
Synergistic Effects of Natural Products and Mesenchymal Stem Cells in Osteoarthritis Treatment: A Narrative Review

Abstract
1. Introduction
Literature Search Methodology
2. Osteoarthritis and MSC Therapies
2.1. Overview of Osteoarthritis (OA)
2.2. Pathophysiology of Osteoarthritis
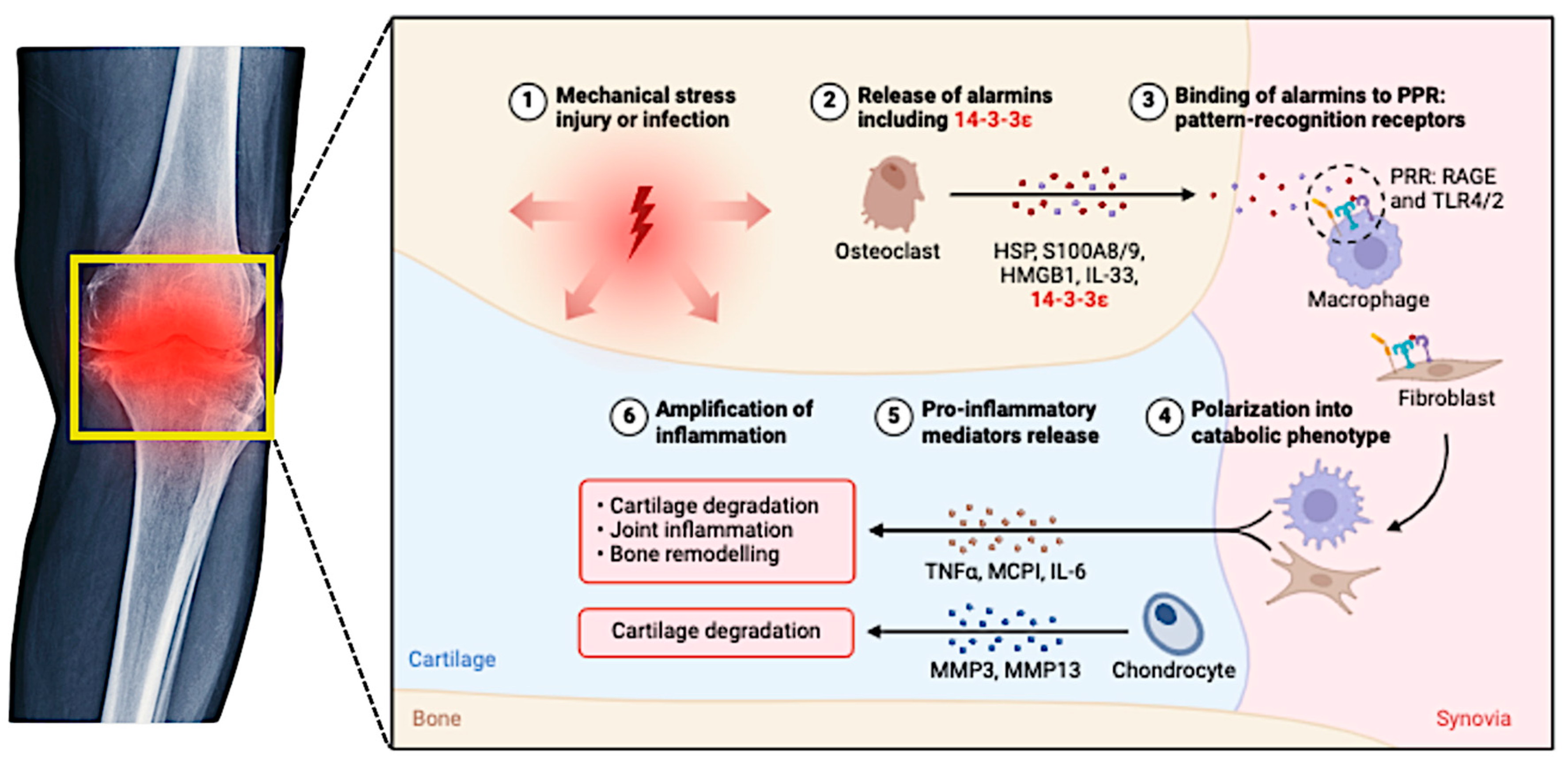
2.3. Inflammatory Pathways in Osteoarthritis
2.4. Mesenchymal Stem Cells (MSCs)
3. Natural Products
3.1. Natural Products in Enhancing MSC Therapies
3.2. Specific Natural Products and Their Effects on MSCs
3.2.1. Curcumin
3.2.2. Resveratrol
3.2.3. Quercetin
3.2.4. Epigallocatechin Gallate (EGCG)
4. Combination Therapies: MSCs and Natural Products
4.1. Synergistic Effects of MSCs and Natural Products

{kind=link}
{kind=link}
| Category | Natural Product | Model Used | Outcomes | Author |
|---|---|---|---|---|
| Enhancement of MSC Survival and Differentiation | Curcumin Dosage regimens: General wellness: 500–1000 mg daily. Arthritis and joint pain: 1000–1500 mg daily, often divided into smaller doses. Heart health: 500–700 mg daily. Cognitive health: 500–1000 mg daily. Maximum safe limit: up to 8000 mg per day for short durations. | in vitro/ clinical studies | Decreased oxidative stress and inflammation improve MSC viability and differentiation potential. | [79,81,90] |
| Resveratrol Dosage regimens: Anti-aging: 150–500 mg per day; up to 1000 mg daily for more pronounced effects. Heart health: 100–250 mg daily; higher doses of 250–500 mg per day for existing cardiovascular conditions. Anti-inflammatory: up to 1500 mg daily for up to 3 months; higher doses of 2000–3000 mg daily for 2–6 months. | in vitro | Promotes bone growth, reduces inflammation, and enhances regeneration. | [69,78,108] | |
| Quercetin Dosage regimens: General wellness: 500 mg per day, often combined with vitamin C or bromelain to enhance absorption. Allergies or inflammation: 500–1000 mg per day, divided into multiple doses. | in vitro | Supports bone formation and decreases inflammation, especially in age-related bone loss. | [69,92,93] | |
| Modulation of Inflammatory Microenvironment | Curcumin and resveratrol combination (no information) | in vitro/in vivo | Inhibits TNF-α-induced inflammation, suppresses NF-κB signaling, reduces vascular inflammation, and enhances MSC function in inflammatory conditions. | [95,96,109,110] |
| Quercetin Dosage regimens: General wellness: 500 mg per day, often combined with vitamin C or bromelain to enhance absorption. Allergies or inflammation: 500–1000 mg per day, divided into multiple doses. | in vitro/in vivo | Enhances MSCs’ immunomodulatory capacity and modulates inflammatory signaling pathways. | [97,98] | |
| Improvement of Bioavailability and Efficacy | Curcumin Dosage regimens: General wellness: 500–1000 mg daily. Arthritis and joint pain: 1000–1500 mg daily, often divided into smaller doses. Heart health: 500–700 mg daily. Cognitive health: 500–1000 mg daily. Maximum safe limit: up to 8000 mg per day for short durations | in vitro/in vivo | Improved efficacy through structural modifications or nano-delivery systems enhances solubility and absorption, maximizing the therapeutic potential of MSCs. | [99,100,101,102] |
| Resveratrol and curcumin (no information) | in vitro/in vivo | Low concentrations of compounds work synergistically, improving the therapeutic outcomes of MSC-based therapies more effectively than when used individually. | [103,104,105,106] | |
| Case Studies and Applications | Crocin (no information) | in vivo | Significant improvements in cell survival and reductions in oxidative stress highlight the potential of natural products to enhance MSC efficacy in lung injury models. | [1,107] |
| Resveratrol Dosage regimens: Anti-aging: 150–500 mg per day; up to 1000 mg daily for more pronounced effects. Heart health: 100–250 mg daily; higher doses of 250–500 mg per day for existing cardiovascular conditions. Anti-inflammatory: up to 1500 mg daily for up to 3 months; higher doses of 2000–3000 mg daily for 2–6 months | in vivo | Ameliorates inflammation, promotes osteogenic differentiation in periodontal tissues, and demonstrates potential in dental applications of MSC therapy. | [108] |
4.2. Evidence from Preclinical Studies
4.3. Insights from Clinical Trials
4.4. Mechanisms Underlying Synergistic Effects
4.5. Challenges, Considerations and Future Direction
5. Mechanisms of Action
5.1. Modulation of Inflammatory Pathways
5.2. Reduction of Oxidative Stress
5.3. Promotion of Chondrogenic Differentiation
5.4. Enhanced Delivery via Biomaterials
5.5. Immune Modulation
5.6. Future Perspectives
5.7. Perspectives on Clinical Practice and Translation
6. Challenges and Considerations
6.1. Standardization and Quality Control
6.2. Bioavailability and Delivery
6.3. Safety and Potential Side Effects
6.4. Regulatory Hurdles
7. Challenges, Limitations, and Conflicting Evidence
7.1. Bioavailability and Stability Challenges
7.2. Variability in MSC Sources and Treatment Efficacy
7.3. Conflicting Clinical Data on MSC + Natural Product Therapies
7.4. Lack of Regulatory Guidelines and Standardized Protocols
7.5. Future Research Priorities
8. Conclusions and Future Directions
8.1. Research Priorities for Advancing MSC + Natural Product Therapies
8.2. Clinical Translation: Roadmap for the Next 5–10 Years
- Preclinical refinement (0–2 years): This phase focuses on optimizing bioavailability solutions, comparing MSC sources, and conducting high-throughput screening to identify the most effective MSC–natural product combinations.
- Small-scale clinical trials (2–5 years): During this period, phase I/II clinical trials will assess safety, dosing, and preliminary efficacy. Simultaneously, standardized MSC culture and expansion protocols will be developed, and collaboration with regulatory agencies will define safety standards for combined therapies.
- Large-scale clinical adoption (5–10 years): The final phase involves conducting multi-center phase III trials, establishing personalized treatment strategies based on patient biomarkers, and achieving regulatory approval and commercialization of MSC–natural product combination therapy for OA.
8.3. The Future of MSC + Natural Product Therapy for OA
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| NSAIDs | Nonsteroidal Anti-Inflammatory Drugs |
| MSCs | Mesenchymal Stem Cells |
| OA | Osteoarthritis |
| PRP | Platelet-Rich Plasma |
| EGCG | Epigallocatechin Gallate |
| COMP | Cartilage Oligomeric Matrix Protein |
| C2C | Collagen Type II Cleavage Products |
| IL-1β | Interleukin-1β |
| IL-6 | Interleukin-6 |
| IL-17 | Interleukin-17 |
| TNF-α | Tumor Necrosis Factor-Alpha |
| miRNAs | MicroRNAs |
| MMPs | Matrix Metalloproteinases |
| NF-κB | Nuclear Factor Kappa-Light-Chain-Enhancer of Activated B Cells |
| MAPK | Mitogen-Activated Protein Kinase |
| ROS | Reactive Oxygen Species |
| NO | Nitric Oxide |
| Nrf2 | Nuclear Factor Erythroid 2-Related Factor 2 |
| Wnt | Wingless-Related Integration Site |
| Notch | Notch Gene |
| TGF-β | Transforming Growth Factor-Beta |
| TLR | Toll-Like Receptor |
| PTOA | Post-Traumatic Osteoarthritis |
| CaMKK2 | Calcium/Calmodulin-Dependent Protein Kinase Kinase 2 |
| SIRT1 | Sirtuin (Silent Mating Type Information Regulation 2 Homolog) 1 |
| COX-2 | Cyclooxygenase-2 |
| PI3K/AKT | Phosphatidylinositol 3-Kinase/Protein Kinase B (Also Known as Akt) |
| ROCK1 | Rho-Associated, Coiled-Coil-Containing Protein Kinase 1 |
| TLR9 | Toll-Like Receptor 9 |
| mTOR | Mammalian Target of Rapamycin |
| ADMSCs | Adipose-Derived MSCs |
| sEV-CUR | Curcumin-Loaded Small Extracellular Vesicles |
References
- Li, Y.; Xie, W.; Xiao, W.; Dou, D. Progress in Osteoarthritis Research by the National Natural Science Foundation of China. Bone Res. 2022, 10, 41. [Google Scholar] [CrossRef] [PubMed]
- ur Rehman, S.; Iqbal, S.; Umair Shahid, M.; Soman Jahangir, M.; Latif Malik, A. Cartilage: Structure, Function, and the Pathogenesis of Osteoarthritis. In Advancements in Synovial Joint Science—Structure, Function, and Beyond; IntechOpen: London, UK, 2024. [Google Scholar]
- Muthu, S.; Korpershoek, J.V.; Novais, E.J.; Tawy, G.F.; Hollander, A.P.; Martin, I. Failure of Cartilage Regeneration: Emerging Hypotheses and Related Therapeutic Strategies. Nat. Rev. Rheumatol. 2023, 19, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Nurul, A.A.; Azlan, M.; Ahmad Mohd Zain, M.R.; Sebastian, A.A.; Fan, Y.Z.; Fauzi, M.B. Mesenchymal Stem Cells: Current Concepts in the Management of Inflammation in Osteoarthritis. Biomedicines 2021, 9, 785. [Google Scholar] [CrossRef] [PubMed]
- Vadhan, A.; Gupta, T.; Hsu, W.L. Mesenchymal Stem Cell-Derived Exosomes as a Treatment Option for Osteoarthritis. Int. J. Mol. Sci. 2024, 25, 9149. [Google Scholar] [CrossRef]
- Česnik, A.B.; Švajger, U. The Issue of Heterogeneity of MSC-Based Advanced Therapy Medicinal Products–a Review. Front. Cell Dev. Biol. 2024, 12, 1400347. [Google Scholar] [CrossRef]
- Marchese, P. Development of a High Throughput Screening Strategy for Drug Discovery: From Marine Fungi to Stem Cell Applications. Ph.D. Thesis, National University of Ireland Galway, Galway, Ireland, 2021. [Google Scholar]
- Cutolo, E.A.; Caferri, R.; Campitiello, R.; Cutolo, M. The Clinical Promise of Microalgae in Rheumatoid Arthritis: From Natural Compounds to Recombinant Therapeutics. Mar. Drugs 2023, 21, 630. [Google Scholar] [CrossRef]
- Shi, S.; Zhang, L.; Jiang, K. Polysaccharide Nanosystems for Osteoarthritis Therapy: Mechanisms, Combinations, and Future Directions. Int. J. Biol. Macromol. 2024, 279, 135146. [Google Scholar] [CrossRef]
- Wang, Q.; Ying, L.; Wei, B.; Ji, Y.; Xu, Y. Effects of Quercetin on Apoptosis and Extracellular Matrix Degradation of Chondrocytes Induced by Oxidative Stress-Mediated Pyroptosis. J. Biochem. Mol. Toxicol. 2022, 36, e22951. [Google Scholar] [CrossRef]
- Wang, Z.; Efferth, T.; Hua, X.; Zhang, X.A. Medicinal Plants and Their Secondary Metabolites in Alleviating Knee Osteoarthritis: A Systematic Review. Phytomedicine 2022, 105, 154347. [Google Scholar] [CrossRef]
- Østerås, N.; Bunzli, S. Introduction to OA, Communication, and Person-Centered Care. In Osteoarthritis Health Professional Training Manual; Academic Press: Cambridge, MA, USA, 2023; pp. 1–14. [Google Scholar] [CrossRef]
- Surmachevska, N.; Rubio, J. Senescence in Osteoarthritis: Overview of Mechanisms and Therapeutics. Eur. J. Rheumatol. 2023, 11, S3–S6. [Google Scholar] [CrossRef]
- Fiksman, F.; Krekhovska-Lepiavko, O.M.; Lokay, B.A. Osteoarthritis: Its prevalence, risk factors, clinical manifestation, diagnosis and treatment. Медсестринствo 2023, 4, 7–9. [Google Scholar] [CrossRef]
- Bueno, N.P.; Hertel, F.C.; Fernandes e Oliveira, H.F.; Arany, P.; Beloti, M.M.; Marques, M.M.; Ferraz, E.P. Enhancing Osteoblast Differentiation and Bone Repair: The Priming Effect of Photobiomodulation on Adipose Stromal Cells. J. Photochem. Photobiol. B Biol. 2024, 260, 113040. [Google Scholar] [CrossRef] [PubMed]
- Huaco, V.; Tawil, B. Osteoarthritis: Physiology, Disease, Treatments, Market Analysis. Adv. Tissue Eng. Regen. Med. Open Access 2023, 9, 24–27. [Google Scholar] [CrossRef]
- Tuncay Duruöz, M.; Öz, N.; Gürsoy, D.E.; Hande Gezer, H. Clinical Aspects and Outcomes in Osteoarthritis. Best. Pract. Res. Clin. Rheumatol. 2023, 37, 101855. [Google Scholar] [CrossRef] [PubMed]
- Rahimi Darehbagh, R.; Seyedoshohadaei, S.A.; Ramezani, R.; Rezaei, N. Stem Cell Therapies for Neurological Disorders: Current Progress, Challenges, and Future Perspectives. Eur. J. Med. Res. 2024, 29, 386. [Google Scholar] [CrossRef]
- Shaik, M.I.; Hamdi, I.H.; Sarbon, N.M. A Comprehensive Review on Traditional Herbal Drinks: Physicochemical, Phytochemicals and Pharmacology Properties. Food Chem. Adv. 2023, 3, 100460. [Google Scholar] [CrossRef]
- Cai, X.; Yuan, S.; Zeng, Y.; Wang, C.; Yu, N.; Ding, C. New Trends in Pharmacological Treatments for Osteoarthritis. Front. Pharmacol. 2021, 12, 645842. [Google Scholar] [CrossRef]
- Ashraf, I.; Khan, Q.U.; Malik, F.; Asghar, S.S.; Mansoor, A.; Mansoor, E. Unveiling the Pathophysiology of Osteoarthritis in Joint Anatomy. J. Health Rehabil. Res. 2024, 4, 1478–1483. [Google Scholar] [CrossRef]
- Verma, R.; Nath, R.; Dhadiwal, R.K.; Daftary, G.V.; Jolapara, M.A.; Shah, R.A.; Patil, N.N. Mechanisms of Action of Native Collagen Type II and Aflapin® on the Pathophysiology of Osteoarthritis and Their Evidences. Int. J. Res. Orthop. 2024, 10, 1098–1107. [Google Scholar] [CrossRef]
- Coaccioli, S.; Sarzi-Puttini, P.; Zis, P.; Rinonapoli, G.; Varrassi, G. Osteoarthritis: New Insight on Its Pathophysiology. J. Clin. Med. 2022, 11, 6013. [Google Scholar] [CrossRef]
- Gilbert, S.J.; Jones, R.; Egan, B.J.; Bonnet, C.S.; Evans, S.L.; Mason, D.J. Investigating Mechanical and Inflammatory Pathological Mechanisms in Osteoarthritis Using MSC-Derived Osteocyte-like Cells in 3D. Front. Endocrinol. 2024, 15, 1484912. [Google Scholar] [CrossRef] [PubMed]
- Szala, D.; Kopańska, M.; Trojniak, J.; Jabłoński, J.; Hanf-Osetek, D.; Snela, S.; Zawlik, I. The Role of MicroRNAs in the Pathophysiology of Osteoarthritis. Int. J. Mol. Sci. 2024, 25, 6352. [Google Scholar] [CrossRef] [PubMed]
- Sharif, M.U.; Aslam, H.M.; Iftakhar, T.; Abdullah, M. Pathophysiology of Cartilage Damage in Knee Osteoarthritis and Regenerative Approaches toward Recovery. J. Bone Jt. Dis. 2024, 39, 32–44. [Google Scholar] [CrossRef]
- Chen, B.; Wang, L.; Xie, D.; Wang, Y. Exploration and Breakthrough in the Mode of Chondrocyte Death—A Potential New Mechanism for Osteoarthritis. Biomed. Pharmacother. 2024, 170, 115990. [Google Scholar] [CrossRef]
- Singh, A.; Rai, V.; Pandey, S.; Chavan, M.; Ketha, D. Osteoarthritis: Insights into Pathogenesis and Futuristic Treatment Strategies. Int. J. Res. Orthop. 2022, 8, 765–774. [Google Scholar] [CrossRef]
- Mukherjee, A.; Das, B. The Role of Inflammatory Mediators and Matrix Metalloproteinases (MMPs) in the Progression of Osteoarthritis. Biomater. Biosyst. 2024, 13, 100090. [Google Scholar] [CrossRef]
- Wang, M.N.; Liu, L.; Zhao, L.P.; Yuan, F.; Fu, Y.B.; Xu, X.B.; Li, B. Research of Inflammatory Factors and Signaling Pathways in Knee Osteoarthritis. China J. Orthop. Traumatol. 2020, 33, 388–392. [Google Scholar]
- Chow, Y.Y.; Chin, K.Y. The Role of Inflammation in the Pathogenesis of Osteoarthritis. Mediat. Inflamm. 2020, 2020, 8293921. [Google Scholar] [CrossRef]
- Wu, P.; Li, M.; Shi, X.; Jie, L.; Mao, J.; Yin, S. The Identification of Key Genes and Pathways in Osteoarthritis-Related Inflammatory Synoviocytes by Bioinformatics Analysis. Preprint 2022. [Google Scholar] [CrossRef]
- Okikiade, A.; Osharode, A.; Oyewole, A.; Ogunesan, D.; Oladejo, D.; Oshobu, I.; Browne, K. Understanding the Role of Inflammation in Secondary Osteoarthritis. Asian J. Med. Health 2022, 20, 60–74. [Google Scholar] [CrossRef]
- Lee, Y.T.; Yunus, M.H.M.; Ugusman, A.; Yazid, M.D. Natural Compounds Affecting Inflammatory Pathways of Osteoarthritis. Antioxidants 2022, 11, 1722. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Rebouh, N.Y. Anti-Osteoarthritis Mechanism of the Nrf2 Signaling Pathway. Biomedicines 2023, 11, 3176. [Google Scholar] [CrossRef]
- Han, P.F.; Zhang, Z.L.; Chen, T.Y.; Zhao, R.P.; Zhang, R.; Li, X.D.; Li, P.C.; Wei, L.; Lv, Z.; Wei, X.C. Initial Effects of Inflammation-Related Cytokines and Signaling Pathways on the Pathogenesis of Post-Traumatic Osteoarthritis. Front. Nurs. 2018, 5, 91–96. [Google Scholar] [CrossRef]
- Riggs, K.C.; Sankar, U. Inflammatory Mechanisms in Post-Traumatic Osteoarthritis: A Role for CaMKK2. Immunometabolism 2023, 5, e00031. [Google Scholar] [CrossRef]
- Bar-Or, D.; Rael, L.T.; Thomas, G.W.; Brody, E.N. Inflammatory Pathways in Knee Osteoarthritis: Potential Targets for Treatment. Curr. Rheumatol. Rev. 2015, 11, 50–58. [Google Scholar] [CrossRef]
- Tian, R.; Su, S.; Yu, Y.; Liang, S.; Ma, C.; Jiao, Y.; Xing, W.; Tian, Z.; Jiang, T.; Wang, J. Revolutionizing Osteoarthritis Treatment: How Mesenchymal Stem Cells Hold the Key. Biomed. Pharmacother. 2024, 173, 116458. [Google Scholar] [CrossRef]
- Kwon, D.G.; Kim, M.K.; Jeon, Y.S.; Nam, Y.C.; Park, J.S.; Ryu, D.J. State of the Art: The Immunomodulatory Role of MSCs for Osteoarthritis. Int. J. Mol. Sci. 2022, 23, 1618. [Google Scholar] [CrossRef]
- Huang, Y.; Wu, Q.; Tam, P.K.H. Immunomodulatory Mechanisms of Mesenchymal Stem Cells and Their Potential Clinical Applications. Int. J. Mol. Sci. 2022, 23, 10023. [Google Scholar] [CrossRef]
- Jovic, D.; Yu, Y.; Wang, D.; Wang, K.; Li, H.; Xu, F.; Liu, C.; Liu, J.; Luo, Y. A Brief Overview of Global Trends in MSC-Based Cell Therapy. Stem Cell Rev. Rep. 2022, 18, 1525–1545. [Google Scholar] [CrossRef] [PubMed]
- Dunn, C.M.; Kameishi, S.; Grainger, D.W.; Okano, T. Strategies to Address Mesenchymal Stem/Stromal Cell Heterogeneity in Immunomodulatory Profiles to Improve Cell-Based Therapies. Acta Biomater. 2021, 133, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Ceruso, A.; Gonzalez-Pujana, A.; Igartua, M.; Santos-Vizcaino, E.; Hernandez, R.M. Latest Advances to Enhance the Therapeutic Potential of Mesenchymal Stromal Cells for the Treatment of Immune-Mediated Diseases. Drug Deliv. Transl. Res. 2021, 11, 498–514. [Google Scholar] [CrossRef] [PubMed]
- Zhidu, S.; Ying, T.; Rui, J.; Chao, Z. Translational Potential of Mesenchymal Stem Cells in Regenerative Therapies for Human Diseases: Challenges and Opportunities. Stem Cell Res. Ther. 2024, 15, 266. [Google Scholar] [CrossRef]
- Pérez-Lozano, M.L.; Cesaro, A.; Mazor, M.; Esteve, E.; Berteina-Raboin, S.; Best, T.M.; Lespessailles, E.; Toumi, H. Emerging Natural-Product-Based Treatments for the Management of Osteoarthritis. Antioxidants 2021, 10, 265. [Google Scholar] [CrossRef]
- Wang, L.; He, C. Nrf2-Mediated Anti-Inflammatory Polarization of Macrophages as Therapeutic Targets for Osteoarthritis. Front. Immunol. 2022, 13, 967193. [Google Scholar] [CrossRef]
- Chopra, B.; Dhingra, A.K. Natural Products: A Lead for Drug Discovery and Development. Phytother. Res. 2021, 35, 4660–4702. [Google Scholar] [CrossRef]
- Karthikeyan, A.; Joseph, A.; Nair, B.G. Promising Bioactive Compounds from the Marine Environment and Their Potential Effects on Various Diseases. J. Genet. Eng. Biotechnol. 2022, 20, 14. [Google Scholar] [CrossRef]
- Chaachouay, N.; Zidane, L. Plant-Derived Natural Products: A Source for Drug Discovery and Development. Drugs Drug Candidates 2024, 3, 184–207. [Google Scholar] [CrossRef]
- Huynh, T.T.T.; Quang, M.T.; Vu, H.Y.T. Modulation of Inflammatory Signaling Pathways by Natural Products in Osteoarthritis: Mechanisms, Challenges, and Future Directions. Trop. J. Pharm. Res. 2024, 23, 1387–1396. [Google Scholar] [CrossRef]
- Wang, X.; He, W.; Huang, H.; Han, J.; Wang, R.; Li, H.; Long, Y.; Wang, G.; Han, X. Recent Advances in Hydrogel Technology in Delivering Mesenchymal Stem Cell for Osteoarthritis Therapy. Biomolecules 2024, 14, 858. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Wang, Z.; Dong, L.; Zhang, D.; Shang, F.; Li, A.; Gao, Y.; Bai, Q.; Liu, D.; Xie, X.; et al. Natural Small Molecules Synergize Mesenchymal Stem Cells for Injury Repair in Vital Organs: A Comprehensive Review. Stem Cell Res. Ther. 2024, 15, 243. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Long, Y.; Wang, Y.; Chin, K.-Y. Osteoarthritis: An Integrative Overview from Pathogenesis to Management. Malays. J. Pathol. 2024, 46, 369. [Google Scholar] [PubMed]
- Costa, L.A.; Eiro, N.; Fraile, M.; Gonzalez, L.O.; Saá, J.; Garcia-Portabella, P.; Vega, B.; Schneider, J.; Vizoso, F.J. Functional Heterogeneity of Mesenchymal Stem Cells from Natural Niches to Culture Conditions: Implications for Further Clinical Uses. Cell. Mol. Life Sci. 2021, 78, 447–467. [Google Scholar] [CrossRef]
- Gao, Y.; Xu, X.; Zhang, X. Targeting Different Phenotypes of Macrophages: A Potential Strategy for Natural Products to Treat Inflammatory Bone and Joint Diseases. Phytomedicine 2023, 118, 154952. [Google Scholar] [CrossRef]
- Gonzalez-Fernandez, P.; Rodríguez-Nogales, C.; Jordan, O.; Allémann, E. Combination of Mesenchymal Stem Cells and Bioactive Molecules in Hydrogels for Osteoarthritis Treatment. Eur. J. Pharm. Biopharm. 2022, 172, 41–52. [Google Scholar] [CrossRef]
- Schulze-Tanzil, G. Experimental Therapeutics for the Treatment of Osteoarthritis. J. Exp. Pharmacol. 2021, 13, 101–125. [Google Scholar] [CrossRef]
- Nguyen, T.H.; Duong, C.M.; Nguyen, X.H.; Than, U.T.T. Mesenchymal Stem Cell-Derived Extracellular Vesicles for Osteoarthritis Treatment: Extracellular Matrix Protection, Chondrocyte and Osteocyte Physiology, Pain and Inflammation Management. Cells 2021, 10, 2887. [Google Scholar] [CrossRef]
- Koroljević, Z.D.; Jordan, K.; Ivković, J.; Bender, D.V.; Perić, P. Curcuma as an Anti-Inflammatory Component in Treating Osteoarthritis. Rheumatol. Int. 2023, 43, 589–616. [Google Scholar] [CrossRef]
- Yang, S.; Sun, M.; Zhang, X. Protective Effect of Resveratrol on Knee Osteoarthritis and Its Molecular Mechanisms: A Recent Review in Preclinical and Clinical Trials. Front. Pharmacol. 2022, 13, 921003. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, X.; Xu, W.; Li, Y.; Lai, R.; Qiu, X.; Chen, X.; Chen, Z.; Mi, B.; Wu, M.; et al. Translational Challenges and Prospective Solutions in the Implementation of Biomimetic Delivery Systems. Pharmaceutics 2023, 15, 2623. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.S.; Liao, W.Y.; Huang, C.W.; Chang, C.H. Adipose-Derived Stem Cells Preincubated with Green Tea EGCG Enhance Pancreatic Tissue Regeneration in Rats with Type 1 Diabetes through ROS/Sirt1 Signaling Regulation. Int. J. Mol. Sci. 2022, 23, 3165. [Google Scholar] [CrossRef] [PubMed]
- Burczak, A.; Kosiedowska, M.; Borkowska, P.; Kowalski, J. Cytoprotective Roles of Epigallocatechin Gallate and Resveratrol on Staurosporine-Treated Mesenchymal Stem Cells in In Vitro Culture. Herba Pol. 2021, 67, 45–52. [Google Scholar] [CrossRef]
- El-Desoky Mohamady, R.E.; Elwia, S.K.; Abo El Wafa, S.M.; Mohamed, M.A. Effect of Mesenchymal Stem Cells Derived Exosomes and Green Tea Polyphenols on Acetic Acid Induced Ulcerative Colitis in Adult Male Albino Rats. Ultrastruct. Pathol. 2022, 46, 147–163. [Google Scholar] [CrossRef]
- Yang, Q.; Xu, Y.; Bin, X.; Chan, K.P.; Chen, S.; Qian, Z.; Yao, Y.; Yuan, X.L.; Qiu, K.; Huang, Y.; et al. Combined Treatment of Human Mesenchymal Stem Cells and Green Tea Extract on Retinal Ganglion Cell Regeneration in Rats after Optic Nerve Injury. Exp. Eye Res. 2024, 239, 109787. [Google Scholar] [CrossRef]
- Xu, S.; Chang, L.; Zhao, X.; Hu, Y.; Lin, Y.; Chen, Z.; Ren, X.; Mei, X. Preparation of Epigallocatechin Gallate Decorated Au-Ag Nano-Heterostructures as NIR-Sensitive Nano-Enzymes for the Treatment of Osteoarthritis through Mitochondrial Repair and Cartilage Protection. Acta Biomater. 2022, 144, 168–182. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhang, M.; Sun, Y.; Li, M.; Chang, C.; Liu, W.; Zhu, X.; Wei, L.; Wen, F.; Liu, Y. Effects of Adipose Derived Stem Cells Pretreated with Resveratrol on Sciatic Nerve Regeneration in Rats. Sci. Rep. 2023, 13, 5812. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Avantario, P.; Azzollini, D.; Buongiorno, S.; Viapiano, F.; Campanelli, M.; Ciocia, A.M.; De Leonardis, N.; et al. Effects of Resveratrol, Curcumin and Quercetin Supplementation on Bone Metabolism—A Systematic Review. Nutrients 2022, 14, 3519. [Google Scholar] [CrossRef]
- Wang, H.; Yan, Y.; Pathak, J.L.; Hong, W.; Zeng, J.; Qian, D.; Hao, B.; Li, H.; Gu, J.; Jaspers, R.T.; et al. Quercetin Prevents Osteoarthritis Progression Possibly via Regulation of Local and Systemic Inflammatory Cascades. J. Cell Mol. Med. 2023, 27, 515–528. [Google Scholar] [CrossRef]
- Fang, S.; Zhang, B.; Xiang, W.; Zheng, L.; Wang, X.; Li, S.; Zhang, T.; Feng, D.; Gong, Y.; Wu, J.; et al. Natural Products in Osteoarthritis Treatment: Bridging Basic Research to Clinical Applications. Chin. Med. 2024, 19, 25. [Google Scholar] [CrossRef]
- Han, X.; Jia, G.F.; Zhu, F. Resveratrol Alleviates Osteoporosis by Promoting Osteogenic Differentiation of Bone Marrow Mesenchymal Stem Cells via SITR1/PI3K/AKT Pathway. Int. J. Morphol. 2024, 42, 216–224. [Google Scholar] [CrossRef]
- Ruan, H.; Zhu, T.; Wang, T.; Guo, Y.; Liu, Y.; Zheng, J. Quercetin Modulates Ferroptosis via the SIRT1/Nrf−2/HO−1 Pathway and Attenuates Cartilage Destruction in an Osteoarthritis Rat Model. Int. J. Mol. Sci. 2024, 25, 7461. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, E.J. Hormesis and Adult Adipose-Derived Stem Cells. Pharmacol. Res. 2021, 172, 105803. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Song, Z.; Yu, J.; Ren, B.; Dong, Y.; You, Y.; Zhang, Z.; Jia, C.; Zhao, Y.; Zhou, X.; et al. Supramolecular Self-Assembly of EGCG-Selenomethionine Nanodrug for Treating Osteoarthritis. Bioact. Mater. 2024, 32, 164–176. [Google Scholar] [CrossRef]
- Razavi, B.M.; Ghasemzadeh Rahbardar, M.; Hosseinzadeh, H. A Review of Therapeutic Potentials of Turmeric (Curcuma longa) and Its Active Constituent, Curcumin, on Inflammatory Disorders, Pain, and Their Related Patents. Phytother. Res. 2021, 35, 6489–6513. [Google Scholar] [CrossRef]
- Memarzia, A.; Khazdair, M.R.; Behrouz, S.; Gholamnezhad, Z.; Jafarnezhad, M.; Saadat, S.; Boskabady, M.H. Experimental and Clinical Reports on Anti-Inflammatory, Antioxidant, and Immunomodulatory Effects of Curcuma Longa and Curcumin, an Updated and Comprehensive Review. BioFactors 2021, 47, 311–350. [Google Scholar] [CrossRef]
- Li, W.; Xiang, Z.; Yu, W.; Huang, X.; Jiang, Q.; Abumansour, A.; Yang, Y.; Chen, C. Natural Compounds and Mesenchymal Stem Cells: Implications for Inflammatory-Impaired Tissue Regeneration. Stem Cell Res. Ther. 2024, 15, 34. [Google Scholar] [CrossRef]
- Li, C.; Xu, Y.; Zhang, J.; Zhang, Y.; He, W.; Ju, J.; Wu, Y.; Wang, Y. The Effect of Resveratrol, Curcumin and Quercetin Combination on Immuno-Suppression of Tumor Microenvironment for Breast Tumor-Bearing Mice. Sci. Rep. 2023, 13, 13278. [Google Scholar] [CrossRef]
- Deng, J.; Ouyang, P.; Li, W.; Zhong, L.; Gu, C.; Shen, L.; Cao, S.; Yin, L.; Ren, Z.; Zuo, Z.; et al. Curcumin Alleviates the Senescence of Canine Bone Marrow Mesenchymal Stem Cells during in Vitro Expansion by Activating the Autophagy Pathway. Int. J. Mol. Sci. 2021, 22, 11356. [Google Scholar] [CrossRef]
- Xu, C.; Zhai, Z.; Ying, H.; Lu, L.; Zhang, J.; Zeng, Y. Curcumin Primed ADMSCs Derived Small Extracellular Vesicle Exert Enhanced Protective Effects on Osteoarthritis by Inhibiting Oxidative Stress and Chondrocyte Apoptosis. J. Nanobiotechnology 2022, 20, 123. [Google Scholar] [CrossRef]
- Ghorbaninejad, M.; Khademi-Shirvan, M.; Hosseini, S.; Meyfour, A.; Shahhoseini, M.; Baghaban Eslaminejad, M. Effective Role of Curcumin on Expression Regulation of EZH2 Histone Methyltransferase as a Dynamic Epigenetic Factor in Osteogenic Differentiation of Human Mesenchymal Stem Cells. Biochim. Biophys. Acta Gene Regul. Mech. 2023, 1866, 194903. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Zhang, Q.; Zou, Z.; Li, Z.; Jin, M.; An, J.; Li, H.; Ma, J. Curcumin Supplementation Enhances Bone Marrow Mesenchymal Stem Cells to Promote the Anabolism of Articular Chondrocytes and Cartilage Repair. Cell Transplant. 2021, 30, 0963689721993776. [Google Scholar] [CrossRef] [PubMed]
- Strecanska, M.; Danisovic, L.; Ziaran, S.; Cehakova, M. The Role of Extracellular Matrix and Hydrogels in Mesenchymal Stem Cell Chondrogenesis and Cartilage Regeneration. Life 2022, 12, 2066. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Xu, H.; Qian, W. The Role and Current Research Status of Resveratrol in the Treatment of Osteoarthritis and Its Mechanisms: A Narrative Review. Drug Metab. Rev. 2024, 56, 399–412. [Google Scholar] [CrossRef]
- Aleebrahim-Dehkordi, E.; Soveyzi, F.; Arian, A.S.; Hamedanchi, N.F.; Hasanpour-Dehkordi, A.; Rafieian-Kopaei, M. Quercetin and Its Role in Reducing the Expression of Pro-Inflammatory Cytokines in Osteoarthritis. Antiinflamm Antiallergy Agents Med. Chem. 2022, 21, 153–165. [Google Scholar] [CrossRef]
- Yamaura, K.; Nelson, A.L.; Nishimura, H.; Rutledge, J.C.; Ravuri, S.K.; Bahney, C.; Philippon, M.J.; Huard, J. Therapeutic Potential of Senolytic Agent Quercetin in Osteoarthritis: A Systematic Review and Meta-Analysis of Preclinical Studies. Ageing Res. Rev. 2023, 90, 101989. [Google Scholar] [CrossRef]
- Hridayanka, K.S.N.; Duttaroy, A.K.; Basak, S. Bioactive Compounds and Their Chondroprotective Effects for Osteoarthritis Amelioration: A Focus on Nanotherapeutic Strategies, Epigenetic Modifications, and Gut Microbiota. Nutrients 2024, 16, 3587. [Google Scholar] [CrossRef]
- Li, W.; Huang, Y.; Fan, L.; Yangzom, D.; Zhang, K.; Shen, L.; Cao, S.; Gu, C.; Yu, S. Curcumin Liposomes Alleviate Senescence of Bone Marrow Mesenchymal Stem Cells by Activating Mitophagy. Sci. Rep. 2024, 14, 31291. [Google Scholar] [CrossRef]
- Xia, S.; Weng, T.; Jin, R.; Yang, M.; Yu, M.; Zhang, W.; Wang, X.; Han, C. Curcumin-Incorporated 3D Bioprinting Gelatin Methacryloyl Hydrogel Reduces Reactive Oxygen Species-Induced Adipose-Derived Stem Cell Apoptosis and Improves Implanting Survival in Diabetic Wounds. Burns Trauma. 2022, 10, tkac001. [Google Scholar] [CrossRef]
- Ma, C.Y.; Zhai, Y.; Li, C.T.; Liu, J.; Xu, X.; Chen, H.; Tse, H.F.; Lian, Q. Translating Mesenchymal Stem Cell and Their Exosome Research into GMP Compliant Advanced Therapy Products: Promises, Problems and Prospects. Med. Res. Rev. 2024, 44, 919–938. [Google Scholar] [CrossRef]
- Ilyas, S.; Lee, J.; Lee, D. Emerging Roles of Natural Compounds in Osteoporosis: Regulation, Molecular Mechanisms and Bone Regeneration. Pharmaceuticals 2024, 17, 984. [Google Scholar] [CrossRef] [PubMed]
- Silvestrini, A.; Giordani, C.; Bonacci, S.; Giuliani, A.; Ramini, D.; Matacchione, G.; Sabbatinelli, J.; Di Valerio, S.; Pacetti, D.; Procopio, A.D.; et al. Anti-Inflammatory Effects of Olive Leaf Extract and Its Bioactive Compounds Oleacin and Oleuropein-Aglycone on Senescent Endothelial and Small Airway Epithelial Cells. Antioxidants 2023, 12, 1509. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liu, Z.; Luo, Y.; Li, X.; Huang, G.; Chen, H.; Li, A.; Qin, S. The Role of Flavonoids in the Osteogenic Differentiation of Mesenchymal Stem Cells. Front. Pharmacol. 2022, 13, 849513. [Google Scholar] [CrossRef] [PubMed]
- Gowd, V.; Kanika; Jori, C.; Chaudhary, A.A.; Rudayni, H.A.; Rashid, S.; Khan, R. Resveratrol and Resveratrol Nano-Delivery Systems in the Treatment of Inflammatory Bowel Disease. J. Nutr. Biochem. 2022, 109, 109101. [Google Scholar] [CrossRef]
- Ghahremani, H.; Bahramzadeh, A.; Bolandnazar, K.; Emamgholipor, S.; Hosseini, H.; Meshkani, R. Resveratrol as a Potential Protective Compound against Metabolic Inflammation. Acta Biochim. Iran. 2023, 1, 50–64. [Google Scholar] [CrossRef]
- Fakhri, S.; Abbaszadeh, F.; Moradi, S.Z.; Cao, H.; Khan, H.; Xiao, J. Effects of Polyphenols on Oxidative Stress, Inflammation, and Interconnected Pathways during Spinal Cord Injury. Oxid. Med. Cell Longev. 2022, 2022, 8100195. [Google Scholar] [CrossRef]
- Jantan, I.; Haque, M.A.; Arshad, L.; Harikrishnan, H.; Septama, A.W.; Mohamed-Hussein, Z.A. Dietary Polyphenols Suppress Chronic Inflammation by Modulation of Multiple Inflammation-Associated Cell Signaling Pathways. J. Nutr. Biochem. 2021, 93, 108634. [Google Scholar] [CrossRef]
- Khan, M.I.; Hossain, M.I.; Hossain, M.K.; Rubel, M.H.K.; Hossain, K.M.; Mahfuz, A.M.U.B.; Anik, M.I. Recent Progress in Nanostructured Smart Drug Delivery Systems for Cancer Therapy: A Review. ACS Appl. Bio Mater. 2022, 5, 971–1012. [Google Scholar] [CrossRef]
- Rahiman, N.; Markina, Y.V.; Kesharwani, P.; Johnston, T.P.; Sahebkar, A. Curcumin-Based Nanotechnology Approaches and Therapeutics in Restoration of Autoimmune Diseases. J. Control. Release 2022, 348, 264–286. [Google Scholar] [CrossRef]
- Gayathri, K.; Bhaskaran, M.; Selvam, C.; Thilagavathi, R. Nano Formulation Approaches for Curcumin Delivery—A Review. J. Drug Deliv. Sci. Technol. 2023, 82, 104326. [Google Scholar] [CrossRef]
- Hafez Ghoran, S.; Calcaterra, A.; Abbasi, M.; Taktaz, F.; Nieselt, K.; Babaei, E. Curcumin-Based Nanoformulations: A Promising Adjuvant towards Cancer Treatment. Molecules 2022, 27, 5236. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Afzal, S.; Zheng, Y.F.; Münch, G.; Li, C.G. Synergistic Protective Effect of Curcumin and Resveratrol against Oxidative Stress in Endothelial EAhy926 Cells. Evid.-Based Complement. Altern. Med. 2021, 2021, 2661025. [Google Scholar] [CrossRef] [PubMed]
- Patra, S.; Pradhan, B.; Nayak, R.; Behera, C.; Rout, L.; Jena, M.; Efferth, T.; Bhutia, S.K. Chemotherapeutic Efficacy of Curcumin and Resveratrol against Cancer: Chemoprevention, Chemoprotection, Drug Synergism and Clinical Pharmacokinetics. Semin. Cancer Biol. 2021, 73, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Ghaeini Hesarooeyeh, Z.; Basham, A.; Sheybani-Arani, M.H.; Abbaszadeh, M.; Salimi Asl, A.; Moghbeli, M.; Saburi, E. Effect of Resveratrol and Curcumin and the Potential Synergism on Hypertension: A Mini-Review of Human and Animal Model Studies. Phytother. Res. 2024, 38, 42–58. [Google Scholar] [CrossRef]
- Laszló, I.P.; Laszló, M.R.; Popescu, T.; Toma, V.; Ion, R.M.; Moldovan, R.; Filip, G.A.; Cainap, C.; Clichici, S.; Muresan, A. The Comparative Effects of Resveratrol and Curcumin in Combination with Photodynamic Therapy. Med. Pharm. Rep. 2022, 95, 165–178. [Google Scholar] [CrossRef]
- Ra, K.; Park, S.C.; Lee, B.C. Female Reproductive Aging and Oxidative Stress: Mesenchymal Stem Cell Conditioned Medium as a Promising Antioxidant. Int. J. Mol. Sci. 2023, 24, 5053. [Google Scholar] [CrossRef]
- Ma, Y.; Qian, Y.; Chen, Y.; Ruan, X.; Peng, X.; Sun, Y.; Zhang, J.; Luo, J.; Zhou, S.; Deng, C. Resveratrol Modulates the Inflammatory Response in HPDLSCs via the NRF2/HO-1 and NF-ΚB Pathways and Promotes Osteogenic Differentiation. J. Periodontal Res. 2024, 59, 162–173. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, X.; Si, H. Synergistic Anti-Inflammatory Effects and Mechanisms of the Combination of Resveratrol and Curcumin in Human Vascular Endothelial Cells and Rodent Aorta. J. Nutr. Biochem. 2022, 108, 109083. [Google Scholar] [CrossRef]
- Salehi, B.; Cruz-Martins, N.; Butnariu, M.; Sarac, I.; Bagiu, I.C.; Ezzat, S.M.; Wang, J.; Koay, A.; Sheridan, H.; Adetunji, C.O.; et al. Hesperetin’s Health Potential: Moving from Preclinical to Clinical Evidence and Bioavailability Issues, to Upcoming Strategies to Overcome Current Limitations. Crit. Rev. Food Sci. Nutr. 2022, 62, 4449–4464. [Google Scholar] [CrossRef]
- Harney, T.L.; Harney, T.L. Resveratrol and Curcumin: Extending the Frontier of Phytomedicine. In Medicinal Plants-Harnessing the Healing Power of Plants; IntechOpen: Rijeka, Croatia, 2024. [Google Scholar] [CrossRef]
- Liu, Y.; Li, C.; Deng, M.; Ma, Y.; Jin, Z.; Shen, C. Potential Role of Herbal Remedies on Mesenchymal Stem Cells: An Overview of New Therapeutic Strategies for Osteoporosis. J. Organoid Biosci. 2024, 2, 60–88. [Google Scholar] [CrossRef]
- Vikal, A.; Maurya, R.; Bhowmik, S.; Khare, S.; Raikwar, S.; Patel, P.; Das Kurmi, B. Resveratrol: A Comprehensive Review of Its Multifaceted Health Benefits, Mechanisms of Action, and Potential Therapeutic Applications in Chronic Disease. Pharmacol. Res. Nat. Prod. 2024, 3, 100047. [Google Scholar] [CrossRef]
- Jamshidi, V.; Halabian, R.; Saeedi, P.; Bagheri, H.; Ghoochani, B.F.N.M. Accelerating Synergistic Effects of Preconditioned Mesenchymal Stem Cells with Crocin and Dexamethasone in Pulmonary Epithelial Cells Injury. Toxicol. Res. 2023, 12, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yu, H.; Zhang, Y.; Chang, X.; Liu, C.; Wen, X.; Tian, F.; Li, Y. Curcumin Alleviates Osteoarthritis Through the P38MAPK Pathway: Network Pharmacological Prediction and Experimental Confirmation. J. Inflamm. Res. 2024, 17, 5039–5056. [Google Scholar] [CrossRef] [PubMed]
- Makuch, S.; Więcek, K.; Woźniak, M. The Immunomodulatory and Anti-Inflammatory Effect of Curcumin on Immune Cell Populations, Cytokines, and in Vivo Models of Rheumatoid Arthritis. Pharmaceuticals 2021, 14, 309. [Google Scholar] [CrossRef]
- Wei, Y.; Guo, A.; Liu, Z.; Zhang, L.; Liao, W.; Liu, J.; Mao, L.; Yuan, F.; Gao, Y. Development of Curcumin Loaded Core-Shell Zein Microparticles Stabilized by Cellulose Nanocrystals and Whey Protein Microgels through Interparticle Interactions. Food Funct. 2021, 12, 6936–6949. [Google Scholar] [CrossRef]
- Sable, A.A.; Kunwar, A.; Barik, A. Alginate and Chitosan-Based Delivery Systems for Improving the Bioavailability and Therapeutic Efficacy of Curcumin. Pharmaceutics 2024, 16, 423. [Google Scholar] [CrossRef]
- Yao, J.; Liu, X.; Sun, Y.; Dong, X.; Liu, L.; Gu, H. Curcumin-Alleviated Osteoarthritic Progression in Rats Fed a High-Fat Diet by Inhibiting Apoptosis and Activating Autophagy via Modulation of MicroRNA-34a. J. Inflamm. Res. 2021, 14, 2317–2331. [Google Scholar] [CrossRef]
- Vassallo, V.; Di Meo, C.; Toro, G.; Alfano, A.; Iolascon, G.; Schiraldi, C. Hyaluronic Acid-Based Injective Medical Devices: In Vitro Characterization of Novel Formulations Containing Biofermentative Unsulfated Chondroitin or Extractive Sulfated One with Cyclodextrins. Pharmaceuticals 2023, 16, 1429. [Google Scholar] [CrossRef]
- Sheng, S.; Wang, X.; Liu, X.; Hu, X.; Shao, Y.; Wang, G.; Mao, D.; Li, C.; Chen, B.; Chen, X. The Role of Resveratrol on Rheumatoid Arthritis: From Bench to Bedside. Front. Pharmacol. 2022, 13, 829677. [Google Scholar] [CrossRef]
- Markov, A.; Thangavelu, L.; Aravindhan, S.; Zekiy, A.O.; Jarahian, M.; Chartrand, M.S.; Pathak, Y.; Marofi, F.; Shamlou, S.; Hassanzadeh, A. Mesenchymal Stem/Stromal Cells as a Valuable Source for the Treatment of Immune-Mediated Disorders. Stem Cell Res. Ther. 2021, 12, 192. [Google Scholar] [CrossRef]
- Liang, C.C.; Xing, H.; Wang, C.Y.; Xu, X.F.; Hao, Y.; Qiu, B. Resveratrol Protection against IL-1β-Induced Chondrocyte Damage via the SIRT1/FOXO1 Signaling Pathway. J. Orthop. Surg. Res. 2022, 17, 406. [Google Scholar] [CrossRef] [PubMed]
- Cong, L.; Lei, M.Y.; Liu, Z.Q.; Liu, Z.F.; Ma, Z.; Liu, K.; Li, J.; Deng, Y.; Liu, W.; Xu, B. Resveratrol Attenuates Manganese-Induced Oxidative Stress and Neuroinflammation through SIRT1 Signaling in Mice. Food Chem. Toxicol. 2021, 153, 112283. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.G.; Best, T.M.; Huard, J.; Philippon, M.; Hornicek, F.; Duan, Z.; Griswold, A.J.; Kaplan, L.D.; Hare, J.M.; Kouroupis, D. Therapeutic Perspectives for Inflammation and Senescence in Osteoarthritis Using Mesenchymal Stem Cells, Mesenchymal Stem Cell-Derived Extracellular Vesicles and Senolytic Agents. Cells 2023, 12, 1421. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.R.; Lee, Y.H.; Bat-Ulzii, A.; Chatterjee, S.; Bhattacharya, M.; Chakraborty, C.; Lee, S.S. Bioactivity, Molecular Mechanism, and Targeted Delivery of Flavonoids for Bone Loss. Nutrients 2023, 15, 919. [Google Scholar] [CrossRef]
- Wang, N.; Wang, L.; Yang, J.; Wang, Z.; Cheng, L. Quercetin Promotes Osteogenic Differentiation and Antioxidant Responses of Mouse Bone Mesenchymal Stem Cells through Activation of the AMPK/SIRT1 Signaling Pathway. Phytother. Res. 2021, 35, 2639–2650. [Google Scholar] [CrossRef]
- Xing, X.; Tang, Q.; Zou, J.; Huang, H.; Yang, J.; Gao, X.; Xu, X.; Ma, S.; Li, M.; Liang, C.; et al. Bone-Targeted Delivery of Senolytics to Eliminate Senescent Cells Increases Bone Formation in Senile Osteoporosis. Acta Biomater. 2023, 157, 352–366. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, C.; Wen, L.; Ling, Z.; Xia, J.; Cheng, B.; Peng, J. Quercetin Ameliorates Senescence and Promotes Osteogenesis of BMSCs by Suppressing the Repetitive Element-triggered RNA Sensing Pathway. Int. J. Mol. Med. 2025, 55, 4. [Google Scholar] [CrossRef]
- Liu, L.; Liu, Y.; Zhen, Y.; Guo, T.; Wang, C.; Shen, L.; Li, W. Quercetin Inhibits Cytotoxicity of PC12 Cells Induced by Amyloid-Beta 25-35 via Stimulating Estrogen Receptor α, Activating ERK1/2, and Inhibiting Apoptosis. Open Life Sci. 2022, 17, 230–242. [Google Scholar] [CrossRef]
- Goyal, A.; Agrawal, N. Quercetin: A Potential Candidate for the Treatment of Arthritis. Curr. Mol. Med. 2021, 22, 325–335. [Google Scholar] [CrossRef]
- Kim, J.G.; Sharma, A.R.; Lee, Y.-H.; Chatterjee, S.; Choi, Y.J.; Rajvansh, R.; Chakraborty, C.; Lee, S.-S. Therapeutic Potential of Quercetin as an Antioxidant for Bone-Muscle-Tendon Regeneration and Aging. Aging Dis. 2024, 16, 1–25. [Google Scholar] [CrossRef]
- Samadi, F.; Kahrizi, M.S.; Heydari, F.; Arefnezhad, R.; Roghani-Shahraki, H.; Mokhtari Ardekani, A.; Rezaei-Tazangi, F. Quercetin and Osteoarthritis: A Mechanistic Review on the Present Documents. Pharmacology 2022, 107, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Shen, P.; Lin, W.; Ba, X.; Huang, Y.; Chen, Z.; Han, L.; Qin, K.; Huang, Y.; Tu, S. Quercetin-Mediated SIRT1 Activation Attenuates Collagen-Induced Mice Arthritis. J. Ethnopharmacol. 2021, 279, 114213. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Lin, Y.; Fang, X.; Yang, J.; Chen, Z. Epigallocatechin-3-Gallate Promotes Osteo-/Odontogenic Differentiation of Stem Cells from the Apical Papilla through Activating the Bmp–Smad Signaling Pathway. Molecules 2021, 26, 1580. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, B.; Esmaeilizade, Z.; Omrani, M.D.; Ghaderian, S.M.H.; Rajabibazl, M.; Fazeli, Z. The Effect of Co-Treating Human Mesenchymal Stem Cells with Epigallocatechin Gallate and Hypoxia-Inducible Factor-1 on the Expression of RANKL/RANK/OPG Signaling Pathway, Osteogenesis, and Angiogenesis Genes. Regen. Eng. Transl. Med. 2022, 8, 117–124. [Google Scholar] [CrossRef]
- Komsa-Penkova, R.; Stoycheva, S.; Tonchev, P.; Stavreva, G.; Todinova, S.; Georgieva, G.; Yordanova, A.; Kyurkchiev, S.; Altankov, G. Morphological and Quantitative Evidence for Altered Mesenchymal Stem Cell Remodeling of Collagen in an Oxidative Environment—Peculiar Effect of Epigallocatechin-3-Gallate. Polymers 2022, 14, 3957. [Google Scholar] [CrossRef]
- Song, C.; Xu, S.; Chang, L.; Zhao, X.; Mei, X.; Ren, X.; Chen, Z. Preparation of EGCG Decorated, Injectable Extracellular Vesicles for Cartilage Repair in Rat Arthritis. Regen. Biomater. 2021, 8, rbab067. [Google Scholar] [CrossRef]
- Guo, X.; Ma, Y.; Min, Y.; Sun, J.; Shi, X.; Gao, G.; Sun, L.; Wang, J. Progress and Prospect of Technical and Regulatory Challenges on Tissue-Engineered Cartilage as Therapeutic Combination Product. Bioact. Mater. 2023, 20, 501–518. [Google Scholar] [CrossRef]
- Gambari, L.; Cellamare, A.; Grassi, F.; Grigolo, B.; Panciera, A.; Ruffilli, A.; Faldini, C.; Desando, G. Overview of Anti-Inflammatory and Anti-Nociceptive Effects of Polyphenols to Halt Osteoarthritis: From Preclinical Studies to New Clinical Insights. Int. J. Mol. Sci. 2022, 23, 15861. [Google Scholar] [CrossRef]
- Wei, F.; Lin, K.; Ruan, B.; Wang, C.; Yang, L.; Wang, H.; Wang, Y. Epigallocatechin Gallate Protects MC3T3-E1 Cells from Cadmium-Induced Apoptosis and Dysfunction via Modulating PI3K/AKT/MTOR and Nrf2/HO-1 Pathways. PeerJ 2024, 12, e17488. [Google Scholar] [CrossRef]
- Molnar, V.; Pavelić, E.; Vrdoljak, K.; Čemerin, M.; Klarić, E.; Matišić, V.; Bjelica, R.; Brlek, P.; Kovačić, I.; Tremolada, C.; et al. Mesenchymal Stem Cell Mechanisms of Action and Clinical Effects in Osteoarthritis: A Narrative Review. Genes 2022, 13, 949. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, T.; Ran, C.; Wang, W.; Piao, F.; Yang, J.; Tian, S.; Li, L.; Zhao, D. Immunoregulatory Paracrine Effect of Mesenchymal Stem Cells and Mechanism in the Treatment of Osteoarthritis. Front. Cell Dev. Biol. 2024, 12, 1411507. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.J.; Rim, Y.A.; Nam, Y.; Ju, J.H. Recent Developments in Clinical Applications of Mesenchymal Stem Cells in the Treatment of Rheumatoid Arthritis and Osteoarthritis. Front. Immunol. 2021, 12, 631291. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Wu, W.; Qu, X. Mesenchymal Stem Cells in Osteoarthritis Therapy: A Review. Am. J. Transl. Res. 2021, 13, 448. [Google Scholar] [PubMed]
- Carneiro, D.d.C.; Araújo, L.T.d.; Santos, G.C.; Damasceno, P.K.F.; Vieira, J.L.; Santos, R.R.d.; Barbosa, J.D.V.; Soares, M.B.P. Clinical Trials with Mesenchymal Stem Cell Therapies for Osteoarthritis: Challenges in the Regeneration of Articular Cartilage. Int. J. Mol. Sci. 2023, 24, 9939. [Google Scholar] [CrossRef]
- Jang, S.; Lee, K.; Ju, J.H. Recent Updates of Diagnosis, Pathophysiology, and Treatment on Osteoarthritis of the Knee. Int. J. Mol. Sci. 2021, 22, 2619. [Google Scholar] [CrossRef]
- Zou, Z.; Li, H.; Yu, K.; Ma, K.; Wang, Q.; Tang, J.; Liu, G.; Lim, K.; Hooper, G.; Woodfield, T.; et al. The Potential Role of Synovial Cells in the Progression and Treatment of Osteoarthritis. Exploration 2023, 3, 20220132. [Google Scholar] [CrossRef]
- Xia, C.; Dai, Z.; Jin, Y.; Chen, P. Emerging Antioxidant Paradigm of Mesenchymal Stem Cell-Derived Exosome Therapy. Front. Endocrinol 2021, 12, 727272. [Google Scholar] [CrossRef]
- Miceli, V.; Bulati, M.; Iannolo, G.; Zito, G.; Gallo, A.; Conaldi, P.G. Therapeutic Properties of Mesenchymal Stromal/Stem Cells: The Need of Cell Priming for Cell-Free Therapies in Regenerative Medicine. Int. J. Mol. Sci. 2021, 22, 763. [Google Scholar] [CrossRef]
- Aixirefu, A.; Chen, R.; Wang, H. Clinical Efficacy of Mesenchymal Stem Cells and Platelet-Rich Plasma in the Therapy of Osteoarthritis: A Meta-Analysis. Am. J. Transl. Res. 2024, 16, 4256. [Google Scholar] [CrossRef]
- Chalidis, B.; Givissis, P.; Papadopoulos, P.; Pitsilos, C. Molecular and Biologic Effects of Platelet-Rich Plasma (PRP) in Ligament and Tendon Healing and Regeneration: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 2744. [Google Scholar] [CrossRef]
- Popescu, M.N.; Iliescu, M.G.; Beiu, C.; Popa, L.G.; Mihai, M.M.; Berteanu, M.; Ionescu, A.M. Autologous Platelet-Rich Plasma Efficacy in the Field of Regenerative Medicine: Product and Quality Control. Biomed. Res. Int. 2021, 2021, 4672959. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Troya, M.; Tierno, R.; Zalduendo, M.; Alkhraisat, M.H. The Effectiveness of Platelet-Rich Plasma as a Carrier of Stem Cells in Tissue Regeneration: A Systematic Review of Pre-Clinical Research. Cells Tissues Organs 2021, 210, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Copp, G.; Robb, K.P.; Viswanathan, S. Culture-Expanded Mesenchymal Stromal Cell Therapy: Does It Work in Knee Osteoarthritis? A Pathway to Clinical Success. Cell Mol. Immunol. 2023, 20, 626–650. [Google Scholar] [CrossRef] [PubMed]
- Calcat-i-Cervera, S.; Sanz-Nogués, C.; O’Brien, T. When Origin Matters: Properties of Mesenchymal Stromal Cells From Different Sources for Clinical Translation in Kidney Disease. Front. Med. 2021, 8, 728496. [Google Scholar] [CrossRef]
- Wilson, A.J.; Brown, N.; Rand, E.; Genever, P.G. Attitudes Towards Standardization of Mesenchymal Stromal Cells—A Qualitative Exploration of Expert Views. Stem Cells Transl. Med. 2023, 12, 745–757. [Google Scholar] [CrossRef]
- Fountzilas, E.; Tsimberidou, A.M.; Vo, H.H.; Kurzrock, R. Clinical Trial Design in the Era of Precision Medicine. Genome Med. 2022, 14, 101. [Google Scholar] [CrossRef]
- Mahmoudian, A.; Lohmander, L.S.; Mobasheri, A.; Englund, M.; Luyten, F.P. Early-Stage Symptomatic Osteoarthritis of the Knee—Time for Action. Nat. Rev. Rheumatol. 2021, 17, 621–632. [Google Scholar] [CrossRef]
- Gerami, M.H.; Khorram, R.; Rasoolzadegan, S.; Mardpour, S.; Nakhaei, P.; Hashemi, S.; Al-Naqeeb, B.Z.T.; Aminian, A.; Samimi, S. Emerging Role of Mesenchymal Stem/Stromal Cells (MSCs) and MSCs-Derived Exosomes in Bone- and Joint-Associated Musculoskeletal Disorders: A New Frontier. Eur. J. Med. Res. 2023, 28, 86. [Google Scholar] [CrossRef]
- Zhang, Z.; Yang, X.; Cao, X.; Qin, A.; Zhao, J. Current Applications of Adipose-Derived Mesenchymal Stem Cells in Bone Repair and Regeneration: A Review of Cell Experiments, Animal Models, and Clinical Trials. Front. Bioeng. Biotechnol. 2022, 10, 942128. [Google Scholar] [CrossRef]
- Ivanovski, S.; Han, P.; Peters, O.A.; Sanz, M.; Bartold, P.M. The Therapeutic Use of Dental Mesenchymal Stem Cells in Human Clinical Trials. J. Dent. Res. 2024, 103, 1173–1184. [Google Scholar] [CrossRef]
- Nasim, N.; Sandeep, I.S.; Mohanty, S. Plant-Derived Natural Products for Drug Discovery: Current Approaches and Prospects. Nucleus 2022, 65, 399–411. [Google Scholar] [CrossRef] [PubMed]
- Yuan, D.; Guo, Y.; Pu, F.; Yang, C.; Xiao, X.; Du, H.; He, J.; Lu, S. Opportunities and Challenges in Enhancing the Bioavailability and Bioactivity of Dietary Flavonoids: A Novel Delivery System Perspective. Food Chem. 2024, 430, 137115. [Google Scholar] [CrossRef] [PubMed]
- Manzari, M.T.; Shamay, Y.; Kiguchi, H.; Rosen, N.; Scaltriti, M.; Heller, D.A. Targeted Drug Delivery Strategies for Precision Medicines. Nat. Rev. Mater. 2021, 6, 351–370. [Google Scholar] [CrossRef] [PubMed]
- Alam, S.; Sarker, M.M.R.; Afrin, S.; Richi, F.T.; Zhao, C.; Zhou, J.R.; Mohamed, I.N. Traditional Herbal Medicines, Bioactive Metabolites, and Plant Products Against COVID-19: Update on Clinical Trials and Mechanism of Actions. Front. Pharmacol. 2021, 12, 671498. [Google Scholar] [CrossRef]
- Maleitzke, T.; Hildebrandt, A.; Dietrich, T.; Appelt, J.; Jahn, D.; Otto, E.; Zocholl, D.; Baranowsky, A.; Duda, G.N.; Tsitsilonis, S.; et al. The Calcitonin Receptor Protects against Bone Loss and Excessive Inflammation in Collagen Antibody-Induced Arthritis. iScience 2022, 25, 103689. [Google Scholar] [CrossRef]
- Li, W.; Sun, K.; Hu, F.; Chen, L.; Zhang, X.; Wang, F.; Yan, B. Protective Effects of Natural Compounds against Oxidative Stress in Ischemic Diseases and Cancers via Activating the Nrf2 Signaling Pathway: A Mini Review. J. Biochem. Mol. Toxicol. 2021, 35, e22658. [Google Scholar] [CrossRef]
- Zhang, Q.; Liu, J.; Duan, H.; Li, R.; Peng, W.; Wu, C. Activation of Nrf2/HO-1 Signaling: An Important Molecular Mechanism of Herbal Medicine in the Treatment of Atherosclerosis via the Protection of Vascular Endothelial Cells from Oxidative Stress. J. Adv. Res. 2021, 34, 43–63. [Google Scholar] [CrossRef]
- Thiruvengadam, M.; Venkidasamy, B.; Subramanian, U.; Samynathan, R.; Shariati, M.A.; Rebezov, M.; Girish, S.; Thangavel, S.; Dhanapal, A.R.; Fedoseeva, N.; et al. Bioactive Compounds in Oxidative Stress-Mediated Diseases: Targeting the Nrf2/Are Signaling Pathway and Epigenetic Regulation. Antioxidants 2021, 10, 1859. [Google Scholar] [CrossRef]
- Zhang, M.J.; Sun, W.W.; Yang, J.; Shi, D.D.; Dai, X.F.; Li, X.M. The Effect of Preventing Oxidative Stress and Its Mechanisms in the Extract from Sonchus Brachyotus DC. Based on the Nrf2-Keap1-ARE Signaling Pathway. Antioxidants 2023, 12, 1677. [Google Scholar] [CrossRef]
- Scuto, M.; Trovato Salinaro, A.; Caligiuri, I.; Ontario, M.L.; Greco, V.; Sciuto, N.; Crea, R.; Calabrese, E.J.; Rizzolio, F.; Canzonieri, V.; et al. Redox Modulation of Vitagenes via Plant Polyphenols and Vitamin D: Novel Insights for Chemoprevention and Therapeutic Interventions Based on Organoid Technology. Mech. Ageing Dev. 2021, 199, 111551. [Google Scholar] [CrossRef]
- Machado, I.F.; Miranda, R.G.; Dorta, D.J.; Rolo, A.P.; Palmeira, C.M. Targeting Oxidative Stress with Polyphenols to Fight Liver Diseases. Antioxidants 2023, 12, 1212. [Google Scholar] [CrossRef] [PubMed]
- Di Giacomo, C.; Malfa, G.A.; Tomasello, B.; Bianchi, S.; Acquaviva, R. Natural Compounds and Glutathione: Beyond Mere Antioxidants. Antioxidants 2023, 12, 1445. [Google Scholar] [CrossRef] [PubMed]
- Tudino, V.; Ibba, R.; Carullo, G.; Artamonov, M.Y.; Pyatakovich, F.A.; Minenko, I.A. Synergistic Antioxidant Effects of Molecular Hydrogen and Cold Atmospheric Plasma in Enhancing Mesenchymal Stem Cell Therapy. Antioxidants 2024, 13, 1584. [Google Scholar] [CrossRef] [PubMed]
- Mateu-Sanz, M.; Tornín, J.; Ginebra, M.P.; Canal, C. Cold Atmospheric Plasma: A New Strategy Based Primarily on Oxidative Stress for Osteosarcoma Therapy. J. Clin. Med. 2021, 10, 893. [Google Scholar] [CrossRef]
- Wu, Z.; Yang, Z.; Liu, L.; Xiao, Y. Natural Compounds Protect against the Pathogenesis of Osteoarthritis by Mediating the NRF2/ARE Signaling. Front. Pharmacol. 2023, 14, 1188215. [Google Scholar] [CrossRef]
- Zheng, Z.; Wang, X.; Ouyang, L.; Chen, W.; Zhang, L.; Cao, Y. Antioxidants Improve the Proliferation and Efficacy of HUC-MSCs against H2O2-Induced Senescence. Antioxidants 2023, 12, 1334. [Google Scholar] [CrossRef]
- Hasan, A.A.; Tatarskiy, V.; Kalinina, E. Synthetic Pathways and the Therapeutic Potential of Quercetin and Curcumin. Int. J. Mol. Sci. 2022, 23, 14413. [Google Scholar] [CrossRef]
- Sul, O.J.; Ra, S.W. Quercetin Prevents Lps-induced Oxidative Stress and Inflammation by Modulating Nox2/Ros/Nf-kb in Lung Epithelial Cells. Molecules 2021, 26, 6949. [Google Scholar] [CrossRef]
- Zhang, C.; Weng, Y.; Wang, H.; Zhan, S.; Li, C.; Zheng, D.; Lin, Q. A Synergistic Effect of Triptolide and Curcumin on Rheumatoid Arthritis by Improving Cell Proliferation and Inducing Cell Apoptosis via Inhibition of the IL-17/NF-ΚB Signaling Pathway. Int. Immunopharmacol. 2024, 142, 112953. [Google Scholar] [CrossRef]
- Hong, S.; Dia, V.P.; Zhong, Q. Synergistic Anti-Inflammatory Activity of Apigenin and Curcumin Co-Encapsulated in Caseins Assessed with Lipopolysaccharide-Stimulated RAW 264.7 Macrophages. Int. J. Biol. Macromol. 2021, 193, 702–712. [Google Scholar] [CrossRef]
- Asgharian, P.; Tazekand, A.P.; Hosseini, K.; Forouhandeh, H.; Ghasemnejad, T.; Ranjbar, M.; Hasan, M.; Kumar, M.; Beirami, S.M.; Tarhriz, V.; et al. Potential Mechanisms of Quercetin in Cancer Prevention: Focus on Cellular and Molecular Targets. Cancer Cell Int. 2022, 22, 257. [Google Scholar] [CrossRef] [PubMed]
- Rhman, M.A.; Devnarain, N.; Khan, R.; Owira, P.M.O. Synergism Potentiates Oxidative Antiproliferative Effects of Naringenin and Quercetin in MCF-7 Breast Cancer Cells. Nutrients 2022, 14, 3437. [Google Scholar] [CrossRef] [PubMed]
- Kashyap, A.; Umar, S.M.; Dev J.R., A.; Mendiratta, M.; Prasad, C.P. In Vitro Anticancer Efficacy of a Polyphenolic Combination of Quercetin, Curcumin, and Berberine in Triple Negative Breast Cancer (TNBC) Cells. Phytomedicine Plus 2022, 2, 100265. [Google Scholar] [CrossRef]
- Chittasupho, C.; Manthaisong, A.; Okonogi, S.; Tadtong, S.; Samee, W. Effects of Quercetin and Curcumin Combination on Antibacterial, Antioxidant, In Vitro Wound Healing and Migration of Human Dermal Fibroblast Cells. Int. J. Mol. Sci. 2022, 23, 142. [Google Scholar] [CrossRef]
- Asnaashari, S.; Amjad, E.; Sokouti, B. Synergistic Effects of Flavonoids and Paclitaxel in Cancer Treatment: A Systematic Review. Cancer Cell Int. 2023, 23, 211. [Google Scholar] [CrossRef]
- Krajka-Kuźniak, V.; Baer-Dubowska, W. Modulation of Nrf2 and NF-ΚB Signaling Pathways by Naturally Occurring Compounds in Relation to Cancer Prevention and Therapy. Are Combinations Better than Single Compounds? Int. J. Mol. Sci. 2021, 22, 8223. [Google Scholar] [CrossRef]
- Jena, A.B.; Dash, U.C.; Duttaroy, A.K. An in Silico Investigation on the Interactions of Curcumin and Epigallocatechin-3-Gallate with NLRP3 Inflammasome Complex. Biomed. Pharmacother. 2022, 156, 113890. [Google Scholar] [CrossRef]
- Supriyadi, R.; Koswara, M.I.A.; Soelaeman, M.A.; Huang, I. The Effect of Antioxidants Supplementation on Oxidative Stress and Proinflammatory Biomarkers in Patients with Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 1413–1426. [Google Scholar] [CrossRef]
- Li, J.; Zhao, P.; Tian, Y.; Li, K.; Zhang, L.; Guan, Q.; Mei, X.; Qin, Y. The Anti-Inflammatory Effect of a Combination of Five Compounds From Five Chinese Herbal Medicines Used in the Treatment of COPD. Front. Pharmacol. 2021, 12, 709702. [Google Scholar] [CrossRef]
- Tang, H.; Hosein, A.; Mattioli-Belmonte, M. Traditional Chinese Medicine and Orthopedic Biomaterials: Host of Opportunities from Herbal Extracts. Mater. Sci. Eng. C 2021, 120, 111760. [Google Scholar] [CrossRef]
- Kciuk, M.; Garg, A.; Rohilla, M.; Chaudhary, R.; Dhankhar, S.; Dhiman, S.; Bansal, S.; Saini, M.; Singh, T.G.; Chauhan, S.; et al. Therapeutic Potential of Plant-Derived Compounds and Plant Extracts in Rheumatoid Arthritis—Comprehensive Review. Antioxidants 2024, 13, 775. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Lu, J.J.; Ding, J. Natural Products in Cancer Therapy: Past, Present and Future. Nat. Prod. Bioprospect 2021, 11, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wan, H.; Tong, X.; He, Y.; Yang, J.; Zhang, L.; Shao, C.; Ding, Z.; Wan, H.; Li, C. An Integrative Strategy for Discovery of Functional Compound Combination from Traditional Chinese Medicine: Danhong Injection as a Model. Biomed. Pharmacother. 2021, 138, 111451. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wu, R.; Yu, H.; Zheng, Q.; Chen, Y. Bioactive Herbal Extracts of Traditional Chinese Medicine Applied with the Biomaterials: For the Current Applications and Advances in the Musculoskeletal System. Front. Pharmacol. 2021, 12, 778041. [Google Scholar] [CrossRef]
- Zhang, Y.; Lou, Y.; Wang, J.; Yu, C.; Shen, W. Research Status and Molecular Mechanism of the Traditional Chinese Medicine and Antitumor Therapy Combined Strategy Based on Tumor Microenvironment. Front. Immunol. 2021, 11, 609705. [Google Scholar] [CrossRef]
- Matuszewska, K.; Pereira, M.; Petrik, D.; Lawler, J.; Petrik, J. Normalizing Tumor Vasculature to Reduce Hypoxia, Enhance Perfusion, and Optimize Therapy Uptake. Cancers 2021, 13, 4444. [Google Scholar] [CrossRef]
- Deng, S.; Cao, H.; Cui, X.; Fan, Y.; Wang, Q.; Zhang, X. Optimization of Exosome-Based Cell-Free Strategies to Enhance Endogenous Cell Functions in Tissue Regeneration. Acta Biomater. 2023, 171, 68–84. [Google Scholar] [CrossRef]
- Wang, Y.; Wen, J.; Lu, T.; Han, W.; Jiao, K.; Li, H. Mesenchymal Stem Cell-Derived Extracellular Vesicles in Bone-Related Diseases: Intercellular Communication Messengers and Therapeutic Engineering Protagonists. Int. J. Nanomedicine 2024, 19, 3233–3257. [Google Scholar] [CrossRef]
- Chu, C.H.; Lee, R.P.; Wu, W.T.; Chen, I.H.; Yeh, K.T.; Wang, C.C. Advancing Osteoarthritis Treatment: The Therapeutic Potential of Mesenchymal Stem Cell-Derived Exosomes and Biomaterial Integration. Biomedicines 2024, 12, 2478. [Google Scholar] [CrossRef]
- Cheng, J.; Sun, Y.; Ma, Y.; Ao, Y.; Hu, X.; Meng, Q. Engineering of MSC-Derived Exosomes: A Promising Cell-Free Therapy for Osteoarthritis. Membranes 2022, 12, 739. [Google Scholar] [CrossRef]
- Kumari, S.; Goyal, A.; Gürer, E.S.; Yapar, E.A.; Garg, M.; Sood, M.; Sindhu, R.K. Bioactive Loaded Novel Nano-Formulations for Targeted Drug Delivery and Their Therapeutic Potential. Pharmaceutics 2022, 14, 1091. [Google Scholar] [CrossRef] [PubMed]
- Sampath, S.J.P.; Rath, S.N.; Kotikalapudi, N.; Venkatesan, V. Beneficial Effects of Secretome Derived from Mesenchymal Stem Cells with Stigmasterol to Negate IL-1β-Induced Inflammation in-Vitro Using Rat Chondrocytes—OA Management. Inflammopharmacology 2021, 29, 1701–1717. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.A.; Khalifa, A.M.; Mohamed, A.A.; Galhom, R.A.; Korayem, H.E.; Abd El-Fadeal, N.M.; Abd-Eltawab Tammam, A.; Khalifa, M.M.; Elserafy, O.S.; Abdel-Karim, R.I. Bone-Marrow-Derived Mesenchymal Stem Cells, Their Conditioned Media, and Olive Leaf Extract Protect against Cisplatin-Induced Toxicity by Alleviating Oxidative Stress, Inflammation, and Apoptosis in Rats. Toxics 2022, 10, 526. [Google Scholar] [CrossRef] [PubMed]
- Jiang, E.; Chen, X.; Bi, Y.; Pan, C.; Li, X.; Lan, X. Curcumin Inhibits Oxidative Stress and Apoptosis Induced by H2O2 in Bovine Adipose-Derived Stem Cells (BADSCs). Animals 2024, 14, 3421. [Google Scholar] [CrossRef]
- Gopalakrishna, R.; Oh, A.; Hou, L.; Lee, E.; Aguilar, J.; Li, A.; Mack, W.J. Flavonoid Quercetin and Its Glucuronide and Sulfate Conjugates Bind to 67-KDa Laminin Receptor and Prevent Neuronal Cell Death Induced by Serum Starvation. Biochem. Biophys. Res. Commun. 2023, 671, 116–123. [Google Scholar] [CrossRef]
- Liu, H.; Guan, H.; He, F.; Song, Y.; Li, F.; Sun-Waterhouse, D.; Li, D. Therapeutic Actions of Tea Phenolic Compounds against Oxidative Stress and Inflammation as Central Mediators in the Development and Progression of Health Problems: A Review Focusing on MicroRNA Regulation. Crit. Rev. Food Sci. Nutr. 2024, 64, 8414–8444. [Google Scholar] [CrossRef]
- Jomova, K.; Raptova, R.; Alomar, S.Y.; Alwasel, S.H.; Nepovimova, E.; Kuca, K.; Valko, M. Reactive Oxygen Species, Toxicity, Oxidative Stress, and Antioxidants: Chronic Diseases and Aging. Arch. Toxicol. 2023, 97, 2499. [Google Scholar]
- Al-Azab, M.; Idiiatullina, E.; Safi, M.; Hezam, K. Enhancers of Mesenchymal Stem Cell Stemness and Therapeutic Potency. Biomed. Pharmacother. 2023, 162, 114356. [Google Scholar] [CrossRef]
- Zhang, K.; Du, X.; Gao, Y.; Liu, S.; Xu, Y. Mesenchymal Stem Cells for Treating Alzheimer’s Disease: Cell Therapy and Chemical Reagent Pretreatment. J. Alzheimers Dis. 2023, 93, 863–878. [Google Scholar] [CrossRef]
- Zhou, F.; Peterson, T.; Fan, Z.; Wang, S. The Commonly Used Stabilizers for Phytochemical-Based Nanoparticles: Stabilization Effects, Mechanisms, and Applications. Nutrients 2023, 15, 3881. [Google Scholar] [CrossRef]
- Salla, M.; Karaki, N.; El Kaderi, B.; Ayoub, A.J.; Younes, S.; Abou Chahla, M.N.; Baksh, S.; El Khatib, S. Enhancing the Bioavailability of Resveratrol: Combine It, Derivatize It, or Encapsulate It? Pharmaceutics 2024, 16, 569. [Google Scholar] [CrossRef] [PubMed]
- Hashemzadeh, H.; Hanafi-Bojd, M.Y.; Iranshahy, M.; Zarban, A.; Raissi, H. The Combination of Polyphenols and Phospholipids as an Efficient Platform for Delivery of Natural Products. Sci. Rep. 2023, 13, 2501. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Lv, Y.; Li, X.; Bao, H.; Cao, X.; Huang, J.; Zhang, Z. SOD-Functionalized Gold Nanoparticles as ROS Scavenger and CT Contrast Agent for Protection and Imaging Tracking of Mesenchymal Stem Cells in Idiopathic Pulmonary Fibrosis Treatment. Chem. Eng. J. 2023, 459, 141603. [Google Scholar] [CrossRef]
- Wu, S.; Zhou, Z.; Li, Y.; Wu, R.; Jiang, J. Pretreatment of Human Umbilical Cord Mesenchymal Stem Cell-Derived Exosomes with Quercetin Enhances the Healing of Diabetic Skin Wounds by Modulating Host-Microbiota Interactions. Int. J. Nanomedicine 2024, 19, 12557–12581. [Google Scholar] [CrossRef] [PubMed]
- Zawani, M.; Fauzi, M.B. Epigallocatechin Gallate: The Emerging Wound Healing Potential of Multifunctional Biomaterials for Future Precision Medicine Treatment Strategies. Polymers 2021, 13, 3656. [Google Scholar] [CrossRef]
- Chaudhuri, R.; Samanta, A.; Saha, P.; Ghosh, S.; Sinha, D. The Potential of Epigallocatechin Gallate in Targeting Cancer Stem Cells: A Comprehensive Review. Curr. Med. Chem. 2024, 31, 5255–5280. [Google Scholar] [CrossRef]
- Moudgil, K.D.; Venkatesha, S.H. The Anti-Inflammatory and Immunomodulatory Activities of Natural Products to Control Autoimmune Inflammation. Int. J. Mol. Sci. 2023, 24, 95. [Google Scholar] [CrossRef]
- Las Heras, K.; Garcia-Orue, I.; Rancan, F.; Igartua, M.; Santos-Vizcaino, E.; Hernandez, R.M. Modulating the Immune System towards a Functional Chronic Wound Healing: A Biomaterials and Nanomedicine Perspective. Adv. Drug Deliv. Rev. 2024, 210, 115342. [Google Scholar] [CrossRef]
- Fernandes, A.; Rodrigues, P.M.; Pintado, M.; Tavaria, F.K. A Systematic Review of Natural Products for Skin Applications: Targeting Inflammation, Wound Healing, and Photo-Aging. Phytomedicine 2023, 115, 154824. [Google Scholar] [CrossRef]
- Li, P.; Ou, Q.; Shi, S.; Shao, C. Immunomodulatory Properties of Mesenchymal Stem Cells/Dental Stem Cells and Their Therapeutic Applications. Cell Mol. Immunol. 2023, 20, 558–569. [Google Scholar] [CrossRef]
- Kou, M.; Huang, L.; Yang, J.; Chiang, Z.; Chen, S.; Liu, J.; Guo, L.; Zhang, X.; Zhou, X.; Xu, X.; et al. Mesenchymal Stem Cell-Derived Extracellular Vesicles for Immunomodulation and Regeneration: A next Generation Therapeutic Tool? Cell Death Dis. 2022, 13, 580. [Google Scholar] [CrossRef] [PubMed]
- Hristova-Panusheva, K.; Xenodochidis, C.; Georgieva, M.; Krasteva, N. Nanoparticle-Mediated Drug Delivery Systems for Precision Targeting in Oncology. Pharmaceuticals 2024, 17, 677. [Google Scholar] [CrossRef] [PubMed]
- Swami, P.N.; Andriamifidy, H.F.; Haque, S.; Reed, T.; Khan, A.; Grande, D.A. Exosomes from the Synovial Microenvironment in Joint Homeostasis and Osteoarthritis. J. Cartil. Jt. Preserv. 2024, 4, 100220. [Google Scholar] [CrossRef]
- Wu, Y.; Li, J.; Zeng, Y.; Pu, W.; Mu, X.; Sun, K.; Peng, Y.; Shen, B. Exosomes Rewire the Cartilage Microenvironment in Osteoarthritis: From Intercellular Communication to Therapeutic Strategies. Int. J. Oral. Sci. 2022, 14, 40. [Google Scholar] [CrossRef]
- An, X.; Wang, J.; Xu, K.; Zhao, R.C.; Su, J. Perspectives on Osteoarthritis Treatment with Mesenchymal Stem Cells and Radix Achyranthis Bidentatae. Aging Dis. 2024, 15, 1029–1045. [Google Scholar]
- Arifka, M.; Wilar, G.; Elamin, K.M.; Wathoni, N. Polymeric Hydrogels as Mesenchymal Stem Cell Secretome Delivery System in Biomedical Applications. Polymers 2022, 14, 1218. [Google Scholar] [CrossRef]
- Li, Z.; Liu, J.; Song, J.; Yin, Z.; Zhou, F.; Shen, H.; Wang, G.; Su, J. Multifunctional Hydrogel-Based Engineered Extracellular Vesicles Delivery for Complicated Wound Healing. Theranostics 2024, 14, 4198–4217. [Google Scholar] [CrossRef]
- Heo, S.; Noh, M.; Kim, Y.; Park, S. Stem Cell-Laden Engineered Patch: Advances and Applications in Tissue Regeneration. ACS Appl. Bio Mater. 2025, 8, 62–87. [Google Scholar] [CrossRef]
- Adepu, S.; Ramakrishna, S. Controlled Drug Delivery Systems: Current Status and Future Directions. Molecules 2021, 26, 5905. [Google Scholar] [CrossRef]
- Liang, J.; Liu, P.; Yang, X.; Liu, L.; Zhang, Y.; Wang, Q.; Zhao, H. Biomaterial-Based Scaffolds in Promotion of Cartilage Regeneration: Recent Advances and Emerging Applications. J. Orthop. Transl. 2023, 41, 54–62. [Google Scholar] [CrossRef]
- Ma, M.; Zou, F.; Abudureheman, B.; Han, F.; Xu, G.; Xie, Y.J.; Qiao, K.; Peng, J.; Guan, Y.; Meng, H.; et al. Magnetic Microcarriers with Accurate Localization and Proliferation of Mesenchymal Stem Cell for Cartilage Defects Repairing. ACS Nano 2023, 17, 6373–6386. [Google Scholar] [CrossRef] [PubMed]
- Rohila, A.; Shukla, R. Recent Advancements in Microspheres Mediated Targeted Delivery for Therapeutic Interventions in Osteoarthritis. J. Microencapsul. 2024, 41, 434–455. [Google Scholar] [CrossRef] [PubMed]
- Bao, C.; He, C. The Role and Therapeutic Potential of MSC-Derived Exosomes in Osteoarthritis. Arch. Biochem. Biophys. 2021, 710, 109002. [Google Scholar] [CrossRef]
- Kim, K.I.I.; Lee, M.C.; Lee, J.H.; Moon, Y.W.; Lee, W.S.; Lee, H.J.; Hwang, S.C.; In, Y.; Shon, O.J.; Bae, K.C.; et al. Clinical Efficacy and Safety of the Intra-Articular Injection of Autologous Adipose-Derived Mesenchymal Stem Cells for Knee Osteoarthritis: A Phase III, Randomized, Double-Blind, Placebo-Controlled Trial. Am. J. Sports Med. 2023, 51, 2243–2253. [Google Scholar] [CrossRef] [PubMed]
- Freitag, J.; Chamberlain, M.; Wickham, J.; Shah, K.; Cicuttini, F.; Wang, Y.; Solterbeck, A.; Kenihan, L.; Kelly, L.A.; Castelluccio, R.; et al. Safety and Efficacy of an Allogeneic Adipose-Derived Mesenchymal Stem Cell Preparation in the Treatment of Knee Osteoarthritis: A Phase I/IIa Randomised Controlled Trial. Osteoarthr. Cartil. Open 2024, 6, 100500. [Google Scholar] [CrossRef]
- Vizoso, F.J.; Costa, L.A.; Eiro, N. New Era of Mesenchymal Stem Cell-Based Medicine: Basis, Challenges and Prospects. Rev. Clínica Española 2023, 223, 619–628. [Google Scholar] [CrossRef]
- Galderisi, U.; Peluso, G.; Di Bernardo, G. Clinical Trials Based on Mesenchymal Stromal Cells Are Exponentially Increasing: Where Are We in Recent Years? Stem Cell Rev. Rep. 2022, 18, 23–36. [Google Scholar] [CrossRef]
- Joshi, S.; Allabun, S.; Ojo, S.; Alqahtani, M.S.; Shukla, P.K.; Abbas, M.; Wechtaisong, C.; Almohiy, H.M. Enhanced Drug Delivery System Using Mesenchymal Stem Cells and Membrane-Coated Nanoparticles. Molecules 2023, 28, 2130. [Google Scholar] [CrossRef]
- Ghazal, M.M.; Zakiyyah, Z.M.M.; Ahmad Mohd Zain, M.R.; Ismail, S. A Narrative Review on Advances in Knee Osteoarthritis Treatment: Current Status and Emerging Trends. Niger. Health J. 2019, 25, 16–30. [Google Scholar] [CrossRef]
- Freitag, J.; Bates, D.; Wickham , J.; Shah, K.; Huguenin , L.; Tenen , A. Adipose-Derived Mesenchymal Stem Cell Therapy in the Treatment of Knee Osteoarthritis: A Randomized Controlled Trial. Regenerative Med. 2019, 14, 213–230. [Google Scholar] [CrossRef]

| Treatment Category | Specific Treatments | Description | Effects |
|---|---|---|---|
| Non-Pharmacological | Regular physical activity | Promotes mobility and joint function | Aids weight reduction and overall health improvement |
| Lifestyle modifications | Diet and other health-related changes | Critical for patients with obesity or poor nutrition | |
| Weight management | Lifestyle changes, including diet and exercise | Reduces joint stress and improves overall health | |
| Physical therapy | Exercises to improve joint mobility and muscle strength | Alleviates pain and enhances functional capacity | |
| Pharmacological | Glucosamine and chondroitin | Supplements for cartilage health | Clinical results are inconsistent; generally not recommended |
| Steroid injections | Corticosteroid injections for acute pain relief | Short-term pain relief and long-term use should be monitored | |
| Duloxetine | Antidepressant approved for chronic pain in knee OA | Offers better relief in combination therapies compared to NSAIDs alone | |
| Opioids/narcotics | Strong analgesics for severe cases | Effective but associated with addiction and adverse effects | |
| Paracetamol | Analgesic for mild to moderate pain relief | Safe but less effective than NSAIDs | |
| Nonsteroidal anti-inflammatory drugs | Cyclooxygenase inhibitors for pain relief | Effective pain relief but requires caution due to gastrointestinal side effects. | |
| Viscosupplementation | Hyaluronic acid injection for joint lubrication | Offers potential chondroprotective benefits; effectiveness is debated | |
| Surgical | Arthroscopy | Minor surgical adjustment within the joint | Less invasive, but the long-term effectiveness is debated |
| Microfracture surgery | Stimulates growth of new cartilage | Standard due to low cost, it results in less-durable fibrocartilage | |
| Total joint arthroplasty | Full joint replacement surgery | Practical in advanced cases; significant improvements in quality of life | |
| Emerging Treatments | Platelet-rich plasma (PRP) | Concentrated platelets for tissue regeneration | Aids in inflammatory response modulation |
| Gene therapy | Introducing therapeutic genes directly to the joint | Potential for long-term effects and slowing degenerative processes | |
| Small molecule inhibitors | Target specific pathways of joint inflammation | Promising disease modification and symptomatic relief | |
| Stem cell therapy | Mesenchymal stem cells for tissue regeneration | Potentially modulates inflammation and promotes regeneration |
| Authors & Year | Study Type | Natural Product | MSC Source | Main Findings | Limitations |
|---|---|---|---|---|---|
| [67] | In vitro | Curcumin Dosage: 500–2000 mg/day; frequency: daily, divided doses | Bone marrow MSCs | Enhances chondrogenic differentiation and reduces oxidative stress | Lacks in vivo validation |
| [68] | Animal (OA model) | ResveratrolDosage: 150–500 mg/day (up to 1000 mg); frequency: once daily or divided doses | Adipose-derived MSCs | Reduces cartilage degradation and inflammation | No human trial evidence |
| [69] | Clinical trial | Resveratrol Dosage: 150–500 mg/day (up to 1000 mg); frequency: once daily or divided doses | Bone marrow MSCs | Improved pain and function in knee OA patients | Small sample size (n = 30) |
| [70] | In vitro | Quercetin Dosage: 500–1000 mg/day; frequency: divided doses | Umbilical cord MSCs | Anti-inflammatory effects, reduces MMP expression | No long-term study |
| [71] | In vivo (rat model) | EGCG Dosage: 400–800 mg/day; frequency: once or twice daily | Bone marrow MSCs | Protects cartilage from inflammatory damage | Bioavailability concerns |
| [72] | In vivo (mouse model) | Resveratrol Dosage: 40 mg/kg/day; once daily, 4 weeks. s | Bone marroe MSCs | Enhances osteogenic differentiation by activating SIRT1 | No in vivo data |
| [73] | In vitro | Quercetin Dosage: 500–1000 mg/day; frequency: divided doses | Bone marrow MSCs | Modulates macrophage polarization, reduces inflammatory cytokines | Needs validation in animal models |
| [63] | In vivo (OA model) | EGCG Dosage: 400–800 mg/day; frequency: once or twice daily | Bone marrow MSCs | Protects MSCs from apoptosis and oxidative stress | No clinical translation yet |
| [74] | In vitro and in vivo | Curcumin + resveratrol (no information) | Bone marrow MSCs | Synergistic effect in reducing TNF-α-induced inflammation | Dosage standardization needed |
| [56] | In vitro | Quercetin + EGCG (no information) | Bone marrow MSCs | Enhances MSC survival under oxidative stress | No human trial conducted |
| [52] | Animal (OA model) | Curcumin-loaded nanoparticles Dosage: 10.32% drug loading; frequency: sustained release over 10 days | Bone marrow MSCs | Improves MSC retention and differentiation in OA joints | Requires more safety studies for clinical use |
| [75] | In vivo (OA model) | EGCG-loaded hydrogelsDosage: 10 mg/kg; frequency: sustained release | Adipose-derived MSCs | Increases MSC viability and cartilage regeneration | Lacks clinical trial data |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfaqeh, H.H.; Idrus, R.B.H.; Saim, A.B.; Nordin, A. Synergistic Effects of Natural Products and Mesenchymal Stem Cells in Osteoarthritis Treatment: A Narrative Review. Curr. Issues Mol. Biol. 2025, 47, 445. https://doi.org/10.3390/cimb47060445
Alfaqeh HH, Idrus RBH, Saim AB, Nordin A. Synergistic Effects of Natural Products and Mesenchymal Stem Cells in Osteoarthritis Treatment: A Narrative Review. Current Issues in Molecular Biology. 2025; 47(6):445. https://doi.org/10.3390/cimb47060445
Chicago/Turabian StyleAlfaqeh, Hamoud H., Ruszymah Binti Hj Idrus, Aminuddin Bin Saim, and Abid Nordin. 2025. "Synergistic Effects of Natural Products and Mesenchymal Stem Cells in Osteoarthritis Treatment: A Narrative Review" Current Issues in Molecular Biology 47, no. 6: 445. https://doi.org/10.3390/cimb47060445
APA StyleAlfaqeh, H. H., Idrus, R. B. H., Saim, A. B., & Nordin, A. (2025). Synergistic Effects of Natural Products and Mesenchymal Stem Cells in Osteoarthritis Treatment: A Narrative Review. Current Issues in Molecular Biology, 47(6), 445. https://doi.org/10.3390/cimb47060445