Venous Thromboembolism Recurrence in Latvian Population: Single University Hospital Data

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
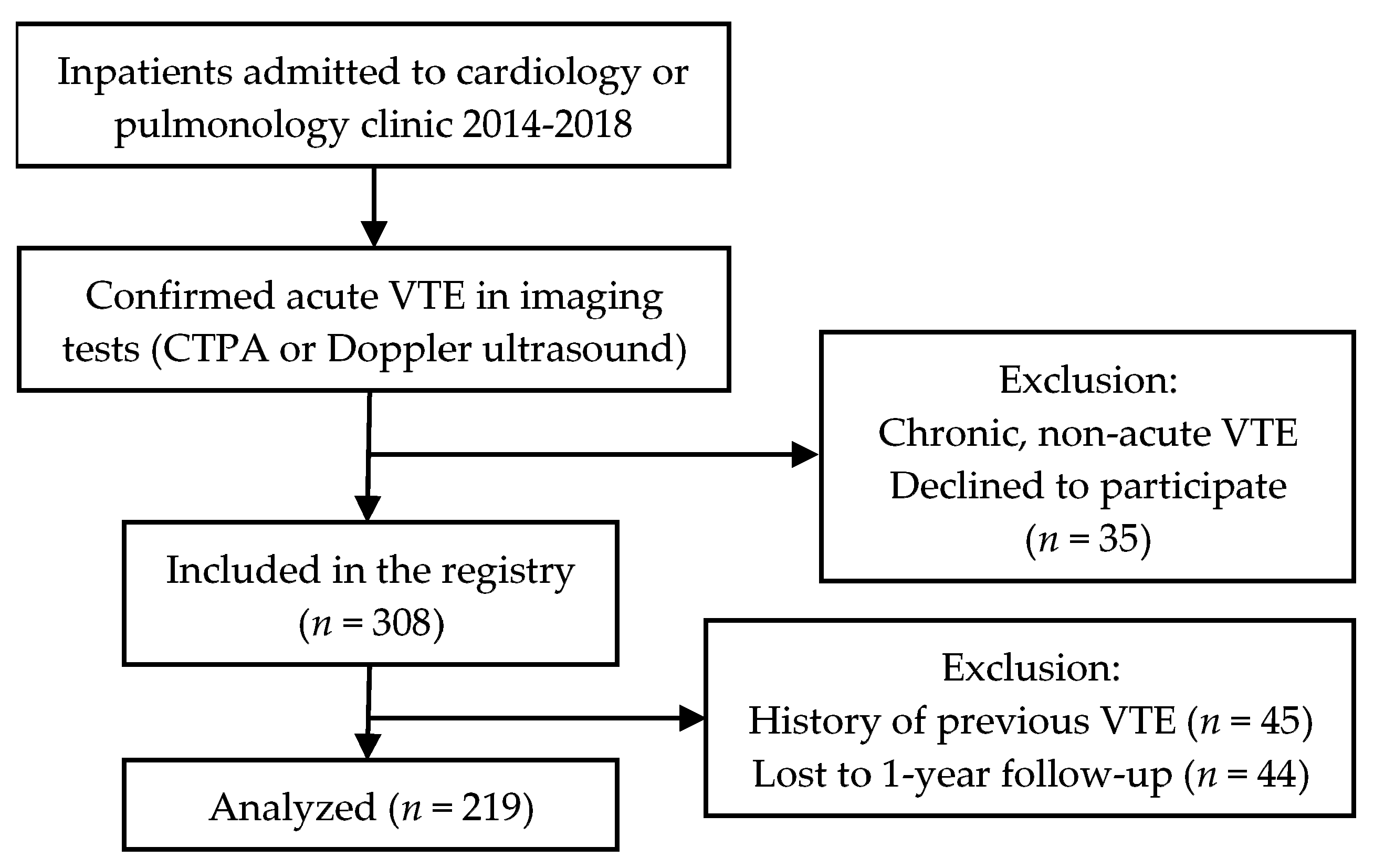
2.1. Study Population
2.2. Study Design
2.3. Statistical Analysis
3. Results
3.1. Patient Cohort
3.2. Clinical Factors
3.3. Anticoagulation Strategies
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- DeMonaco, N.A.; Dang, Q.; Kapoor, W.N.; Ragni, M.V. Pulmonary Embolism Incidence Is Increasing with Use of Spiral Computed Tomography. Am. J. Med. 2008, 121, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Burge, A.; Freeman, K.; Klapper, P.; Haramati, L. Increased diagnosis of pulmonary embolism without a corresponding decline in mortality during the CT era. Clin. Radiol. 2008, 63, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Martinez, C.; Cohen, A.T.; Bamber, L.; Rietbrock, S. Epidemiology of first and recurrent venous thromboembolism: A population-based cohort study in patients without active cancer. Thromb. Haemost. 2014, 112, 255–263. [Google Scholar] [PubMed]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef] [PubMed]
- Rodger, M.A.; Kahn, S.R.; Wells, P.S.; Anderson, D.A.; Chagnon, I.; Le Gal, G.; Solymoss, S.; Crowther, M.; Perrier, A.; White, R.; et al. Identifying unprovoked thromboembolism patients at low risk for recurrence who can discontinue anticoagulant therapy. Can. Med Assoc. J. 2008, 179, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Eichinger, S.; Heinze, G.; Jandeck, L.M.; Kyrle, P.A. Risk assessment of recurrence in patients with unprovoked deep vein thrombosis or pulmonary embolism: The vienna prediction model. Circulation 2010, 121, 1630–1636. [Google Scholar] [CrossRef] [PubMed]
- Tosetto, A.; Iorio, A.; Marcucci, M.; Baglin, T.; Cushman, M.; Eichinger, S.; Palareti, G.; Poli, D.; Tait, R.; Douketis, J. Predicting disease recurrence in patients with previous unprovoked venous thromboembolism: A proposed prediction score (DASH). J. Thromb. Haemost. 2012, 10, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, V.; Kim, E.S.H. Risk of Recurrent Venous Thromboembolism After an Initial Episode: Risk Stratification and Implications for Long-term Treatment. Curr. Cardiol. Rep. 2019, 21, 24. [Google Scholar] [CrossRef] [PubMed]
- Kakkos, S.; Kirkilesis, G.; Tsolakis, I. Editor’s Choice—Efficacy and Safety of the New Oral Anticoagulants Dabigatran, Rivaroxaban, Apixaban, and Edoxaban in the Treatment and Secondary Prevention of Venous Thromboembolism: A Systematic Review and Meta-analysis of Phase III Trials. Eur. J. Vasc. Endovasc. Surg. 2014, 48, 565–575. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Ageno, W.; Cannegieter, S.C.; Cosmi, B.; Geersing, G.J.; Kyrle, P.A. Categorization of patients as having provoked or unprovoked venous thromboembolism: Guidance from the SSC of ISTH. J. Thromb. Haemost. 2016, 14, 1480–1483. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Yoshikawa, Y.; Morimoto, T.; Amano, H.; Takase, T.; Hiramori, S.; Kim, K.; Oi, M.; Akao, M.; Kobayashi, Y.; et al. The association of recurrence and bleeding events with mortality after venous thromboembolism: From the COMMAND VTE Registry. Int. J. Cardiol. 2019, 292, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Ay, C.; Posch, F.; Kaider, A.; Zielinski, C.; Pabinger, I. Estimating risk of venous thromboembolism in patients with cancer in the presence of competing mortality. J. Thromb. Haemost. 2015, 13, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Einstein—PE Investigators. Oral Rivaroxaban for the Treatment of Symptomatic Pulmonary Embolism. N. Engl. J. Med. 2012, 366, 1287–1297. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Kakkar, A.K.; Goldhaber, S.Z.; Schellong, S.; Eriksson, H.; Mismetti, P.; Christiansen, A.V.; Friedman, J.; le Maulf, F.; Peter, N.; et al. Treatment of Acute Venous Thromboembolism With Dabigatran or Warfarin and Pooled Analysis. Circulation 2014, 129, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Outes, A.; Terleira-Fernandez, A.I.; Lecumberri, R.; Suarez-Gea, M.L.; Vargas-Castrillon, E. Direct oral anticoagulants in the treatment of acute venous thromboembolism: A systematic review and meta-analysis. Thromb. Res. 2014, 134, 774–782. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Patients (n = 219) |
|---|---|
| Age, years, mean ± SD | 68 ± 16 (range: 19–93) |
| Sex, female, n (%) | 139 (63.5) |
| Body-mass index, kg/m2, mean ± SD | 28.7 ± 6.0 |
| Obesity (BMI ≥ 30), n (%) | 78 (35.6) |
| Unprovoked VTE, n (%) | 38 (17.4) |
| Active cancer, n (%) | 29 (13.2) |
| Factor | Recurrences, n IR per 100 Person-Years (95% CI) | p-Value | |
|---|---|---|---|
| Sex | Male | 5 5.3 (2.6–10.6) | 0.761 |
| Female | 8 6.3 (2.6–15.0) | ||
| Active cancer | Yes | 3 23.5 (7.6–72.8) | 0.036 * |
| No | 10 4.6 (2.5–8.5) | ||
| Transient risk factors for primary VTE | Yes | 4 4.8 (1.8–12.7) | 0.710 |
| No | 9 6.1 (3.2–11.7) | ||
| Transient risk factors for primary VTE (with no persistent risk factors) | Yes | 2 7.0 (1.8–28.0) | 0.698 |
| No | 11 5.4 (3.0–9.8) | ||
| Minor persistent risk factors (excluding cancer patients) | Yes | 6 4.4 (2.0–9.7) | 0.833 |
| No | 4 5.0 (1.9–13.2) | ||
| Unprovoked VTE vs Provoked VTE | Yes | 3 6.5 (2.1–20.3) | 0.743 |
| No | 10 5.4 (2.9–10.0) | ||
| Charlson Comorbidity Index ≥4 points | Yes | 10 8.3 (4.5–15.4) | 0.081 |
| No | 3 2.7 (0.9–8.4) | ||
| Arterial hypertension | Yes | 6 4.2 (1.9–9.4) | 0.245 |
| No | 7 8.1 (3.8–16.9) | ||
| Atrial fibrillation | Yes | 4 10.9 (4.1–29.1) | 0.179 |
| No | 9 4.6 (2.4–8.9) | ||
| Anemia | Yes | 4 6.5 (2.4–17.2) | 0.728 |
| No | 9 5.3 (2.8–10.2) | ||
| Thrombocytopenia | Yes | 3 10.3 (3.3–32.1) | 0.287 |
| No | 10 4.9 (2.7–9.2) | ||
| Thrombocytosis | Yes | 1 9.7 (1.4–69.0) | 0.559 |
| No | 12 5.4 (3.1–9.6) | ||
| Obesity | Yes | 5 5.2 (2.2–12.5) | 0.829 |
| No | 8 6.0 (3.0–12.0) | ||
| Discontinuation of anticoagulation | Yes | 4 3.3 (1.2–8.8) | 0.129 |
| No | 9 8.2 (4.3–15.8) | ||
| Anticoagulation >6 months † | Yes | 5 3.1 (1.3–7.5) | 0.653 |
| No | 1 1.6 (0.2–12.3) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ģībietis, V.; Kigitoviča, D.; Strautmane, S.; Meilande, K.; Kalējs, V.R.; Zaičenko, A.; Maķe, K.; Lejnieks, A.; Skride, A. Venous Thromboembolism Recurrence in Latvian Population: Single University Hospital Data. Medicina 2019, 55, 510. https://doi.org/10.3390/medicina55090510
Ģībietis V, Kigitoviča D, Strautmane S, Meilande K, Kalējs VR, Zaičenko A, Maķe K, Lejnieks A, Skride A. Venous Thromboembolism Recurrence in Latvian Population: Single University Hospital Data. Medicina. 2019; 55(9):510. https://doi.org/10.3390/medicina55090510
Chicago/Turabian StyleĢībietis, Valdis, Dana Kigitoviča, Sintija Strautmane, Kitija Meilande, Verners Roberts Kalējs, Anastasija Zaičenko, Kristīne Maķe, Aivars Lejnieks, and Andris Skride. 2019. "Venous Thromboembolism Recurrence in Latvian Population: Single University Hospital Data" Medicina 55, no. 9: 510. https://doi.org/10.3390/medicina55090510
APA StyleĢībietis, V., Kigitoviča, D., Strautmane, S., Meilande, K., Kalējs, V. R., Zaičenko, A., Maķe, K., Lejnieks, A., & Skride, A. (2019). Venous Thromboembolism Recurrence in Latvian Population: Single University Hospital Data. Medicina, 55(9), 510. https://doi.org/10.3390/medicina55090510