A Critical Analysis of the Exercise Prescription and Return to Activity Advice That Is Provided in Patient Information Leaflets Following Lumbar Spine Surgery



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Pilot Testing
2.4. Evaluation
3. Results
3.1. Exercises
3.2. Dosage of Exercise Prescription
3.3. Return to “Normal” Activities
3.4. Recognition of Uncertainty
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Disease, G.B.D.; Injury, I.; Prevalence, C.; Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar]
- Frymoyer, J.W. Lumbar disk disease: Epidemiology. Instr. Course Lect. 1992, 41, 217–223. [Google Scholar] [PubMed]
- Ozkara, G.O.; Ozgen, M.; Ozkara, E.; Armagan, O.; Arslantas, A.; Atasoy, M.A. Effectiveness of physical therapy and rehabilitation programs starting immediately after lumbar disc surgery. Turk. Neurosurg. 2015, 25, 372–379. [Google Scholar] [PubMed]
- Rushton, A.; Wright, C.; Heap, A.; White, L.; Eveleigh, G.; Heneghan, N. Survey of current physiotherapy practice for patients undergoing lumbar spinal fusion in the United Kingdom. Spine (Phila Pa 1976) 2014, 39, E1380–E1387. [Google Scholar] [CrossRef] [PubMed]
- Madera, M.; Brady, J.; Deily, S.; McGinty, T.; Moroz, L.; Singh, D.; Tipton, G.; Truumees, E.; Group for the Seton Spine Rehabilitation Study. The role of physical therapy and rehabilitation after lumbar fusion surgery for degenerative disease: A systematic review. J. Neurosurg. Spine 2017, 26, 694–704. [Google Scholar] [CrossRef]
- Janssen, E.; Scheijen, E.; Meeteren, N.; Bie, R.; Lenssen, A.; Willems, P.; Hoogeboom, T.; Janssen, E.R.C.; Scheijen, E.E.M.; van Meeteren, N.L.U.; et al. Determining clinical practice of expert physiotherapy for patients undergoing lumbar spinal fusion: A cross-sectional survey study. Eur. Spine J. 2016, 25, 1533–1541. [Google Scholar] [CrossRef] [PubMed]
- Ostelo, R.W.J.G.; de Vet, H.C.W.; Berfelo, M.W.; Kerckhoffs, M.R.; Vlaeyen, J.W.S.; Wolters, P.M.J.C.; van den Brandt, P.A. Effectiveness of behavioral graded activity after first-time lumbar disc surgery: Short term results of a randomized controlled trial. Eur. Spine J. 2003, 12, 637–644. [Google Scholar] [CrossRef]
- Greenwood, J.; McGregor, A.; Jones, F.; Mullane, J.; Hurley, M. Rehabilitation Following Lumbar Fusion Surgery: A Systematic Review and Meta-Analysis. Spine (Phila Pa 1976) 2016, 41, E28–E36. [Google Scholar] [CrossRef]
- Mancuso, C.A.; Duculan, R.; Girardi, F.P. Healthy Physical Activity Levels Below Recommended Thresholds Two Years After Lumbar Spine Surgery. Spine (03622436) 2017, 42, E241–E247. [Google Scholar] [CrossRef]
- Wainwright, T.W.; Immins, T.; Middleton, R.G. Enhanced recovery after surgery (ERAS) and its applicability for major spine surgery. Best Pr. Res: Clin. Anaesthesiol. 2016, 30, 91–102. [Google Scholar] [CrossRef]
- Sustersic, M.; Gauchet, A.; Foote, A.; Bosson, J.-L. How best to use and evaluate Patient Information Leaflets given during a consultation: A systematic review of literature reviews. Health Expect 2017, 20, 531–542. [Google Scholar] [CrossRef] [PubMed]
- McCartney, M. Patient information leaflets: “a stupid system”. BMJ 2013, 347, f4748. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, T.W.; Burgess, L.C. To what extent do current total hip and knee replacement patient information resources adhere to enhanced recovery after surgery principles? Physiotherapy 2018, 104, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Low, M.; Burgess, L.C.; Wainwright, T.W. Patient Information Leaflets for Lumbar Spine Surgery: A Missed Opportunity. BMC Musculoskelet Disord 2019. In Review. [Google Scholar]
- Incs, N. National Collaborating Centre for Primary Care (UK). In Low Back Pain: Early Management of Persistent Non-specific Low Back Pain; Royal College of General Practitioners: London, UK, 2009. [Google Scholar]
- Dixon-Woods, M. Writing wrongs? An analysis of published discourses about the use of patient information leaflets. Soc. Sci. Med. 2001, 52, 1417–1432. [Google Scholar] [CrossRef]
- Grime, J.C.; Ong, B.N. Constructing osteoarthritis through discourse--a qualitative analysis of six patient information leaflets on osteoarthritis. BMC Musculoskelet. Disord. 2007, 8, 34. [Google Scholar] [CrossRef] [PubMed]
- Hodges, P.W.; Richardson, C.A. Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis. Spine (Phila Pa 1976) 1996, 21, 2640–2650. [Google Scholar] [CrossRef]
- Hides, J.A.; Jull, G.A.; Richardson, C.A. Long-term effects of specific stabilizing exercises for first-episode low back pain. Spine (Phila Pa 1976) 2001, 26, E243–E248. [Google Scholar] [CrossRef]
- Smith, B.E.; Littlewood, C.; May, S. An update of stabilisation exercises for low back pain: A systematic review with meta-analysis. BMC Musculoskelet. Disord. 2014, 15, 416. [Google Scholar] [CrossRef]
- Low, M. A Time to Reflect on Motor Control in Musculoskeletal Physical Therapy. J. Orthop. Sports Phys. 2018, 48, 833–836. [Google Scholar] [CrossRef]
- Basson, A.; Olivier, B.; Ellis, R.; Coppieters, M.; Stewart, A.; Mudzi, W. The Effectiveness of Neural Mobilization for Neuromusculoskeletal Conditions: A Systematic Review and Meta-analysis. J. Orthop. Sports Phys. 2017, 47, 593–615. [Google Scholar] [CrossRef] [PubMed]
- Trust, S.T.H.N.F. Preparing for Your Discectomy. Available online: https://www.southtees.nhs.uk/content/uploads/MICB2846-V2-Discectomy.pdf (accessed on 14 March 2019).
- Deyo, R.A. Biopsychosocial care for chronic back pain. Bmj 2015, 350, h538. [Google Scholar] [CrossRef] [PubMed]
- Saragiotto, B.T.; de Almeida, M.O.; Yamato, T.P.; Maher, C.G. Multidisciplinary Biopsychosocial Rehabilitation for Nonspecific Chronic Low Back Pain. Phys. 2016, 96, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Lall, M.P.; Restrepo, E. The Biopsychosocial Model of Low Back Pain and Patient-Centered Outcomes Following Lumbar Fusion. Orthop. Nurs. 2017, 36, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Deisseroth, K.; Hart, R.A. Symptoms of post-traumatic stress following elective lumbar spinal arthrodesis. Spine (Phila Pa 1976) 2012, 37, 1628–1633. [Google Scholar] [CrossRef]
- Hart, R.; Perry, E.; Hiratzka, S.; Kane, M.; Deisseroth, K. Post-traumatic stress symptoms after elective lumbar arthrodesis are associated with reduced clinical benefit. Spine (Phila Pa 1976) 2013, 38, 1508–1515. [Google Scholar] [CrossRef] [PubMed]
- Saragiotto, B.T.; Maher, C.G.; Yamato, T.P.; Costa, L.O.; Menezes Costa, L.C.; Ostelo, R.W.; Macedo, L.G. Motor control exercise for chronic non-specific low-back pain. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.; Cho, K.; Shim, S.; Yu, J.; Jung, J. Effects of Exercise Rehabilitation on Pain, Disability, and Muscle Strength after Posterior Lumbar Interbody Fusion Surgery: A Randomized Controlled Trial. J. Phys. Sci. 2012, 24, 1037–1040. [Google Scholar] [CrossRef]
- Hides, J.A.; Boughen, C.L.; Stanton, W.R.; Strudwick, M.W.; Wilson, S.J. A magnetic resonance imaging investigation of the transversus abdominis muscle during drawing-in of the abdominal wall in elite Australian Football League players with and without low back pain. J. Orthop. Sports Phys. 2010, 40, 4–10. [Google Scholar] [CrossRef][Green Version]
- Gallois, M.; Davergne, T.; Ledinot, P.; Ravaud, P.; Regnaux, J.-P. Dosage of Preventive or Therapeutic Exercise Interventions: Review of Published Randomized Controlled Trials and Survey of Authors. Arch. Phys. Med. Rehabil. 2017, 98, 2558–2565. [Google Scholar] [CrossRef]
- Scrimshaw, S.V.; Maher, C.G. Randomized controlled trial of neural mobilization after spinal surgery. Spine (Phila Pa 1976) 2001, 26, 2647–2652. [Google Scholar] [CrossRef]
- McCartney, M. Margaret McCartney: When can I get back to running after my operation? BMJ 2017, 359. [Google Scholar] [CrossRef]
- Hutton, M. Spinal Services GIRFT Programme National Specialty Report; NHS: London, UK, 2019. [Google Scholar]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced Recovery after Surgery: A Review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Process |
|---|
|
| Inclusion | Exclusion |
|---|---|
| Patient | |
| Lumbar spinal fusion patients (all surgical techniques) for back and leg pain or for the treatment for low back pain following previous decompression surgery for predominant leg pain. Lumbar decompressions surgery (laminectomy, discectomy) for predominant leg pain. Patients aged over 16 years. | Any other spine surgery (lumbar disc replacement, correction of spinal deformity, removal of spinal tumours). Patients under 16 years old. |
| Information | |
| Postoperative physiotherapy. Exercise prescription. Home rehabilitation programmes. Return to normal activity advice. | |
| Source | |
| English NHS Hospital. | Independent Providers of Healthcare. Charity or Research Institute Information Blogs. |
| Format | |
| PDF or Word Document. Hospital provided webpage. Latest version. | Archived versions. |
| Theme | Definition and Aims | Examples |
|---|---|---|
| Isometric muscle activation | A theme of exercises whereby the muscle length stays the same during contraction. Usually, this exercise is given to reduce joint motion while still achieving a level of recruitment of muscle activity. It is usually given to either protect joint loading or to isolate individual muscle contractions. | Transversus abdominus in supine, isometric quadriceps, isometric gluteal and pelvic floor exercises |
| Range of movement | A theme of exercises that intends to provide movement across a specified range to the joint region. This can be across one or more joints depending on the area specified. | Knee rolls, hip flexion, extension, abduction, trunk side bends, ankle dorsi/plantarflexion and pelvic tilting |
| Neurodynamic | A theme of exercises that aims at restoring the homoeostasis in and around the nervous system by mobilisation of the nervous stem itself or the structures that surround the nervous system [22]. | Seated knee flexion/extension and hamstring stretch |
| Movement control | A theme of exercises that intends to produce specific restraints to joint or body motion in order to reduce ‘aberrant’ joint movement or body motion. | Side lying hip abduction (clam), supine bent knee fall out |
| Exercise | Theme | Frequency n (%) |
|---|---|---|
| Transverse abdominus | Isometric muscle activation | 7 (47%) |
| Knee rolls | Range of movement | 5 (34%) |
| Static glutes | Isometric muscle activation | 4 (27%) |
| Ankle pumps | Range of movement | 4 (27%) |
| Neurodynamic exercises | Neurodynamic | 4 (27%) |
| Pelvic tilts | Range of movement | 3 (20%) |
| Hip flexion | Range of movement | 3 (20%) |
| Static quadriceps | Isometric muscle activation | 2 (13%) |
| Hip abduction (bent knee fall out) | Movement control | 2 (13%) |
| Standing side bends | Range of movement | 1 (7%) |
| Hip extension | Range of movement | 1 (7%) |
| Side-lying clam exercise | Movement control | 1 (7%) |
| Hamstring stretch | Range of movement | 1 (7%) |
| Heel raises | Range of movement | 1 (7%) |
| Sit to stand | Functional Strength | 1 (7%) |
| Activity | Examples of Range of Advice for Return to “Normal” Activity | |
|---|---|---|
| Fusion surgery | Decompression surgery | |
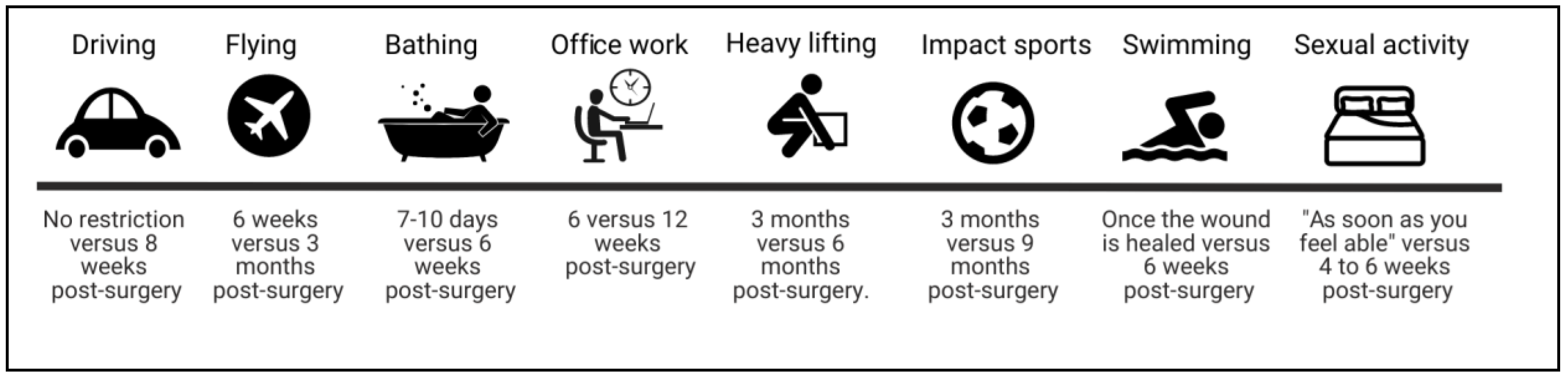
| Driving | No restriction versus 8 weeks post-surgery | 24 hours versus 6 weeks post-surgery |
| Flying | 6 weeks versus 3 months post-surgery | 2 weeks versus 2 months |
| Sexual activity | “As soon as you feel comfortable” versus 4–6 weeks post-surgery | “As soon as you feel comfortable” versus 3–4 weeks post-surgery |
| Bathing | 7–10 days versus 6 weeks post-surgery | No restriction if wound is protected versus 6 weeks post-surgery |
| Office work | 6 versus 12 weeks post-surgery | 2 weeks versus 8 weeks post-surgery. |
| Manual Work | 6 weeks versus 6 months post-surgery | 6 weeks versus 6 months post-surgery |
| Heavy lifting | Definition of heavy lifting: 10 kg. Return to heavy lifting: 3 months versus 6 months post-surgery. | Definition of heavy lifting: 1 kg (half a full kettle) versus 10 kg Return to heavy lifting: 4–6 weeks post-surgery. |
| Swimming | Once the wound is healed versus 6 weeks after surgery. | Straight after surgery versus 6 weeks post-surgery. |
| High impact sports | 3 months versus 9 months post-surgery | 4 weeks versus 6 months post-surgery |
| Posture | Vary posture every 20 min versus every 40 min | Vary posture every 20 min versus every 60 min |
| Discharge home | Expected discharge on day 2 following surgery versus 5–7 days. | Expected discharge on the day of surgery versus 5–7 days after surgery. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Low, M.; Burgess, L.C.; Wainwright, T.W. A Critical Analysis of the Exercise Prescription and Return to Activity Advice That Is Provided in Patient Information Leaflets Following Lumbar Spine Surgery. Medicina 2019, 55, 347. https://doi.org/10.3390/medicina55070347
Low M, Burgess LC, Wainwright TW. A Critical Analysis of the Exercise Prescription and Return to Activity Advice That Is Provided in Patient Information Leaflets Following Lumbar Spine Surgery. Medicina. 2019; 55(7):347. https://doi.org/10.3390/medicina55070347
Chicago/Turabian StyleLow, Matthew, Louise C. Burgess, and Thomas W. Wainwright. 2019. "A Critical Analysis of the Exercise Prescription and Return to Activity Advice That Is Provided in Patient Information Leaflets Following Lumbar Spine Surgery" Medicina 55, no. 7: 347. https://doi.org/10.3390/medicina55070347
APA StyleLow, M., Burgess, L. C., & Wainwright, T. W. (2019). A Critical Analysis of the Exercise Prescription and Return to Activity Advice That Is Provided in Patient Information Leaflets Following Lumbar Spine Surgery. Medicina, 55(7), 347. https://doi.org/10.3390/medicina55070347