


A Clinical Case of Multisystem Inflammatory Syndrome After SARS-CoV-2 Infection Associated with Group A β-Hemolytic Streptococcus Coinfection and Venous Thrombosis in a Child with Congenital Thrombophilia


 ,
,
Abstract
1. Introduction
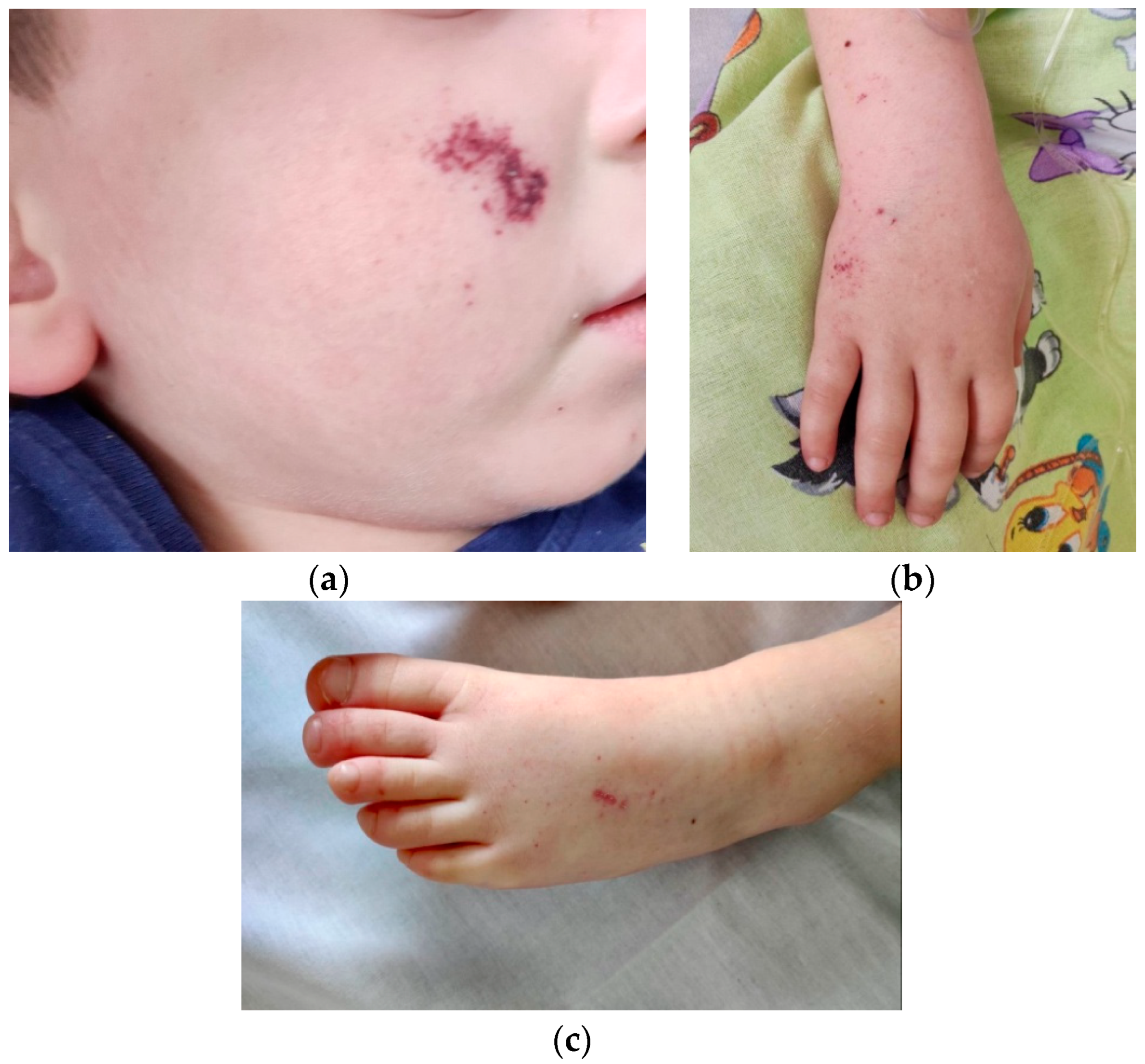
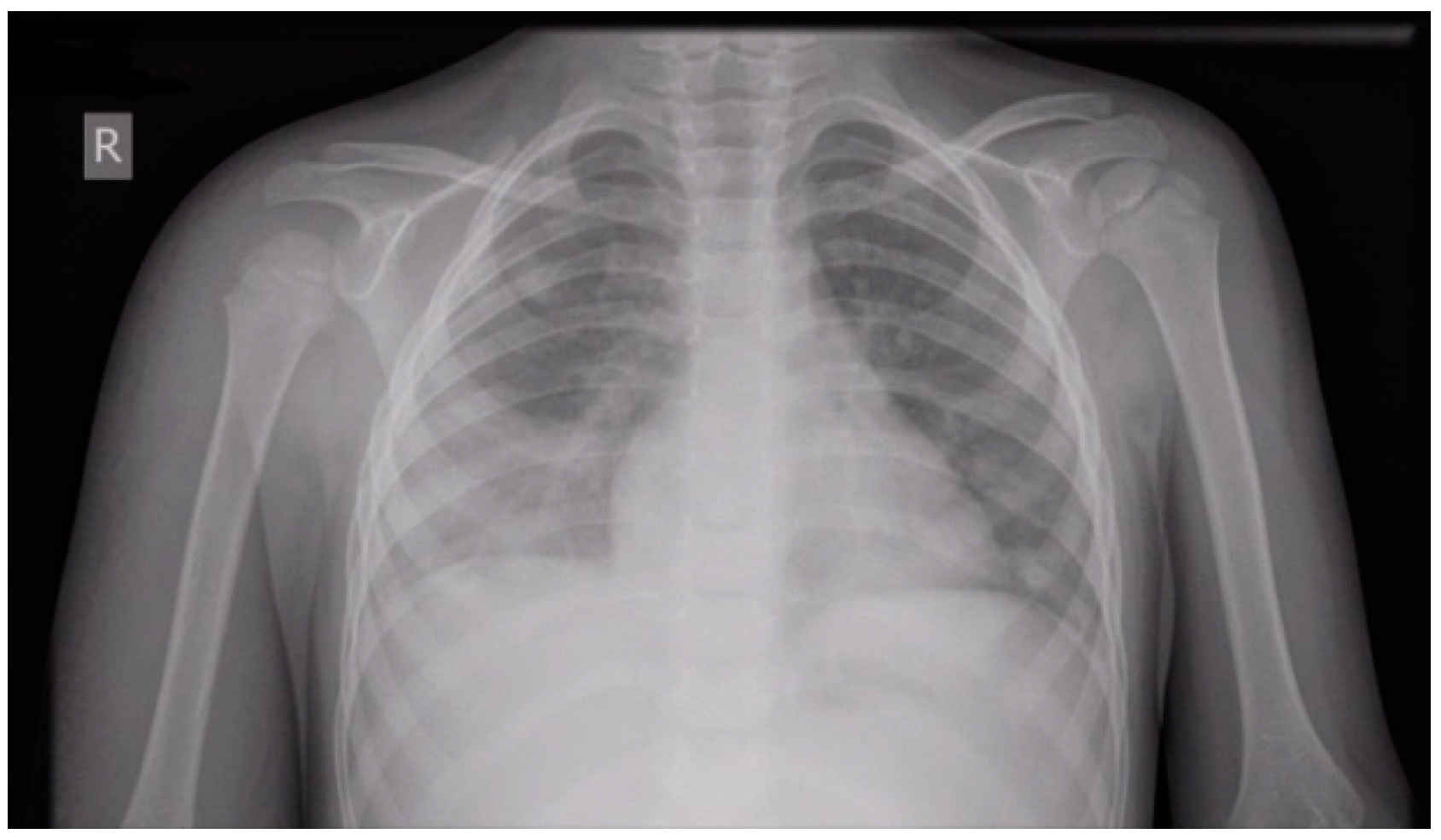
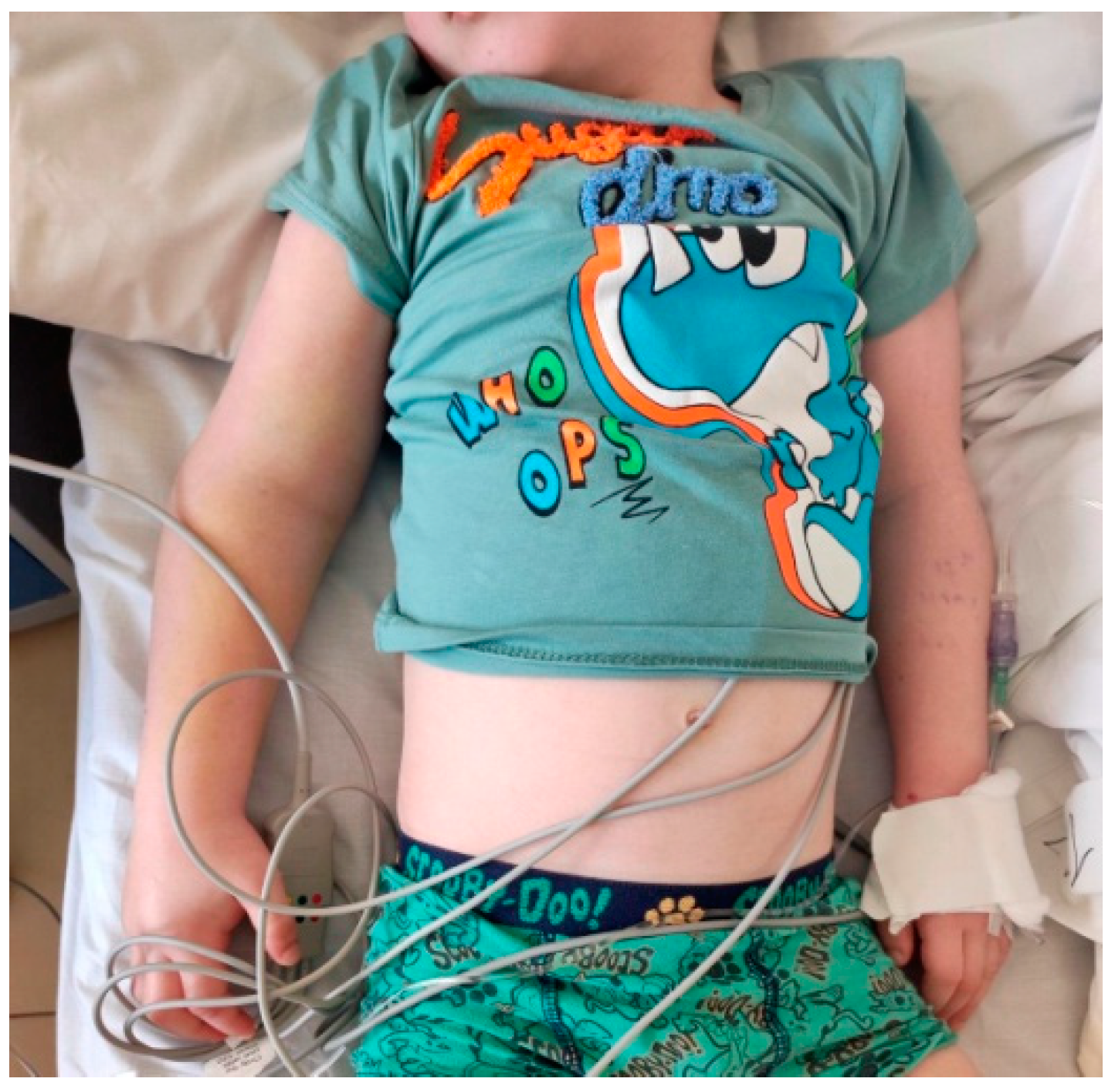
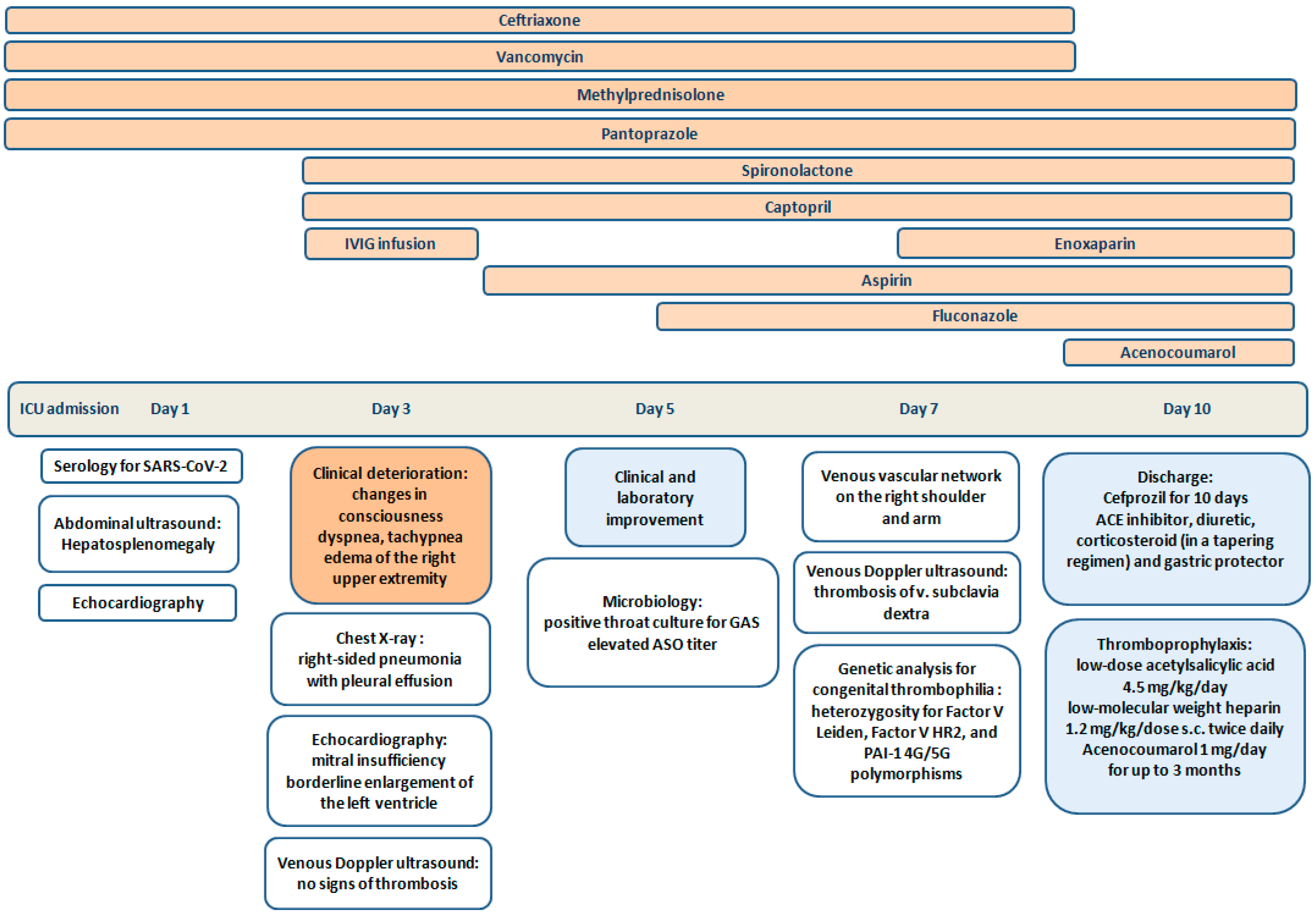
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Multisystem Inflammatory Syndrome in Children and Adolescents with COVID-19 Scientific Brief 15 May 2020 Background [Internet]. 2020. Available online: https://www.who.int/publications/i/item/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (accessed on 1 September 2022).
- Porritt, R.A.; Binek, A.; Paschold, L.; Rivas, M.N.; McArdle, A.; Yonker, L.M.; Alter, G.; Chandnani, H.K.; Lopez, M.; Fasano, A.; et al. The autoimmune signature of hyperinflammatory multisystem inflammatory syndrome in children. J. Clin. Investig. 2021, 131, e151520. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ganeva, M.; Teltcharova, A.; Dimirova, A.; Hristova, D.; Temelkova, K.; Vasilev, T.; Kostova, V.; Stefanov, S. Multisystem inflammatory syndrome in children: A year and a half of experience of University Children’s Hospital, Sofia, Bulgaria, PReS2022-ABS-1262. In Proceedings of the 28th European Paediatric Rheumatology Congress (PReS 2022), Prague, Czech Republic, 20–23 September 2022. [Google Scholar]
- CDC COVID Data Tracker: Multisystem Inflammatory Syndrome in Children (MIS-C). Available online: https://covid.cdc.gov/covid-data-tracker/#pediatric-data (accessed on 7 December 2023).
- Caorsi, R.; Consolaro, A.; Speziani, C.; Sozeri, B.; Ulu, K.; Faugier-Fuentes, E.; Menchaca-Aguayo, H.; Ozen, S.; Sener, S.; Rahman, S.A.; et al. The HyperPed-COVID international registry: Impact of age of onset, disease presentation and geographical distribution on the final outcome of MIS-C. J. Autoimmun. 2024, 147, 103265. [Google Scholar] [CrossRef] [PubMed]
- Lassandro, G.; Palmieri, V.V.; Palladino, V.; Amoruso, A.; Faienza, M.F.; Giordano, P. Venous Thromboembolism in Children: From Diagnosis to Management. Int. J. Environ. Res. Public Health 2020, 17, 4993. [Google Scholar] [CrossRef]
- Al-Ghafry, M.; Vagrecha, A.; Malik, M.; Levine, C.; Uster, E.; Aygun, B.; Appiah-Kubi, A.; Vlachos, A.; Capone, C.A.; Rajan, S.; et al. Multisystem Inflammatory Syndrome in Children (MIS-C) and the Prothrombotic State: Coagulation Profiles and Rotational Thromboelastometry in a MIS-C Cohort. J. Thromb. Haemost. 2021, 19, 1764–1770. [Google Scholar] [CrossRef]
- Trapani, S.; Rubino, C.; Lasagni, D.; Pegoraro, F.; Resti, M.; Simonini, G.; Indolfi, G. Thromboembolic complications in children with COVID-19 and MIS-C: A narrative review. Front. Pediatr. 2022, 10, 944743. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, W.S. Preventing Thrombosis in Children with MIS-C. J. Pediatr. 2023, 262, 113766. [Google Scholar] [CrossRef]
- Maniscalco, V.; Niccolai, R.; Marrani, E.; Maccora, I.; Bertini, F.; Pagnini, I.; Simonini, G.; Lasagni, D.; Trapani, S.; Mastrolia, M.V. Thrombotic Events in MIS-C Patients: A Single Case Report and Literature Review. Children 2023, 10, 618. [Google Scholar] [CrossRef]
- Whitworth, H.B.; Sartain, S.E.; Kumar, R.; Armstrong, K.; Ballester, L.; Betensky, M.; Cohen, C.T.; Diaz, R.; Diorio, C.; Goldenberg, N.A.; et al. Rate of thrombosis in children and adolescents hospitalized with COVID-19 or MIS-C. Blood 2021, 138, 190–198. [Google Scholar] [CrossRef] [PubMed]
- McArdle, A.J.; Vito, O.; Patel, H.; Seaby, E.G.; Shah, P.; Wilson, C.; Broderick, C.; Nijman, R.; Tremoulet, A.H.; Munblit, D.; et al. Treatment of Multisystem Inflammatory Syndrome in Children. N. Engl. J. Med. 2021, 385, 11–22. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Channon-Wells, S.; Vito, O.; McArdle, A.J.; Seaby, E.G.; Patel, H.; Shah, P.; Pazukhina, E.; Wilson, C.; Broderick, C.; D’Souza, G.; et al. Immunoglobulin, glucocorticoid, or combination therapy for multisystem inflammatory syndrome in children: A propensity-weighted cohort study. Lancet Rheumatol. 2023, 5, e184–e199. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Henderson, L.A.; Canna, S.W.; Friedman, K.G.; Gorelik, M.; Lapidus, S.K.; Bassiri, H.; Behrens, E.M.; Kernan, K.F.; Schulert, G.S.; Seo, P.; et al. American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 3. Arthritis Rheumatol. 2022, 74, E1–E20. [Google Scholar] [CrossRef] [PubMed]
- Abraham, P.; Marin, G.; Filleron, A.; Michon, A.-L.; Marchandin, H.; Godreuil, S.; Rodière, M.; Sarrabay, G.; Touitou, I.; Meslin, P.; et al. Evaluation of post-infectious inflammatory reactions in a retrospective study of 3 common invasive bacterial infections in pediatrics. Medicine 2022, 101, e30506. [Google Scholar] [CrossRef]
- Cheng, M.H.; Zhang, S.; Porritt, R.A.; Rivas, M.N.; Paschold, L.; Willscher, E.; Binder, M.; Arditi, M.; Bahar, I. Superantigenic character of an insert unique to SARS-CoV-2 spike supported by skewed TCR repertoire in patients with hyperinflammation. Proc. Natl. Acad. Sci. USA 2020, 117, 25254–25262. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Riitano, F.; Valentini, P. Pediatric inflammatory multisystem syndrome temporally related with SARS-CoV-2: Immunological similarities with acute rheumatic fever and toxic shock syndrome. Front. Pediatr. 2020, 8, 574. [Google Scholar] [CrossRef] [PubMed]
- La Torre, F.; Calabrese, G.; Signorile, K.; Bizzoco, F.; Mastrorilli, C.; Strippoli, A.; Amato, D.; Carella, F.; Vairo, U.; Giordano, P.; et al. Efficacy of sildenafil and high-dose anakinra in an MIS-C patient with pulmonary vasculitis: A case report. Front. Pediatr. 2023, 10, 1015617. [Google Scholar] [CrossRef]
- Cobo-Vázquez, E.; Aguilera-Alonso, D.; Carrasco-Colom, J.; Calvo, C.; Saavedra-Lozano, J.; Mellado, I.; Grandioso, D.; Rincón, E.; Jové, A.; Cercenado, E.; et al. Increasing incidence and severity of invasive Group A streptococcal disease in Spanish children in 2019–2022. Lancet Reg. Health-Eur. 2023, 27, 100597. [Google Scholar] [CrossRef]
- Cobo-Vázquez, E.; Aguilera-Alonso, D.; Carbayo, T.; Figueroa-Ospina, L.M.; Sanz-Santaeufemia, F.; Baquero-Artigao, F.; Vázquez-Ordoñez, C.; Carrasco-Colom, J.; Blázquez-Gamero, D.; Jiménez-Montero, B.; et al. Epidemiology and clinical features of Streptococcus pyogenes bloodstream infections in children in Madrio, Spain. Eur. J. Pediatr. 2023, 182, 3057–3062. [Google Scholar] [CrossRef]
- Goldstein, B.; Giroir, B.; Randolph, A. International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatr. Crit. Care Med. 2005, 6, 2–8. [Google Scholar] [CrossRef]
- Oehmcke, S.; Mörgelin, M.; Malmström, J.; Linder, A.; Chew, M.; Thorlacius, H.; Herwald, H. Stimulation of blood mononuclear cells with bacterial virulence factors leads to the release of pro-coagulant and pro-inflammatory microparticles. Cell. Microbiol. 2011, 14, 107–119. [Google Scholar] [CrossRef]
- Oehmcke, S.; Mörgelin, M.; Herwald, H. Activation of the human contact system on neutrophil extracellular traps. J. Innate Immun. 2009, 1, 225–230. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Brill, A.; Duerschmied, D.; Schatzberg, D.; Monestier, M.; Myers, D.D., Jr.; Wrobleski, S.K.; Wakefield, T.W.; Hartwig, J.H.; Wagner, D.D. Extracellular DNA traps promote thrombosis. Proc. Natl. Acad. Sci. USA 2010, 107, 15880–15885. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Diorio, C.; McNerney, K.O.; Lambert, M.; Paessler, M.; Anderson, E.M.; Henrickson, S.E.; Chase, J.; Liebling, E.J.; Burudpakdee, C.; Lee, J.H.; et al. Evidence of thrombotic microangiopathy in children with SARS-CoV-2 across the spectrum of clinical presentations. Blood Adv. 2020, 4, 6051–6063. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, L.R.; Rose, E.B.; Horwitz, S.M.; Collins, J.P.; Newhams, M.M.; Son, M.B.F.; Newburger, J.W.; Kleinman, L.C.; Heidemann, S.M.; Martin, A.A.; et al. Multisystem inflammatory syndrome in U.S. children and adolescents. N. Engl. J. Med. 2020, 383, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, L.; Shekhar, S.; Bansal, A.; Kumar, S. COVID-19 associated arterial ischaemic stroke and multisystem inflammatory syndrome in children: A case report. Lancet Child Adolesc. Health 2021, 5, 88–90. [Google Scholar] [CrossRef] [PubMed]
- Krasic, S.; Popovic, S.; Kravljanac, R.; Prijic, S.; Vukomanovic, V. Intracardiac Thrombosis in the Three-Year-Old Boy with Normal Left Ventricle Systolic Function in MIS-C Associated with COVID-19. Mediterr. J. Hematol. Infect. Dis. 2022, 14, e2022028. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ozyurek, E.; Balta, G.; Degerliyurt, A.; Parlak, H.; Aysun, S.; Gürgey, A. Significance of factor V, prothrombin, MTHFR, and PAI-1 genotypes in childhood cerebral thrombosis. Clin. Appl. Thromb. 2007, 13, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Alfirevic, Z.; Simundic, A.-M.; Nikolac, N.; Sobocan, N.; Alfirevic, I.; Stefanovic, M.; Vucicevic, Z.; Topic, E. Frequency of Factor II G20210A, Factor V Leiden, MTHFR C677T and PAI-1 5G/4G Polymorphism in Patients with Venous Thromboembolism: Croatian Case Control Study. Biochem. Medica 2010, 20, 229–235. [Google Scholar] [CrossRef]
- Monagle, P.; Cuello, C.A.; Augustine, C.; Bonduel, M.; Brandão, L.R.; Capman, T.; Chan, A.K.C.; Hanson, S.; Male, C.; Meerpohl, J.; et al. American Society of Hematology 2018 Guidelines for management of venous thromboembolism: Treatment of pediatric venous thromboembolism. Blood Adv. 2018, 2, 3292–3316. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normal Ranges | Day 1 * | Day 3 | Day 5 ** | Day 7 | |
|---|---|---|---|---|---|
| White blood count | 5.5–15.5 × 109/L | 37.43 | 19.26 | 24.99 | 25.79 |
| Lymphocytes | 29–65% | 3.4 | 17.1 | 15.5 | 17.7 |
| Neutrophils | 30–60% | 94.5 | 76.4 | 82.1 | 79.9 |
| Red blood count | 3.9–5.1 × 1012/L | 4.51 | 3.06 | 3.57 | 3.76 |
| Hemoglobin | 111–143 g/L | 114 | 75 | 87 | 93 |
| Platelets | 286–509 × 109/L | 82 | 74 | 430 | 633 |
| Erythrocyte sedimentation rate | 1–18 mm/h | 35 | – | – | 30 |
| C-reactive protein | 0–5 mg/L | 503.27 | >200 | 20.4 | 20.5 |
| Procalcitonin | <0.1 ng/mL | 42.29 | – | 14.58 | 0.3 |
| Ferritin | 4.4–64 ng/mL | 8494.2 | 667 | – | 509 |
| Uric acid | 0–420 µmol/L | 610 | 289 | – | 256 |
| Albumin | 38–54 g/L | 31.99 | – | – | 35.77 |
| Troponin I | 0–1 ng/mL | <0.01 | 0.011 | 0.003 | <0.01 |
| NT-pro BNP | <300 pg/mL | 9105 | 1357 | 420 | 302 |
| ASAT | <50 U/L | 159 | – | – | 15 |
| ALAT | <36 U/L | 64 | – | – | 12 |
| LDH | 120–300 U/L | 975 | 284 | – | 324 |
| Antistreptolysin O titer | 0–150 IU/mL | 6.16 | – | – | 178.52 |
| Fibrinogen | 200–400 mg/dL | 354 | 274 | – | 314 |
| D-dimer | <500 ng/mL | >3000 | 2878 | 1895 | 936.5 |
| aPTT | 28–34 s | 47.4 | 24.3 | 24.7 | 25.9 |
| INR | 0.9–1.2 | 2.06 | 1.37 | 1.28 | 1.07 |
| Prothrombin time | 11–14 s | 27 | 18.7 | 17 | 12.7 |
| SARS-CoV-2 IgM/IgA | >0.6 BAU/mL | 1.78 | – | – | – |
| SARS-CoV-2 IgG | >1.6 BAU/mL | 8.4 | – | – | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoyanova, Z.; Temelkova, K.; Ganeva, M.; Vasilev, T.; Dasheva-Dimitrova, A.; Kibarova-Hristova, D.; Stefanov, S. A Clinical Case of Multisystem Inflammatory Syndrome After SARS-CoV-2 Infection Associated with Group A β-Hemolytic Streptococcus Coinfection and Venous Thrombosis in a Child with Congenital Thrombophilia. Curr. Issues Mol. Biol. 2025, 47, 334. https://doi.org/10.3390/cimb47050334
Stoyanova Z, Temelkova K, Ganeva M, Vasilev T, Dasheva-Dimitrova A, Kibarova-Hristova D, Stefanov S. A Clinical Case of Multisystem Inflammatory Syndrome After SARS-CoV-2 Infection Associated with Group A β-Hemolytic Streptococcus Coinfection and Venous Thrombosis in a Child with Congenital Thrombophilia. Current Issues in Molecular Biology. 2025; 47(5):334. https://doi.org/10.3390/cimb47050334
Chicago/Turabian StyleStoyanova, Zdravka, Katya Temelkova, Margarita Ganeva, Teodor Vasilev, Anna Dasheva-Dimitrova, Desislava Kibarova-Hristova, and Stefan Stefanov. 2025. "A Clinical Case of Multisystem Inflammatory Syndrome After SARS-CoV-2 Infection Associated with Group A β-Hemolytic Streptococcus Coinfection and Venous Thrombosis in a Child with Congenital Thrombophilia" Current Issues in Molecular Biology 47, no. 5: 334. https://doi.org/10.3390/cimb47050334
APA StyleStoyanova, Z., Temelkova, K., Ganeva, M., Vasilev, T., Dasheva-Dimitrova, A., Kibarova-Hristova, D., & Stefanov, S. (2025). A Clinical Case of Multisystem Inflammatory Syndrome After SARS-CoV-2 Infection Associated with Group A β-Hemolytic Streptococcus Coinfection and Venous Thrombosis in a Child with Congenital Thrombophilia. Current Issues in Molecular Biology, 47(5), 334. https://doi.org/10.3390/cimb47050334