Abstract
Inflammation in primary teeth (PT) is commonly associated with a lower sensibility to painful stimuli, compared to permanent teeth, and usually leads to late presentation for dental treatment. Data obtained on the molecular assessments of dental pulp and clinical examinations could guide practitioners to conduct precise diagnoses and correct treatments. The aim of our pilot study was to assess the levels of several biomarkers (e.g., mineralization, oxidative stress, and inflammation) in primary teeth. The research included 46 dental pulp specimens collected from the primary teeth of children and adolescents between the ages of 6 and 12. The experimental groups consisted of 18 samples collected from primary teeth with acute pulpitis and 15 samples from chronically inflamed pulp tissues. The control group was represented by 13 specimens acquired from clinically healthy primary teeth. The enzyme-linked immunosorbent assay (ELISA) technique was used to determine the protein expression of tumor necrosis factor-α (TNF-α), superoxide dismutase-3 (SOD-3), osteocalcin, and transforming growth factor-β1 (TGF-β1) in the lysates. Our results revealed that all of the studied parameters presented statistically significant (p ≤ 0.05) increased levels in both experimental groups compared to the control samples. Furthermore, osteocalcin presented statistically significant increased concentrations in chronically- versus acute-inflamed pulp samples (p ≤ 0.05). The studied molecules may have an influential role in acute and chronic pulp inflammation in primary teeth.
1. Introduction
Dental caries are produced by cariogenic bacteria, which, in a sugar-rich environment, release acids that demineralize the hard dental tissues. Carious lesions progress and cavities can be detected in the structures of the teeth if preventive actions are not employed in the early phases of demineralization [1]. Dentinal tubules are penetrated by bacteria and their metabolites, resulting in an inflammatory process and immunological responses in the dental pulp tissue. These types of reactions can stop bacterial infections in the early stages and promote pulpal healing by formatting a dentine barrier in the affected area. Local accumulation of inflammation mediators, such as cytokines, chemokines, and other molecules, such as growth factors and oxidative stress markers, characterize pulpitis [2].
TNF-α is a proinflammatory cytokine released by immune cells, as a response to an infection, and can stimulate the formation of acute-phase inflammation proteins or other proinflammatory cytokines, having, as a result, vasodilatation, increased permeability in blood vessels, and extravasation of leukocytes in the injured area [3]. Reactive oxygen intermediates (ROIs) are released during inflammation and are used by immune cells for antimicrobial actions, but they can also cause damage at cellular and extracellular levels if accumulated in high concentrations. TNF-α is also capable of stimulating the formation of ROI from neutrophils [4]. Antioxidant enzymes, such as SOD-3, are part of the local cellular defense mechanism and neutralize the harmful effects of ROIs by eliminating them in high amounts [5,6]. Mature odontoblasts take part in the formation of the new matrix of reactionary dentine, and in the latest differentiation stage, they express osteocalcin, a reparative protein generated as a response to injury of pulp tissue [7,8]. Furthermore, TGF-β1 is a capable modulator of tissue repair and may be part of reparative dentinogenesis by differentiating pulp cells into odontoblasts [9].
Dental pulp pathology classification may vary according to different authors and dental schools, and as a result, may lead to confusion. Irreversible pulp inflammation may be acute or chronic, depending on the clinical and histological findings [10]. Other terms for “irreversible acute inflammation” may be “irreversible symptomatic pulpitis”, while “irreversible chronic inflammation” may be found as “irreversible asymptomatic pulpitis”. We chose to study the levels of different biomarkers in the irreversible acute and chronic pulpal pathology of primary teeth because the reversible stages of pulpal inflammation in primary dentition are short in time and are not usually diagnosed due to the rapid evolution of the inflammation of irreversible pathology, and due to the late presentation of the patient at the dental clinic. Reversible stages of pulp inflammation are, in general, symptomless, or they are characterized by less intense and shorter episodes of pain, which can lead a patient to not seek immediate dental treatment [11].
Clinical and histological traits of irreversible dental pulp inflammation can characterize acute or chronic pulpitis [10]. Concerning the clinical terminology of pulp inflammation, manifestations depend on the duration of the injurious agent and the onset or lack of dental treatment, which will prevent further extension of the infection and will provide pulpal healing. Acute irreversible pulpitis is characterized by painful sudden episodes, which lead the patient to seek emergency dental treatment. The pain often lingers to cold stimuli and is constant and spontaneous; the patient is usually not able to precisely identify the painful tooth [12]. In most cases, analgesic medication is not effective. Microscopically acute inflammation is accompanied by increased vascular permeability, exudation of fluid, serum proteins, inflammatory mediators, and cells, especially polymorphonuclear leukocytes (PMN), into the affected area [13,14]. If the injurious agent is removed, healing of the dental pulp tissue can be achieved. Persistence of the injury may facilitate chronic dental pulp conditions [14].
Most cases of irreversible chronic pulpitis can be painless or a dull located pain may be present [10]. With chronic dental pulp inflammation, accumulation of a granuloma-like tissue and irreversible destruction of the parenchymal tissue, which is covered by a connective and fibrous tissue, takes place [13]. Fibroblasts and vascular endothelium proliferation, as well as an invasion of lymphocytes, plasma cells, macrophages, and inflammatory mediators occur [14]. Additionally, in irreversible chronic pulpitis, an activation of cell-mediated bacterial lysate, cytokine system, can be observed, together with T and B cell stimulation [13]. Chronic inflammation of the dental pulp may be preceded by an acute inflammatory process or it can be primary [14].
The World Health Organization (WHO) has reported that approximately 530 million children worldwide present dental caries in their primary dentitions, which, if left untreated, may cause pain, discomfort, tooth loss, or even infection [15]. Most oral health conditions are preventable if discovered and treated in the early stages [15]. A high intake of sugar from a very young age, absences, inconsistencies in following daily (and correct) oral hygiene practices, or susceptibility of teeth surfaces associated with longtime exposure, could contribute toward carious developments in primary teeth, which could rapidly progress to the dental pulp, leading to inflammation.
The structure of dental pulp in primary and permanent teeth is similar; it includes cells, fibers, blood vessels, and nerves. Dental pulp in primary teeth has some particularities, such as the regressive potential of all components in time, which contribute to the decrease of the pulp’s defense mechanisms, and as a result, irreversible pulp response rapidly occurs [16]. In the dental pulp of primary teeth, there are also less nerve fibers, less myelinated axons, and less mechanoreception complexes. Moreover, the development of subodontoblastic plexuses is incomplete, and they release short bundles in dentine and pre-dentine. With a moderate injury, the dental pulp of primary teeth can easily form tertiary dentine. The density of the dental nerve fibers is lower in primary versus permanent teeth; consequently, the two dentitions have different pain thresholds [16]. These peculiarities justify the lower pain sensibility of the deciduous teeth compared to the permanent teeth, and may partially explain the advanced progressive stage of the pulp tissue pathology, as well as the delayed presentation for treatment [16].
Numerous biomarkers have been evaluated in human inflamed dental pulp samples from permanent teeth, but to the best of our knowledge, only one study focused on primary dentition [17]. Additionally, not many studies include irreversible acute and chronically-inflamed pulp samples as experimental groups. In this context, we aimed to analyze several biomarkers in samples collected from the primary teeth of children with acute and chronically inflamed pulp versus clinically healthy pulp tissues; we expect that the results of this research will be helpful in the future, in making accurate diagnoses and treatments in pulpal pathology. We tested the hypothesis that various biochemical markers have different concentrations in healthy, acute inflamed, and chronically inflamed dental pulp tissues, collected from primary teeth.
2. Materials and Methods
2.1. Subjects
The present research included 46 participants, from 6 to 12 years of age, who sought dental treatment at the Pedodontics Department of the Carol Davila University of Medicine and Pharmacy in Bucharest, Romania. Informed consent was obtained from the legal guardians of all underaged patients. The study was approved by the Ethics Committee of the Carol Davila University of Medicine and Pharmacy (document no. 5751/05.03.2021). Our research included only healthy, medical condition-free, cooperative subjects.
2.2. Criteria for Diagnosis
Dental pulp from a single primary tooth of each patient was collected for the study (n = 46). Dental pulp samples were divided into three groups, according to the provenience: (a) primary teeth with clinical diagnoses of acute pulpitis (n = 18); (b) primary teeth with clinical diagnoses of chronic closed pulpitis (n = 15); and (c) clinically healthy primary teeth (n = 13). Experimental groups were represented by acute and chronically inflamed dental pulp samples while the control group consisted of clinically normal/healthy dental pulp tissue. All primary teeth included did not present pathologic root resorption of more than 2/3 of the root length. Acute inflamed pulp specimens were collected from primary teeth that presented deep cavities with/without fillings, having antecedents of spontaneous, diffuse, and lingering pain resilient to analgesics. Additionally, samples of dental pulp with chronic inflammation were obtained from teeth that presented deep cavities with/without fillings, having a closed pulp chamber, and with antecedents of dull pain or more episodes of dental pain, which could be precisely located. Percussion in the clinically acute inflamed teeth revealed a positive response, whereas the response for the chronically inflamed teeth was negative. Clinically acute inflamed teeth presented hyperexcitability at thermal (cold) stimulation. Chronically inflamed teeth presented hypoexcitability when tested with a cold stimulant. The control group was represented by clinically healthy dental pulp tissues, without a history of pain or presence of dental caries/fractures. Radiographic examinations were also performed to exclude the existence of root canal treatments, periapical pathosis, or other types of pathologies, which may interfere with the actual clinical diagnosis.
2.3. Procedures for Samples Collection
The samples were collected and prepared according to protocols previously published by Gusman et al. [18]. Aseptic conditions were applied for the dental pulp collection: professional cleaning of the teeth and cleaning of the tooth surfaces were performed with 70% alcohol. Infiltration anesthesia was administered for all teeth, while a “rubber dam” was placed for the teeth with acute and chronic pulp inflammation, avoiding blood and bacterial contamination. Pulpectomy was performed; after careful removal of the carious lesion and of the roof of the pulp chamber, pulp tissue with inflammation (acute and chronic) specimens were collected with sterile barbed broaches (VDW GmbH, Munich, Germany). A sterile saline solution at room temperature with minimal pressure was used to irrigate the root canals during the collection of the pulp tissues. The healthy dental pulp specimens were obtained after the extraction of deciduous teeth with prolonged retention on the dental arch. Subsequent to extraction, the teeth were split longitudinally with an elevator. Sterile spoon excavators (LM Dental, Planmeca Group, Parainen, Finland) were used to collect dental pulp tissues in a single piece, which were afterwards employed in Eppendorf tubes, together with 5 mL of saline solution, and stored at −70 °C until further analysis.
2.4. Pulp Lysates Preparation and Determination Using Enzyme-Linked Immunosorbent Assay (ELISA) Analysis
Dental pulp tissues were defrosted for 30 min. To prepare the phosphate-buffered saline (PBS) solution with pH 7.0, we dissolved 1 PBS tablet (Invitrogen/GIBCO, Waltham, MA, USA) in 50 mL of distilled water. Subsequently, we added 1 mL of PBS solution to each sample, and then crushed the pulp tissue with a glass rod. Afterwards, the samples were sonicated for 3 min and centrifuged for 10 min at 4000 rpm. Supernatants were gathered for ELISA determination. To prevent protein denaturation throughout preparation, all pulp samples were kept on ice.
Using a semiautomatic ELISA analyzer (STAT FAX 303-PLUS from Awareness Technologies, Palm City, FL, USA) and commercial systems of ELISA kits (Elabscience, Houston, TX, USA), our research group determined TNF-α, SOD-3, osteocalcin, and TGF-β1 levels in all the collected samples. The analysis was performed in duplicate, employing the sandwich ELISA technique, as recommended by the manufacturer of the kit, following the protocol of Subaric et al. [2].
2.5. Data Analysis
All of the data from the study were analyzed using IBM SPSS Statistics 25. Quantitative variables were tested for normal distribution using the Shapiro–Wilk test and were written as averages with standard deviations or medians with interquartile ranges. Quantitative independent variables were tested using Kruskal–Wallis H tests/Welch ANOVA tests, according to their distributions and their inequality of variances. Post-hoc analyses were made using Dunn–Bonferroni tests or Games–Howell tests. Statistically significant (SS) differences were established at p values less than 0.05 (p ≤ 0.05).
3. Results
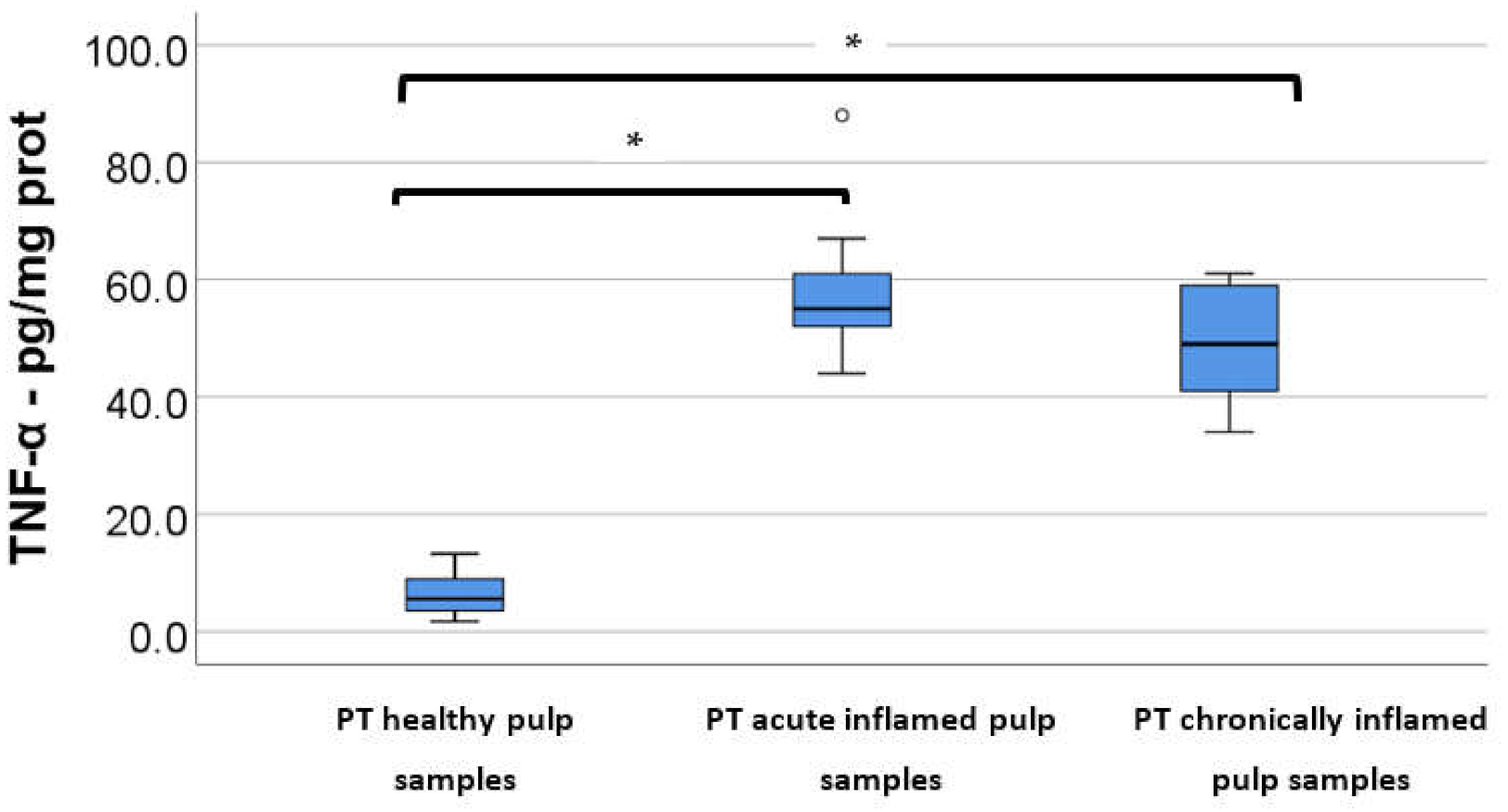
The mean age of the participants in the study was 8.58 ± 1.39 years old. The control group had a mean age ± SD of 8.35 ± 1.46 years old; for the acute pulpitis group, it was 8.8 ± 1.06 years old; for the chronic pulpitis group, it was 8.52 ± 1.68 years old. ELISA analysis was performed to establish the presence of the following biomarkers: TNF-α, SOD-3, osteocalcin, and TGF-β1. Table 1 and Figure 1, Figure 2, Figure 3 and Figure 4 show the protein expressions of biomarkers in the control and experimental groups. Comparisons between groups were made according to the results of the Shapiro–Wilk tests, showing a non-parametric distribution for TNF-α and a normal distribution for the rest of the variables (in which case, Levene’s test showed an inequality of variances between groups). Differences for all biomarkers were statistically significant between groups (p < 0.05). Post-hoc tests showed that all biomarkers were significantly lower in the control group in comparison to the acute/chronic pulpitis groups, while differences between the acute and chronic pulpitis groups were not significant (p > 0.05), except for the protein levels of osteocalcin, which were significantly higher in chronic pulpitis compared to acute pulpitis (p = 0.002) (Table 2).

Table 1.
Protein expression of biomarkers in the control and experimental groups.
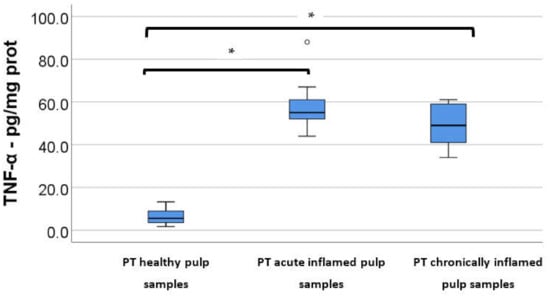
Figure 1.
TNF-α protein levels (pg/mg) in the control group versus acute/chronic pulpitis. (* Indicates statistically significant differences). (The circle in the graphic is an indication that an outlier is present.)
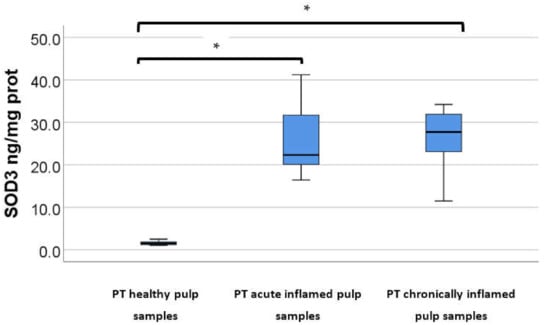
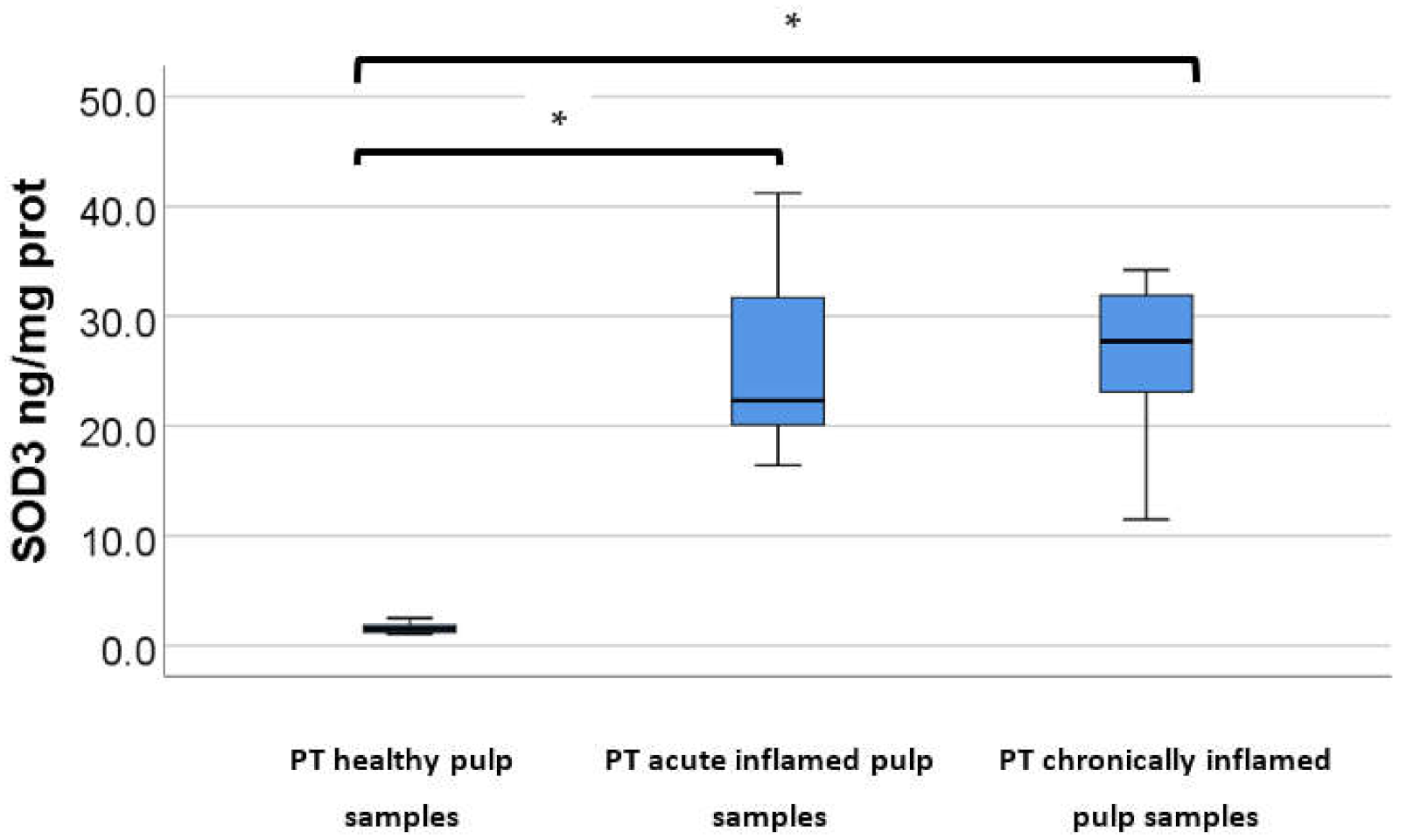
Figure 2.
SOD-3 protein levels (ng/mg) in the control group versus acute/chronic pulpitis. (* Indicates statistically significant differences).
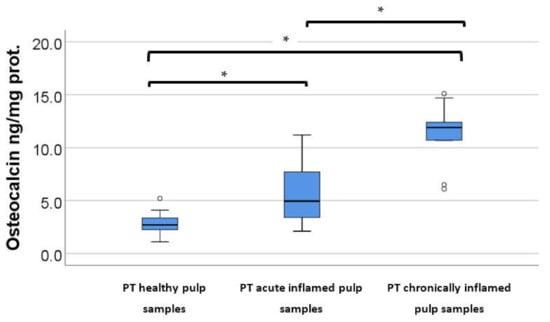
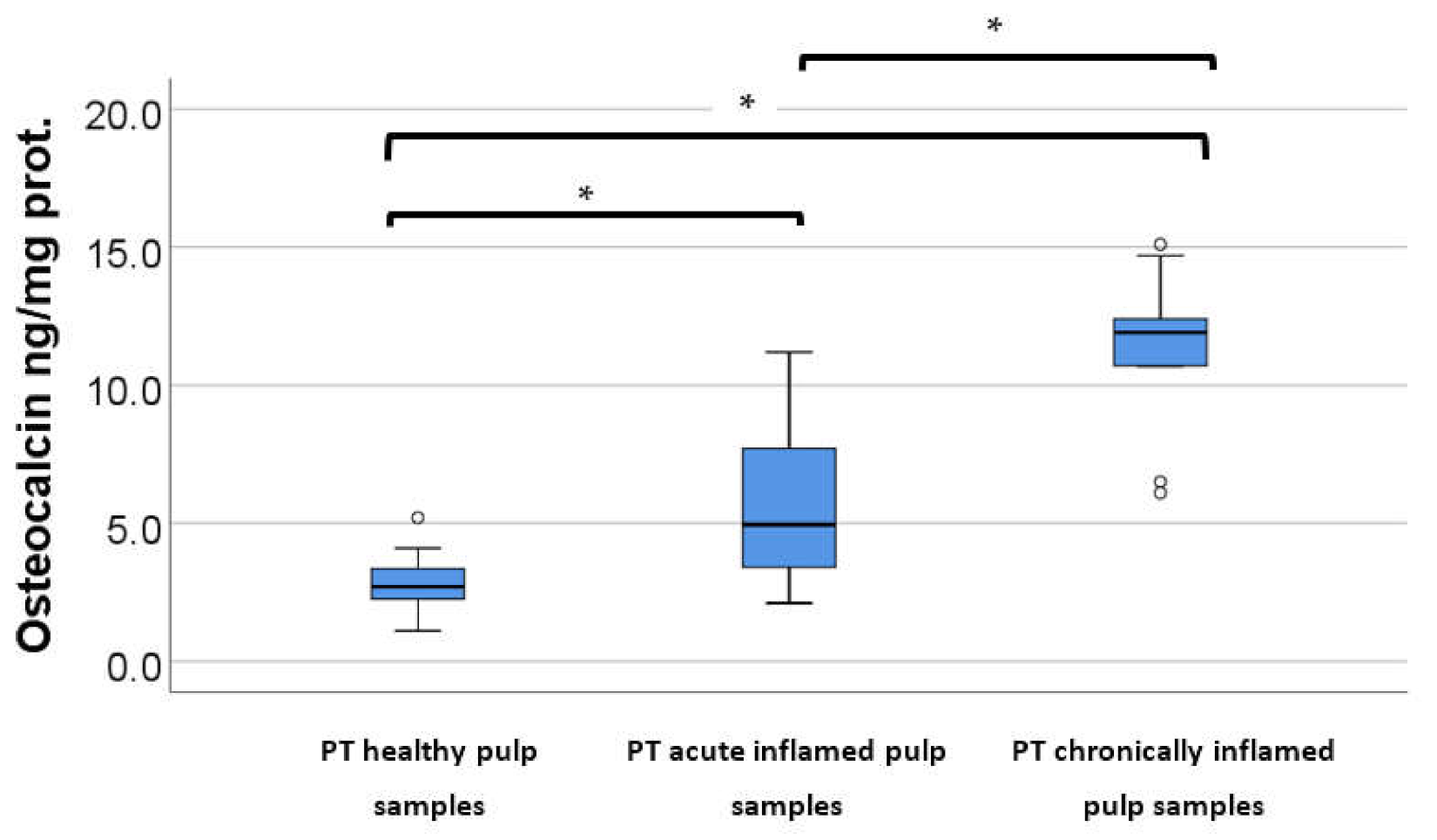
Figure 3.
Osteocalcin protein levels (ng/mg) in the control group versus acute/chronic pulpitis. (* Indicates statistically significant differences). The circles in the graphic are an indication that an outlier is present.)
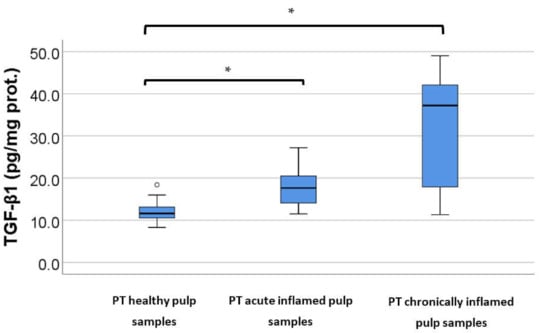
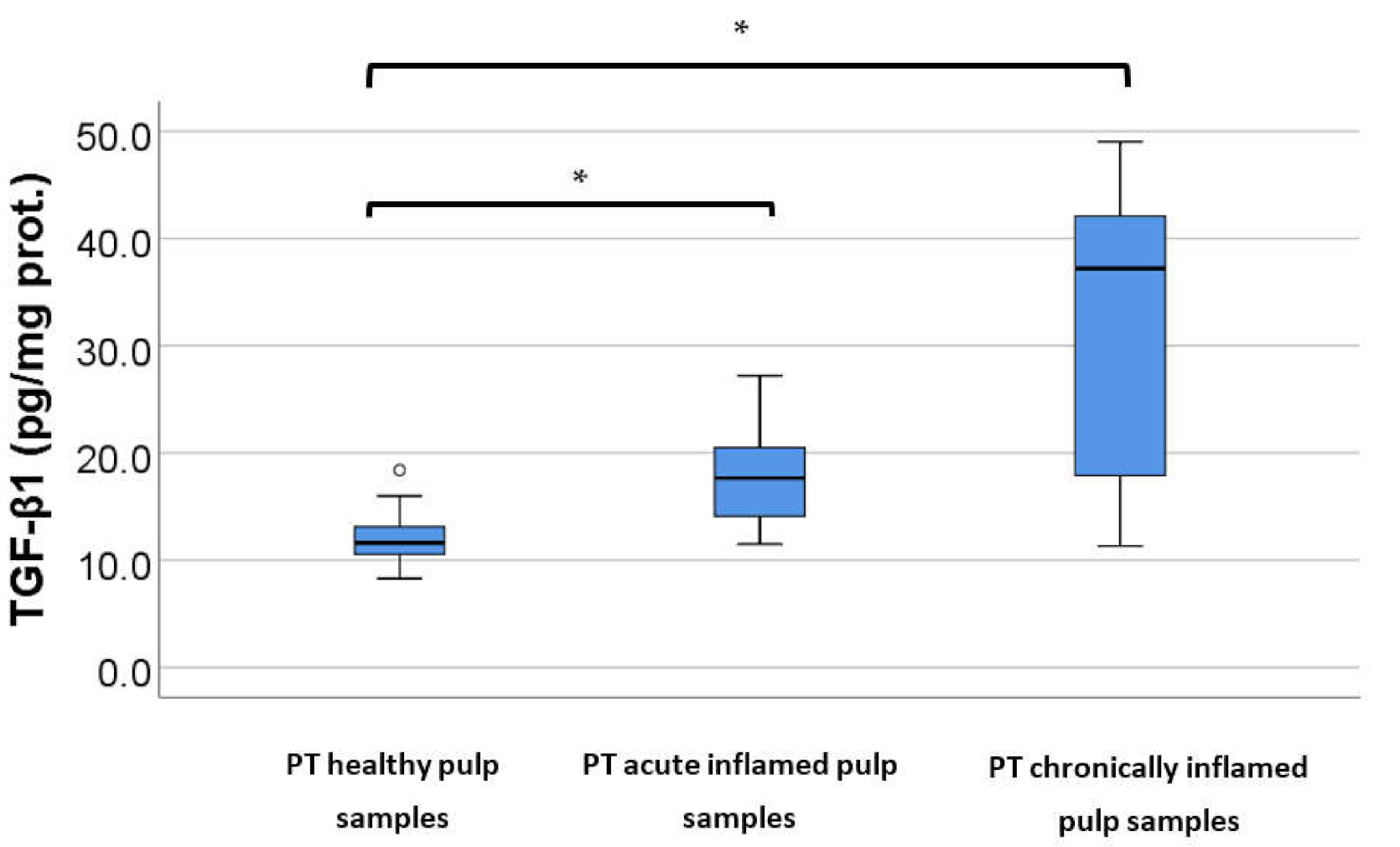
Figure 4.
TGF-β1 protein levels (ng/mg) in the control group versus acute/chronic pulpitis. (* Indicates statistically significant differences). (The circle in the graphic is an indication that an outlier is present.)
Table 2.
Post-hoc analysis of protein expression of biomarkers in the control and experimental groups.
4. Discussion
The present study showed that biochemical markers, such as TNF-α, SOD-3, osteocalcin, and TGF-β1, have statistically significant higher levels in acute and chronically inflamed versus healthy pulp samples obtained from primary teeth. Moreover, osteocalcin presented statistically significant elevated levels in the chronically inflamed pulp versus acute inflamed pulp tissues (Table 1 and Table 2, Figure 1, Figure 2, Figure 3 and Figure 4). All biomarkers were detected in the three groups of vital dental pulp specimens. The study hypothesis was confirmed as the levels of the biomarkers differed in all three groups of pulp samples. The studied biomarkers have strong interconnections in the inflammation processes of the dental pulp characterized by molecular and cellular mechanisms.
The results of the present research are analogous to the ones of our previous study, in which we evaluated the levels of TNF-α, SOD-3, osteocalcin, and TGF-β1 in symptomatic irreversibly inflamed pulp samples obtained from the permanent teeth of children and adolescents. In both studies, symptomatic irreversibly (acute) inflamed pulp tissues revealed significant elevated levels of the studied biomarkers compared to the control group. These results may indicate the existence of similar mechanisms of inflammation, oxidative stress, and mineralization in the primary and permanent teeth of children and adolescents, although, from a clinical and histological perspective, particularities exist (see introduction).
Regarding the levels of the studied biomarkers—in chronically inflamed versus healthy pulp samples obtained from primary teeth, all of them expressed statistically significant higher levels in the experimental compared to the control group. Statistically significant elevated levels of other biological markers, e.g., IL-4 and IgE, were also found in chronically inflamed pulp samples, such as in the study by Sattari et al. [19], in which the experimental group precisely consisted of chronic hyperplastic pulpitis from the permanent teeth of young patients. Subaric et al. [2] determined the protein expression of IL-1β in chronic open pulpitis, chronic closed pulpitis, and healthy pulp samples, using ELISA, without data about the provenience of the pulp tissues. IL-1β levels were found to be statistically significantly higher in the group with chronic closed pulpitis compared to the chronic open pulpitis (p < 0.01), as well as in the group with chronic closed pulpitis versus the controls (p < 0.01). They did not report any statistically significant differences between chronic open pulpitis and the control group (p = 0.081). The differences in the overall concentration of IL-1β in chronically inflamed versus healthy pulp tissues was not statistically significant (p = 0.590). The results of a study conducted by Evrosimovska et al. [20], using the ELISA method, revealed that MMP-1, MMP-8, and MMP-13 had statistically significant (p < 0.01) increased levels in dental pulp with chronic inflammation versus the control group.
Osteocalcin presented statistically significant augmented concentrations in the chronically inflamed pulp sample group compared to acute inflamed pulp tissues (p = 0.002). In chronic inflammation, granulation tissue replaces the normal architecture of the dental pulp and proliferation of small vessels may take place [21]. Histologically, chronically inflamed dental pulp is characterized by a chronic inflammatory infiltrate consisting of lymphocytes, histiocytes, and plasmocytes, newly formed vessels (through angiogenesis), fibroblasts proliferation, and collagen, which results in a fibrous tissue. Osteocalcin was associated with the presence of markers of angiogenesis, and it was also localized in areas of fibrosis [8], which may explain the elevated levels in chronically inflamed pulp samples in our study. On the other hand, Abd-Elmeguid et al. [8] reported that osteocalcin may have an important role in chronic pulpitis without irreversible changes. More studies are needed to elucidate the actual mechanisms of osteocalcin and other biomarkers in chronic pulpal inflammation.
TNF-α is produced by macrophages, as a response to dental infections, and may stimulate neutrophils to form high concentrations of ROI [6]. The present results are partially in agreement with the results by Pezelj-Ribaric et al. [22], who, by using the same method of testing, found statistically significant elevated levels of TNF-α in irreversible asymptomatic and symptomatic pulpitis samples (p = 0.000), but they also reported SS differences between the samples of irreversible symptomatic and asymptomatic pulp samples (p = 0.000), without mentioning the origin of pulp tissue (primary/permanent teeth). Other studies with similar results, but realized on pulp samples from permanent teeth, include those by Abd-Elmeguid et al. [8], with statistically significant higher levels (p < 0.01) in irreversibly inflamed pulp tissues, which were clinically sensitive to hot stimuli with spontaneous lingering pain; ElSalhy et al. [23], with higher concentrations in irreversibly inflamed symptomatic pulpitis samples compared to the control group (p < 0.05); Kokkas et al. [24], with statistically significant elevated levels (p = 0.015) in irreversible pulpitis samples extracted from teeth with prolonged or spontaneous pain versus the control group; and Keller et al. [25], with statistically significant elevated levels in pulp samples obtained from teeth with acute pulp inflammation (p = 0.05). Even though ElSalhy et al. [23] utilized pulpal blood for protein determination, Keller et al. [25] and Kokkas et al. [24] investigated TNF-α gene expression using RT-PCR; the inflamed pulp samples expressed increased levels of TNF-α versus normal pulp tissues. We found a single paper [26], without mentioning if samples were collected from primary/permanent teeth, where the authors reported the study groups as “normal pulp tissue”, “acute pulpitis”, and “chronic pulpitis”, with SS differences between normal and acute and chronic pulpitis specimens (p < 0.01). The results were comparable to the ones in our research; however, statistically significant differences between the acute and chronic pulpitis group (p < 0.05) were also reported, in contrast with our results.
In our study, statistically significant elevated levels of SOD-3 (p < 0.001) were observed in both acute and chronically inflamed pulp samples, compared to healthy pulp specimens. ROIs are produced in physiological and pathological conditions, but their concentrations differ in each situation. In healthy tissues, ROIs are produced in small quantities, but elevated levels of ROI, produced by macrophages, may cause excessive tissue damage and lipid peroxidation, protein oxidation, and nucleic acid damage [27]. Gene expression determination of Cu, Zn-SOD, and Mn-SOD isoenzymes in irreversibly symptomatic and inflamed pulp samples from permanent teeth revealed statistically significant elevated levels in the cases of irreversible pulpitis [28]. Although Davis et al. [29] do not mention the type of inflammation of the permanent dental pulp samples used in their study, our results are similar to the data they presented, regarding statistically significant elevated levels (p = 0.0001) of Cu, Zn-SOD observed in inflamed pulp specimens compared to the controls. The data obtained in our research are also in accordance with the results of a study by Ge et al. [30], who highlighted statistically significant elevated levels of SOD in permanent teeth with irreversible inflammation versus healthy pulp tissues. Tulunoglu et al. [31] focused on the total activity of SOD in irreversibly inflamed (no mention if symptomatic or asymptomatic) and healthy pulp samples obtained from the permanent teeth of adolescents, the differences between the two groups not being statistically significant. A study by Varvara’s et al. [32] presented results that contradicted with the data obtained by our research team, as their results displayed statistically significant elevated levels (p < 0.00) of Cu, Zn-SOD activity, using spectrophotometric methods, in the control group versus clinically healthy and symptomatic human dental pulp samples from permanent teeth. As we mentioned in our previous study, the advanced pulp pathology and progression of inflammation, which may cause destruction of the enzyme, and the different methods used to test the presence of the biomarker, may have contributed to these different results.
Our results are also in accordance with the results of Piattelli et al. [33], who observed statistically significant augmented levels of TGF-β1 in permanent teeth with irreversible pulp inflammation, with spontaneous and prolonged episodes of pain versus healthy dental pulp samples. TGF-β1 is a multifunctional cytokine and angiogenic growth factor, and its effects are dependent upon the types of target cells and local concentrations [34]. It is also a potent immunosuppressant, and it may have a crucial role in the dentine–pulp complex reparative process as it can trigger matrix secretion and formation of type I collagen [35]. It is supposed that TGF-β1 is sequestered in the dentine matrix and released during carious processes and reparation mechanisms, such as reparative dentinogenesis [33,36]. Various studies showed that TGF-β1 can regulate matrix turnover and may stimulate growth and differentiation of pulp cells when used as pulp capping material [36,37].
A multiplex assay was used by Abd-Elmeguid et al. [8] to analyze osteocalcin levels in pulp samples with irreversible inflammation versus healthy pulp specimens from permanent teeth, revealing statistically significant elevated levels in the inflamed pulp group (p < 0.05), the results being parallel to ours. Mature osteoblasts secrete osteocalcin in their latest differentiation stage [38,39]. Osteocalcin, a non-collagenous protein, is expressed in mature odontoblasts that form the new matrix of reactionary dentine, as demonstrated by Hirata et al. [40]. Osteocalcin levels are increased after bone fractures and may remain elevated during tissue healing, with an important role in bone reparation [41,42]. Macrophages are the dominant inflammatory cells in pulp inflammation and express osteocalcin in their terminal differentiations to osteoblasts [8].
One of the limitations of our study is represented by the small number of samples. Unfortunately, the COVID-19 pandemic also attributed to a negative impact in the research field; thus, our access to patients was limited as the academic activity was limited to online courses for a long period of time and all dental treatments were postponed. The evaluation of more biochemical markers was also intended, but the delivery of some reagents and kits for analysis was delayed, also because of the pandemic and the restrictions. Despite that, further studies should be conducted to clarify the role of the studied biomarkers in acute and chronically inflamed pulp tissues, as results among different studies vary.
Evaluations into other various biomarkers are also needed in order to help establish dental pulp condition. Precisely, a potential marker could be the anti-cyclic citrullinated peptide antibodies (anti-CPP), which was evaluated by Ballini et al. [43] in patients with periodontal disease, another major oral condition, and in patients with periodontal disease and rheumatoid arthritis. The results of their study did not show a correlation with the clinical signs of pathology, but citrullination of proteins by the P. gingivalis (present in endodontic infections) PAD enzyme could lead to local inflammation in the infected endodontic space [44]. More studies in the field are needed, and an evaluation of anti-CPP antibodies in dental pulp should be considered as a probable diagnostic marker in the assessment of the inflammatory condition of the pulp.
A rapid, more intense case of pulp inflammation or long-term pulpitis can lead to localized odontoblast death. TGF-β released from the dentine matrix after demineralization is capable of signaling what may lead to the differentiation of stem cells in odontoblast-like cells [45]. Stem cells have different origins and crucial roles in reparative and regenerative procedures [46,47]. They can be undifferentiated mesenchymal cells from the pulp core, which are differentiated under the inductive signal of various markers (e.g., TGF-β), and due to their plasticity can be divided in specific cell lineages [46,48]. They are also capable of limitless self-renewal and may have an important role in treating hard dental tissue defects after an injury, by differentiating in odontoblast-like cells and secreting reparative dentine, which will lead to pulpal healing and reparation [46]. Induced pluripotent stem cells (iPSCs) are also promising, as they can participate in the regeneration of mineralized tissues [47]. Exogenous stem cells can be placed in the pulp if severe lesions occur and irreversible damage takes place, aiming for regeneration of pulp tissue and mineralized matrix formation [47,49].
During the inflammatory process of the dental pulp, molecular modifications precede macroscopic and microscopic inflammatory alterations; thus, early diagnoses may be established if biomarker determination could be put into practice. One attempt could be done by obtaining pulpal tissue through minimal invasive treatments, such as vital pulpotomy or even partial pulpotomy, if possible, and testing for the presence of biomarkers, the result being corroborated with the patient’s clinical findings. We should also consider non-invasive methods for the assessment of pulpal conditions, such as dentinal fluid collections, which contain serum proteins and immunoglobulins [6,50]. Seeking dental treatment at an early stage of inflammation and recognizing the pulp condition is compulsory to apply non-invasive/minimal invasive methods.
Molecular evaluation of biomarkers associated with short-term pain caused by thermal stimulation, which can be precisely localized, can lead to reversible pulp inflammation diagnosis, which is usually treated by partial or total pulpotomy, aiming for pulpal healing. A spontaneous, lingering pain to thermal stimuli related to biomarker assessment is indicative of an acute irreversible inflammation, which is usually followed by complete pulpectomy. On the other hand, a dull pain with hypoexcitability on cold stimulation and marker evaluation may establish the diagnosis of chronic inflamed dental pulp, followed by pulpectomy and root canal treatment. As all dental pulp inflammation types, either reversible or irreversible (acute or chronic), are associated with higher concentrations of biomarkers compared to healthy pulp samples, more studies and tools are needed in order to establish the range of these concentrations for each type of inflammation pathology so that the findings of the present and future studies can be put in practice. There is also a need for clinical, feasible methods to assess the protein expressions of these biomolecules in daily practices, and ELISA may be the most appropriate, accurate, and promising tool [6].
From the perspective of a clinician who works with children and adolescents, an early diagnosis of pulp pathology in primary teeth (such as reversible inflammation) is essential and will lead to a suitable and more conservative treatment, which will promote tissue healing through dentine deposition by reparative dentinogenesis, and conservation of pulp vitality. Eliminating the inflamed pulp lesion, while the rest of the pulp is still healthy, and placing a biocompatible material (e.g., MTA), will facilitate healing and reparation through reparative dentine bridge formation [49]. Subsequently, root resorption will continue in a physiological way, maintaining the deciduous teeth on the dental arch until natural exfoliation and replacement with permanent teeth occurs. If a late diagnosis is made, irreversible inflammation usually occurs, and it is followed by pulpectomy and root canal treatment. In that case, teeth may become more susceptible to re-infection, fractures, or pathological resorption [49], and they may be followed by early extraction, which is frequently associated with malocclusion, such as crowding, delay, or earlier eruption of permanent teeth, chewing, and esthetic problems, and the need for more complex treatments.
5. Conclusions
In primary teeth, acute and chronic inflamed pulp tissues presented significantly elevated levels of TNF-α, SOD-3, TGF-β1, and osteocalcin compared to healthy pulp samples, while osteocalcin may play a crucial role in the chronic pulp inflammation of primary teeth. This study provides useful information regarding molecular-based methods, such as ELISA, which, if associated with clinical diagnosis of pulp conditions, may offer new perspectives in evaluating the severity of pulpal inflammation, and could help in making the correct dental treatment choice, with a focus on maintaining pulp vitality, avoiding future local and general unpleasant consequences.
Author Contributions
Conceptualization, K.K., A.R.T., A.V. and M.G.; methodology, K.K., M.T., A.V., A.R.T., M.B., M.G.; software, T.-C.S., I.-I.S.-S., D.M.; validation, A.R.T., M.B., M.G.; formal analysis, T.-C.S., D.M., I.-I.S.-S.; investigation, K.K., M.I., T.-C.S., D.M.; resources, K.K., T.-C.S., D.M., I.-I.S.-S.; data curation, K.K., M.I., M.T., M.B.; writing—original draft preparation, K.K., T.-C.S., D.M., I.-I.S.-S.; writing—review and editing, M.I., M.T., A.V.; visualization, K.K., I.-I.S.-S.; supervision, M.I., M.T., A.V., A.R.T., M.B., M.G.; project administration, M.I., M.T., A.V., A.R.T., M.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Carol Davila University of Medicine and Pharmacy (5751/05.03.2021).
Informed Consent Statement
Informed consent was obtained from the caregivers of all minor subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available due to privacy reasons.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Farges, J.C.; Alliot-Licht, B.; Renard, E.; Ducret, M.; Gaudin, A.; Smith, A.J.; Cooper, P.R. Dental Pulp Defence and Repair Mechanisms in Dental Caries. Mediat. Inflamm. 2015, 2015, 230251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Šubarić, L.; Mitić, A.; Matvijenko, V.; Jovanović, R.; Živković, D.; Perić, D.; Vlahović, Z. Interleukin 1-beta analysis in chronically inflamed and healthy human dental pulp. Vojnosanit. Pregl. 2017, 74, 256–260. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Bester, J.; Pretorius, E. The inflammatory effects of TNF-alpha and complement component 3 on coagulation. Sci. Rep. 2018, 8, 1812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.C.; Lin, W.N.; Cho, R.L.; Wang, C.Y.; Hsiao, L.D.; Yang, C.M. TNF-alpha-Induced cPLA2 Expression via NADPH Oxidase/Reactive Oxygen Species-Dependent NF-kappaB Cascade on Human Pulmonary Alveolar Epithelial Cells. Front. Pharmacol. 2016, 7, 447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Branicky, R.; Noe, A.; Hekimi, S. Superoxide dismutases: Dual roles in controlling ROS damage and regulating ROS signaling. J. Cell Biol. 2018, 217, 1915–1928. [Google Scholar] [CrossRef]
- Zanini, M.; Meyer, E.; Simon, S. Pulp Inflammation Diagnosis from Clinical to Inflammatory Mediators: A Systematic Review. J. Endod. 2017, 43, 1033–1051. [Google Scholar] [CrossRef]
- Ji, S.; Song, S.; Lee, J.; Kim, J.; Kim, J. Characterization of Odontoblasts in Supernumerary Tooth-derived Dental Pulp Stem Cells between Passages by Real-Time PCR. J. Korean Acad. Pediatr. Dent. 2021, 48, 291–301. [Google Scholar] [CrossRef]
- Abd-Elmeguid, A.; Abdeldayem, M.; Kline, L.W.; Moqbel, R.; Vliagoftis, H.; Yu, D.C. Osteocalcin expression in pulp inflammation. J. Endod. 2013, 39, 865–872. [Google Scholar] [CrossRef]
- Chisini, L.A.; Conde, M.C.; Alcazar, J.C.; Silva, A.F.; Nor, J.E.; Tarquinio, S.B.; Demarco, F.F. Immunohistochemical Expression of TGF-beta1 and Osteonectin in engineered and Ca(OH)2-repaired human pulp tissues. Braz. Oral Res. 2016, 30, e93. [Google Scholar] [CrossRef] [Green Version]
- Giuroiu, C.L.; Caruntu, I.D.; Lozneanu, L.; Melian, A.; Vataman, M.; Andrian, S. Dental Pulp: Correspondences and Contradictions between Clinical and Histological Diagnosis. BioMed Res. Int. 2015, 2015, 960321. [Google Scholar] [CrossRef]
- Ghaderi, F.; Jowkar, Z.; Tadayon, A. Caries Color, Extent, and Preoperative Pain as Predictors of Pulp Status in Primary Teeth. Clin. Cosmet. Investig. Dent. 2020, 12, 263–269. [Google Scholar] [CrossRef]
- Aishuwariya, T.; Ramesh, S. Evaluation Of Interleukin 6, Interleukin 8, TNF Alpha as Biomarkers For Pulpitis—In Vivo Study. Int. J. Dent. Oral Sci. 2021, 8, 1492–1497. [Google Scholar] [CrossRef]
- Tripodi, D.; Latrofa, M.; D’ercole, S. Microbiological aspects and inflammatory response of pulp tissue in traumatic dental lesions. Eur. J. Inflamm. 2007, 5, 1721–1727. [Google Scholar] [CrossRef] [Green Version]
- American Association of Endodontists. Glossary of Endodontic Terms; American Association of Endodontists: Chicago, IL, USA, 2020. [Google Scholar]
- WHO. Oral Health. Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 10 December 2021).
- Raducanu, A.M. Pedodontie Indrumar Practic, 1st ed.; Bren: Bucharest, Romania, 2018. (In Romanian) [Google Scholar]
- Suwanchai, A.; Theerapiboon, U.; Chattipakorn, N.; Chattipakorn, S.C. NaV 1.8, but not NaV 1.9, is upregulated in the inflamed dental pulp tissue of human primary teeth. Int. Endod. J. 2012, 45, 372–378. [Google Scholar] [CrossRef]
- Gusman, H.; Santana, R.B.; Zehnder, M. Matrix metalloproteinase levels and gelatinolytic activity in clinically healthy and inflamed human dental pulps. Eur. J. Oral. Sci. 2002, 110, 353–357. [Google Scholar] [CrossRef]
- Sattari, M.; Haghighi, A.K.; Tamijani, H.D. The relationship of pulp polyp with the presence and concentration of immunoglobulin E, histamine, interleukin-4 and interleukin-12. Aust. Endod. J. 2009, 35, 164–168. [Google Scholar] [CrossRef]
- Evrosimovska, B.; Dimova, C.; Kovacevska, I.; Panov, S. Concentration of collagenases (MMP-1, -8, -13) in patients with chronically inflamed dental pulp tissue. Prilozi 2012, 33, 191–204. [Google Scholar]
- Serra, M.B.; Barroso, W.A.; da Silva, N.N.; Silva, S.D.N.; Borges, A.C.R.; Abreu, I.C.; Borges, M. From Inflammation to Current and Alternative Therapies Involved in Wound Healing. Int. J. Inflam. 2017, 2017, 3406215. [Google Scholar] [CrossRef] [Green Version]
- Pezelj-Ribaric, S.; Anic, I.; Brekalo, I.; Miletic, I.; Hasan, M.; Simunovic-Soskic, M. Detection of tumor necrosis factor alpha in normal and inflamed human dental pulps. Arch. Med. Res. 2002, 33, 482–484. [Google Scholar] [CrossRef]
- Elsalhy, M.; Azizieh, F.; Raghupathy, R. Cytokines as diagnostic markers of pulpal inflammation. Int. Endod. J. 2013, 46, 573–580. [Google Scholar] [CrossRef]
- Kokkas, A.B.; Goulas, A.; Varsamidis, K.; Mirtsou, V.; Tziafas, D. Irreversible but not reversible pulpitis is associated with up-regulation of tumour necrosis factor-alpha gene expression in human pulp. Int. Endod. J. 2007, 40, 198–203. [Google Scholar] [CrossRef]
- Keller, J.F.; Carrouel, F.; Staquet, M.J.; Kufer, T.A.; Baudouin, C.; Msika, P.; Bleicher, F.; Farges, J.C. Expression of NOD2 is increased in inflamed human dental pulps and lipoteichoic acid-stimulated odontoblast-like cells. Innate Immun. 2011, 17, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Ding, W.-S.; Zhao, J.; Liu, Z.-H.; Wang, J.-H. Detection of TNF-α in dental pulps of normal, acute and chronic pulpitis. J. Shandong Univ. (Health Sci.) 2005, 1, 25. [Google Scholar]
- Baumgardner, K.R.; Sulfaro, M.A. The anti-inflammatory effects of human recombinant copper-zinc superoxide dismutase on pulp inflammation. J. Endod. 2001, 27, 190–195. [Google Scholar] [CrossRef]
- Bodor, C.; Matolcsy, A.; Bernath, M. Elevated expression of Cu, Zn-SOD and Mn-SOD mRNA in inflamed dental pulp tissue. Int. Endod. J. 2007, 40, 128–132. [Google Scholar] [CrossRef]
- Davis, W.L.; Jacoby, B.H.; Craig, K.R.; Wagner, G.; Harrison, J.W. Copper-zinc superoxide dismutase activity in normal and inflamed human dental pulp tissue. J. Endod. 1991, 17, 316–318. [Google Scholar] [CrossRef]
- Ge, J.; Ji, J.; Wang, T. Superoxide dismutase and malonyl dialdehyde in human pulp tissue. Zhonghua Kou Qiang Yi Xue Za Zhi 1996, 31, 201–203. [Google Scholar]
- Tulunoglu, O.; Alacam, A.; Bastug, M.; Yavuzer, S. Superoxide dismutase activity in healthy and inflamed pulp tissues of permanent teeth in children. J. Clin. Pediatr. Dent. 1998, 22, 341–345. [Google Scholar]
- Varvara, G.; Traini, T.; Esposito, P.; Caputi, S.; Perinetti, G. Copper-zinc superoxide dismutase activity in healthy and inflamed human dental pulp. Int. Endod. J. 2005, 38, 195–199. [Google Scholar] [CrossRef]
- Piattelli, A.; Rubini, C.; Fioroni, M.; Tripodi, D.; Strocchi, R. Transforming growth factor-beta 1 (TGF-beta 1) expression in normal healthy pulps and in those with irreversible pulpitis. Int. Endod. J. 2004, 37, 114–119. [Google Scholar] [CrossRef]
- Jarad, M.; Kuczynski, E.A.; Morrison, J.; Viloria-Petit, A.M.; Coomber, B.L. Release of endothelial cell associated VEGFR2 during TGF-beta modulated angiogenesis in vitro. BMC Cell Biol. 2017, 18, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niwa, T.; Yamakoshi, Y.; Yamazaki, H.; Karakida, T.; Chiba, R.; Hu, J.C.; Nagano, T.; Yamamoto, R.; Simmer, J.P.; Margolis, H.C.; et al. The dynamics of TGF-beta in dental pulp, odontoblasts and dentin. Sci. Rep. 2018, 8, 4450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurent, P.; Camps, J.; About, I. Biodentine(TM) induces TGF-beta1 release from human pulp cells and early dental pulp mineralization. Int. Endod. J. 2012, 45, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Chang, H.H.; Lin, P.S.; Huang, Y.A.; Chan, C.P.; Tsai, Y.L.; Lee, S.Y.; Jeng, P.Y.; Kuo, H.Y.; Yeung, S.Y.; et al. Effects of TGF-beta1 on plasminogen activation in human dental pulp cells: Role of ALK5/Smad2, TAK1 and MEK/ERK signalling. J. Tissue Eng. Regen. Med. 2018, 12, 854–863. [Google Scholar] [CrossRef]
- Manolagas, S.C. Osteocalcin promotes bone mineralization but is not a hormone. PLoS Genet. 2020, 16, e1008714. [Google Scholar] [CrossRef]
- Moser, S.C.; van der Eerden, B.C.J. Osteocalcin-A Versatile Bone-Derived Hormone. Front. Endocrinol. 2018, 9, 794. [Google Scholar] [CrossRef] [Green Version]
- Hirata, M.; Yamaza, T.; Mei, Y.F.; Akamine, A. Expression of osteocalcin and Jun D in the early period during reactionary dentin formation after tooth preparation in rat molars. Cell Tissue Res. 2005, 319, 455–465. [Google Scholar] [CrossRef]
- Ho, M.H.; Yao, C.J.; Liao, M.H.; Lin, P.I.; Liu, S.H.; Chen, R.M. Chitosan nanofiber scaffold improves bone healing via stimulating trabecular bone production due to upregulation of the Runx2/osteocalcin/alkaline phosphatase signaling pathway. Int. J. Nanomed. 2015, 10, 5941–5954. [Google Scholar] [CrossRef] [Green Version]
- Vetra, A.; Smane, L.; Pilmane, M.; Vilka, L. Osteopontin, osteocalcin, and osteoprotegerin expression in human tissue affected by cleft lip and palate. SHS Web Conf. 2016, 30, 00008. [Google Scholar] [CrossRef] [Green Version]
- Ballini, A.; Tete, S.; Scattarella, A.; Cantore, S.; Mastrangelo, F.; Papa, F.; Nardi, G.M.; Perillo, L.; Crincoli, V.; Gherlone, E.; et al. The role of anti-cyclic citrullinated peptide antibody in periodontal disease. Int. J. Immunopathol. Pharmacol. 2010, 23, 677–681. [Google Scholar] [CrossRef]
- Cooper, P.R.; Chicca, I.J.; Holder, M.J.; Milward, M.R. Inflammation and Regeneration in the Dentin-pulp Complex: Net Gain or Net Loss? J. Endod. 2017, 43, S87–S94. [Google Scholar] [CrossRef]
- Mullen, A.C.; Wrana, J.L. TGF-beta Family Signaling in Embryonic and Somatic Stem-Cell Renewal and Differentiation. Cold Spring Harb. Perspect. Biol. 2017, 9, a022186. [Google Scholar] [CrossRef]
- Cappare, P.; Tete, G.; Sberna, M.T.; Panina-Bordignon, P. The Emerging Role of Stem Cells in Regenerative Dentistry. Curr. Gene Ther. 2020, 20, 259–268. [Google Scholar] [CrossRef]
- Tete, G.; D’Orto, B.; Nagni, M.; Agostinacchio, M.; Polizzi, E.; Agliardi, E. Role of induced pluripotent stem cells (IPSCS) in bone tissue regeneration in dentistry: A narrative review. J. Biol. Regul. Homeost. Agents 2020, 34, 1–10. [Google Scholar]
- Ledesma-Martinez, E.; Mendoza-Nunez, V.M.; Santiago-Osorio, E. Mesenchymal Stem Cells Derived from Dental Pulp: A Review. Stem. Cells Int. 2016, 2016, 4709572. [Google Scholar] [CrossRef] [Green Version]
- Harichane, Y.; Hirata, A.; Dimitrova-Nakov, S.; Granja, I.; Goldberg, A.; Kellermann, O.; Poliard, A. Pulpal progenitors and dentin repair. Adv. Dent. Res. 2011, 23, 307–312. [Google Scholar] [CrossRef]
- Brizuela, C.; Meza, G.; Mercade, M.; Inostroza, C.; Chaparro, A.; Bravo, I.; Briceno, C.; Hernandez, M.; Giner, L.; Ramirez, V. Inflammatory biomarkers in dentinal fluid as an approach to molecular diagnostics in pulpitis. Int. Endod. J. 2020, 53, 1181–1191. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).