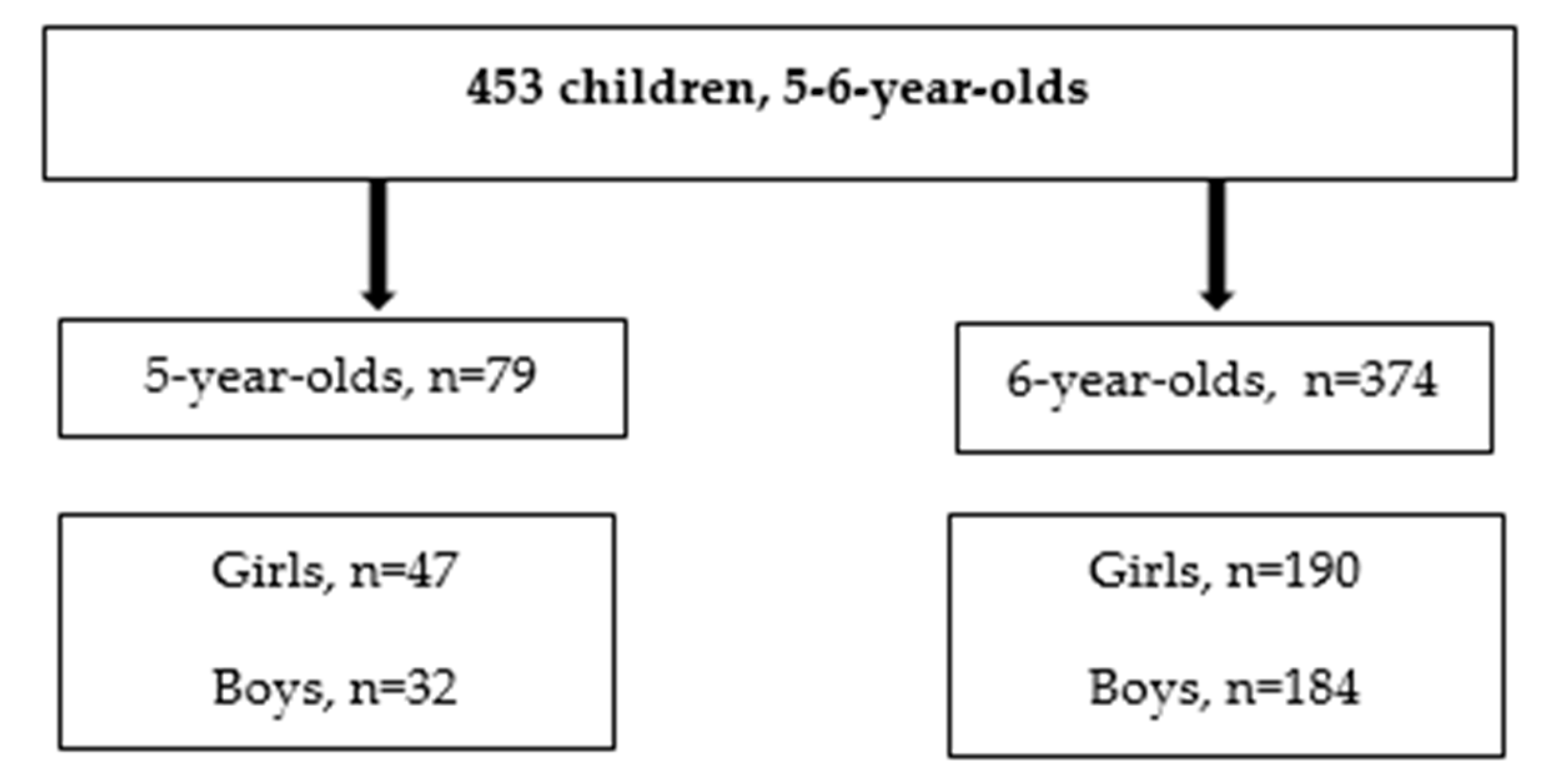
2.1. Study Design, Population and Sample Selection
2.2. Clinical Examinations
- 0.
- sound surface,
- 1.
- active noncavitated lesion,
- 2.
- active enamel microcavity,
- 3.
- active enamel and dentin cavity,
- 4.
- inactive noncavitated lesion,
- 5.
- inactive enamel microcavity,
- 6.
- inactive enamel and dentin cavity,
- 7.
- filling,
- 8.
- filling + active lesion (noncavitated or cavitated),
- 9.
- filling + inactive lesion (noncavitated or cavitated),
- 10.
- tooth extracted due to caries.
- 11.
- no plaque,
- 12.
- film of plaque adhering to the free gingival margin and adjacent area of the tooth,
- 13.
- moderate accumulation of soft deposits on the tooth surface and gingival margin, which could be seen with the naked eye, and
- 14.
- plaque covering entire surface of the tooth.
2.3. Collection of Nonclinical Data
- regular toothbrushing, 2 times per day,
- regular toothbrushing, once per day,
- irregular toothbrushing (several times per week), and
- no toothbrushing at all.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
Consent for Publication
References
- Fejerskov, O.; Nyvad, B.; Kidd, E.A.M. Dental caries: What is it? In Dental Caries: The Disease and Its Clinical Management, 3rd ed.; Fejerskov, O., Nyvad, B., Kidd, E., Eds.; Whiley Blackwell: Oxford, UK, 2015; pp. 7–10. [Google Scholar]
- Thylstrup, A.; Bruun, C.; Holmen, L. In vivo caries models – mechanisms for caries initiation and arrestment. Adv. Dent. Res. 1994, 8, 144–157. [Google Scholar] [CrossRef]
- Fejerskov, O. Concepts of dental caries for understanding the disease. Community Dent. Oral Epidemiol. 1997, 25, 5–12. [Google Scholar] [CrossRef]
- Baelum, V.; Machiulskiene, V.; Nyvad, B.; Richards, A.; Vaeth, M. Application of survival analysis to carious lesion transitions in intervention trials. Community Dent. Oral Epidemiol. 2003, 31, 252–260. [Google Scholar] [CrossRef]
- Maltz, M.; Barbachan, E.; Silva, B.; Carvalho, D.Q.; Volkweis, A. Results after two years of non-operative treatment of occlusal surface in children with high caries prevalence. Braz. Dent. J. 2003, 14, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, K.R.; Christiansen, M.E. Outcomes of a non-operative caries treatment programme for children and adolescents. Caries Res. 2005, 39, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Kuzmina, I.; Ekstrand, K.R. Outcomes 18 years after implementation of a non-operative caries preventive program—The Nexö-method—On children in Moscow, Russia. Community Dent. Oral Epidemiol 2015, 43, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Machiulskiene, V.; Nyvad, B.; Baelum, V. Prevalence and severity of dental caries in 12-year-old children in Kaunas, Lithuania 1995. Caries Res. 1998, 32, 175–180. [Google Scholar] [CrossRef]
- Ismail, A. Diagnostic levels in dental public health planning. Caries Res. 2004, 38, 199–203. [Google Scholar] [CrossRef]
- Baelum, V.; Heidmann, J.; Nyvad, B. Dental caries paradigms in diagnosis and diagnostic research. Eur. J. Oral Sci. 2006, 114, 263–677. [Google Scholar] [CrossRef]
- Machiulskiene, V.; Carvalho, J.C. Clinical Diagnosis of Dental Caries in XXI Century: Introductory Paper. ORCA Saturday Afternoon Symposium, 2016. Caries Res. 2018, 52, 387–391. [Google Scholar] [CrossRef]
- Razmiene, J. Oral Hygiene Condition and Dental Caries Severity in 4–6 Year-Old Children Attending Pre-School Institutions in Lithuania and Relationship between Dental Caries Severity and Socioeconomic Status of the Family. Ph.D. Thesis, LSMU, Kaunas, Lithuania, 2013. [Google Scholar]
- Nyvad, V.; Machiulskiene, V.; Baelum, V. Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions. Caries Res. 1999, 33, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Löe, H.; Silness, J. Periodontal disease in pregnancy. Prevalence and severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef] [PubMed]
- WHO. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Bernabe, E.; Sheiham, A. Age, period and cohort trends in caries of permanent teeth in four developed countries. Am. J. Public Health 2014, 104, E115–E121. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.C. Caries process on occlusal surfaces: Evolving evidence and understanding. Caries Res. 2014, 48, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Larmas, M.A.; Virtanen, J.I.; Bloigu, R.S. Timing of first restorations in permanent teeth: A new system for oral health determination. J. Dent. 1995, 23, 347–352. [Google Scholar] [CrossRef]
- Carvalho, J.C.; Dige, I.; Machiulskiene, V.; Qvist, V.; Bakhshandeh, A.; Fatturi-Parolo, C.; Maltz, M. Occlusal Caries: Biological Approach for Its Diagnosis and Management. Caries Res. 2016, 50, 527–542. [Google Scholar] [CrossRef]
- Alves, L.S.; Zenkner, J.E.; Wagner, M.B.; Damé-Teixeira, N.; Susin, C.; Maltz, M. Eruption Stage of Permanent Molars and Occlusal Caries Activity/Arrest. J. Dent. Res. 2014, 93 (Suppl. 7), 114S–119S. [Google Scholar] [CrossRef]
- Joseph, C.; Velly, A.M.; Pierre, A.; Bourgeois, D.; Muller-Bolla, M. Dental health of 6-year-old children in Alpes Maritimes, France. Eur. Arch. Paediatr. Dent. 2011, 12, 256–263. [Google Scholar] [CrossRef]
- Carvalho, J.C.; Ekstrand, K.R.; Thylstrup, A. Dental plaque and caries on occlusal surfaces of first permanent molars in relation to stage of eruption. J. Dent. Res. 1989, 68, 773–779. [Google Scholar] [CrossRef]
- Quaglio, I.M.; Sousa, M.B.; Andenghi, T.M.; Mendes, F.M.; Imparato, J.C.P.; Pinheiro, S.L. Association between clinical parameters and the presence of active caries lesions in first permanent molars. Braz. Oral Res. 2006, 20, 358–363. [Google Scholar] [CrossRef]
- Siudikiene, J.; Machiulskiene, V.; Nyvad, B.; Tenovuo, J.; Nedzelskiene, I. Dental caries and salivary status in children with type 1 diabetes mellitus, related to metabolic control of the disease. Eur. J. Oral Sci. 2006, 114, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.C.; Mestrinho, H.D.; Oliveira, L.S.; Varjao, M.M.; Aimee, N.; Qvist, V. Validation of the Visible Occlusal Plaque Index (VOPI) in estimating caries lesion activity. J. Dent. 2017, 64, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Hausen, H.; Baelum, V. How accurately can we assess the risk for developing caries lesions? In Dental Caries: The Disease and Its Clinical Management, 3rd ed.; Fejerskov, O., Nyvad, B., Kidd, E., Eds.; Whiley Blackwell: Oxford, UK, 2015; pp. 423–438. [Google Scholar]
- Holmes, R.D. Tooth brushing frequency and risk of new carious lesions. Evid. Based Dent. 2016, 17, 98–99. [Google Scholar] [CrossRef] [PubMed]
- Baginska, J.; Rodakowska, E.; Milewski, R.; Kierklo, A. Dental caries in primary and permanent molars in 7–8-year-old schoolchildren evaluated with Caries Assessment Spectrum and Treatment (CAST) index. BMC Oral Health 2014, 14, 74. [Google Scholar] [CrossRef] [PubMed]
- Nyvad, B.; Machiulskiene, V.; Baelum, V. Construct and Predictive Validity of Clinical Caries Diagnostic Criteria Assessing Lesion Activity. J. Dent. Res. 2003, 82, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Séllos, M.C.; Soviero, V.M. (Reliability of the Nyvad criteria for caries assessment in primary teeth. Eur. J. Oral Sci. 2011, 119, 225–231. [Google Scholar] [CrossRef]
- Tikhonova, S.M.; Feine, J.S.; Pustavoitava, N.N.; Allison, P.J. Reproducibility and diagnostic outcomes of two visual-tactile criteria used by dentists to assess caries lesion activity: A cross-over study. Caries Res. 2014, 48, 126–136. [Google Scholar] [CrossRef]
- Jepsen, S.; Blanco, J.; Buchalla, W.; Carvalho, J.C.; Dietrich, T.; Dörfer, C.; Eaton, K.A.; Figuero, E.; Frencken, J.E.; Graziani, F.; et al. Prevention and control of dental caries and periodontal diseases at individual and population level: Consensus report of group 3 of joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol. 2017, 44 (Suppl. 18), S85–S93. [Google Scholar]
- Splieth, C.H.; Christiansen, J.; Foster Page, L.A. Caries epidemiology and community dentistry: Chances for future improvements in caries risk groups. Outcomes of the ORCA Saturday afternoon symposium, Greifswald, 2014. Part 1. Caries Res. 2016, 50, 9–16. [Google Scholar] [CrossRef]
- Carvalho, J.C.; Thylstrup, A.; Ekstrand, K.R. Results after 3 years of non-operative occlusal caries treatment of erupting permanent first molars. Community Dent. Oral Epidemiol. 1992, 20, 187–192. [Google Scholar] [CrossRef]
- Axelsson, P.; Nyström, B.; Lindhe, J. The long-term effect of a plaque control program on tooth mortality, caries and periodontal disease in adults. Results after 30 years of maintenance. J. Clin. Periodontol. 2004, 31, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Hausen, H.; Seppa, L.; Poutanen, R.; Niinimaa, A.; Lahti, S.; Kärkkäinen, S.; Pietilä, I. Noninvasive control of dental caries in children with active initial lesions. A randomized clinical trial. Caries Res. 2007, 41, 384–391. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age Group, n | DF-S (WHO) | DF-S (Nyvad) | Decayed Surfaces (Nyvad Criteria) | Filled Surfaces | ||||
|---|---|---|---|---|---|---|---|---|
| Total | Active, Noncavitated | Active, Cavitated | Inactive, Noncavitated | Inactive, Cavitated | ||||
| M (SD), Median (IQR 25%–75%) | ||||||||
| 5-year-olds | 0.33 (1.02) | 1.01 (2.17) | 1.01 (2.17) | 0.63 (1.54) | 0.33 (1.02) | 0.05 (0.45) | 0 | 0 |
| n = 79 | 0 (0–0.0) * | 0 (0–0.0) * | 0 (0–0.0) * | 0 (0–0.0) | 0 (0–0.0) * | 0 (0–0.0) * | ||
| 6-year-olds | 0.81 (1.48) | 1.95 (3.05) | 1.84 (2.93) | 0.95 (2.06) | 0.67 (0.28) | 0.19 (0.90) | 0.03 (0.27) | 0.11 (0.7) |
| n = 374 | 0 (0–1.0) | 0 (0–3.0) | 0 (0–3.0) | 0 (0–1.0) | 0 (0–1.0) | 0 (0–0.0) | 0 (0–0.0) | 0 (0–0.0) * |
| p value | <0.001 | 0.002 | 0.004 | 0.12 | 0.01 | 0.04 | 0.34 | 0.003 |
| 5–6-year-olds | 0.73 (1.42) | 1.79 (2.93) | 1.7 (2.83) | 0.89 (1.98) | 0.61 (1.24) | 0.17 (0.84) | 0.02 (0.24) | 0.09 (0.64) |
| n = 453 | 0 (0–1.0) | 0 (0–3.0) | 0 (0–3.0) | 0 (0–1.0) | 0 (0–1.0) | 0 (0–0.0) | 0 (0–0.0) | 0 (0–0.0) |
| Age Group, n | Decayed Surfaces (Nyvad Criteria) | ||||
|---|---|---|---|---|---|
| Active, Noncavitated | Active, Cavitated | Inactive, Noncavitated | Inactive, Cavitated | Filled Surfaces | |
| M (SD), Median (IQR 25–75%), Prevalence N (%) | |||||
| 5-year-olds n = 79 | 0.35 (1.24) | 0.19 (0.68) | 0.05 (0.45) | 0 | 0 |
| 0 (0–0.0) | 0 (0–0.0) | 0 (0–0.0) | |||
| 11 (14%) | 7 (9%) * | 1 (1%) | |||
| 6-year-olds n = 374 | 0.66 (1.85) | 0.51 (1.0) | 0.14 (0.63) | 0.03 (0.27) | 0.07 (0.34) |
| 0 (0–1.0) | 0 (0–1.0) | 0 (0–0.0) | 0 (0–0.0) | 0 (0–0.0) | |
| 65 (17%) | 94 (25%) * | 24 (6%) | 5 (1%) | 17 (5%) | |
| p value | 0.361/0.455 | 0.002/0.002 | 0.072/0.068 | 0.302/0.592 | 0.054/0.053 |
| 5–6-year-olds n = 453 | 0.61 (1.76) | 0.45 (0.97) | 0.13 (0.6) | 0.02 (0.24) | 0.06 (0.34) |
| 0 (0–0.0) | 0 (0–0.0) | 0 (0–0.0) | 0 (0–0.0) | 0 (0–0.0) | |
| 76 (17%) | 101 (22%) | 25 (6%) | 5 (1%) | 17 (4%) | |
| Age, Years | Active Caries (Noncavitated and Cavitated Lesions) | ||
|---|---|---|---|
| n (%) of Individuals with Active Lesions | OR (95% CI) | ||
| Dental plaque (plaque scores) | |||
| 5–6 | No plaque (0+1), n = 224 | 34 (15) | 1 7.36 (4.70–11.52) |
| Plaque present (2+3), n = 230 | 131 (57) | ||
| p value * | <0.001 | ||
| 5 | No plaque (0+1), n = 35 | 4 (11) | 1 4.01 (1.19–13.49) |
| Plaque present (2+3), n = 44 | 15 (34) | ||
| p value | 0.019 | ||
| 6 | No plaque (0+1), n = 188 | 30 (16) | 1 8.73 (5.35–14.25) |
| Plaque present (2+3), n = 186 | 116 (62) | ||
| p value | <0.001 | ||
| Self-reported toothbrushing frequency | |||
| 5–6 | 1–2 times per day, n = 360 | 103 (29) | 1 4.99 (3.063–8.13) |
| Irregularly/never, n = 93 | 62 (67) | ||
| p value | <0.001 | ||
| 5 | 1–2 times per day, n = 58 | 8 (14) | 1 6.88 (2.21–21.41) |
| Irregularly/never, n = 21 | 11 (52) | ||
| p value | <0.001 | ||
| 6 | 1–2 times per day, n = 302 | 95 (32) | 1 5.29 (3.01–9.29) |
| Irregularly/never, n = 72 | 51 (71) | ||
| p value | <0.001 | ||
| Predictor | High DF-S, Odds Ratio (95% CI) |
|---|---|
| High % dmfs * | 4.2 (2.7–6.8) |
| Age, years | 2.7 (1.3–5.4) |
| Self-reported tooth brushing frequency | 2.5 (1.5–4.3) |
| Nagelkerke R Square = 0.3; Overall Percentage = 81.2 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mačiulskienė, V.; Razmienė, J.; Andruškevičienė, V.; Bendoraitienė, E. Estimation of Caries Treatment Needs in First Permanent Molars of Lithuanian 5–6-Year-Old Children, Based on Caries Lesion Activity Assessment. Medicina 2020, 56, 105. https://doi.org/10.3390/medicina56030105
Mačiulskienė V, Razmienė J, Andruškevičienė V, Bendoraitienė E. Estimation of Caries Treatment Needs in First Permanent Molars of Lithuanian 5–6-Year-Old Children, Based on Caries Lesion Activity Assessment. Medicina. 2020; 56(3):105. https://doi.org/10.3390/medicina56030105
Chicago/Turabian StyleMačiulskienė, Vita, Jaunė Razmienė, Vilija Andruškevičienė, and Eglė Bendoraitienė. 2020. "Estimation of Caries Treatment Needs in First Permanent Molars of Lithuanian 5–6-Year-Old Children, Based on Caries Lesion Activity Assessment" Medicina 56, no. 3: 105. https://doi.org/10.3390/medicina56030105
APA StyleMačiulskienė, V., Razmienė, J., Andruškevičienė, V., & Bendoraitienė, E. (2020). Estimation of Caries Treatment Needs in First Permanent Molars of Lithuanian 5–6-Year-Old Children, Based on Caries Lesion Activity Assessment. Medicina, 56(3), 105. https://doi.org/10.3390/medicina56030105