A Systematic Review and Meta-Analysis Evaluating Antibiotic Prophylaxis in Dental Implants and Extraction Procedures



Abstract
1. Introduction
1.1. Antimicrobial Prescribing Trends in Dentistry
1.2. Antibiotic Resistance
1.3. Clinical Guidelines
- Patients at risk of infectious endocarditis (except in non-surgical dental procedures)
- Immuno-compromised patients
- For prolonged and extensive surgical interventions
- Surgery in infected sites
- When large foreign materials are implanted
1.4. Study Aim
2. Methods
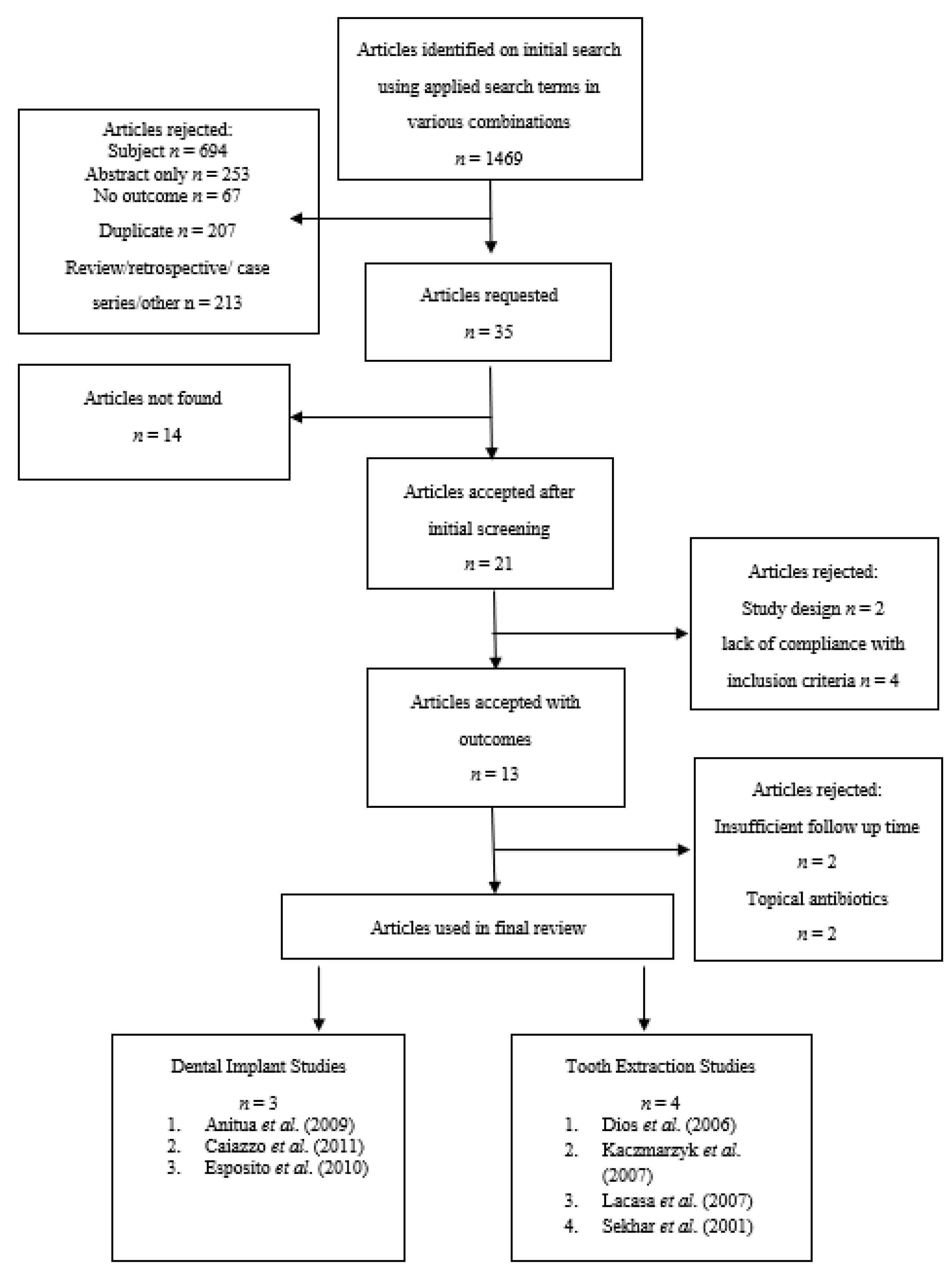
2.1. Search Strategy
2.2. Study Criteria
2.3. Quality Assessment and Risk of Bias
- Patient blinding
- Assessor blinding
- Allocation concealment
- Participant compliance with follow-up
3. Results
3.1. Extraction Studies
3.1.1. Dios et al. (2006) Trial
3.1.2. Lacasa et al. (2007) Trial
3.1.3. Kaczmarzyk et al. (2007) Trial
3.1.4. Sekhar et al. (2001) Trial
3.2. Dental Implant Studies
3.2.1. Esposito et al. (2010)
3.2.2. Anitua et al. (2009)
3.2.3. Caiazzo et al. (2011)
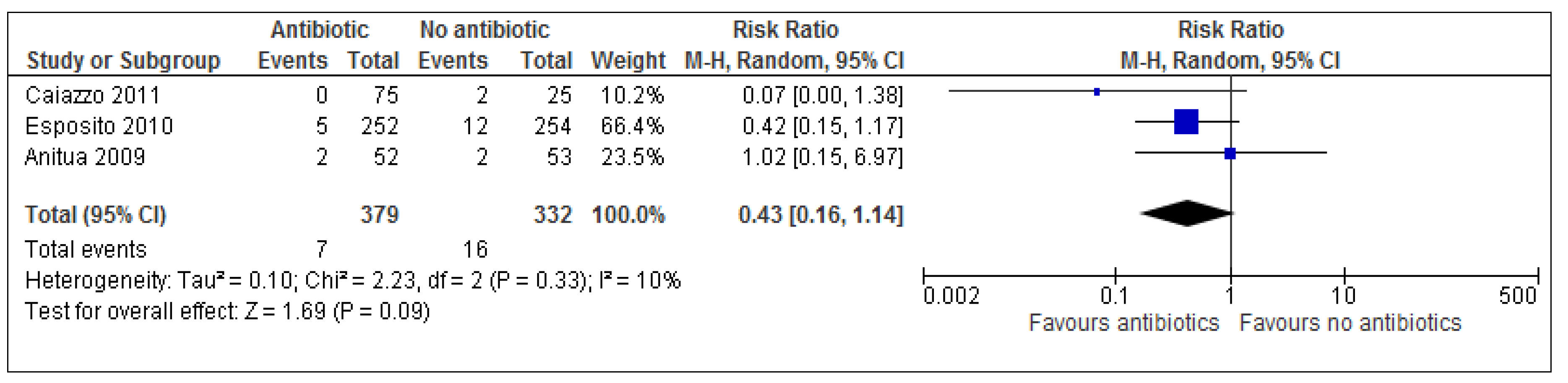
3.3. Implant Failure
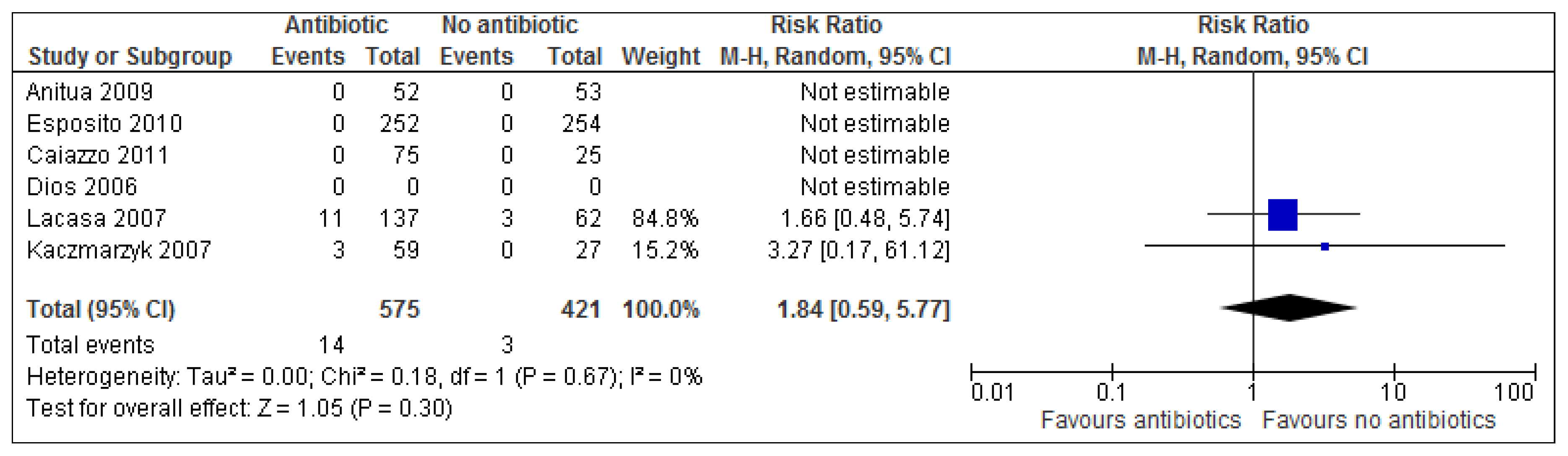
3.4. Adverse Events
4. Discussion
4.1. Dental Extraction
4.2. Dental Implants
4.3. Other Views
4.4. Limitations
4.5. Implications for Dentists
4.6. Implications for Further Work
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Outcome Measures and Statistical Analysis Using REVMAN 5.0 Software
Appendix B. CASP Forms Checklists Templates Were Used from CASP International Network (2013)
| Section (A) Are the results of the review valid? |
| Screening Questions 1. Did the trial address a clearly focused issue? |
| Yes. The authors evaluated the efficacy of Amoxicillin 2 g preoperatively vs moxifloxacin 400 mg vs. clindamycin 600 mg preoperatively vs. placebo (5-day treatment) for the prevention of bacteraemia following dental extraction. |
| 2. Was the assignment of patients to treatments randomised? |
| Yes. Randomisation was based on a single sequence of random assignments using a computer generated randomisation list. |
| 3. Were all of the patients who entered the trial properly accounted for at its conclusion? |
| Yes. All 221 patients had been accounted for in results and conclusion of the study |
| Detailed questions 4. Were patients, health workers and study personnel ‘blind’ to treatment? |
| Study is described as ‘double-blind’. |
| 5. Were the groups similar at the start of the trial? |
| Size and composition of all three groups were similar Amoxicillin 2 g preoperatively (n = 56): 34 (M)/22 (F), mean age = 23.8 years Moxifloxacin 400 mg preoperatively (n = 58): 29 (M)/29 (F), mean age = 22.4 years Clindamycin 600 mg preoperatively (n = 54): 34 (M)/20 (F), mean age = 24 years Placebo (n = 53): 29 (M)/24 (F), mean age = 26.1 years The range of total extractions per group ranged from 53–58. |
| 6. Aside from the experimental intervention were the groups treated equally? |
| All patients were subjected to the same inclusion/ exclusion criteria and all extractions were conducted in the Santiago de Compostela University Hospital (Spain) under general anaesthesia. |
| Section (B) What are the results? |
| 7. How large was the treatment effect? |
| The presence of bacteraemia following dental extraction was measured as the outcome of interest. Streptococcus spp. were the most commonly identified bacteria in all groups ranging from 44 to 68% with the lowest percentage being detected from the amoxicillin group (p < 0.0001). Amoxicillin and moxifloxacin prophylaxis showed high efficacies (p < 0.001 and p < 0.05 respectively) in reducing prevalence and duration or bacteraemia. Clindamycin prophylaxis was seen to be non-effective (p < 0.9). |
| 8. How precise was the estimate of the treatment effect? |
| No confidence intervals are provided in the study, however p-values have been provided. |
| Section (C) Will the results help locally? |
| 9. Can the results be applied in your context? (or to the local population?) |
| Results may not be applicable to a general population. Patients did not comprise of the elderly, young children, immunocompromised patients or those at risk of IE. Patient mean age was in mid-20’s. A larger sample size would be required. Furthermore, the procedures were carried out in a hospital setting rather than a dental practice. General anaesthesia was used, but local anaesthetic is more commonly for tooth extraction (depending on complexity of extraction). |
| 10. Were all clinically important outcomes considered? |
| No. Adverse events were not considered as an outcome measure. Signs of infection were not considered as outcome measures. |
| 11. Are the benefits worth the harms and costs? |
| The study shows that amoxicillin and moxifloxacin prophylaxis showed high efficacies (p < 0.001 and p < 0.05 respectively) in reducing prevalence and duration or bacteraemia following dental extraction, and therefore beneficial. This of course in turn would be highly likely to reduce postoperative complications. Commonly prescribed antibiotics used in dentistry are relatively cheap in the UK, however the type of antibiotic prescribed to patients should be strongly considered by prescribers as well as considering the genuine need for that particular patient, for example, in general, the elderly, immunocompromised and younger patients would seem more likely to benefit from prophylactic antibiotics as opposed to blind prescribing for each and every individual undergoing tooth extraction. |
| Section (A) Are the results of the review valid? |
| Screening Questions 1. Did the trial address a clearly focused issue? |
| Yes. The authors attempted to test the efficacy of two dosing regimens of prophylactic antibiotics for the removal of impacted third molars. The Intervention used was metronidazole 1 g orally 1hr preoperatively vs. metronidazole 400 mg orally 4 times daily for 5 days vs. placebo. |
| 2. Was the assignment of patients to treatments randomised? |
| Method of sequence generation was not fully described; however, study claims to have used randomisation in sealed envelopes (allocation). |
| 3. Were all of the patients who entered the trial properly accounted for at its conclusion? |
| 151 patients were randomised at the beginning of the study and 125 were accounted for at its conclusion. The results of those who did not complete the study were also provided and statistically analysed, finding no significant differences between groups. |
| Detailed questions 4. Were patients, health workers and study personnel ‘blind’ to treatment? |
| The outcome assessor was blinded to allocated treatment. Study is described as double-blind (dosing schedule is different in each group). |
| 5. Were the groups similar at the start of the trial? |
| Size of all four groups saw slight variation in number of participants shown below. The composition of each group saw slight variations: Metronidazole 1 g orally 1 h preoperatively (n = 44): 25 (M)/19 (F), mean age = 28 years Metronidazole 400 mg orally 4 times daily for 5 days (n = 47): 30 (M)/17 (F), mean age = 29 years Placebo (n = 34): 15 (M)/19 (F), mean age = 26 years The range of total extractions per group ranged from 99–103. |
| 6. Aside from the experimental intervention were the groups treated equally? |
| All patients were subjected to the same inclusion/exclusion criteria and all extractions were conducted in one treatment centre in India. It is worthy to note however that surgeons performing the extraction were of different skill levels i.e., some were consultants, post-graduate trainees or house officers. |
| Section (B) What are the results? |
| 7. How large was the treatment effect? |
| No significant differences in outcome between three groups (p = 0.09). The only significant difference seen was the degree of swelling in the 5 day group (p = 0.03). Overall, antibiotic prophylaxis does not seem to reduce morbidity after third molar extraction surgery. |
| 8. How precise was the estimate of the treatment effect? |
| No confidence intervals are provided. Only standard deviation figures were provided for individual results. Overall the study showed no statistically significant results to recommend prophylactic antibiotics for the extraction of third molars. |
| Section (C) Will the results help locally? |
| 9. Can the results be applied in your context? (or to the local population?) |
| Results may not be applicable to a general population. Patients did not comprise of the elderly, young children, immunocompromised patients or those at risk of IE. A larger sample size would be required. Furthermore, surgeons were of different skill levels and the procedure itself was not carried out in a dental practice were most extractions are carried out in the UK. |
| 10. Were all clinically important outcomes considered? |
| No. Adverse events were not considered as an outcome measure. |
| 11. Are the benefits worth the harms and costs? |
| Results were not statistically significant (p > 0.05), and so there is not enough evidence to support the use of antibiotics in this case. Metronidazole is relatively cheap in the UK but the risk of other complications such as microbial resistance may outweigh the benefit if it is to be routinely prescribed for a procedure which in this case has failed to show statistically significant results. |
| Section (A) Are the results of the review valid? |
| Screening Questions 1. Did the trial address a clearly focused issue? |
| Yes. To evaluate the efficacy of antibiotic prophylaxis for dental implant placement. The intervention used was amoxicillin 2 g pre-op vs. amoxicillin 2 g daily pre & post-op (7 days) vs. amoxicillin 2 g post-op (7 days) vs. placebo. Outcomes considered were implant failure, postoperative complications assessed post-op at weeks 1, 2, 4 and 8, adverse events. |
| 2. Was the assignment of patients to treatments randomised? |
| Yes. Computer generated restricted randomisation lists (13 in total) were formed using equal groups of participants. Randomised codes were enclosed in sequentially numbered, identical, opaque, sealed envelopes. Treatment allocation was concealed to investigators in charge of enrolling and treating the patients. |
| 3. Were all of the patients who entered the trial properly accounted for at its conclusion? |
| Two exclusions were made from the control group (antibiotic group) and one from the non-antibiotic group with reasons provided. Patients were analysed in groups they were randomised to. |
| Detailed questions 4. Were patients, health workers and study personnel ‘blind’ to treatment? |
| Yes. Patients and operators/outcome assessors were blinded to intervention. The statistician was also kept blind when performing all analyses for this study |
| 5. Were the groups similar at the start of the trial? |
| Yes. Similar Amoxicillin group (n = 52): 114 (M)/138 (F). Mean age 49.1 Placebo group (n = 254): 112 (M)/132 (F). Mean age 47.9 |
| 6. Aside from the experimental intervention were the groups treated equally? |
| Yes. Patients were treated in 10 private Italian practices. The number of implant placements for each group were similar (498; antibiotic group vs. 483; control group). |
| Section (B) What are the results? |
| 7. How large was the treatment effect? |
| No statistically significant differences were seen to be observed. However trends to favour the antibiotic group. The study furthermore concludes immediate post-extractive implants were more likely to fail. Implant failure: 7 in antibiotic group vs. 13 placebo group Prosthesis failure: 4 failures in antibiotic group vs. 10 placebo group Adverse events: none reported. Post-operative complications: 11 in antibiotic group vs. 13 in placebo group |
| 8. How precise was the estimate of the treatment effect? |
| Confidence interval not provided. p = 0.083 for overall implant losses (not statistically significant). |
| Section (C) Will the results help locally? |
| 9. Can the results be applied in your context? (or to the local population?) |
| Cannot tell. Implant placement is not limited to sex/age. Most patients in this trial were >40 years. Results may not be generalisable to a whole general population. Patients did not comprise of the elderly, young children, immunocompromised patients or those at risk of IE. A larger sample size would be required. |
| 10. Were all clinically important outcomes considered? |
| Yes. All outcomes considered and reported, however confidence intervals should have been provided. A different dosing regimen group could also have been used. |
| 11. Are the benefits worth the harms and costs? |
| Can’t tell. Trends are clearly in favour of antibiotics as more implant, prosthesis failures and post-operative complications were seen in the placebo group vs. antibiotic group. Despite this the results were not statistically significant (p = 0.083). No adverse events were reported but this may be due to the small sample size of the study. Amoxicillin is relatively cheap in the UK but the risk of other complications such as microbial resistance may outweigh the benefit if it is to be routinely prescribed for a procedure which fails to show statistically significant results. |
| Section (A) Are the results of the review valid? |
| Screening Questions 1. Did the trial address a clearly focused issue? |
| Yes. The authors attempted to evaluate the efficacy of two antibiotic regimens (single dose clindamycin and multidose clindamycin (5 days) for the reduction of inflammatory complications in patients undergoing third molar surgery with bone removal (extraction). Outcomes of interest were trismus, facial swelling, body temperature, pain, submandibular lynphadenopathy and alveolar osteitis. |
| 2. Was the assignment of patients to treatments randomised? |
| A random number table was used for to determine group assignment for each patient in advance. Furthermore, allocation concealment involved opaque and sequentially numbered envelopes. |
| 3. Were all of the patients who entered the trial properly accounted for at its conclusion? |
| Nine out of 100 patients did not check in for follow up. Three had been disqualified due to various described complications and two had resigned during the trail without stating any reasons. Therefore 86 patients in total were analysed statistically at the end of the trial. |
| Detailed questions 4. Were patients, health workers and study personnel ‘blind’ to treatment? |
| Patients, clinicians and statisticians were all blinded. |
| 5. Were the groups similar at the start of the trial? |
| Sizes of all three groups were similar (n = 27–31) The composition of each group was very similar except one group composed of a higher female population. Clindamycin 600 mg preoperatively then 300 mg placebo for 5 days: 8 (M)/23 (F), mean age = 23.4 years Clindamycin 600 mg preoperatively then 300 mg placebo for 5 days post-op: 9 (M)/19 (F), mean age = 23.5 years placebo: 6 (M)/21 (F), mean age = 24.6 years Total extractions between groups ranged from 27–31. |
| 6. Aside from the experimental intervention were the groups treated equally? |
| Yes. All groups were treated at one treatment center in Poland and subject to the same inclusion/exclusion criteria. |
| Section (B) What are the results? |
| 7. How large was the treatment effect? |
| There was no statistically significant differences observed between groups for postoperative alveolar osteitis, pain scores, postoperative trismus and facial swelling (p > 0.05). Regarding a change in body temperature, a statistically significant difference between groups was recorded (p = 0.03). Despite this one statistically significant result for this study, the authors conclude that there is not enough evidence to suggest that clindamycin used prophylactically by itself or with subsequent 5-day therapy fails to demonstrate significant efficacy for prevention of inflammatory complications after third molar surgery. |
| 8. How precise was the estimate of the treatment effect? |
| The X2 test was used to evaluate trismus, facial swelling, lymphadenopathy and alveolar osteitis using an odds ratio with a confidence interval of 95%. The Krukal-Wallis rank test was used to analyse surgery duration, analgesic intake, body temperature and level of pain experienced. |
| Section (C) Will the results help locally? |
| 9. Can the results be applied in your context? (or to the local population?) |
| Results may not be applied to a whole general population. Patients were not treated in a general dental surgery, where most extractions take place. Patients did not comprise of the elderly, young children, immunocompromised patients or those at risk of IE. The mean age of patients across all three groups was in the mid 20’s, and so they may be more applicable to younger adults, however even then, larger sample sizes than this study would also require to represent a typical population of patients. |
| 10. Were all clinically important outcomes considered? |
| No. All-important outcomes were considered except adverse events were not reported. |
| 11. Are the benefits worth the harms and costs? |
| Results described above are not statistically significant. In the case of this study, adverse events were not reported. With regards to cost, clindamycin is relatively cheap in the UK but the risk of other complications such as microbial resistance may outweigh the benefit if it is to be routinely prescribed for an extraction procedure which is uncomplicated and of short duration. Overall, the study shows there is little benefit from taking prophylactic antibiotics for the reduction in inflammatory complications following third molar surgery. |
| Section (A) Are the results of the review valid? |
| Screening Questions 1. Did the trial address a clearly focused issue? |
| Yes. The authors attempted to evaluate the efficacy of two sustained release antibiotic regimens for the reduction of infection after third molar surgery (extraction): Pre-op amoxicillin/clavulanate 2000/125 mg vs post-op amoxicillin/clavulanate 2000/125 mg vs. placebo (5 day treatment). Outcomes of interest were Infection (purulent discharge in surgical site, pain, local abscess, increased heat, pyrexia, trismus, dental osteitis. All evaluated on days 1, 3, 7 post-op. |
| 2. Was the assignment of patients to treatments randomised? |
| Allocation concealment is not mentioned and therefore an unclear risk. Also random sequence generation is mentioned as randomised, however the method of how it was generated has not been provided. |
| 3. Were all of the patients who entered the trial properly accounted for at its conclusion? |
| Every patient was accounted for at conclusion. |
| Detailed questions 4. Were patients, health workers and study personnel ‘blind’ to treatment? |
| All were blinded. |
| 5. Were the groups similar at the start of the trial? |
| Size of all four groups were identical (n = 75 for each group). The composition of each group was very similar except one group composed of a higher female population. Pre-op amoxicillin/clavulanate 2000/125 mg: 33 (M)/42 (F), mean age = 29.7 years post-op amoxicillin/clavulanate 2000/125 mg: 37 (M)/48 (F), mean age = 52 years placebo: 26 (M)/49 (F), mean age = 28.2 years Each group had a total of 75 extractions (1 extraction per patient) |
| 6. Aside from the experimental intervention were the groups treated equally? |
| Yes. All groups were treated at one treatment centre and subject to the same inclusion/exclusion criteria. |
| Section (B) What are the results? |
| 7. How large was the treatment effect? |
| Higher rate of infection was seen in placebo group (16%) vs. single dose prophylaxis (5.3%) vs. 5 day pre-emptive therapy (2.7%) (p = 0.006) meaning results were statistically significant. A significant result was seen in the correlation between the longer duration of surgery and rate of infection (p = 0.011) (although initially this was not an outcome of interest). Pre-emptive and pre-operative antibiotics vs. placebo saw a greater reduction of postoperative pain on day 3 (p = 0.0001) Overall pre-emptive therapy is better suited for more complex procedures (extraction including bone removal). Prophylaxis is more beneficial in simpler procedures. |
| 8. How precise was the estimate of the treatment effect? |
| Details on CI were not included for results of the study; however they were provided for the reasoning behind why 75 patients were required in each study group in order to achieve a sufficient sample size (based on a previous pilot study with smaller samples sizes) |
| Section (C) Will the results help locally? |
| 9. Can the results be applied in your context? (or to the local population?) |
| Results may not be generalisable to a whole general population. Patients were not treated in a general dental surgery, where most extractions take place. Patients did not comprise of the elderly, young children, immunocompromised patients or those at risk of IE. The mean age of patients across all three groups was in the late 20’s. A larger sample size would also be required. |
| 10. Were all clinically important outcomes considered? |
| Yes, however the CI for each outcome considered was not provided (although p values were). |
| 11. Are the benefits worth the harms and costs? |
| Results described above are statistically significant. Generally adverse events were seen more frequently in the pre-emptive antibiotic group and with greater effect compared to prophylaxis and placebo groups. Therefore the choice of antibiotic regimen should be carefully considered when judging the difficulty of extraction and the benefits of administration to each individual patient. With regards to cost, amoxicillin is relatively cheap in the UK but the risk of other complications such as microbial resistance may outweigh the benefit if it is to be routinely prescribed for an extraction procedure which is uncomplicated and of short duration. |
| Section (A) Are the results of the review valid? |
| Screening Questions 1. Did the trial address a clearly focused issue? |
| Yes. The study compared the efficacyand safety of oral amoxicillin 2 g with identical placebo tablets taken prophylacticaly (1 h before implant placement) for single dental implants in bone type 2 & 3. Outcomes considered. Outcomes of interest included implant failure, postoperative complications assessed post-op at weeks 1, 2, 4 & 8, adverse events and microbiological evaluation. |
| 2. Was the assignment of patients to treatments randomised? |
| How was this carried out? Was the allocation sequence concealed from researchers and patients? Yes. Researchers had a concealed envelope for each patient to establish randomly assigned treatment if necessary (envelope opened at end of study). If a side effect was observed, then the clinician was allowed to open the envelope before the end of the study. |
| 3. Were all of the patients who entered the trial properly accounted for at its conclusion? |
| A 52 patients were enrolled into the antibiotic group and 53 patients were enrolled into the placebo group for which results for all patients were given at the end of the study. |
| Detailed questions 4. Were patients, health workers and study personnel ‘blind’ to treatment? |
| Yes. Researchers and patients were blinded to the received treatment group. |
| 5. Were the groups similar at the start of the trial? |
| Size of both groups were almost identical (antibiotic group n = 52 & non antibiotic group n = 53. The composition of each group was also similar except the male to female ratio in one of the groups: Amoxicillin 2 g 1h pre-op: 15 (M)/37 (F), mean age = 49 years. Placebo (identical tablets) 2 g 1hr pre-op: 20 (M)/33 (F), mean age 53. |
| 6. Aside from the experimental intervention were the groups treated equally? |
| Yes. This study only included people requiring a single implant into bone of medium quality. Only one implant was provided to each patient in each group. Patients were also treated in same country (8 Spanish dental practices) |
| Section (B) What are the results? |
| 7. How large was the treatment effect? |
| Outcome measures included: Implant failures: 2 failures occurred in each group Adverse events: none reported Postoperative infections: 6 in each group. The probability of not having and infection was 88.8% in the non-antibiotic group vs. 88.8% in the antibiotic group. No statistical differences reported (p = 0.0960) Characteristics of saprophytic flora: no statistically significant results observed, the amoxicillin did not alter or modify the nature of the saprophytic flora (p = 0.362) Overall the study concludes that there is no statistically significant data to suggest antibiotic prophylaxis when placing single implants in patients with bone types 2 & 3. |
| 8. How precise was the estimate of the treatment effect? |
| The type of treatment applied did not significantly affect the probability of occurrence of infections (OR 0.97—CI 95% 0.29–3.2) |
| Section (C) Will the results help locally? |
| 9. Can the results be applied in your context? (or to the local population?) |
| Results may not be generalisable to a whole general population. Patients did not comprise of the elderly, young children, immunocompromised patients or those at risk of IE. A larger sample size would be required. Furthermore, only patients with bone types 2 & 3 were used and so results are more applicable to these patients. |
| 10. Were all clinically important outcomes considered? |
| Yes. All outcomes considered and reported. A different dosing regimen group could also have been tested. |
| 11. Are the benefits worth the harms and costs? |
| Not in this case. Insufficient statistically significant evidence. Results were not statistically significant (p > 0.05). Amoxicillin is relatively cheap in the UK but the risk of other complications such as microbial resistance may outweigh the benefit if it is to be routinely prescribed for a procedure which fails to show statistically significant results. |
| Section (A) Are the results of the review valid? |
| Screening Questions 1. Did the trial address a clearly focused issue? |
| Yes. The authors attempted to determine the minimum effective regimen of antibiotic prophylaxis (amoxicillin) for dental implant surgery. The intervention used was amoxicillin 2 g pre-op vs. amoxicillin 2 g daily pre-& post-op (7days) vs. amoxicillin 2 g post-op (7days) vs. placebo. |
| 2. Was the assignment of patients to treatments randomised? |
| No information regarding the allocation concealment procedure was provided. A computer generated randomisation list was produced to allocate patients into one of four groups. |
| 3. Were all of the patients who entered the trial properly accounted for at its conclusion? |
| All adults were treated in two private Italian dental practices. Results for all 100 patients (4 groups of 25) who entered the trial were provided at the end of the trial. |
| Detailed questions 4. Were patients, health workers and study personnel ‘blind’ to treatment? |
| Operators were not blinded as they were recording the outcome measures. |
| 5. Were the groups similar at the start of the trial? |
| Size of all four groups were identical (n = 25 for each group). The composition of each group saw slight variations: Amoxicillin 2 g 1 h pre-op (n = 25): 13 (M)/12 (F), mean age = 52 years Amoxicillin 2 g 1 h pre-op + amoxicillin 2 g daily for 7 days post-op (n = 25): 12 (M)/13 (F), mean age = 45 years Amoxicillin 2 g daily post-op for 7 days (n = 25): 7 (M)/18 (F), mean age = 42 years No antibiotic (n = 25): 10 (M)/15 (F), mean age = 43 years The range of total implants per group ranged from 29–48. |
| 6. Aside from the experimental intervention were the groups treated equally? |
| Yes. All groups were treated at two Italian private dental clinics subject to the same inclusion/exclusion criteria. |
| Section (B) What are the results? |
| 7. How large was the treatment effect? |
| Outcomes of interest included: Implant failure: 2 implant failures in no antibiotic group No postoperative complications observed post-op at weeks 1, 2, 4 and 8 Adverse events: none reported |
| 8. How precise was the estimate of the treatment effect? |
| Power analysis showed only 15% with confidence at 99% and 35% at 95% CI. However further calculations revealed that in order to achieve a power of 75% with 99% confidence, 133 samples are required in each group; a much larger quantity than the current 25 per group is required to further provide strong statistical evidence of the absence of treatment effect. |
| Section (C) Will the results help locally? |
| 9. Can the results be applied in your context? (or to the local population?) |
| Results may not be generalisable to a whole general population. Patients did not comprise of the elderly, young children, immunocompromised patients or those at risk of IE. A larger sample size would be required. |
| 10. Were all clinically important outcomes considered? |
| Yes. All outcomes considered and reported. A different dosing regimen group could also have been tested. |
| 11. Are the benefits worth the harms and costs? |
| Not in this case. Insufficient statistically significant evidence (p > 0.05). No adverse events were reported but this may be due to the small sample size of the study. Amoxicillin is relatively cheap in the UK but the risk of other complications such as microbial resistance may outweigh the benefit if it is to be routinely prescribed for a procedure which fails to show statistically significant results. |
References
- Lewis, M.A.O. Why we must reduce dental prescription of antibiotics: European Union Antibiotic Awareness Day. Br. Dent. J. 2008, 205, 537–538. [Google Scholar] [CrossRef] [PubMed]
- Alanis, A.J. Resistance to Antibiotics: Are We in the Post-Antibiotic Era? Arch. Med. Res. 2005, 36, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Guillemot, D. Antibiotic use in humans and bacterial resistance. Curr. Opin. Microbiol. 1999, 2, 494–498. [Google Scholar] [CrossRef]
- McCaul, L.; Jenkins, W.; Kay, E. The reasons for extraction of permanent teeth in Scotland: A 15-year follow-up study. Br. Dent. J. 2001, 190, 658–662. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Surgeons of England (RCS). Guidelines for Selecting Appropriate Patients to Receive Treatment with Dental Implants: Priorities for the NHS; Royal College of Surgeons of England (RCS): London, UK, 2014. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; Worthington, H.V. Interventions for replacing missing teeth: Antibiotics at dental implant placement to prevent complications. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Scottish Intercollegiate Guidelines Network (SIGN). Antibiotic Prophylaxis in Surgery; A National Clinical Guideline. SIGN 104; SIGN: Edinburgh, Scotland, 2014. [Google Scholar]
- Gynther, G.; KÃndell, P.Ã.; Moberg, L.; Heimdahl, A. Dental implant installation without antibiotic prophylaxis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1998, 85, 509–511. [Google Scholar] [CrossRef]
- Martin, M.V.; Kanatas, A.N.; Hardy, P. Antibiotic prophylaxis and third molar surgery. Br. Dent. J. 2005, 198, 327–330. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.B.; Larson, E.L. Antibiotic prophylaxis and postoperative complications after tooth extraction and implant placement: A review of the literature. J. Dent. 2007, 35, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, A.; Morkel, J.A.; Zafar, S. Antibiotic prophylaxis in third molar surgery: A randomized double-blind placebo-controlled clinical trial using split-mouth technique. Int. J. Oral Maxillofac. Surg. 2010, 39, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Sekhar, C.H.; Narayanan, V.; Baig, M.F. Role of antimicrobials in third molar surgery: Prospective, double blind, randomized, placebo-controlled clinical study. Br. J. Oral Maxillofac. Surg. 2001, 39, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Scottish Dental Clinical Effectiveness Programme. Drug Prescribing for Dentistry. Dental Clinical Guide. 2011. [Google Scholar]
- Swift, J.Q.; Gulden, W.S. Antibiotic therapy managing odontogenic infections. Dent. Clin. N. Am. 2002, 46, 623–633. [Google Scholar] [CrossRef]
- Caiazzo, A.; Casavecchia, P.; Barone, A.; Brugnami, F.A. Pilot Study to Determine the Effectiveness of Different Amoxicillin Regimens in Implant Surgery. J. Oral Implantol. 2011, 37, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Palmer, N.; Pealing, R.; Ireland, R.; Martin, M. A study of prophylactic antibiotic prescribing in National Health Service general dental practice in England. Br. Dent. J. 2000, 189, 43–46. [Google Scholar] [PubMed]
- Dar-Odeh, N.; Abu-Hammad, A.; Khraisat, S. Antibiotic prescribing practices by dentists: A review. Ther. Clin. Risk Manag. 2010, 6, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.; Calder, L.; Thomas, D.W. Antibiotic prescribing for dental conditions: General medical practitioners and dentists compared. Br. Dent. J. 2000, 188, 398–400. [Google Scholar] [PubMed]
- Salako, N.O.; Rotimi, V.O.; Adib, S.; Al-Mutawa, S. Pattern of antibiotic prescription in the management of oral diseases among dentists in Kuwait. J. Dent. 2004, 32, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Al-Haroni, M.S. Knowledge of prescribing antimicrobials among Yemeni general dentists. Acta Odontol. Scand. 2006, 64, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Ramu, C.; Padmanabhan, T.V. Indications of antibiotic prophylaxis in dental practice- review. Asian Pac. J. Trop. Biomed. 2012, 2, 749–754. [Google Scholar] [CrossRef]
- Joint Formulary Committee (Ed.) British National Formulary; BMJ Group & Pharmaceutical Press: London, UK, 2013.
- World Health Organization. Essential Medicines and Health Products: Antimicrobial Resistance. 2014. Available online: http://www.who.int/medicines/areas/rational_use/emp_amr/en/ (accessed on 1 October 2018).
- World Health Organization. Global Antimicrobial Resistance Surveillance System (GLASS) Report: Early Implementation 2016–2017. 2017. Available online: http://www.who.int/glass/resources/publications/early-implementation-report/en/ (accessed on 1 October 2018).
- Public Health: European Commission. EU Action on Antimicrobial Resistance: Factsheet. 2018. [Google Scholar]
- Public Health: European Commission. EU One Health Action Plan Against AMR. 2017. [Google Scholar]
- World Health Organization. WHO Global Strategy Recommendations; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Tidy, C. Infective Endocarditis. 2015. Available online: https://patient.info/doctor/infective-endocarditis-pro (accessed on 1 October 2018).
- National Institute for Health and Clinical Excellence (NICE). NICE guidance on prophylaxis against infective endocarditis. Inpharma Weekly 2008, 2. [Google Scholar]
- Medical Protection Society (2013) Antibiotic Prophylaxis. Dental Protection [online]. Available online: http://www.dentalprotection.org/uk/news/positionstatements/ABcover (accessed on 28 December 2013).
- Gupta, D.M.; Boland, R.J.; Aron, D.C. The physicians experience of changing clinical practice: A struggle to unlearn. Implement. Sci. 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Cottingham, K.J. Summary of: NICE guideline and current practice of antibiotic prophylaxis for high risk cardiac patients (HRCP) among dental trainers and trainees in the United Kingdom (UK). Br. Dent. J. 2012, 213, 180–181. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sibbald, B.; Roland, M. Understanding Controlled Trials: Why Are Randomised Controlled Trials Important? BMJ 1998, 316, 201. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Orive, G.; Aguirre, J.J.; Ardanza, B.; AndÃa, I. 5-year clinical experience with BTI®dental implants: Risk factors for implant failure. J. Clin. Periodontol. 2008, 35, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarzyk, T.; Wichlinski, J.; Stypulkowska, J.; Zaleska, M.; Pana, M.; Woron, J. Single-dose and multi-dose clindamycin therapy fails to demonstrate efficacy in preventing infectious and inflammatory complications in third molar surgery. Int. J. Oral Maxillofac. Surg. 2007, 36, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Dios, D.P.; Carmona, I.T.; Posse, L.J.; Henriquez, M.J.; Feijoo, F.J.; Fernandez, A.M. Comparative Efficacies of Amoxicillin, Clindamycin, and Moxifloxacin in Prevention of Bacteremia following Dental Extractions. Antimicrob. Agents Chemother. 2006, 50, 2996–3002. [Google Scholar] [CrossRef] [PubMed]
- Lacasa, J.M.; Jimenez, J.A.; Ferras, V.; Bossom, M.; Sola-Morales, O.; Garcia-Rey, C.; Aguilar, L.; Garau, J. Prophylaxis versus pre-emptive treatment for infective and inflammatory complications of surgical third molar removal: A randomized, double-blind, placebo-controlled, clinical trial with sustained release amoxicillin/clavulanic acid (1000/62.5 mg). Int. J. Oral Maxillofac. Surg. 2007, 36, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Lodi, G.; Figini, L.; Sardella, A.; Carrassi, A.; Del Fabbro, M.; Furness, S. Antibiotics to prevent complications following tooth extractions. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef]
- The Cochrane Collaboration. The Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011.
- Soheilipour, S.; Scambler, S.; Dickinson, C.; Dunne, S.M.; Burke, M.; Jabbarifar, S.E.; Newton, J.T. Antibiotic prophylaxis in dentistry: Part I. A qualitative study of professionals’ views on the NICE guideline. Br. Dent. J. 2011, 211, E1. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibiotic | Class | Drug Mechanism | Spectrum of Activity | Common Indications in Dentistry | Dose Range | Comments |
|---|---|---|---|---|---|---|
| Amoxicillin | Penicillin | Inhibits biosynthesis of cell wall | Broad spectrum. Active against certain gram + and gram − organisms | Dentoavleolar abscess | 250 mg three times daily (dose can be doubled in severe infections) | Just as effective as phenoxymethyl penicillin but better absorbed. Ineffective to beta lactamase producing organisms. |
| Ampicillin | Penicillin | Inhibits biosynthesis of cell wall | Broad spectrum. Active against certain gram + and gram − organisms | Dentoavleolar abscess | 500–1000 mg four times daily | See amoxicillin |
| Penicillin V Phenoxymethylpenicillin | Penicillin | Inhibits biosynthesis of cell wall | More active against gram + than gram - | Dentoavleolar abscess. Should not be used in serious infections. | 500 mg four times daily (dose can be doubled in severe infections) | Gastric acid-stable therefore suitable for oral administration unlike penicillin G |
| Co-Amoxiclav | Penicillin | Inhibits biosynthesis of cell wall | Broad spectrum. Active against beta-lactamase producing bacteria resistant to amoxicillin | Severe dental infection with spreading cellulitis or dental infection non-responsive to 1st line antibacterial. | 250 mg/125 mg (ampicillin/clauvic acid) combination tablet three times daily (higher dose of 500 mg/125 mg in severe infections) | A mixture of clauvulanic acid acting as beta-lacamase inhibitor (as potassium clavulanate) and amoxicillin (as trihydrate/sodium salt) |
| Cefalexin | Cephalosporin | Binds to penicillin binding proteins and inhibits cell wall synthesis. | More active against aerobes | Dental infections resistant to penicillin VK | 250–1500 mg four times daily | Offer little advantage over penicillin’s in dental infections but useful in those with hypersensitivity to penicillin’s |
| Cefradine | Cephalosporin | Binds to penicillin binding proteins and inhibits cell wall synthesis. | More active against aerobes | Dental infections resistant to penicillin VK | 250–1000 mg four times daily | See Cephalexin |
| Metronidazole | Metronidazole | Inhibiting nucleic acid synthesis | High activity against anaerobic bacteria and protozoa | Acute necrotising gingivitis, pericoronitis | 200–250 mg three times daily | High concentration builds up achievable in tissue. |
| Clarithromycin | Macrolide | Inhibits bacterial peptide translation | Similar but not identical to penicillin | 2nd line drug treatment for dental abscess | 250–500 mg twice daily | Many organisms rapidly develop resistance to macrolides; use should be limited to short courses |
| Doxycycline | Tetracycline | Inhibits bacterial protein synthesis | Effective against oral anaerobes. | Sinusitis | 200 mg initially, 100 mg daily | Due to antibiotic resistance, especially by oral streptococci, tetracycline usefulness is reduced in acute oral infections. |
| Level of Bias | Description |
|---|---|
| High risk | Possible bias seriously affecting the reliability of the results and high risk of bias if one or more of the criteria were not met |
| Low risk | Possible bias not seriously affecting the reliability of the results and low risk of bias if all criterion met |
| Study | Patient Blinding | Assessor Blinding | Allocation Concealment | Withdrawals | Risk of Bias |
|---|---|---|---|---|---|
| Anitua et al. (2009) | Yes | Yes | Concealed | None | Low |
| Caiazzo et al. (2011) | Yes | Yes | Unclear | None | High |
| Esposito et al. (2010) | Yes | Yes | Concealed | Yes (enough reasons have been provided) | Low |
| Sekhar et al. (2001) | Yes | Yes | Concealed | Yes | High |
| Dios et al. (2006) | Yes | Yes | Concealed | None | Low |
| Kaczmarzyk et al. (2007) | Yes | Yes | Concealed | Yes | High |
| Lacasa et al. (2007) | Yes | Yes | Unclear risk | None | Low |
| Study (Author) | Extraction/Implant | Intervention | Number of Participants | Gender (m/f) | Mean Age (Years) | Number of Extractions/Implants |
|---|---|---|---|---|---|---|
| Caiazzo et al. | Implant | Amoxicillin 2 g 1 h pre-op | 25 | 13/12 | 52 | 35 |
| Amoxicillin 2 g 1 h pre-op + amoxicillin 2 g daily for 7 days post-op | 25 | 12/13 | 45 | 36 | ||
| Amoxicillin 2 g daily post-op for 7 days | 25 | 7/18 | 42 | 48 | ||
| No antibiotic | 25 | 10/15 | 43 | 29 | ||
| Anitua et al. | Implant | Amoxicillin 2 g 1 h pre-op | 52 | 15/37 | 49 | 52 |
| Placebo (identical tablests) 2 g 1 h pre-op | 53 | 20/33 | 47 | 53 | ||
| Esposito et al. | Implant | Amoxicillin 2 g 1 h pre-op | 252 | 114/138 | 49.1 | 489 |
| Placebo (no antibiotic) | 254 | 122/132 | 47.6 | 483 | ||
| Sekhar et al. | Extraction | Metronidazole 1 g orally 1 h preoperatively | 44 | 25/19 | 28 | 99 |
| Metronidazole 400 mg orally 4 times daily for 5 days | 47 | 30/17 | 29 | 101 | ||
| placebo | 34 | 15/19 | 26 | 103 | ||
| Dios et al. | Extraction | Amoxicillin 2 g preoperatively | 56 | 34/22 | 23.8 | 56 |
| moxifloxacin 400 mg preoperatively | 58 | 29/29 | 22.4 | 58 | ||
| clindamycin 600 mg preoperatively | 54 | 34/20 | 24 | 54 | ||
| Placebo | 53 | 29/24 | 26.1 | 53 | ||
| Kaczmarzyk et al. | Extraction | Clindamycin 600 mg preoperatively then 300 mg placebo for 5 days | 31 | 8/23 | 23.4 | 31 |
| Clindamycin 600 mg preoperatively then 300 mg placebo for 5 days post-op | 28 | 9/19 | 23.5 | 28 | ||
| placebo | 27 | 6/21 | 24.6 | 27 | ||
| Lacasa et al. | Extraction | Pre-op amoxicillin/clavulanate 2000/125 mg | 75 | 33/42 | 29.7 | 75 |
| post-op amoxicillin/clavulanate 2000/125 mg | 75 | 37/38 | 29.5 | 75 | ||
| placebo | 75 | 26/49 | 28.2 | 75 |
| Study (Author) | Complication/Procedure | Intervention | Patient Sample Size | Study Design | Outcomes Assessed | Location | Results | Comments |
|---|---|---|---|---|---|---|---|---|
| Sekhar et al. (2001) | Lower wisdom tooth extraction | Metronidazole 1 g orally 1h preoperatively vs. metronidazole 400 mg orally 4 times daily for 5 days vs placebo | n = 151 | 3-arm, randomised, double blind | Purulent discharge from wound, dry socket, swelling, pain score | India | Overall, no significant differences in groups from any of the variables. | Outcome assessment procedures were not clearly specified. No power analysis performed. At enrolment patients’ key characteristics not fully assessed. |
| Kaczmarzyk et al. (2007) | Extraction of third molar tooth. | Clindamycin 600 mg preoperatively then 300 mg placebo vs. Clindamycin 600 mg preoperatively then 300 mg placebo post-op vs. placebo (5 day treatment) | n = 86 | 3-arm prospective, randomised, double blind | Using 4-grade scale: Trismus, facial swelling, pain, body temperature & alveolar osteitis. All evaluated on day 1, 2 and 7 (post-op) | Poland | No statistically significant differences in post-op complication rates for third molar extraction from any group. | Incomplete outcome data (attrition bias)—14% patients lost at follow up. Inclusion criteria basic. Exclusion criteria well described. Power analysis performed. Demographic, objective and subjective data clearly defined. |
| Dios et al. (2006) | Tooth extraction for any indication | Amoxicillin 2 g preoperatively vs. moxifloxacin 400 mg vs. clindamycin 600mg (preoperatively vs. placebo (5 day treatment) | n = 221 | 3-arm, randomised, double blind | Postoperative bacteraemia levels determined by microbiological analysis of blood cultures. | Spain | Postoperative measurements of bacteraemia showed decrease in amoxicillin and moxifloxacin (p < 0.0001) vs. placebo | Clear exclusion criteria described, however unclear description of inclusion criteria. Power analysis performed. |
| Lacasa et al. (2006) | Third mandibular surgery required | Pre-op amoxicillin/clavulanate 2000/125 mg vs. post-op amoxicillin/clavulanate 2000/125 mg vs. placebo (5 day treatment) | n = 225 | 3-arm randomised, double blind, parallel, phase III comparative study | Infection (purulent discharge in surgical site, pain, local abscess, increased heat, pyrexia, trismus, dental osteitis. All evaluated on days 1,3,7 post-op. | Spain | Higher rate of infection was seen in placebo group (16%) vs. single dose prophylaxis (5.3%) vs. 5 day pre-emptive therapy (2.7%) (p = 0.006) | Patients lost at each follow up not mentioned. Incomplete outcome data (attrition bias). Randomisation method not clearly defined. Two authors are employed by the funding company. |
| Study (Author) | Complication/Procedure | Intervention | Sample Size | Study Design | Outcomes Assessed | Location | Results | Comments |
|---|---|---|---|---|---|---|---|---|
| Caiazzo et al. (2010) | Dental implant surgery | Amoxicillin 2 g pre-op vs. Amoxicillin 2 g daily pre & post-op (7days) vs. amoxicillin 2 g post-op (7days) vs. placebo | n = 100 | 4-arm, prospective, multicentre parallel, randomised, study (3 month study) | Implant failure, postoperative complications assessed post-op at weeks 1,2,4 and 8, adverse events | Italy | Overall success rate 98.65%. No significant differences between expt. groups (p < 0.05). no implant failures in antibiotic groups, 2 failures in non-antibiotics groups. | Allocation concealment information not provided. No information provided for blinding of operators. |
| Esposito et al. (2010) | Dental implant surgery | Amoxicillin 2g pre-op vs. placebo | n = 506 | Randomised, multicentre, double blind, placebo controlled & parallel (4 month duration) | Implant & prosthesis failure. Post-op complications (assessed weeks 1 & 2 post-op), and adverse events. | Italy | No statistically significant differences observed between groups but trend favoured antibiotic administration. More implant losses in placebo group (p = 0.083) | Limitations of the study well described. Allocation concealment information well provided. Information provided for blinding of operators. All outcome measures reported. |
| Anitua et al. (2009) | Dental implant surgery | Amoxicillin 2g preoperatively vs. moxifloxacin 400 mg vs clindamycin 600 mg preoperatively vs placebo | n = 105 | Randomised, multicentre, double blind, parallel, placebo controlled | Postoperative infections, microbiological analysis, adverse events and implant failures. | Spain | Six post op infections occurred and 2 implant failures in each group. No statistically significant differences observed between groups. | No patient drop outs. Results may be applicable to bone types II & 3 only. No other bone types investigated. |
| Numbers Need to Treat (NNT) |
|---|
| Control group event rate (CER): proportion of outcomes that occur in control group. Experimental group event rate (EER): proportion of outcomes that occur in the experimental group. Absolute risk reduction (ARR) = CER − EER Number needed to treat (NNT) = 1/ARR To prevent implant failure using prophylactic antibiotics: CER = 16/332 = 0.048 EER = 7/379 = 0.018 Absolute risk reduction (ARR) = 0.048 − 0.018 = 0.030 NNT = 1/0.030 = 33.333 Approximately 33 patients undergoing dental implant surgery need to receive antibiotics in order to prevent one implant failure from occurring (NNT) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh Gill, A.; Morrissey, H.; Rahman, A. A Systematic Review and Meta-Analysis Evaluating Antibiotic Prophylaxis in Dental Implants and Extraction Procedures. Medicina 2018, 54, 95. https://doi.org/10.3390/medicina54060095
Singh Gill A, Morrissey H, Rahman A. A Systematic Review and Meta-Analysis Evaluating Antibiotic Prophylaxis in Dental Implants and Extraction Procedures. Medicina. 2018; 54(6):95. https://doi.org/10.3390/medicina54060095
Chicago/Turabian StyleSingh Gill, Amrik, Hana Morrissey, and Ayesha Rahman. 2018. "A Systematic Review and Meta-Analysis Evaluating Antibiotic Prophylaxis in Dental Implants and Extraction Procedures" Medicina 54, no. 6: 95. https://doi.org/10.3390/medicina54060095
APA StyleSingh Gill, A., Morrissey, H., & Rahman, A. (2018). A Systematic Review and Meta-Analysis Evaluating Antibiotic Prophylaxis in Dental Implants and Extraction Procedures. Medicina, 54(6), 95. https://doi.org/10.3390/medicina54060095